")
Back to Journals » Patient Preference and Adherence » Volume 15
Parental Satisfaction with Their Children’s Rapid Palatal Expansion Treatment Provided by Orthodontists and Pediatric Dentists
Authors Alwadei SH , Almotiry K, AlMawash A, Alwadei FH, Alwadei AH
Received 22 November 2020
Accepted for publication 12 January 2021
Published 5 February 2021 Volume 2021:15 Pages 251—258
DOI https://doi.org/10.2147/PPA.S293351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Saleh H Alwadei,1 Khalid Almotiry,2 Amjad AlMawash,3 Farhan H Alwadei,1 Abdurahman H Alwadei3
1Department of Preventive Dental Sciences, College of Dentistry, Prince Sattam Bin Abdulaziz University, Alkharj, Riyadh, Saudi Arabia; 2Ministry of Health, Riyadh, Saudi Arabia; 3Department of Pediatric Dentistry and Orthodontics, College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Correspondence: Saleh H Alwadei
Department of Preventive Dental Sciences, College of Dentistry, Prince Sattam Bin Abdulaziz, University, Alkharj, 11942, Riyadh, Saudi Arabia
Tel +966115886262
Fax +966115886201
Email [email protected]
Background: Dentofacial problems have a definitive impact on patients’ psychological well-being, quality of life, and satisfaction. Therefore, patients’ satisfaction with their dentition should be an essential goal for dental caregivers.
Aim: To compare parental satisfaction with their children’s rapid palatal expansion treatment outcome provided by orthodontists and pediatric dentists.
Materials and Methods: The authors reviewed 605 medical records and contacted 134 parents whose children received early orthodontic treatment from orthodontists and pediatric dentists using a rapid palatal expander. Eighty-eight parents (65.7%) responded to a validated questionnaire about patients’ satisfaction with orthodontic treatment outcomes.
Results: At baseline; there were no significant differences in relation to parent-related demographic variables. However, there were statistically significant differences between patients’ ages and treatment duration (p < 0.001). Independent t-tests showed statistically significant differences in the means for the subscales of doctor–patient relationship and situational aspects (p < 0.05). Spearman’s rho correlation coefficients and multivariate linear regression analysis showed that the overall satisfaction is significantly related to, and can be predicted by, parents’ educational level, child’s gender, and the specialty of the dentist who provided the treatment (p < 0.05).
Conclusion: Overall parental satisfaction with their children’s rapid palatal expansion treatment is significantly higher when provided by pediatric dentists as compared with orthodontists. Factors related to doctor–patient relationship and situational aspects (ie, office location and design, appointment waiting, and treatment duration) significantly impacted parental satisfaction.
Keywords: rapid palatal expansion, parents’ satisfaction, pediatric dentists, orthodontists
Introduction
Dentofacial problems have a definitive impact on patients’ psychological well-being, quality of life, and satisfaction.1–4 Therefore, patients’ satisfaction with their dentition should be an essential goal for dental caregivers. A successful orthodontic treatment must achieve an improved esthetics and a stable functional occlusion.5 Satisfaction with orthodontic treatment outcome can be related to subjective and objective aspects, based on patient/parent perception and professional assessment, respectively. Several authors have examined the relationship between subjective factors and patient satisfaction such as doctor–patient interactions,6 occlusion stability perception,7–9 tooth alignment,9 patients’ personality traits,10,11 and patients’ motivation.12 Parents expect orthodontic treatment to improve their children’s dental health and benefit them on a socio-occupational level.13
Despite early orthodontic treatment (EOT) being a controversial topic, multiple studies have shown varying degrees of its benefits.14–20 Worldwide, previous studies have reported the need for EOT ranging from 21.3% to 59.2%.21–25 In Saudi Arabia, studies reported a similar range, from 21% to 42.8%.26–28 The majority of orthodontists recommend that the first orthodontic examination should be performed at the age of seven years, and when needed, EOT should be performed.29,30 Various data have been reported regarding pediatric dentists providing orthodontic treatment. Previous studies indicate that around 60% to 62% of pediatric dentists provided orthodontic treatment.31,32 In Saudi Arabia, it was reported that 38.8% of pediatric dentists practice orthodontics regularly.33
Very few studies have evaluated patients’ satisfaction with their orthodontic treatment in Saudi Arabia, which reported high degrees of satisfaction.34,35 To our knowledge, no studies have been conducted in Saudi Arabia to compare the outcome of rapid palatal expansion (RPE) treatment between orthodontists and pediatric dentists when measured by parental satisfaction. Therefore, the aim of this study is to evaluate the parental satisfaction with their children’s RPE outcome provided by orthodontists and pediatric dentists.
Materials and Methods
The ethical approval for this study was obtained from the Scientific Research Unit at the College of Medicine, Prince Sattam Bin Abdulaziz University, Alkharj, Riyadh (ethical approval #PSAU/COM/RC/IRB/P/58). In accordance with the Declaration of Helsinki, the participants were informed about the purpose of the study before they consented to participate. The inclusion criteria included parents of healthy children aged from six to twelve years, who received RPE to correct posterior crossbite using a fixed rapid palatal expander and have completed treatment within the last six months. Patients with craniofacial anomalies were excluded from the study. We reviewed 605 recodes of children who received RPE provided by orthodontists and pediatric dentists at five public dental centers or hospitals in Riyadh, Saudi Arabia. We identified 134 children who met the inclusion criteria and contacted their parents, whereby 88 parents (65.7%) participated in the study.
We adopted a previously validated patient satisfaction questionnaire,36 and included 21 items. The original questionnaire consisted of two parts; the first part included socio-demographic questions such as gender and age of parent and child, educational level of parents and the specialty of the dentist who provided the treatment. The second part measured the patient’s satisfaction with orthodontic treatment. The questionnaire comprised of six categories exploring patient satisfaction with: 1) doctor–patient relationship, 2) situational aspects of the orthodontic clinic, 3) dentofacial improvement, 4) psychosocial improvement, 5) dental function, and 6) a residual category. Some of the items in the original questionnaire were removed because they were not relevant to patients’ experiences and parents’ perception of the treatment outcome in the current study, or they were not applicable to how orthodontists and pediatric dentists practice clinically in Saudi Arabia.
The five-point Likert scale questionnaire was translated into Arabic using a ”Dual-Panel” translation method. A bilingual panel of four members who are proficient in both English and Arabic performed independent translations, followed by generating all versions in a panel meeting. The panel’s goal was to generate a valid translated questionnaire in Arabic that can be easily understood by parents. The translated questionnaire was then reviewed by a monolingual panel of eight native Arabic speakers with different educational backgrounds, followed by a focus group discussion to ensure the translated Arabic terms are easily understood. Participants were contacted and briefed about the purpose of the study before they consented to fill out the survey. The questionnaire was distributed and filled out electronically.
Data were analyzed using SPSS program version 22 (IBM Corp. Armonk, NY, USA). We used Chi-square tests to determine differences in demographic variables related to patients and parents. We used independent t-tests to compare differences in parental satisfaction with their children’s RPE outcome provided by orthodontists and pediatric dentists. We also used Spearman’s rho correlation coefficients to analyze the relationship between parental overall satisfaction and the demographic characteristics of patients and their parents. Lastly, we used multivariate linear regression to assess the impact of care provided by orthodontists and pediatric dentists, on the likelihood of parental overall satisfaction, controlling for demographic factors. Statistical significance was set at p-value < 0.05.
Results
Demographics
We used Chi-square tests to determine if there were statistically significant differences between categorical baseline demographic characteristics of patients (and their parents) treated by orthodontists or pediatric dentists (Table 1). No differences were found in relation to parent-related demographic variables. However, there were statistically significant differences between patients’ age and treatment duration (p < 0.001). Regarding patients’ age, treatment of all eleven patients between the age of six to eight years was provided by pediatric dentists (p < 0.0001). Regarding treatment duration, a significantly higher number of patients treated by pediatric dentists had a treatment duration of less than six months, compared to those treated by orthodontists (p < 0.0001). On the contrary, a significantly higher number of patients treated by orthodontists had a treatment duration of six months or less (p < 0.0001) and more than twelve months (p < 0.01), compared to those treated by pediatric dentists.
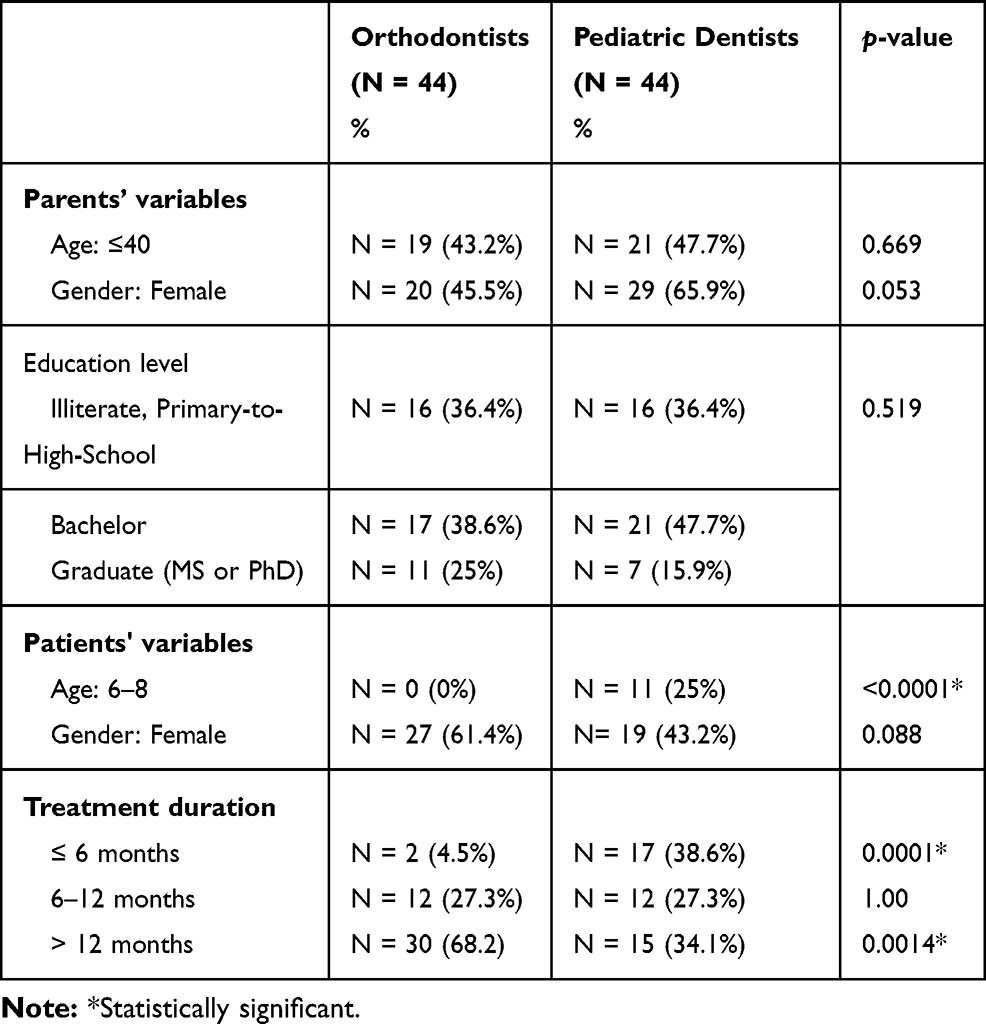 |
Table 1 Results of Chi-Square Comparing the Baseline Demographic Variables between Orthodontists’ and Pediatric Dentists’ Patients |
Parental Satisfaction
Independent t-tests were used to compare differences in the scaled mean values for overall satisfaction and the six dimensions or subscales of doctor–patient relationship, situational aspects, dentofacial improvement, psychosocial improvement, dental function, and residual category, between orthodontists and pediatric dentists. Statistically significant differences were found only in means for the subscales of doctor–patient relationship and situational aspects (p < 0.05). See Table 2.
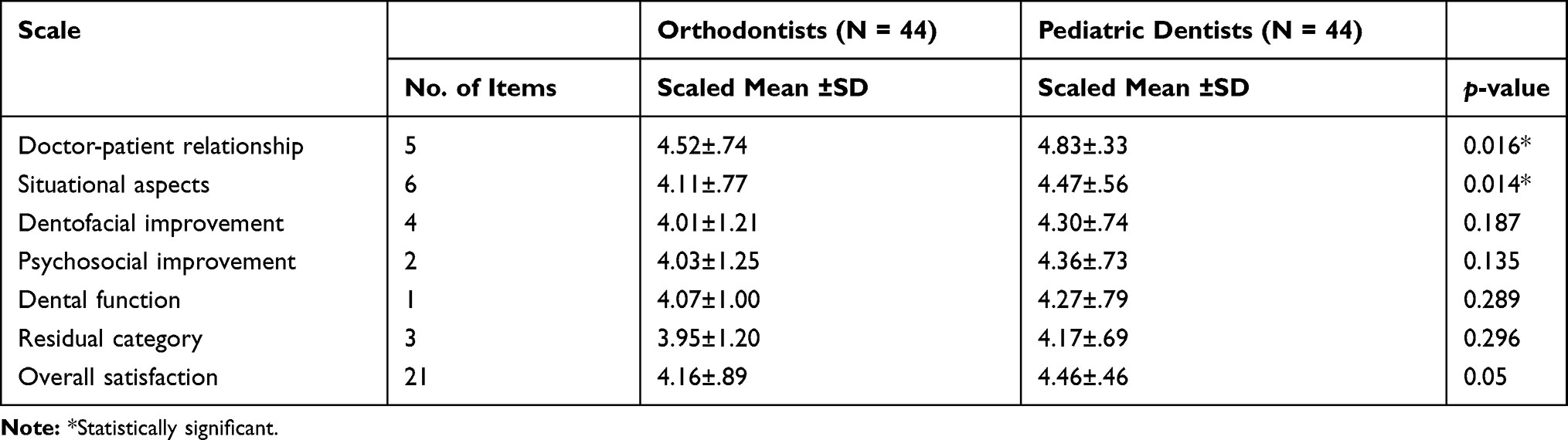 |
Table 2 Results of Independent t-tests for the Subscales and Overall Satisfaction with Orthodontic Care Provided by Orthodontists and Pediatric Dentists |
Independent t-tests were also used to compare differences in parents’ responses to individual items in the satisfaction questionnaire between orthodontists and pediatric dentists. Of the 21 items, six items were statistically significant (Table 3). These items were: 1) “I personally liked the orthodontist(s) who treated my child”, 2) “questions I had about the treatment were answered promptly”, 3) “the dentist was respectful”, 4) “the treatment took about as long as I expected it would”, 5) “the office was modern and conveniently located”, and 6) ”we were rarely kept waiting for appointments”. The means for all these six items were higher for pediatric dentists than for orthodontists (p < 0.05).
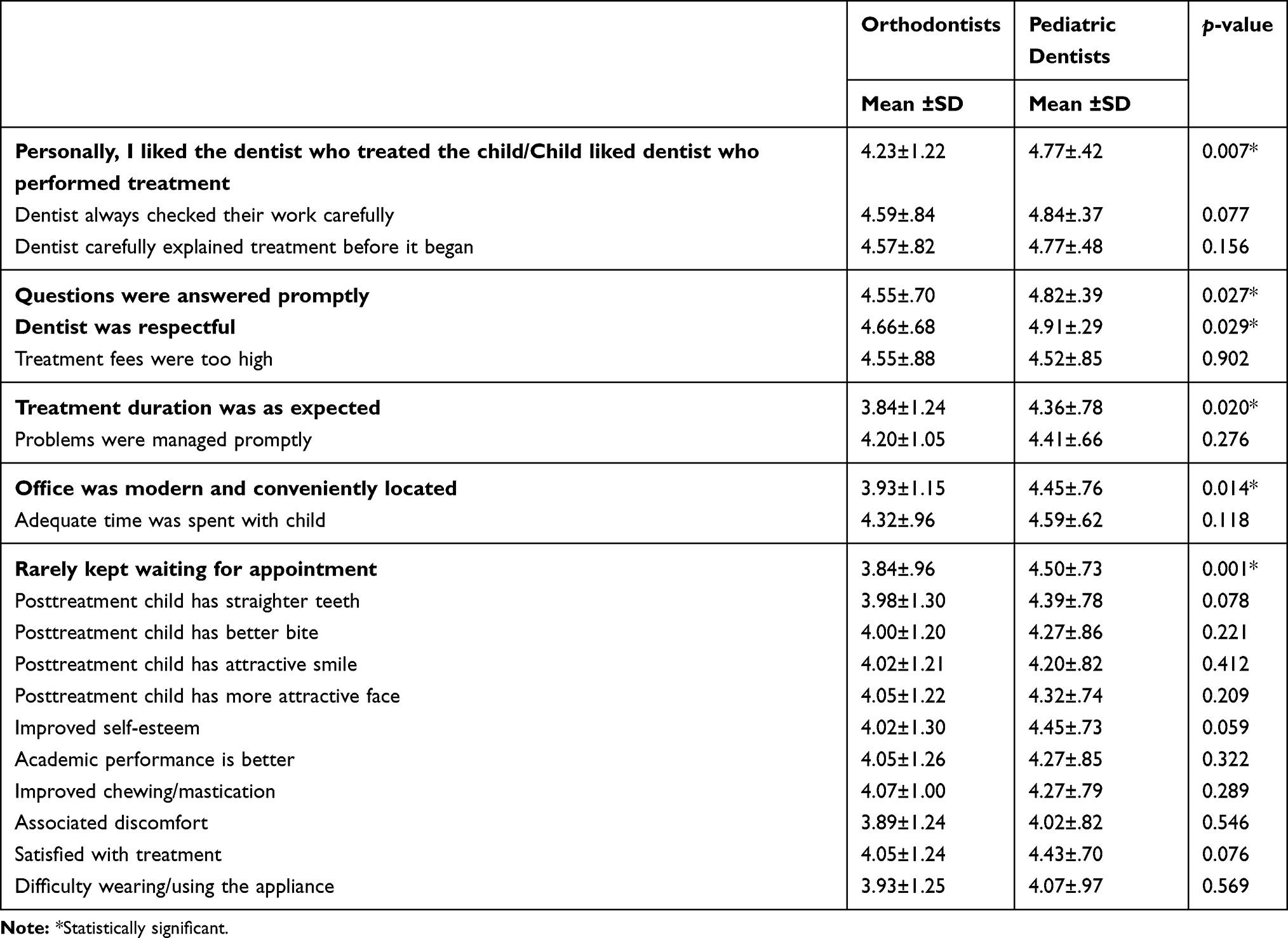 |
Table 3 Results of Independent t-tests Comparing Responses to Individual Items of the Satisfaction Questionnaire between Orthodontists and Pediatric Dentists |
Correlations
We used Spearman’s rho correlation coefficients to analyze the relationship between parental overall satisfaction and baseline demographic characteristics of patients and their parents. There were small negative and statistically significant correlations between parental overall satisfaction and their educational level (r = - 0.34, p < 0.001), as well as child gender (r = –0.29, p < 0.001).
Multivariate Regression Analyses
We used multivariate linear regression to assess the impact of care provided by orthodontists and pediatric dentists on the likelihood of parental overall satisfaction, controlling for other factors such as parents’ age, gender, and educational level, patients’ age and gender, as well as treatment duration (Table 4). After controlling for demographic factors, results indicated that there was a statistically significant difference in overall parental satisfaction with care provided by orthodontists and pediatric dentists (p < 0.05). Therefore, we reject the main research hypothesis that parental overall satisfaction is not different when care is provided by orthodontists or pediatric dentists.
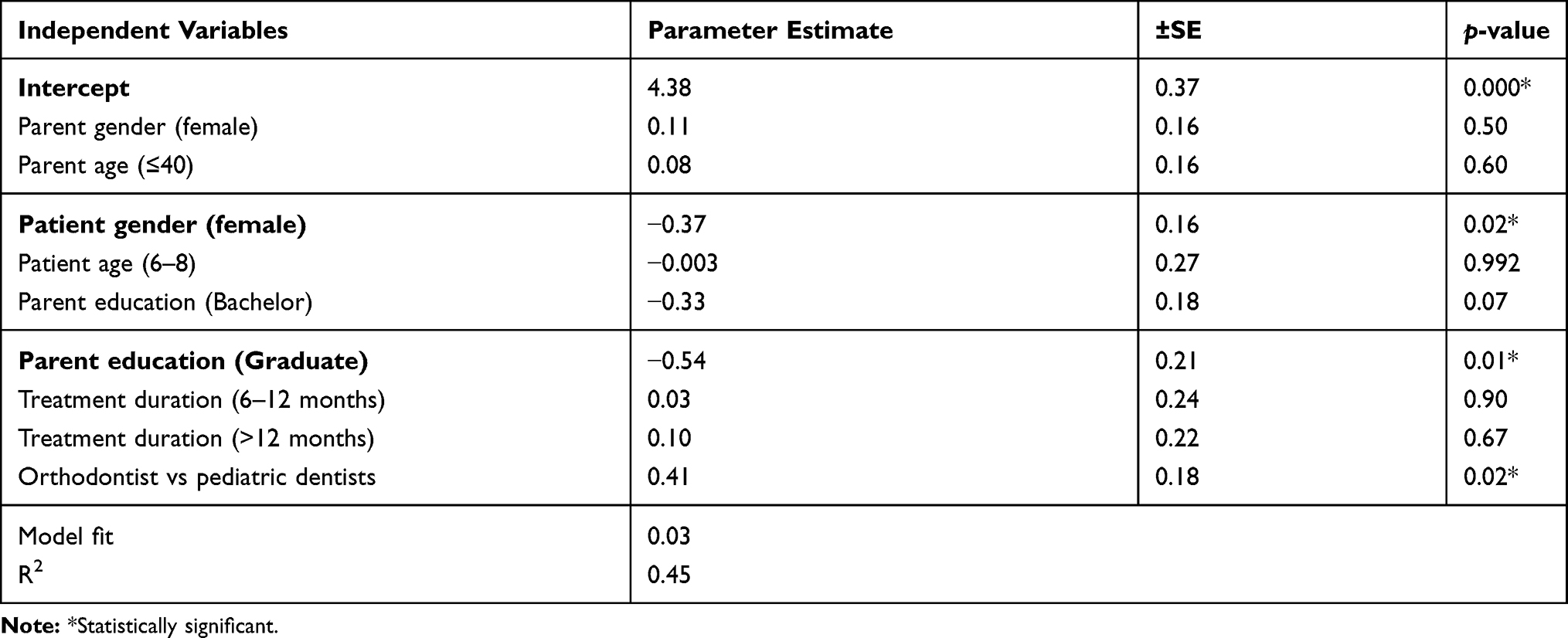 |
Table 4 Multiple Regression Model for Overall Satisfaction with Orthodontic Care between Orthodontists and Pediatric Dentists |
Multivariate linear regression models were also conducted including the six dimensions or subscales of doctor–patient relationship, situational aspects, dentofacial improvement, psychosocial improvement, dental function, and residual category as the dependent variables. Statistically significant differences were found in the dimensions of situational aspects and dental function. Regarding situational aspects, and after controlling for demographic factors, results displayed in Table 5 indicate that there was a statistically significant difference in parental satisfaction with care provided by orthodontists and pediatric dentists (p < 0.01). Regarding dental function, child gender, as a control variable, was the only significant predictor of parents’ satisfaction. Out of the total R2 = 0.221, the unique R2 contribution of child gender was 0.14 (p <0.01). The other resulting models showed no statistically significant differences in the remaining four dimensions or subscales of satisfaction with care provided by orthodontists and pediatric dentists.
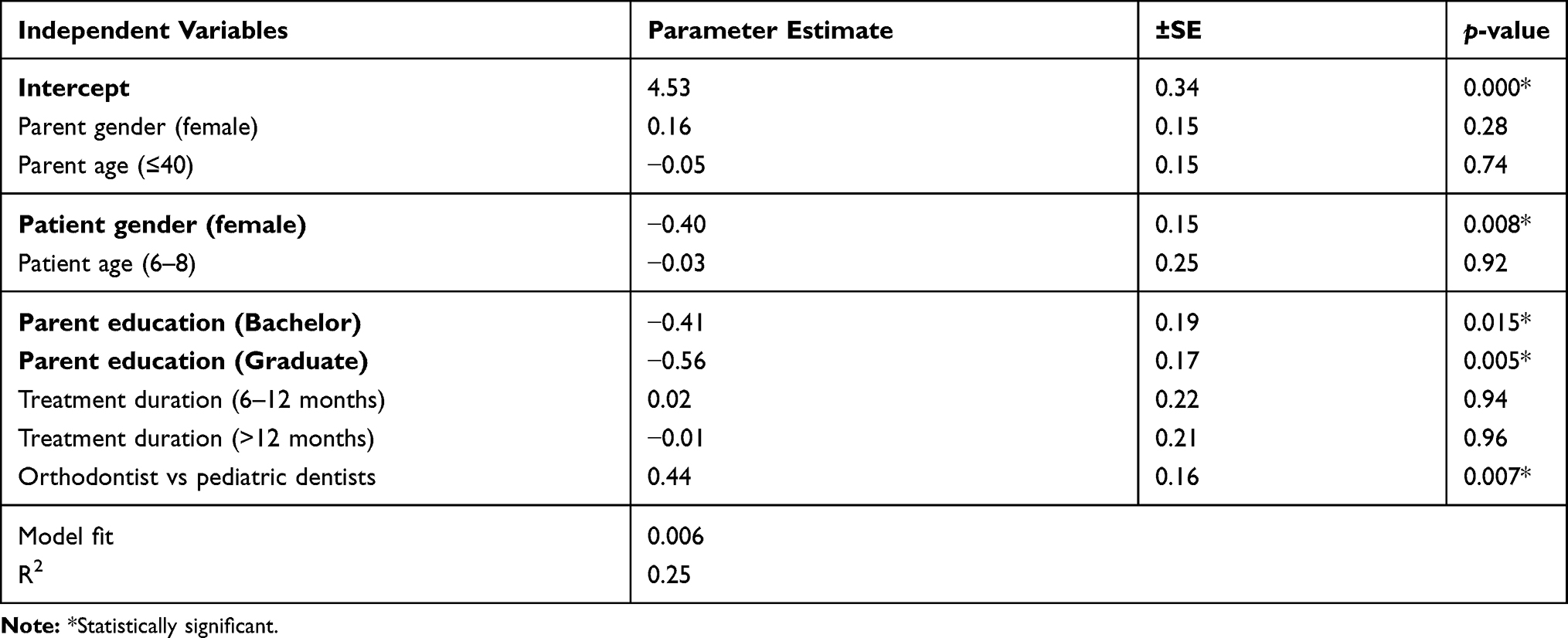 |
Table 5 Multiple Regression Model for the Dimension of Situational Aspects of Orthodontic Care between Orthodontists and Pediatric Dentists |
Discussion
We evaluated parental satisfaction with their children’s rapid palatal expansion (RPE) treatment outcome provided by orthodontists and pediatric dentists. We included patients who had their treatment completed within six months from initiating the study, since it has been shown that time period between treatment completion and satisfaction assessment could affect the perception of treatment outcome.8,37 Also, we included children who received RPE at public dental centers with fixed palatal expanders in order to minimize the effect of other confounding factors that have been shown to have a slight association with orthodontic treatment outcome satisfaction, such as patient compliance,9 appliance type,38 or type of dental center (public vs private).34 At baseline, all patients under the age of eight years were treated by pediatric dentists, which could be attributed to the fact that children at this age are still being seen by their pediatric dentists.
Addressing the primary aim of this study, and in agreement with Baheti and colleagues (2015),39 we found a statistically significant difference in overall parental satisfaction. Mascarenhas et al (2005), however, reported insignificant differences.40 It should be noted that the authors of these studies used different questionnaires and included patients who had comprehensive orthodontic treatment. Moreover, it should be noted that these are the only studies that can be compared to the current study. We also found statistically significant differences in the means for the subscales of doctor–patient relationship and situational aspects. Our findings can be explained, mainly, by pediatric dentists’ better patient relationship and behavioral management, as perceived by parents. Furthermore, parents were more satisfied with pediatric dentists because of situational aspects including office location and design, appointment waiting, and treatment duration. In other words, patients treated by orthodontists had longer treatment and their parents perceived that they were kept longer in the waiting area before their children’s visits, compared to those who have been treated by pediatric dentists. It has been shown that patients demonstrated higher levels of satisfaction with their dental treatment when they were met on time by their doctors and had short dental visits.41 In 2015, a systematic review concluded that dissatisfaction with orthodontic treatment was associated with longer treatment duration.42 Several studies have reported varying periods of time for retention after rapid palatal expansion, ranging from three to nine months.43–46 In this study, the majority of patients treated by orthodontists had their expanders for more than a year, which contributed to their parents’ lower satisfaction with the treatment outcome.
Our correlational and regression analyses showed that overall satisfaction is significantly related to, and can be predicted by, parents’ educational level, child gender, and the specialty of the dentist who provided the treatment. In other words, parents with higher levels of education, parents of female patients and parents whose children were treated by orthodontists were less satisfied with their children’s treatment. To our knowledge, no study has explored the relationship between parents’ educational level and their satisfaction with their children’s orthodontic treatment. However, Kim et al reported higher satisfaction expressed by orthodontic patients with only elementary school education compared with more educated patients.47 With regards to gender, previous authors who explored its relationship with orthodontic treatment satisfaction found no significant relationship,6–8,10,48 while others found it to be significantly related.7,36 Interestingly, and at baseline, parents’ educational level and child gender were not significantly different between orthodontists’ and pediatric dentists’ groups.
One of the limitations of this study is the subjective nature of using a questionnaire that depends on the patients’/parents’ experience and perception. Others have included an objective evaluation of the orthodontic treatment outcome,9 which may not necessarily be reflective of patient satisfaction. Also, the questionnaire we used had fewer items than the original validated questionnaire, which may have affected its sensitivity to elicit more differences. Another limitation of this study is that we did not evaluate other factors that have been strongly associated with orthodontic treatment outcome dissatisfaction, such as pain,48 retention appliances,8,9 and neuroticism.10 In the context of the current study, parental higher satisfaction with pediatric dentists does not necessarily equate to higher quality of orthodontic treatment outcome. Therefore, caution must be taken when interpreting our results. The findings of this study were based exclusively on self-reported responses of parents whose children underwent maxillary expansion to correct posterior crossbite. Thus, it should be borne in mind that our study represents a specific population group and a highly selected sample with relatively strict inclusion criteria and treatment protocol. Consequently, the results from this study can neither be generalized nor applied to other clinical contexts. In other words, we caution against generalizing our findings to all orthodontists and pediatric dentists across different clinical scenarios.
Conclusion
Overall parental satisfaction with their children’s rapid palatal expansion treatment outcome provided by orthodontists and pediatric dentists was significantly different, as parents reported higher satisfaction with pediatric dentists. This study highlights the importance of dimensions related to doctor–patient relationship and situational aspects on satisfaction with rapid palatal expansion treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu Z, McGrath C, Hägg U. The impact of malocclusion/orthodontic treatment need on the quality of life: a systematic review. Angle Orthod. 2009;79(3):585–591. doi:10.2319/042108-224.1
2. Helm S, Kreiborg S, Solow B. Psychosocial implications of malocclusion: a 15-year follow-up study in 30-year-old Danes. Am J Orthod. 1985;87(2):110–118. doi:10.1016/0002-9416(85)90020-X
3. Leao A, Sheiham A. Relation between clinical dental status and subjective impacts on daily living. J Dent Res. 1995;74(7):1408–1413. doi:10.1177/00220345950740071301
4. Slade GD, Spencer AJ. Social impact of oral conditions among older adults. Aust Dent J. 1994;39(6):358–364.
5. Bondemark L, Holm A-K, Hansen K, et al. Long-term stability of orthodontic treatment and patient satisfaction: a systematic review. Angle Orthod. 2007;77(1):181–191.
6. Keles F, Bos A. Satisfaction with orthodontic treatment. Angle Orthod. 2013;83(3):507–511.
7. Uslu O, Akcam MO. Evaluation of long-term satisfaction with orthodontic treatment for skeletal class III individuals. J Oral Sci. 2007;49(1):31–39.
8. Maia NG, Normando D, Maia FA, et al. Factors associated with long-term patient satisfaction. Angle Orthod. 2010;80(6):1155–1158.
9. Mollov ND, Lindauer SJ, Best AM, et al. Patient attitudes toward retention and perceptions of treatment success. Angle Orthod. 2010;80(4):656–661.
10. Al-Omiri MK, Abu Alhaija ES. Factors affecting patient satisfaction after orthodontic treatment. Angle Orthod. 2006;76(3):422–431. doi:10.1043/0003-3219(2006)076[0422:FAPSAO]2.0.CO;2
11. Barker MJ, Thomson WM, Poulton R. Personality traits in adolescence and satisfaction with orthodontic treatment in young adulthood. Aust Orthod J. 2005;21(2):87–93.
12. Oliveira PG, Tavares RR, Freitas JC. Assessment of motivation, expectations and satisfaction of adult patients submitted to orthodontic treatment. Dental Press J Orthod. 2013;18(2):81–87. doi:10.1590/S2176-94512013000200018
13. Bennett ME, Michaels C, O’Brien K, et al. Measuring beliefs about orthodontic treatment: a questionnaire approach. J Public Health Dent. 1997;57(4):215–223. doi:10.1111/j.1752-7325.1997.tb02978.x
14. Lippold C, Stamm T, Meyer U, et al. Early treatment of posterior crossbite-a randomised clinical trial. Trials. 2013;14(1):20. doi:10.1186/1745-6215-14-20
15. Tulloch JC, Phillips C, Koch G, et al. The effect of early intervention on skeletal pattern in Class II malocclusion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 1997;111(4):391–400. doi:10.1016/S0889-5406(97)80021-2
16. Silkestrand S. Interceptive orthodontic care in Uppsala County. A retrospective study on frequency of interceptive treatment, treatment approaches and treatment providers. Stockholm; 2007.
17. Seehra J, Newton J, DiBiase AT. Interceptive orthodontic treatment in bullied adolescents and its impact on self-esteem and oral-health-related quality of life. Eur J Orthod. 2013;35(5):615–621. doi:10.1093/ejo/cjs051
18. Keski-Nisula K, Hernesniemi R, Heiskanen M, et al. Orthodontic intervention in the early mixed dentition: a prospective, controlled study on the effects of the eruption guidance appliance. Am J Orthod Dentofacial Orthop. 2008;133(2):254–260. doi:10.1016/j.ajodo.2006.05.039
19. Karaiskos N, Wiltshire WA, Odlum O, et al. Preventive and interceptive orthodontic treatment needs of an inner-city group of 6- and 9-year-old Canadian children. J Can Dent Assoc. 2005;71(9).
20. Gianelly AA. Treatment of crowding in the mixed dentition. Am J Orthod Dentofacial Orthop. 2002;121(6):569–571. doi:10.1067/mod.2002.124172
21. Singh VP, Sharma A. Epidemiology of malocclusion and assessment of orthodontic treatment need for Nepalese children. Int Sch Res Notices. 2014;2014:1–4. doi:10.1155/2014/768357
22. Ngom PI, Diagne F, Dieye F, et al. Orthodontic treatment need and demand in Senegalese school children aged 12–13 years: an appraisal using IOTN and ICON. Angle Orthod. 2007;77(2):323–330. doi:10.2319/0003-3219(2007)077[0323:OTNADI]2.0.CO;2
23. Souames M, Bassigny F, Zenati N, et al. Orthodontic treatment need in French schoolchildren: an epidemiological study using the index of orthodontic treatment need. Eur J Orthod. 2006;28(6):605–609. doi:10.1093/ejo/cjl045
24. Nobile CG, Pavia M, Fortunato L, et al. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637–641. doi:10.1093/eurpub/ckm016
25. Tausche E. Prevalence of malocclusions in the early mixed dentition and orthodontic treatment need. Eur J Orthod. 2004;26(3):237–244. doi:10.1093/ejo/26.3.237
26. Al-Emran S, Wisth PJ, Böe OE. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18(5):253–255. doi:10.1111/j.1600-0528.1990.tb00070.x
27. Gudipaneni RK, Aldahmeshi RF, Patil SR, et al. The prevalence of malocclusion and the need for orthodontic treatment among adolescents in the northern border region of Saudi Arabia: an epidemiological study. BMC Oral Health. 2018;18(1):16. doi:10.1186/s12903-018-0476-8
28. Haralur SB, Addas MK, Othman HI, et al. Prevalence of malocclusion, its association with occlusal interferences and temporomandibular disorders among the Saudi sub-population. Oral Health Dent Manag. 2014;13(2):164–169.
29. Yang EY, Kiyak HA. Orthodontic treatment timing: a survey of orthodontists. Am J Orthod Dentofacial Orthop. 1998;113(1):96–103. doi:10.1016/S0889-5406(98)70281-1
30. Pietilä I, Pietilä T, Pirttiniemi P, et al. Orthodontists‘ views on indications for and timing of orthodontic treatment in Finnish public oral health care. Eur J Orthod. 2007;30(1):46–51. doi:10.1093/ejo/cjm085
31. Koroluk LD, Jones J, Avery D. Analysis of orthodontic treatment by pediatric dentists and general practitioners in Indiana. ASDC J Dent Child. 1988;55(2):97–101.
32. Hilgers KK, Redford-Badwal D, Reisine S. Orthodontic treatment provided by pediatric dentists. Am J Orthod Dentofacial Orthop. 2003;124(5):551–560. doi:10.1016/S0889-5406(03)00622-X
33. Aldrees AM, Tashkandi NE, AlWanis AA, et al. Orthodontic treatment and referral patterns: a survey of pediatric dentists, general practitioners, and orthodontists. Saudi Dent J. 2015;27(1):30–39.
34. Al Shahrani I, Tikare S, Togoo RA, et al. Patient s satisfaction with orthodontic treatment at King Khalid University, College of Dentistry, Saudi Arabia. Bangladesh J Medical Sci. 2015;14(2):146–150.
35. Aljughaiman A, Alshammari A, Althumairi A, et al. Patient satisfaction with orthodontic treatment received in public and private hospitals in Dammam, Saudi Arabia. Open Access Maced J Med Sci. 2018;6(8):1492.
36. Bos A, Vosselman N, Hoogstraten J, et al. Patient compliance: a determinant of patient satisfaction? Angle Orthod. 2005;75(4):526–531.
37. Birkeland K, Bøe OE, Wisth PJ. Relationship between occlusion and satisfaction with dental appearance in orthodontically treated and untreated groups. A longitudinal study. Eur J Orthod. 2000;22(5):509–518.
38. Bergström K, Halling A, Wilde B. Orthodontic care from the patients’ perspective: perceptions of 27-year-olds. Eur J Orthod. 1998;20(3):319–329.
39. Baheti K, Raghav S, Kanungo H, et al. A comparison of parental satisfaction in the quality of their child’s orthodontic treatment by orthodontists and pedodontists. J Int Oral Health. 2015;7(1):26.
40. Mascarenhas AK, Vig K, Joo B-H. Parents’ satisfaction with their child’s orthodontic care: a comparison of orthodontists and pediatric dentists. Pediatr Dent. 2005;27(6):451–456.
41. Chang W-J, Chang Y-H. Patient satisfaction analysis: identifying key drivers and enhancing service quality of dental care. J Dent Sci. 2013;8(3):239–247.
42. Pachêco-Pereira C, Pereira JR, Dick BD, et al. Factors associated with patient and parent satisfaction after orthodontic treatment: a systematic review. Am J Orthod Dentofacial Orthop. 2015;148(4):652–659.
43. Cross DL, McDonald JP. Effect of rapid maxillary expansion on skeletal, dental, and nasal structures: a postero-anterior cephalometric study. Eur J Orthod. 2000;22(5):519–528.
44. Lima Filho RM, de Oliveira Ruellas AC. Long-term maxillary changes in patients with skeletal Class II malocclusion treated with slow and rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2008;134(3):383–388.
45. Cozza P, Giancotti A, Petrosino A. Rapid palatal expansion in mixed dentition using a modified expander: a cephalometric investigation. J Orthod. 2001;28(2):129–134.
46. Huynh T, Kennedy DB, Joondeph DR, et al. Treatment response and stability of slow maxillary expansion using Haas, hyrax, and quad-helix appliances: a retrospective study. Am J Orthod Dentofacial Orthop. 2009;136(3):331–339.
47. Kim JS, Yoo MS, Ju OJ. Satisfaction with dental care in orthodontic patients. J Dent Hyg Sci. 2006;6(3):207–212.
48. Feldmann I. Satisfaction with orthodontic treatment outcome. Angle Orthodontist. 2014;84(4):581–587.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.