")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 9
Parental attitudes about acquiring a dental home for preschool children: a new concept in the Arab state of Qatar
Authors Hendaus MA, Leghrouz B, Allabwani R, Zainel A, AlHajjaji M, Siddiqui F, Alamri M, Alhammadi AH
Received 2 June 2018
Accepted for publication 21 August 2018
Published 17 October 2018 Volume 2018:9 Pages 123—128
DOI https://doi.org/10.2147/PHMT.S176114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Roosy Aulakh
Mohamed A Hendaus,1–3 Bassil Leghrouz,4 Ruba Allabwani,4 Abdelwahed Zainel,4 Mohamed AlHajjaji,4 Faisal Siddiqui,4 Mohammed Alamri,2 Ahmed H Alhammadi1–3
1Department of Pediatrics, Section of Academic General Pediatrics, Sidra Medicine, Doha, Qatar; 2Department of Pediatrics, Hamad General Corporation, Doha, Qatar; 3Department of Clinical Pediatrics, Weill Cornell Medicine, Doha, Qatar; 4Pediatric Residency Program, Hamad General Corporation, Doha, Qatar
Objective: The purpose of the study was to assess parental perceptions and acceptability of a dental home for their preschool children, a new concept in the state of Qatar.
Methods: A cross-sectional prospective study was conducted at Hamad Medical Corporation, in the state of Qatar. Parents of infants and children <5 years of age were offered an interview survey.
Results: A total of 309 questionnaires were completed (response rate =98%). More than 90% of the participants believed that oral health and dentition affected total-body well-being. Only 18% of parents stated that their children had excellent oral health. Interestingly, more than two-thirds of children had not had a routine dentist visit in the 12 months preceding the interview. Reasons for not having such visits included long appointment times (17.4%), the perception that dental care was expensive (15.5%), the notion that deciduous teeth did not need care (9%), the impression that insurance did not cover dental procedures (8%), unawareness of location of dental centers (4%), the child did not want to go (4%), the notion that children are difficult to handle during a dental procedure (3%), a combination of these factors (33.5%), and other factors (5%). When asked what factors would encourage them to enrol a dental home for their children, almost 20% mentioned speedy appointments followed by dentists specialized in pediatrics (14.3%), child-friendly atmosphere (12%), low cost (12%), close to home (5.7%), none (2.7%), others (2%), and all of the above (32.3%).
Conclusion: Counseling by primary-care physicians can increase dental home acceptability in the state of Qatar, especially that access to health care is easy in our community.
Keywords: dental home, oral health, Qatar
Introduction
Oral health is crucial to well-being and quality of life. The World Health Organization defines oral health as a “. . . a state of being free from mouth and facial pain, oral and throat cancer, oral infection and sores, periodontal (gum) disease, tooth decay, tooth loss, and other diseases and disorders that limit an individual’s capacity in biting, chewing, smiling, speaking, and psychosocial wellbeing [sic]”.1
Oral diseases, such as periodontal disease, oral mucosal lesions, and caries, are considered as major childhood public health issues.2 These conditions can be avoided with early preventive oral health interventions, but unfortunately the literature has suggested that children do not receive regular dental care, due to different perceived barriers.3,4 Moreover, sometimes management of these conditions is usually delayed until the problem is worse, requiring a visit to the emergency department.3
Poor oral health in preschoolers can lead to pain,5 may disturb their growth and quality of life,6,7 and is a robust prognosticator of future dental problems.8–10 A study conducted in the state of Qatar showed that approximately 85% of children 12–14 years of age had dental caries.11 The founding of a dental home may pursue the medical home as an effective preventive and cost-effective model to prevent oral health diseases.12 A dental home is analogous to a medical home, where the child receives preventive care and treatment.13 The American Academy of Pediatric Dentistry advocates that a dental home provide comprehensive, unceasingly accessible, family-centered, compassionate, culturally sensitive, and efficient care for children. This care comprises assessment of oral diseases, management of acute and chronic oral issues, and anticipatory guidance regarding development and growth.14 Referral by the health provider has been advocated as early as 6 months of age and not exceeding 1 year of age.15–17
In 2016, a study was conducted to delineate the prevalence of early childhood caries and enamel defects in 4- and 5-year old Qatari preschool children. The study showed that the prevalence of caries in this age group was 89.2%.18 The state of Qatar is a wealthy, rapidly developing nation with excellent access to medical and dental care.19 It was noticed that changes have occurred in the choice of drinks consumed and their role in the diet.20 The literature has shown that nowadays, milk intake has decreased and consumption of juice and sodas has increased.21
The ramifications of this change in dietary habits may have decreased the intake of calcium and increased rates of childhood obesity and dental caries.20–22 The objectives of this study were to assess parental perceptions and acceptability of a dental home for their children (aged <5 years) and to delineate factors that are influencing the underutilization of dental health care.
Methods
Study design, period, setting, and participants
This study was cross-sectional. The study was approved by the institutional review board and the Hamad Medical Corporation Hospital Committee (17016/17). A questionnaire adopted from several sources23–27 was validated by experts in our organization. It was composed of 24 items that address parent and child demographics, as well as questions related to parental knowledge of oral health and their attitudes and preferences in building a dental home for their children. We chose a convenience sample of 300 participants. There have been no similar studies to extrapolate or calculate the sample needed.
Parents were approached during their visits to our outpatient and inpatient departments. We excluded parents of children with such conditions as developmental delay, musculoskeletal disability, and respiratory compromise, as their needs in a dental home could be very challenging. Verbal consent was taken after explaining the objectives of the study, and participants were informed of why the information was being collected and how it would be used for effective patient-care management. Parents were informed that their participation was voluntary and that their answers were confidential and anonymous. Families did not receive any type of compensation for participating in the study. We also informed them that the project had received approval from Hamad Medical Corporation Ethics Committee. Some of the families preferred face-to-face interview, while others opted to complete the questionnaire by themselves.
Statistical analysis
Qualitative and quantitative data are expressed as percentages. Descriptive statistics were used to summarize demographics and all other characteristics of the participants. Associations between two or more qualitative or categorical variables were assessed using c2 tests. For low frequencies, c2 with continuity-correction factor or Fisher’s exact test was applied. A two-sided P-value <0.05 was statistically significant. Some data were missed, since the study was survey-based. Missed data were not accounted for in the analysis. All statistical analyses were done using SPSS version 21.0 (IBM, Armonk, NY, USA).
Results
A total of 309 questionnaires were completed (response rate 98%). Approximately 85% (n=257) of participating parents were 20–39 years of age, and 70% (n=212) were females. Table 1 summarizes the demographic characteristics of participants.
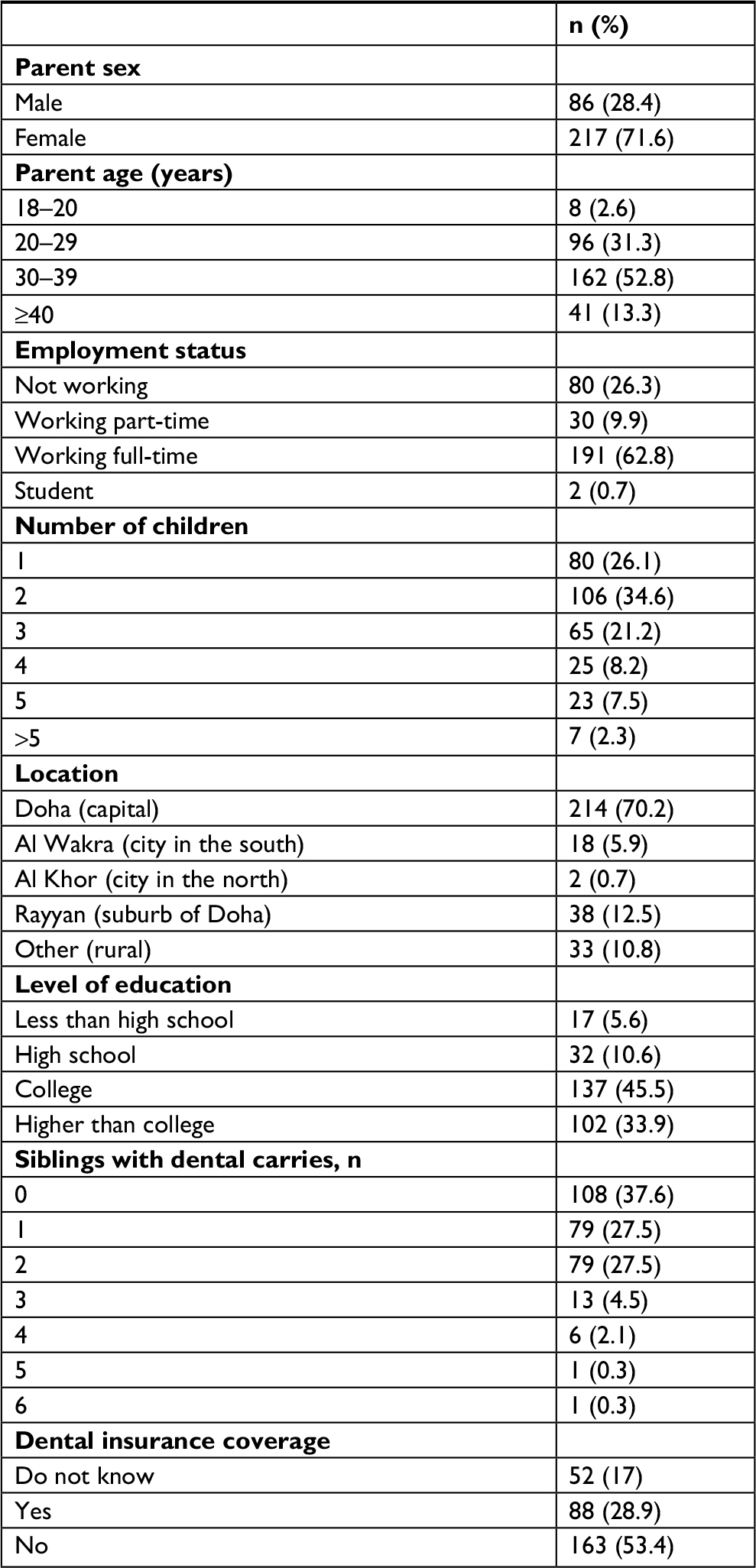 | Table 1 Demographic characteristics of participants |
When assessing parental knowledge and awareness of dental health, >90% (n=272) of participants believed that oral health and dentition affected total-body well-being. Approximately a fifth (n=54) stated that their children had excellent oral health. Parents were eventually asked to describe the dental issues their children possessed, and almost a third mentioned multiple problems (pain, cavities, halitosis, broken teeth, and tooth discoloration), while 20% (n=60) complained solely of cavities. Table 2 summarizes parental knowledge and awareness of dental health.
 | Table 2 Knowledge and awareness of dental health |
In terms of brushing intervals, our study showed that 47% (n=146) of children brushed twice a day. Of those who brushed their teeth, almost 20% supplemented brushing with dental floss or mouthwash. We inquired about parental supervision of brushing teeth, and found that 86% (n=267) of participants advised and monitored, 7% (n=21) advised but did not monitor, and the rest did not care. Interestingly, more than two thirds of children had not had a routine dentist visit in the 12 months preceding the interview. The reasons for not having had such visits are summarized in Table 3.
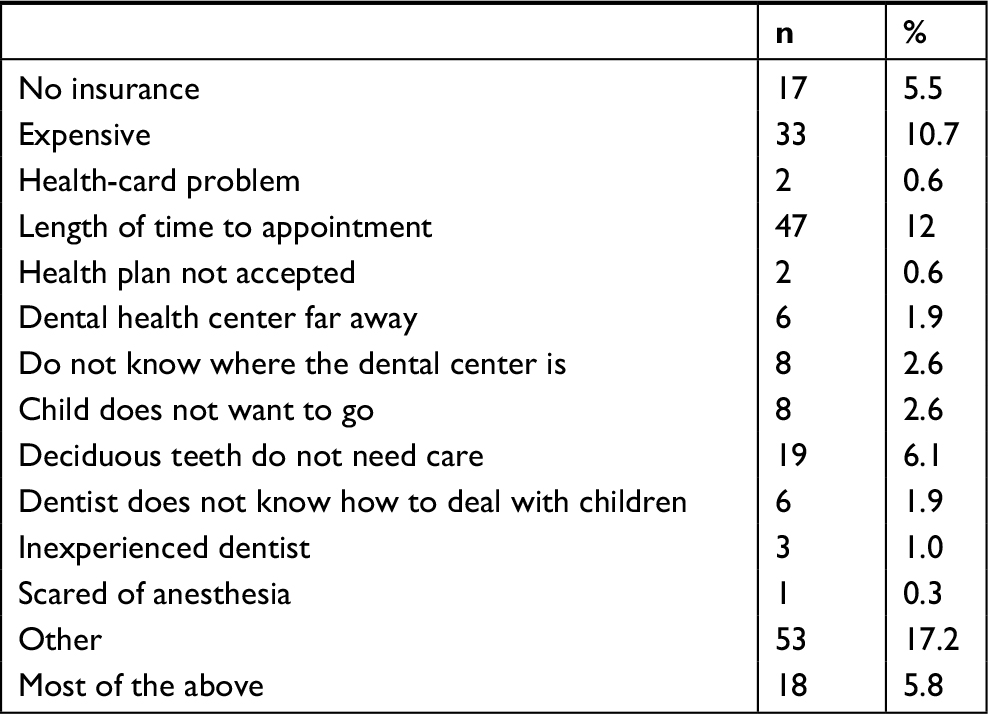 | Table 3 The reasons for not having visited a dentist |
Parents were asked about factors that would encourage them to enrol a dental home for their children, and answered speedy appointments (n=57, 18.4%), child-friendly atmosphere (n=37, 11.7%), dentists specialized in pediatrics (n=43, 13.9%), low cost (n=36, 11.7%), close to home (n=17, 5.5%), others (n=6, 1.9%), and none (n=8, 2.6%). It is worth mentioning that >70% (n=212) of parents believed that the primary pediatrician of the child should start the dental home process. Finally, the level of education and age-group of parents did not influence the idea of creating a dental home for their children (P=0.6 and P=0.585, respectively).
Discussion
Our study provides important new literature related to oral health in preschool children. To our knowledge, this paper is the first in the state of Qatar and in our geographical region to deal with the concept of acquiring a dental home for preschool children.
The findings of the present study show that a substantial number of families perceive oral health issues in their children. The high rate of this perception may reflect a lack of community awareness and perception that prevention and management of caries should begin in preschoolers. In addition, there was parental indifference related to the perception that deciduous teeth are replaceable by permanent teeth.
Early interference with preventive measures might be crucial in preventing dental caries in preschool children. Embedding oral health screening in a well-child visit could be performed routinely.28 The American Academy of Pediatrics recommends performing the first dental risk assessment at 6 months of age and to establish a dental home by 1 year of age for children considered to be at risk for dental caries.29
Poor oral hygiene affects more than just the mouth: it can seriously compromise a child’s general health and quality of life, leading sometimes to failure to thrive and interrupted school attendance.30,31 The ramifications of poor oral health, however, go far beyond medical diseases. Oral disease can also have an economic impact by driving up health-care costs in general.32 Studies have shown that early prevention or intervention can significantly reduce the cost of dental care, especially for families at or below the poverty level.33,34
In addition, those costs may dramatically increase with delaying the first visit to 5 years of age. Although most of our participant parents were aware of the effect of dental health on total-body well-being, over a third did not provide their children with routine dentist visits. The two main reasons behind this omission were related to either delayed dental service or underestimation of the importance of deciduous teeth care. Those barriers can be overcome, especially given the fact that the health system in Qatar provides services to all children residing in its territories.
One of our major results showed that more than two-thirds of children had not had a routine dentist visit in the 12 months preceding the interview. This is an astonishingly high rate in a country where medical and dental resources are generous. The state of Qatar’s health system was ranked 13th best in the world and first in the Middle East in the 2017 Legatum Prosperity Index.35
There is a deficiency in the literature available regarding parental knowledge concerning the oral health of their children. Most of the data have been on school-age children, due to easy approachability, which is difficult in preschool children.36 Chhabra and Chhabra37 studied parental knowledge, attitudes, and cultural beliefs regarding oral health and dental care of preschool children in an Indian population. The study of parents of 620 preschool children showed that deficiency in awareness and knowledge of deciduous teeth and parental fear contributed negatively to their children’s dental care. Moreover, oral health practices were revealed to be at low rates.
Gussy et al38 examined the oral health-related attitudes and knowledge of parents of children aged 12–24 months living in rural areas of Victoria, Australia. The study included 272 parents of preschool children, and showed that a large proportion of participants showed deficiency in confidence in oral health. Moreover, the majority of parents acknowledged that toothpaste can decrease the risk of dental caries, but did not know that it could be used for preschoolers.
Anticipatory guidance is the mechanism of implementing practical, developmentally suitable information about children’s health to inform parents on significant physical and emotional milestones.15 The use of anticipatory guidance in the framework of well-child medical visits during a child’s early years has been shown to diminish the number of hospitalizations, irrespective of race and health status.39 Insight and awareness are essential requirements for changes in attitude, including behaviors related to oral health.40
Pediatricians can play a crucial role in dental health by increasing their involvement in oral health care during well-child visits, especially for children who have difficulty obtaining access to professional dental care.41 This involvement includes counseling on caries prevention, assessment and referral for dental problems, and provision of caries-control treatment, such as application of fluoride varnish, which has been shown to reduce dental decay by 38% if used twice yearly.42 Unfortunately, pediatricians receive very little education on oral health during medical school and residency training and numerous barriers exist, preventing oral health in daily practice.43
This study has considerable strengths, specifically both the quantitative and qualitative feedback. Our study will assist in illustrating the need for dental homes for preschoolers. This study also has limitations. We used a convenience sample. The limitations to external validity are for the most part due to a very new concept. Moreover, there might be a chance that there are specific characteristics related to parental preference in this subject that were not evaluated in this study. Some of the parents opted to have an interview, rather than completing a survey. Despite the fact that there was no coercion or interference from the research team, we consider collecting data by two different methods a limitation. Part of our sample was collected from parents whose children were being followed in the outpatient department, which included parents who provided a higher level of care to their children with regular well-child visits. The sample also included parents of children with medical comorbidities, which could be perceived as more important than oral health. In addition, parental estimation of children’s dental problems may not reflect reality, since children may have oral health issues not identified by parents.
Conclusion
Counseling by primary-care physicians can increase dental-home acceptability in the state of Qatar, especially given the fact that access to health care is easy in our community.
Ethical approval
The Hamad Medical Corporation Ethics Committee approved this study (17016/17).
Acknowledgments
The authors would like to thank the Medical Research Center of Hamad Medical Corporation for its support and ethical approval. This study was presented at the American Academy of Pediatrics National Conference and Exhibition, held in Chicago, IL, USA, on September 16, 2017; and an abstract of the presentation has been published.44
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Oral Health. Available from: http://www.who.int/oral_health/en. Accessed August 15, 2018. | ||
Petersen PE. World Health Organization global policy for improvement of oral health-World Health Assembly 2007. Int Dent J. 2008;58(3):115–121. | ||
Nalliah RP, Allareddy V, Elangovan S, Karimbux N, Allareddy V. Hospital based emergency department visits attributed to dental caries in the United States in 2006. J Evid Based Dent Pract. 2010;10(4):212–222. | ||
Elangovan S, Nalliah R, Allareddy V, Karimbux NY, Allareddy V. Outcomes in patients visiting hospital emergency departments in the United States because of periodontal conditions. J Periodontol. 2011;82(6):809–819. | ||
Slade GD. Epidemiology of dental pain and dental caries among children and adolescents. Community Dent Health. 2001;18(4):219–227. | ||
Anderson HK, Drummond BK, Thomson WM. Changes in aspects of children’s oral-health-related quality of life following dental treatment under general anaesthesia. Int J Paediatr Dent. 2004;14(5):317–325. | ||
Thomas CW, Primosch RE. Changes in incremental weight and well-being of children with rampant caries following complete dental rehabilitation. Pediatr Dent. 2002;24(2):109–113. | ||
Heller KE, Eklund SA, Pittman J, Ismail AA. Associations between dental treatment in the primary and permanent dentitions using insurance claims data. Pediatr Dent. 2000;22(6):469–474. | ||
Haugejorden O, Birkeland JM. Evidence for reversal of the caries decline among Norwegian children. Int J Paediatr Dent. 2002;12(5):306–315. | ||
Skeie MS, Raadal M, Strand GV, Espelid I. The relationship between caries in the primary dentition at 5 years of age and permanent dentition at 10 years of age – a longitudinal study. Int J Paediatr Dent. 2006;16(3):152–160. | ||
Al-Darwish M, El Ansari W, Bener A. Prevalence of dental caries among 12–14 year old children in Qatar. Saudi Dent J. 2014;26(3):115–125. | ||
Allareddy V, Nalliah RP, Haque M, Johnson H, Rampa SB, Lee MK. Hospital-based emergency department visits with dental conditions among children in the United States: nationwide epidemiological data. Pediatr Dent. 2014;36(5):393–399. | ||
Mcgrath C, Bedi R, Dhawan N. Factors influencing older people’s self reported use of dental services in the UK. Gerodontology. 1999;16(2):97–102. | ||
The American Academy of Pediatric Dentistry (AAPD). Policy on the dental home. Reference Manual V 37/NO 6 15/16. Available from: http://www.aapd.org/media/policies_guidelines/p_dentalhome.pdf. Accessed March 27, 2018. | ||
Nowak AJ, Casamassimo PS. The dental home: a primary care oral health concept. J Am Dent Assoc. 2002;133(1):93–98. | ||
Casamassimo P, Holt K. Bright Futures in Practice: Oral Health. Pocket Guide, 2nd ed. Washington, DC: National Maternal and Child Oral Health Resource Center; 2014. | ||
American Academy of Pediatrics Section on Pediatric Dentistry. Oral health risk assessment timing and establishment of the dental home. Pediatrics. 2003;111(5):1113–1116. | ||
Alkhtib A, Ghanim A, Temple-Smith M, Messer LB, Pirotta M, Morgan M. Prevalence of early childhood caries and enamel defects in four and five-year old Qatari preschool children. BMC Oral Health. 2016;16(1):73. | ||
Al-Thani MH, Al-Thani AA, Al-Emadi AA, Al-Chetachi WF, Akram H, Poovelil BV. Oral health status of six-year-old children in Qatar: findings from the national oral health survey. Int J Dent Hyg. 2018;16(2):225–232. | ||
Bener A, Al Darwish MS, Tewfik I, Hoffmann GF. The impact of dietary and lifestyle factors on the risk of dental caries among young children in Qatar. J Egypt Public Health Assoc. 2013;88(2):67–73. | ||
Marshall TA, Broffitt B, Eichenberger-Gilmore J, Warren JJ, Cunningham MA, Levy SM. The roles of meal, snack, and daily total food and beverage exposures on caries experience in young children. J Public Health Dent. 2005;65(3):166–173. | ||
Tewfik I. Childhood Obesity Prevention (CHOP) programme: a conceptual framework for nutrition intervention. Int J Food Safety Nutr Public Health. 2008;1:16–32. | ||
Hendaus M, Jamha H, Siddiqui F, Elsiddig S, Alhammadi A. Parental preference for fluoride varnish a new concept in a rapidly developing nation. 2016;10(2147):1227–1233. | ||
Kenney MK, Kogan MD, Crall JJ. Parental perceptions of dental/oral health among children with and without special health care needs. Ambul Pediatr. 2008;8(5):312–320. | ||
Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70(2):179–187. | ||
Ortiz FR, Santos MD, Landenberger T, Emmanuelli B, Agostini BA, Ardenghi TM. Comparison of Face-To-Face Interview and Telephone Methods of Administration on the Ecohis Scores. Braz Dent J. 2016;27(5):613–618. | ||
Rajalingam S, Rani VL. A descriptive study on awareness about oral health among pediatric practitioners in Kanchipuram district. J Pharm Bioallied Sci. 2016;8(Suppl 1):S144–S146. | ||
Phelan C. The Blue Book oral health program: a collaborative partnership with statewide implications. Health Promot J Austr. 2006;17(2):109–113. | ||
Hale KJ, American Academy of Pediatrics Section on Pediatric Dentistry. Oral health risk assessment timing and establishment of the dental home. Pediatrics. 2003;111(5 Pt 1):1113–1116. | ||
Acs G, Lodolini G, Kaminsky S, Cisneros GJ. Effect of nursing caries on body weight in a pediatric population. Pediatr Dent. 1992;14(5):302–305. | ||
Gift HC, Reisine ST, Larach DC. The social impact of dental problems and visits. Am J Public Health. 1992;82(12):1663–1668. | ||
Texas Dental Association. Building better oral health: a dental home for all Texans. Tex Dent J. 2008;Suppl 1:1–56. | ||
Sheller B, Williams BJ, Lombardi SM. Diagnosis and treatment of dental caries-related emergencies in a children’s hospital. Pediatr Dent. 1997;19(8):470–475. | ||
Kanellis MJ, Damiano PC, Momany ET. Medicaid costs associated with the hospitalization of young children for restorative dental treatment under general anesthesia. J Public Health Dent. 2000;60(1):28–32. | ||
Qatar’s Health System. Hukoomi. Available from: http://portal.www.gov.qa/wps/portal/media-center/news/news-details/qatarshealthsystemrankedthirteenthworldwidefirstinme. Accessed March 27, 2018. | ||
Holm AK. Education and diet in the prevention of caries in the preschool child. J Dent. 1990;18(6):308–314. | ||
Chhabra N, Chhabra A. Parental knowledge, attitudes and cultural beliefs regarding oral health and dental care of preschool children in an Indian population: a quantitative study. Eur Arch Paediatr Dent. 2012;13(2):76–82. | ||
Gussy MG, Waters EB, Riggs EM, Lo SK, Kilpatrick NM. Parental knowledge, beliefs and behaviours for oral health of toddlers residing in rural Victoria. Aust Dent J. 2008;53(1):52–60. | ||
Hakim RB, Bye BV. Effectiveness of compliance with pediatric preventive care guidelines among Medicaid beneficiaries. Pediatrics. 2001;108(1):90–97. | ||
Green W, Kreuter M. Health promotion planning: an educational and ecological approach. 3rd ed. Mountain View, CA: Mayfield Pub. Co.; 1999. | ||
Lewis CW, Grossman DC, Domoto PK, Deyo RA. The role of the pediatrician in the oral health of children: A national survey. Pediatrics. 2000;106(6):E84. | ||
Helfenstein U, Steiner M. Fluoride varnishes (Duraphat): A meta-analysis. Community Dent Oral Epidemiol. 1994;22(1):1–5. | ||
Krol DM. Children’s oral health and the role of the pediatrician. Curr Opin Pediatr. 2010;22(6):804–808. | ||
Siddiqui F, Hendaus MA, Leghrouz B, et al. Parental Attitude in Acquiring a Dental Home for Young Children: A New Concept in Arab State of Qatar. Pediatrics. 2018;142(1):MeetingAbstract. Available from: http://pediatrics.aappublications.org/content/142/1_MeetingAbstract/430. Accessed October 2, 2018. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.