")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 11
Parental Traditional Medicine Use for Children and Associated Factors in North Mecha District, North West Ethiopia
Authors Tizazu D, Workineh Y , Ayalew Y
Received 3 August 2020
Accepted for publication 24 November 2020
Published 16 December 2020 Volume 2020:11 Pages 505—512
DOI https://doi.org/10.2147/PHMT.S275249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Dawit Tizazu, Yinager Workineh, Yeneneh Ayalew
Department of Child Health Nursing, College of Medicine and Health Science, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Dawit Tizazu; Yinager Workineh Tel +251918147549
Email [email protected]; [email protected]
Introduction: Traditional medicine (TM) has existed in human societies before application of modern science to health. Even though there have been many studies conducted on adults’ TMuse, there were limited studies done on the issue of parenteral TM use to children in Ethiopia. Therefore, this study aimed to assess the prevalence and associated factors of parental TM use for children in North Mecha District, North West Ethiopia.
Methods: A community-based cross-sectional study was conducted among 374 parents with children aged under 18 in the North Mecha District from March 1st to 30th, 2020. A multistage sampling technique was used. Kebeles were selected by using a simple random sampling method from the district. Then, the sample size was proportionally allocated to each kebele. Households were selected by using a table of random sampling technique from the kebele. An interviewer-administered questionnaire was used to collect the data. The bivariable and multivariable logistic regression models were used to assess the association between dependent and independent variables. Factors that had a statistically significant association with the dependent variable (p< 0.05) were identified as significant in the multivariable logistic regression analysis.
Results: From 374 sampled participants, 351 of them were participated in the study making a response rate of 93.90%. The prevalence of parental TM use for children was 90.30%. Being non educated [AOR=5.65, 95% CI: (1.25, 25.50)], rural residence [AOR=6.33, 95% CI: (1.97, 20.32)], having good attitude [AOR=4.91, 95% CI: (1.90,12.65)], very poor wealth index [AOR=8.43, 95% CI: (3.08, 23.06)] and accessibility of TM [AOR=4.01, 95% CI: (1.11, 14.38)] were the determinants of TM utilization.
Conclusion: TM use was high in this study. TM utilization was affected by modifiable factors. Therefore, the government should give especial emphasis to factors of parental TM use for children under 18-year-old.
Keywords: traditional medicine; TM, parent, children, Ethiopia
Introduction
About 80% of the world's population depends on traditional medicine (TM) for their primary health care needs.1 The utilization of TM ranges from 70.00% up to 95.00% in developing countries specifically in Asia and Africa.1,2 In Africa, around 90.00% of the population depends on TM use, especially in sub-Saharan Africa.3,4 Similarly, 80.00% of the Ethiopian population depends on TM for their primary health care needs.1,4,5
As a result of the presence of different biodiversity, cultures, beliefs, and languages in Ethiopia, there is increase of utilization of TM ranging from noninvasive up to invasive procedures. The main reason to use TM was accessibility, low price, low income, low educational level, their effectiveness, and inaccessibility of modern health services.6,7
The report in Ethiopia indicated that more than half of all TM are prescribed, dispensed as well as sold illegally by a traditional healer. Half of all users take TM medicine incorrectly.8 Utilization of TM brings negative or dangerous effects on traditional healer or consumer or both.2 As a result of this, many patients have complications, and are hospitalized due to adverse effects of TM.9 The secretive nature of some traditional healers creates barriers to treat and prevent complications.10 In addition to this, utilization of TM causes delays in seeking medical care in case of fatal and chronic diseases.11–13
There was a lack of national standards, official recognition, regulatory bodies and scientific evidence-based for TM therapies in the Ethiopian context.3 Currently, the government has begun to establish a road map on the integration of TM with modern medicine (MM) by setting national standards of TM use.14
TM in Ethiopia is not uniformly practiced. Its uses are considerably diverse and vary significantly between regions. The standard policies and regulations to govern TM use are too weak or do not exist at all. Instead, the users are associated with cultural beliefs. As such, the prevalence and utilization, as well as factors determining TM use for all categories of population in general and pediatric age groups in particular are not adequately studied and documented before. Hence, dealing with TM use among under 18-year-olds is vital to give direction for designing strategies. Therefore, the purpose of this study was to assess the prevalence and associated factors of parental TM use for children in North Mecha District, North West Ethiopia, 2020.
Methods and Materials
Study Area, Design and Period
A community-based cross-sectional study was conducted in North Mecha District from March 1st–30th, 2020. North Mecha District is located 516 Km North West of Addis Ababa, the capital of Ethiopia, and 36 km from Bahir Dar, the capital of the Amhara region. Merawi is the town of North Mecha District. The District has 38 kebeles and around 355,557 populations. From those, 88,592 are under 18 years-old. There is one public hospital, 10 public health centers, 24 health posts, and 4 private clinics. There are 97 health extension workers, 213 diploma Nurses, 76 BSc Nurses, 64 diploma Midwives, 27 BSc Midwives, 26 health officers, and 11 Medical Doctors in this District.15
Participants’ Selection and Exclusion
All parents who have children under 18 years of age and live in the North Mecha district were the source population. All parents with children under 18 who permanently reside in randomly selected kebeles were study participants. On the other hand, parents who were seriously ill during the data collection period were excluded from the study.
Sample Size Determination and Sampling Techniques
The sample size was calculated using Epi-Info version 3.5.1 statistical software package by considering the following assumptions. The assumptions used were 95% confidence interval (CI), 80% power of the study, 2.41 odds ratio, 32.00% of unexposed outcome16 1:1 exposed to unexposed, 10% non-response rate and a design effect of 2. The final sample size was 374.
A multistage sampling technique was employed to select the study subjects. The study area, the North Mecha District, has a total of 38 kebeles. Thirteen kebeles were selected by using a simple random sampling method. The census was carried out to code households with children under 18. The sample size was proportionally allocated to the selected kebeles. Households from each selected kebele were chosen by simple random sampling methods (table of random). Finally, the interviews with parents was carried out in their own homes to maintain their privacy.
Measurements
Data was collected by using an adapted, pre-tested, structured, interviewer-administered questionnaire. The questionnaire was adapted from previous researche carried out on similar topics in Ethiopia.16 Wealth index questions were added to the final version of the questionnaire, but there were no omitted questions. The questionnaire was translated into the local language (Amharic). Consistency and equivalency was checked by translating the Amharic version back to English by another individual who was fluent in both languages. The questionnaire constituted seven parts. The first part comprised of the socio-demographic characteristics of parents. The second part included wealth index measuring items. The third part outlined the type and TM practice. The fourth section addressed the enabling factors, need factors and perceived illness/sickness of the respondents. Fifth part of the questionnaire was about health care experience of the respondents. The final part of the questionnaire contained questions about parental attitude towards TM (Appendix I).
Satisfaction is a feeling of happiness or pleasure because of achieving something or getting what you wanted. The participants’ response in the case of satisfaction was categorized as: 1) completely dissatisfied; 2) somewhat dissatisfied; 3) neither satisfied nor dissatisfied; 4) somewhat satisfied; and 5) completely satisfied.
Efficacy is how well TM works or brings the results that is hoped for. The response of the respondents for this variable was labeled as: 1) very poor; 2) poor; 3) fair; 4) good; and 5) very good.
An attitude is the result of experience or upbringing of the TM utilization. Attitude towards TM use was classified as good when study participants answered greater than or equal to the mean score of the attitude questions and poor if study participants answered below the mean score of attitude questions.17–19 TM, the dependent variable, is anything used in the promotion of health, prevention of illness and treatment of diseases. Currently, it is not considered to be part of MM, but is accepted in that community. TM is neither prescribed by health care professionals nor used commonly as a diet in that particular culture.16,20 If the parents used any of the above defined TM for their children, they are labeled as TM users, and if they did not use, they are classified as non-users.
Data Quality Control
The data collectors and supervisors were trained for two days on the techniques of data collection method. Throughout the data collection time, strict regular monitoring and supervision of the interviewers’ overall activities were done by the supervisor and principal investigator. A pre-test was done outside the study area on 5% of the total sample size to check the consistency of the tool. After the pre-test, any necessary adjustments were made on the tool.
Data Processing and Analysis
The data were cleaned, coded, and entered into Epi data version 3.2 and transferred to SPSS version 25.0 for analysis. Descriptive statistics like frequency, proportions, and percentage were used to summarize the study variable.
Wealth index of the individual household was analyzed by principal component analysis (PCA) method. Due to the binary nature of all test items, polychoric PCA was used. PCA is a variable reduction technique that reduces a set of observed variables into a smaller set of uncorrelated components (i.e., principal components) which account for most of the variance in the observed variables.
Bivariable and multivariable logistic regressions models were used to test association between the dependent and independent variables. Variables with p-value < 0.25 in the binary logistic regression were considered as candidate variables for the multivariable logistic regression model. Factors that had a statically significant association with the dependent variable (p <0.05) were identified as significant in the multivariable logistic regression analysis.
Results
Socio-Demographic Characteristics
From the 374 sampled participants, 351 of them had participants making the response rate of 93.90%. Out of 351 respondents in this study, 249 (70.90%) were female. The mean age of the parents in this study was 38 ± 9.80 years. Two hundred ninety-four (83.80%) participants were Orthodox religion followers. Regarding marital status, 254 (73.80%) of the participants were married. One hundred-eighteen (33.60%) of participants could not read and write. In the case of occupational status, 160 (45.60%) of the respondents were housewives. Of all respondents, 168 (47.90%) of them had one to two children. The mean number of children in the family was 2±0.82. Around one-third of the participants, 215 (61.3.0%) were a very poor wealth index (Table 1).
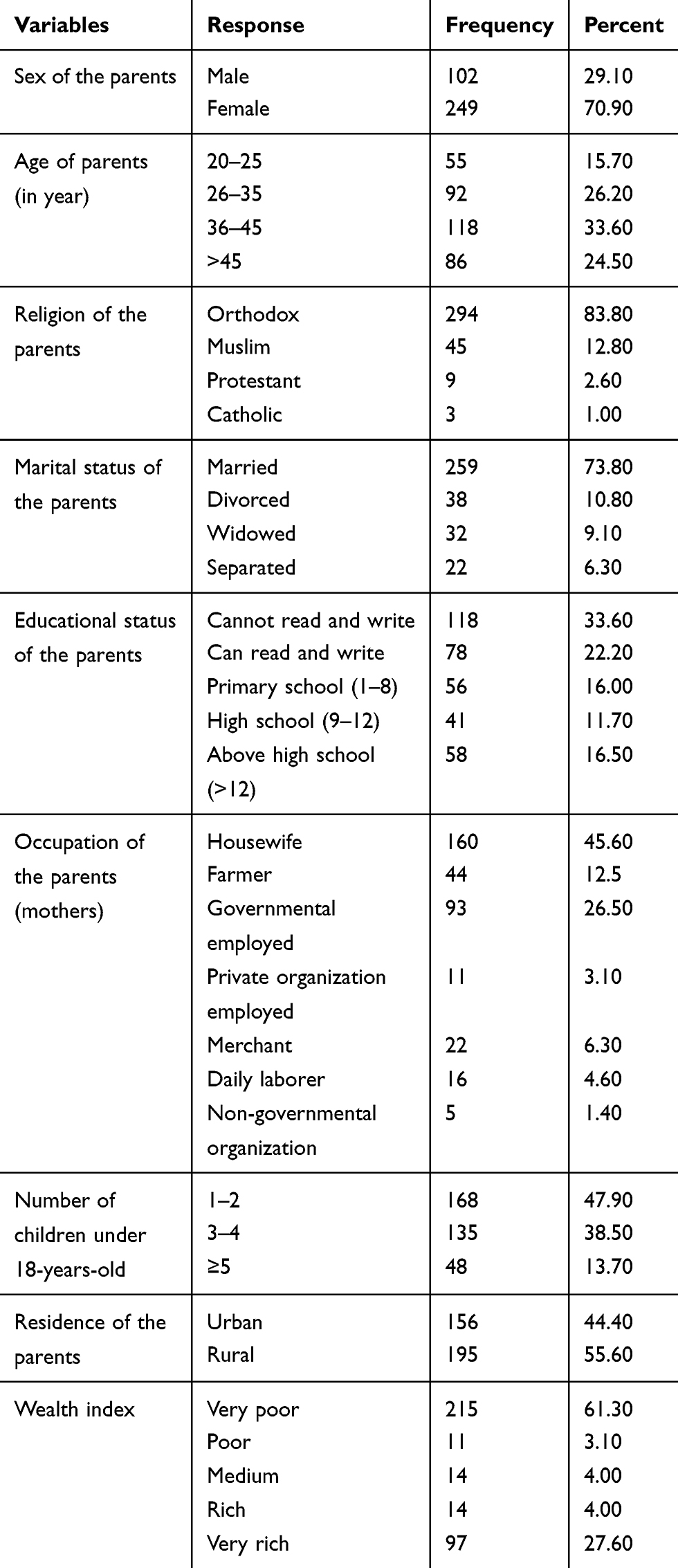 |
Table 1 Socio Demographic Characteristics of Parents in North Mecha District, North West Ethiopia, 2020 (n=351) |
Prevalence of Traditional Medicine Use for Children
From the total participants, 317 (90.30%) of them were used TM for their children in the last 12 months. One hundred thirty-eight (43.50%) respondents used a drinkable form of TM. Among TM users, 175 (55.20%) of them used herbal medicine at least once for their children in the last 12 months (Table 2).
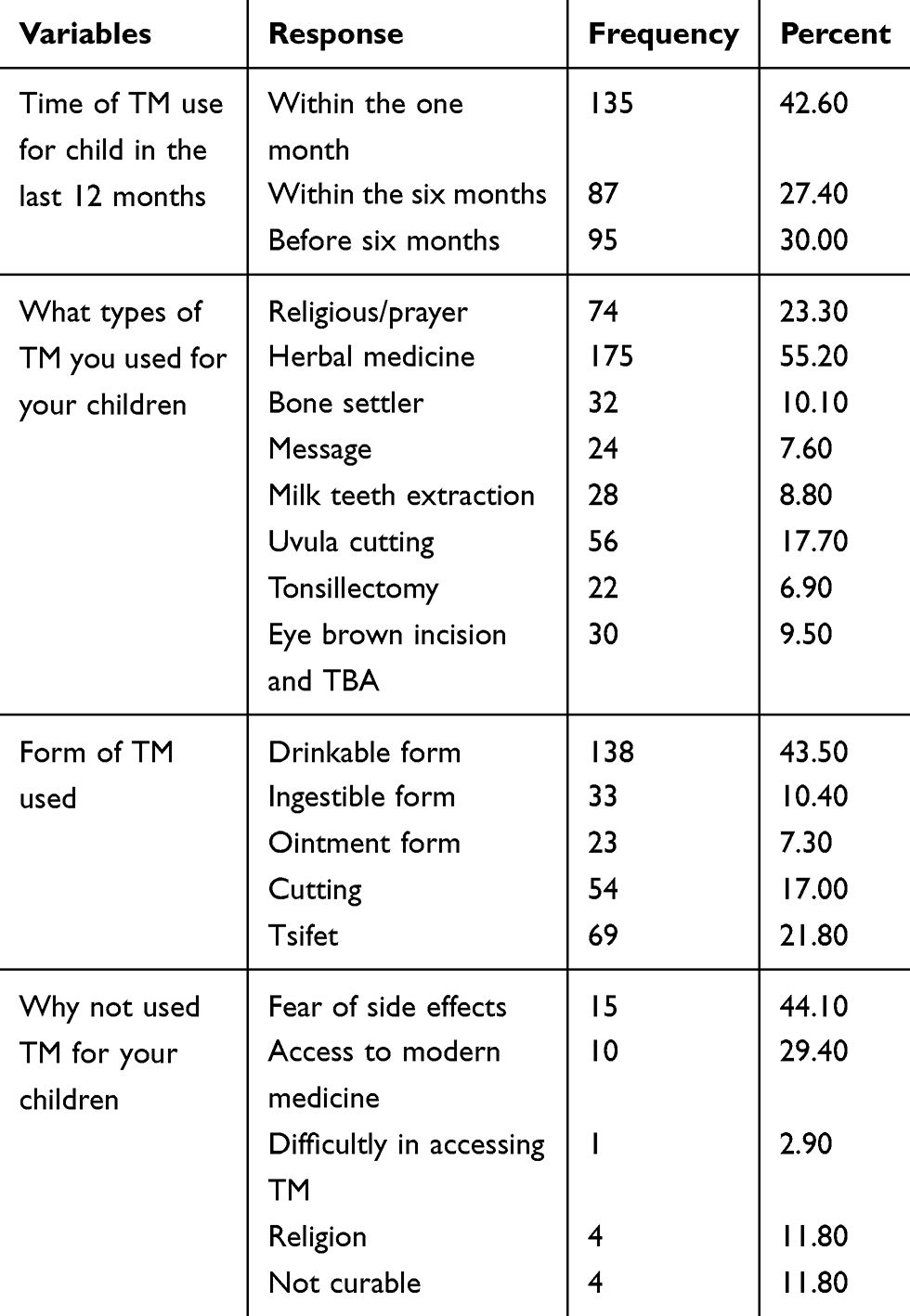 |
Table 2 Parental Traditional Medicine Use for Children in North Mecha District, North West Ethiopia, 2020 (n=351) |
Enabling and Need Factors
Among the total respondents, 117 (39.30%) of them mentioned accessibility as a reason to use TM. Family (43.80%) was a major source of information for the utilization of TM. More than half – 158 (58.40%) – of the parents used TM to treat illness or relief symptoms. From total TM utilizers, 71 (22.70%) and 201 (63.40%) of them used it for respiratory (pulmonary) and chronic diseases, respectively (Table 3).
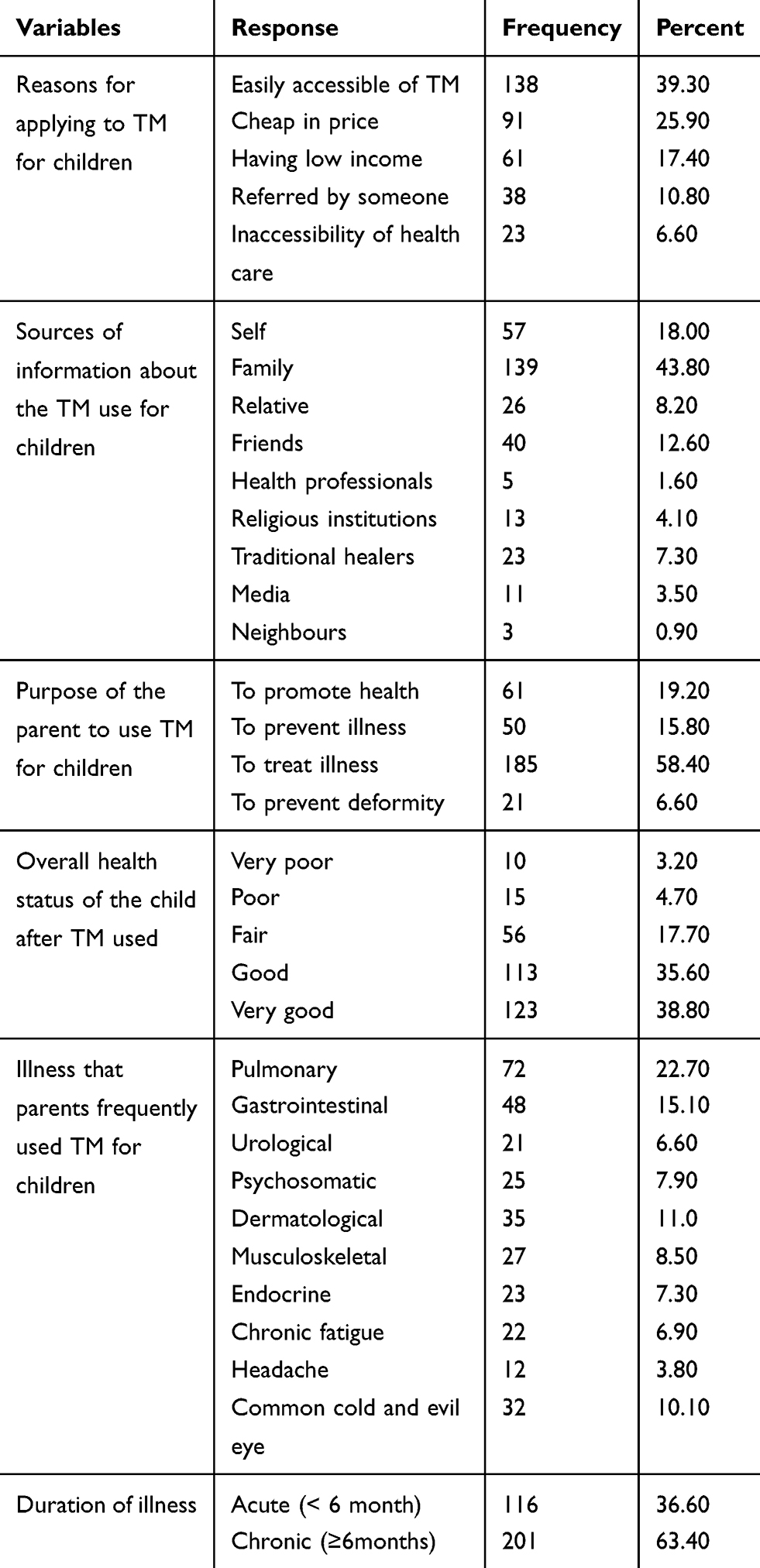 |
Table 3 Enabling and Need Factors for Parental TM Use for Children in North Mecha District, North West Ethiopia, 2020 (n=351) |
Parental Health Care Experience and Attitude Towards TM Use
Among the total participants, 150 (42.70%) of them used TM for themselves. Of the self-TM users, 100 (66.70%) of them were mothers. Seventy-eight (22.20%) participants stated that they were satisfied with TM use. One hundred fifty-three (46.50%) respondents said that the efficacy TM is good. From all the TM users, 134 (40.70%) of them were completely satisfied about the utilization of TM. Regarding attitude towards TM use, 231 (65.80%) had a good attitude towards TM use for children. Nearly three-quarters, 263 (74.90%) of the participants had a plan to use TM in the future. Two hundred-nineteen (62.40%) participants encouraged others to use TM. Two hundred-seventeen (61.80%) participants reported that there were some diseases that are not cured by MM (Table 4).
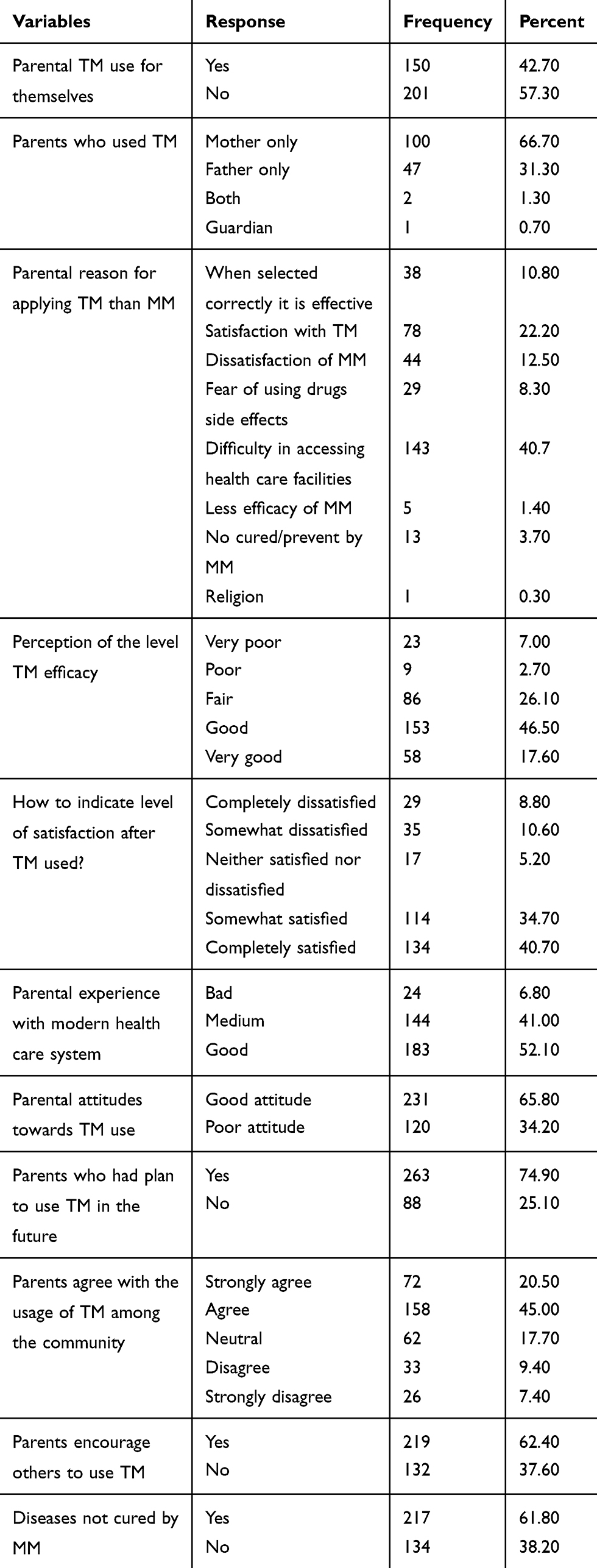 |
Table 4 Parental Health Care Experience and Attitude Towards TM Use for Children in North Mecha District, North West Ethiopia, 2020 (n=351) |
Factors Associated with Traditional Medicine Use for Children
Study participants who did not read and write were 6 times [AOR=5.65, 95% CI: (1.25, 25.50)] more likely to use TM for children than parents who had high school and above educational level. Similarly, parents from the rural residences were 6 times [AOR=6.33, 95% CI: (1.97, 20.32) more likely to use TM for their children when compared to the urban residences. Respondents who had a very poor wealth index had 8 folds [AOR=8.43, 95% CI: (3.08, 23.06)] to use TM for their children when compared to very rich respondents. Regarding the level of attitudes, parents with good attitude towards TM use were 5 times [AOR=4.91, 95% CI: (1.90, 12.65)] more likely to use TM for children than parents with a poor attitude. Additionally, easily accessible of TM increases the utilization of TM by 4 folds [AOR=4.01, 95% CI: (1.11, 14.38)] as compared to inaccessibility of TM (Table 5).
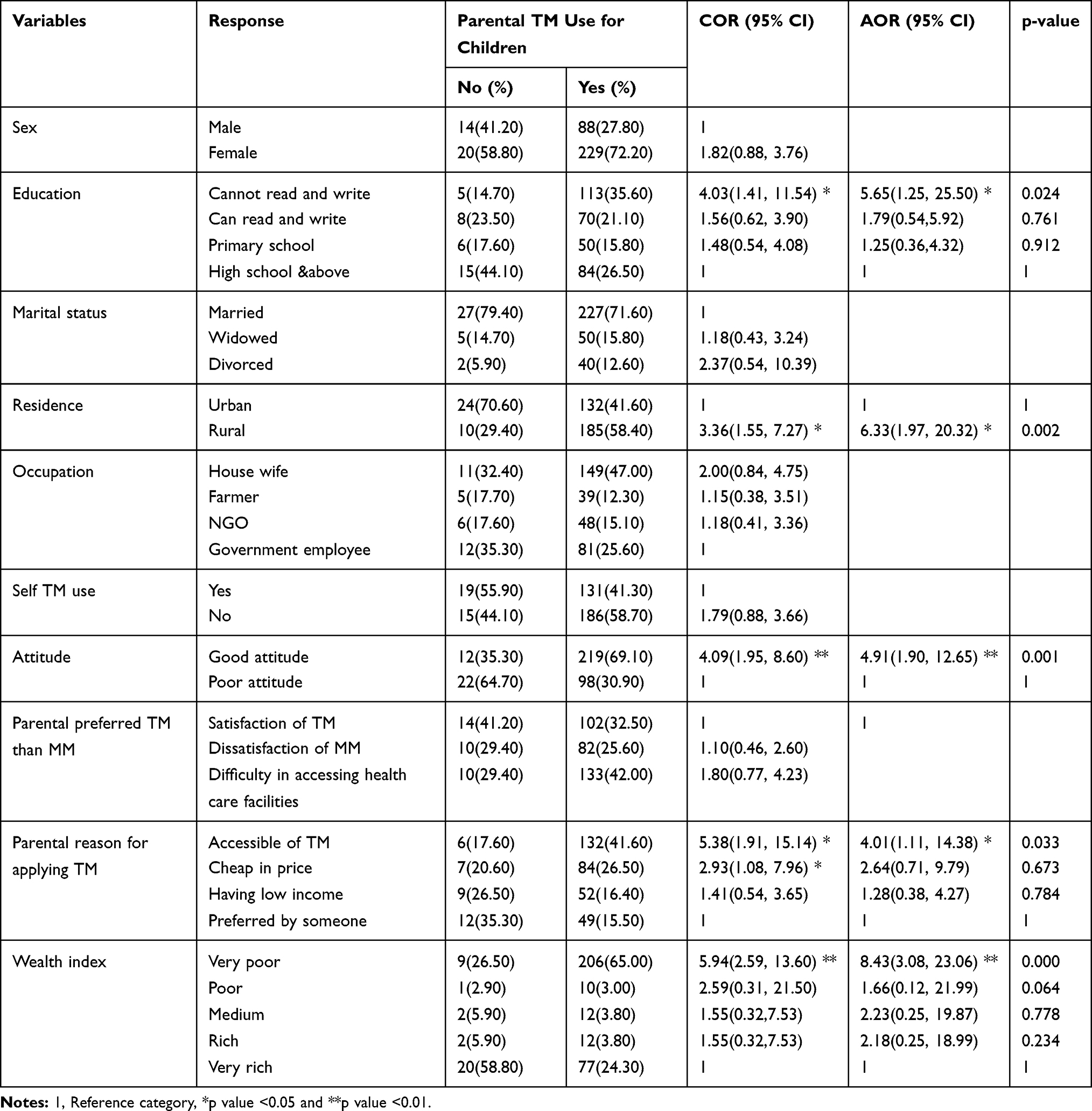 |
Table 5 Factors Associated with Parental TM Used for Children in North Mecha District, North West Ethiopia, 2020 (n=351) |
Discussion
The prevalence of parental TM use for children in this study was 90.3%. This result was almost consistent with the previous studies conducted in Shendi town, Sudan (92%).19 Similarly, this study was in line with the previous studies conducted in Axum town (87.8%)23 and Motta town (88.2%) in Ethiopia.16 On the other hand, this study was lower than the previous study conducted in East Wollega (94.2%) in Ethiopia.22 The possible justification for this discrepancy might be due to the sample size and study population. In this study, the respondents were parents who had children under 18, but the previous study participants were adult individuals. However, the current study finding was higher than the previous studies conducted in Korea (65.3%), Australia (68.5%), United Kingdom 38%, Europe (52%), Nigeria (84%) and Ghana (86.1%).23–28 The high label of TM utilization by participants in Ethiopia is due to the presence of easily accessible TM, low price of TM, low income, low formal educational level and the inaccessibility of modern health services.13
Parental TM use for their children was determined by different factors in the current study. Parents from rural residence had high odds to use TM for children than the urban participants. This study was supported by studies conducted in Australia,26 and East Iran.20 The possible justification for high level of TM utilization in rural residence as compared to urban area is due to the absence of better information, lack of awareness, low level of formal education and scarcity of money or cash to pay for modern health care services.12
Similarly, having a very poor wealth index increases parental TM use for children in this study. This finding was in line with studies conducted in Saudi Arabia,18 East Iran,20 Shendi City, Sudan,19 Axum town,21 and Motta town.16 Another factor that affects parental TM use for children was TM accessibility. Parents who had easily accessible of TM were more likely to use TM for children as compared with their counterparts. This study was consistent with the studies conducted in Shendi City,19 Ghana,25 Axum town21 and Motta town.16 In the same fashion, parents who had a good attitude towards TM were more likely to use TM for children as compared with parents who had a poor attitude towards TM. This finding was supported by other studies conducted in the university of Karbala, Iraq,18 Plateau State, Nigeria17 and East Wollega Zone.22 The last, but not the least, factor that affects the utilization of TM was being non-educated. This finding was similar to the study conducted in the United Kingdom,29 Korea,28 and Australia.27 It is also congruent with the study done in Shendi, Sudan,19 Axum town,21 and Motta town.16 The high level of TM utilization among formally and non-formally educated participants was due to a lack of understanding about MM than formally educated parents.
This study encountered different limitations. First, it faced recall bias since it assessed certain past events. Second, inflated results could be seen since it assessed cultural issues.
Conclusion
TM use was high in the current study area. This high level of TM was mainly determined by modifiable factors. Therefore, the government should give especial emphasis to prevent factors of parental TM use for children under 18.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio; HEWs, health extension workers; MM, modern medicine; OR, odds ratio; SPSS, Statistical Package for Social Science; TM, traditional medicine; WHO, World Health Organization.
Data Sharing Statement
The data of this study can’t be shared publicly due to presence of sensitive (confidential) participants’ information.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The ethical approved was obtained from the Ethical Review Committee of the College of Medicine and Health Sciences, Bahir Dar University with ethical approval number CMHS/IRB/01/008/2020. Written informed consent was taken from each study participant before running the study (Appendix II).
Acknowledgments
We are grateful to Bahir Dar University, kebele leaders, study participants, data collectors and supervisors for the support of the overall process of the research procedure.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. World Health Organization. WHO Global Report on Traditional and Complementary Medicine 2019. World Health Organization; 2019.
2. World Health Organization. WHO Traditional Medicine Strategy 2014–2023. Geneva: World Health Organization; 2015.
3. World Health Organization. The Regional Strategy for Traditional Medicine in the Western Pacific (2011–2020). 2012.
4. Ashenif T. Ethiopian Herbal Medicine Research Article Profile Part 1. 2017.
5. World Health Organization. Traditional Medicine Strategy. 2014:2017
6. Frawley J, Adams J, Sibbritt D, Steel A, Broom A, Gallois C. Prevalence and determinants of complementary and alternative medicine use during pregnancy: results from a nationally representative sample of Australian pregnant women. Aust N Z J Obstet Gynaecol. 2013;53(4):347–352. doi:10.1111/ajo.12056
7. Birdee GS, Phillips RS, Davis RB, Gardiner P. Factors associated with pediatric use of complementary and alternative medicine. Pediatrics. 2010;125(2):249–256. doi:10.1542/peds.2009-1406
8. Haile KT, Ayele AA, Mekuria AB, Demeke CA, Gebresillassie BM, Erku DA. Traditional herbal medicine use among people living with HIV/AIDS in Gondar, Ethiopia: do their health care providers know? Complement Ther Med. 2017;35:14–19. doi:10.1016/j.ctim.2017.08.019
9. Okoronkwo I, Onyia-pat J-L, Okpala P, Agbo M-A, Ndu A. Patterns of complementary and alternative medicine use, perceived benefits, and adverse effects among adult users in Enugu Urban, Southeast Nigeria. Evid Based Complement Alternat Med. 2014;2014:1–6. doi:10.1155/2014/239372
10. Birhan W, Giday M, Teklehaymanot T. The contribution of traditional healers’ clinics to public health care system in Addis Ababa, Ethiopia: a cross-sectional study. J Ethnobiol Ethnomed. 2011;7(1):39. doi:10.1186/1746-4269-7-39
11. Marais A, Steenkamp V, Du Plooy WJ. Conditions frequently self-treated with herbal remedies by patients visiting a tertiary hospital in Gauteng, South Africa. S Afr Fam Pract. 2015;57(1):8–11. doi:10.1080/20786190.2014.977066
12. Bantie GM, Meseret Z, Bedimo M, Bitew A. The prevalence and root causes of delay in seeking healthcare among mothers of under five children with pneumonia in hospitals of Bahir Dar city, North West Ethiopia. BMC Pediatr. 2019;19(1):482. doi:10.1186/s12887-019-1869-9
13. Bopape M, Mothiba T, Malema R. Indigenous practices of traditional health practioners (THPs) methods by mothers of children admitted to the Polokwane/Mankweng hospital complex, Limpopo Province, South Africa. Afr J Phys Health Edu Recreat Dance. 2013;19(Supplement 1):147–158.
14. Hailu F, Cherie A, Gebreyohannis T, Hailu R. Determinants of traditional medicine utilization for children: a parental level study in Tole District, Oromia, Ethiopia. BMC Complement Med Ther. 2020;20(1):1–11. doi:10.1186/s12906-020-02928-1
15. North Mecha Wareda Administration Office. Statistics Data. 2018.
16. Gualu T. Prevalence and Factors Associated with Parental Traditional Medicine Use for Children in Motta Town, Amhara Regional State, Ethiopia, 2014. Addis Ababa University; 2014.
17. Ohemu T, Sariem C, Dafam D, et al. Knowledge, Attitude and Practice of Traditional Medicine Among People of Jos North Local Government Area of Plateau State, Nigeria. 2017.
18. Abdulzahra NC. Attitude of mothers toward herbal treatment of their children. Kerbala J Med. 2012;5(11):1384–1389.
19. Alhadi LE, Mohammed AS, Elnageeb MM, Mohmmed SA. Awareness and Attitude of Mothers About Herbal Medicine Used to Treat Children Aged Under 5 Years in Shendi City, Sudan. 2019.
20. Fesharakinia A, Abedini M. Prevalence of using complementary and alternative medicine in children and its related factors in east Iran. Iran J Pediatr. 2014;24(1):111.
21. Gebrekirstos K, Abebe M, Fantahun A. A cross sectional study on factors associated with harmful traditional practices among children less than 5 years in Axum town, north Ethiopia, 2013. Reprod Health. 2014;11(1):46. doi:10.1186/1742-4755-11-46
22. Gari A, Yarlagadda R, Wolde-Mariam M. Knowledge, attitude, practice, and management of traditional medicine among people of Burka Jato Kebele, West Ethiopia. J Pharm Bioallied Sci. 2015;7(2):136. doi:10.4103/0975-7406.148782
23. Zuzak TJ, Boňková J, Careddu D, et al. Use of complementary and alternative medicine by children in Europe: published data and expert perspectives. Complement Ther Med. 2013;21:S34–S47. doi:10.1016/j.ctim.2012.01.001
24. Oshikoya KA, Senbanjo IO, Njokanma OF, Soipe A. Use of complementary and alternative medicines for children with chronic health conditions in Lagos, Nigeria. BMC Complement Altern Med. 2008;8(1):66. doi:10.1186/1472-6882-8-66
25. Gyasi RM, Siaw LP, Mensah CM. Prevalence and pattern of traditional medical therapy utilisation in Kumasi metropolis and Sekyere south district, Ghana. J Ethnopharmacol. 2015;161:138–146. doi:10.1016/j.jep.2014.12.004
26. Frawley JE, Anheyer D, Davidson S, Jackson D. Prevalence and characteristics of complementary and alternative medicine use by Australian children. J Paediatr Child Health. 2017;53(8):782–787. doi:10.1111/jpc.13555
27. Gad A, Al-Faris E, Al-Rowais N, Al-Rukban M. Use of complementary and alternative medicine for children: a parents’ perspective. Complement Ther Med. 2013;21(5):496–500. doi:10.1016/j.ctim.2013.06.007
28. Kim J-H, Nam C-M, Kim M-Y, Lee D-C. The use of complementary and alternative medicine (CAM) in children: a telephone-based survey in Korea. BMC Complement Altern Med. 2012;12(1):46. doi:10.1186/1472-6882-12-46
29. Crawford NW, Cincotta DR, Lim A, Powell CV. A cross-sectional survey of complementary and alternative medicine use by children and adolescents attending the University Hospital of Wales. BMC Complement Altern Med. 2006;6(1):16. doi:10.1186/1472-6882-6-16
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.