")
Back to Journals » Journal of Pain Research » Volume 12
Parameters associated with efficacy of epidural steroid injections in the management of postherpetic neuralgia: the Mayo Clinic experience
Authors Ghanavatian S, Wie CS, Low RS , Butterfield RJ , Zhang N, Dhaliwal GS , Montoya JM, Swanson DL
Received 12 October 2018
Accepted for publication 18 February 2019
Published 23 April 2019 Volume 2019:12 Pages 1279—1286
DOI https://doi.org/10.2147/JPR.S190646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Shirin Ghanavatian,1 Christopher S Wie,2 Rhonda S Low,3 Richard J Butterfield,4 Nan Zhang,4 Gurman Singh Dhaliwal,5 Jordan M Montoya,6 David L Swanson1
1Department of Dermatology, Mayo Clinic, Scottsdale, AZ, USA; 2Department of Anesthesiology and Perioperative Medicine, Mayo Clinic Hospital, Phoenix, AZ, USA; 3Division of Preventive, Occupational, and Aerospace Medicine, Mayo Clinic, Scottsdale, AZ, USA; 4Biostatistics, Mayo Clinic, Scottsdale, AZ, USA; 5University of Arizona College of Medicine-Phoenix, Phoenix, AZ, USA; 6Mayo Clinic School of Medicine, Scottsdale, AZ, USA
Purpose: Thirty percent of patients with postherpetic neuralgia (PHN) receiving conservative treatment report unsatisfactory pain relief. Epidural steroid injections (ESIs) are commonly used as a therapeutic intervention in these patients. In this study, we aimed to determine if there are variables that predict the efficacy of ESI in patients with PHN.
Patients and methods: We retrospectively identified patients seen at Mayo Clinic who had PHN and received ESI. From their medical records, we abstracted the demographic variables, concurrent medication use, anatomic approach and medication for ESI, and degree of pain relief at 2 and 12 weeks’ postintervention.
Results: None of the studied variables were significantly associated with efficacy of ESI in patients with PHN. PHN that began <11 months before treatment was predictive of a response to ESI at 12 weeks postintervention (positive predictive value, 55%). Patients who reported poor ESI efficacy 2 weeks after the intervention had a 94% chance of still having pain at 12 weeks.
Conclusion: For this cohort of patients with PHN being treated with ESI, no demographic characteristics, concurrently used medications, or type of ESI were associated with ESI treatment efficacy at 2 or 12 weeks after the intervention.
Keywords: herpes zoster, intervention, neuropathy
Introduction
Postherpetic neuralgia (PHN), the most common complication of varicella zoster virus reactivation, may cause serious clinical problems that severely impair quality of life to an extent comparable to cancer, chronic obstructive pulmonary disease, AIDS, and fibromyalgia.1–4 The pain of PHN is severe and may result in anorexia, weight loss, fatigue, depression, and insomnia; taken together, these factors negatively impact work, quality of life, and social activities.5 PHN is caused by nerve damage from a herpes zoster (HZ) infection; pathologically, patients may have primary afferent neural body and axon degeneration, spinal cord atrophy, scarring of the dorsal root ganglion, and loss of epidermal innervation.6,7 These changes contribute to increased N-methyl-D-aspartate glutamate receptor–dependent excitability of spinal dorsal horn neurons,8–10 which contribute to the neuropathic pain of PHN.
Noninvasive management practices, which are widely used for PHN, have not been consistently effective.11,12 Invasive treatment options have been developed, including local infiltration, sympathetic nerve blocks, and intrathecal injections. However, the reported efficacy of the invasive methods also is inconsistent.13–17
Epidural steroid injection (ESI) with the transforaminal and interlaminar administration of steroids and local anesthetics is among the more common treatments for patients with refractory PHN. However, its effectiveness is controversial. To our knowledge, the only study investigating factors associated with improved efficacy of transforaminal ESI for PHN reported a symptom duration of <3 months as the only significant predictor of benefit.18 The specific aims of the present study were to seek other factors associated with the efficacy of ESI in our patient population with PHN and to report our experience for therapeutic success with ESI.
Methods
The Mayo Clinic Institutional Review Board approved this retrospective study.
We searched electronic health records to identify patients with PHN managed by ESI who were seen at Mayo Clinic (Arizona, Florida, and Rochester campuses) from January 1, 1997, through April 1, 2018. PHN was defined as pain in the area of the eruption that persisted for >90 days after the onset of the rash.19–22 The following patient data were recorded: age, sex, comorbidities, concurrent medications, duration of PHN, anatomic approach of ESI, medication used for ESI, number of blocks, treatment date, and degree of pain relief at 2 and 12 weeks' postintervention. Pain relief was noted in the records in multiple ways: 1) as “good,” “moderate,” or “poor”; 2) as percent pain relief; or 3) as a point reduction on a pain scale (1–10, with 10 being severe pain). For records showing percent pain relief or pain scales, we considered up to 20% or a 2-point reduction as poor relief; 30–60% or a 3- to 6-point reduction as moderate relief; and >70% or at least a 7-point reduction as good relief. All patient-specific identifiers were removed from the data set before analysis.
Univariate logistic regression using the Firth penalized likelihood approach23 was used to investigate the association between patient characteristics, concurrent medication use, type of intervention, and moderate-to-good pain relief outcomes at 2 and 12 weeks' postintervention. Receiver operating characteristic analysis and the Youden index were used to establish the optimum cutoff point for PHN duration that would be predictive of moderate-to-good pain relief at 12 weeks. The statistical analysis was completed using SAS software, version 9.3 (SAS Institute Inc.,Cary, NC, USA).
Results
Our initial search of the electronic health records, using the terms “epidural steroid injection” and “postherpetic neuralgia,” yielded 528 medical records. The records were reviewed, and we identified 42 patients meeting the definition of PHN from reactivation of HZ who were treated with ESI (54.8% male). Table 1 summarizes the demographic and clinical characteristics of the patients.
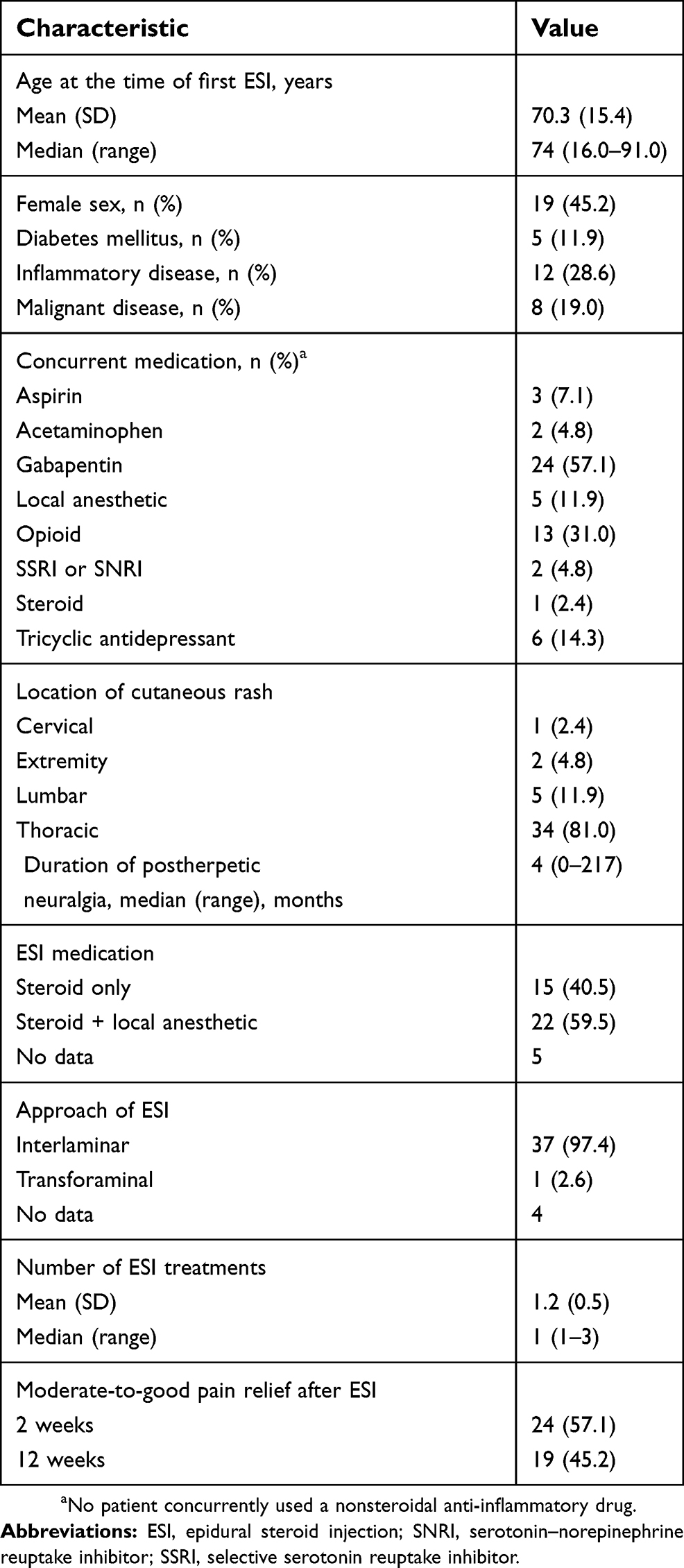 | Table 1 Demographics and clinical characteristics (N=42) |
We did not identify any significant association between moderate-to-good pain relief (at 2 or 12 weeks post-ESI) and patient demographics, concurrent medication use, ESI approach, or medications injected for the intervention (Tables 2 and 3). Patients who reported poor ESI efficacy 2 weeks after the intervention had a 94% chance of still having pain at 12 weeks. Of the 24 patients who had a moderate-to-good pain relief 2 weeks after ESI, 19 (79%) had persistent relief after 12 weeks. PHN duration <11 months was predictive of moderate-to-good pain relief at 12 weeks’ post-ESI, with a positive predictive value of 55.2% (Table 4).
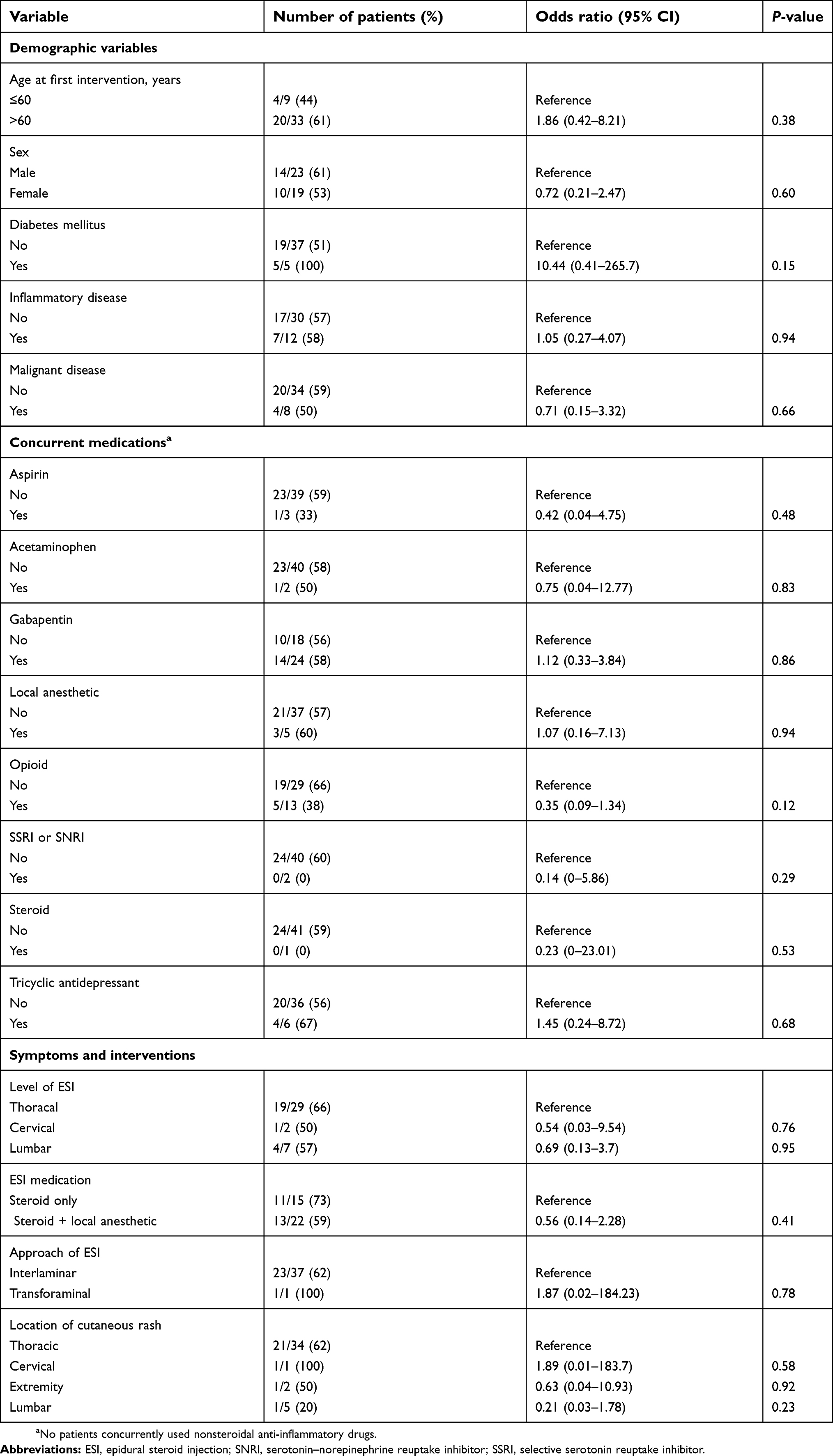 | Table 2 Variables associated with moderate-to-good pain relief, 2 weeks after ESI |
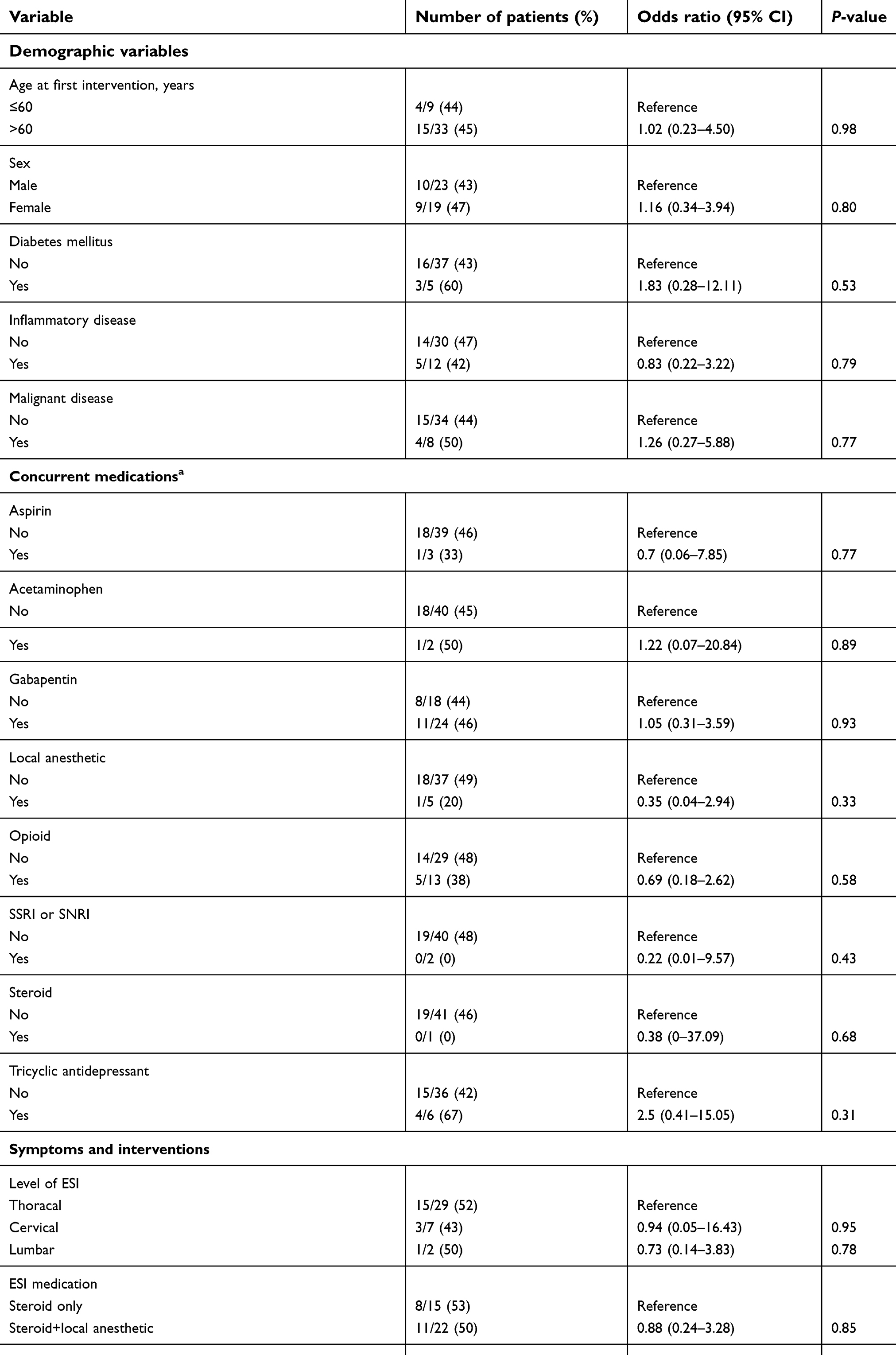 | Table 3 Variables associated with moderate-to-good pain relief, 12 weeks after ESI |
 | Table 4 Sensitivity, specificity, PPV, NPV, and accuracy of likelihood of treatment response based on the duration of PHN |
Discussion
PHN is associated with an impaired quality of life, especially for elderly patients.24 Current American Academy of Neurology guidelines13 for reducing PHN-associated pain recommend TCA, anticonvulsants such as gabapentin and pregabalin, opioids, and topical lidocaine. However, at least 30% of patients with PHN have unsatisfactory relief of pain with these suggested treatments.25 Hence, regional anesthetic procedures, including subcutaneous anesthetic and steroid injections, sympathetic and intrathecal nerve blocks, and ESI, are often used for management of PHN, even though these treatments are not strongly evidence based.
Mixed results have been reported with subcutaneous anesthetic plus steroid injections or sympathetic nerve blocks in the management of PHN.13,14 Intrathecal injections have shown promise, but concerns regarding their safety remain.11,13,14,26–30 The risk of arachnoiditis reported with intrathecal injections likely will prevent this treatment from becoming widely used.27,28,30
The role of ESI in established PHN is also controversial. Although ESI can induce short-term (1-month) pain relief for patients with acute HZ, it is not effective for preventing long-term PHN.15Two studies by Forrest16,17 compared the effects of ESI in patients with 1) PHN lasting >6 months or 2) posttraumatic neuralgia. He reported that the pain of PHN was significantly reduced by ESI with local anesthetics, but the treatment was not as effective for patients with posttraumatic neuralgia. However, it is unclear whether an interlaminar or transforaminal approach was applied.
A case report by Mehta et al5 described a 64-year-old man with refractory thoracic dermatome PHN, 1.5 years after HZ onset; 12 weeks after transforaminal ESI, he had complete resolution of symptoms. Kwak et al18 suggested that the only factor positively associated with the effectiveness of transforaminal ESI was a symptom duration shorter than 12 weeks; factors such as patient age, sex, severity of initial pain, number of nerve blocks, or comorbidities such as diabetes mellitus or malignancy were not associated with the effectiveness of transforaminal ESI. Mixed reports have been published describing the application of interlaminar ESI in HZ and PHN.15,31,32
In our study, 97% of patients were treated with interlaminar ESI. We did not identify any factor that predicted an increased likelihood of moderate-to-good pain relief with interlaminar ESI at 2 and 12 weeks' postintervention. However, we verified the overall effectiveness of the intervention with ESI and noted a sustained benefit when the therapy was given to patients with PHN duration <11 months.
A limitation of our study was that we had only 1 patient for whom a transforaminal approach was confirmed. The transforaminal approach delivers therapy close to the site of inflammation of the targeted dorsal root ganglion and spinal nerve, thereby possibly providing the greatest potential for benefit with limited systemic impact.33,34 We are aware of no published studies that have compared the effect of interlaminar and transforaminal ESI for PHN.
Our study was also limited by its retrospective design; therefore, some aspects of data collection may have been incomplete. A high number of our patients presented to their primary care physicians at the time of HZ, and data such as pain severity and antiviral and adjuvant treatment determined at those consultations were not available for review. Our sample size was small and the study may have been underpowered.
Inherent risks of ESI include infection, bleeding, and minor trauma along the course of the needle; such risks must be acknowledged when considering this treatment.35
In conclusion, this study is the first to investigate predictive factors associated with the efficacy of interlaminar ESI in patients with PHN. PHN duration <11 months was predictive of moderate-to-good pain relief 12 weeks after ESI. Additionally, 80% of patients who reported moderate-to-good treatment efficacy 2 weeks after ESI had continued efficacy at 12 weeks. However, none of the patient characteristics, concurrent medications, or type of intervention administered were associated with efficacy of ESI in PHN. Future studies are warranted to verify this observation. The effectiveness of ESI in PHN is not dependent on patient characteristics, concurrent medications, block numbers, or type of ESI.
Abbreviation list
ESI, epidural steroid injection; HZ, herpes zoster; PHN, postherpetic neuralgia.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Lydick E, Epstein RS, Himmelberger D, White CJ. Herpes zoster and quality of life: a self-limited disease with severe impact. Neurology. 1995;45(12 Suppl 8):S52–53.
2. Johnson RW, Bouhassira D, Kassianos G, Leplege A, Schmader KE, Weinke T. The impact of herpes zoster and post-herpetic neuralgia on quality-of-life. BMC Med. 2010;8:37. doi:10.1186/1741-7015-8-37
3. Chidiac C, Bruxelle J, Daures JP, et al. Characteristics of patients with herpes zoster on presentation to practitioners in France. Clin Infect Dis. 2001;33(1):62–69. doi:10.1086/320884
4. Oster G, Harding G, Dukes E, Edelsberg J, Cleary PD. Pain, medication use, and health-related quality of life in older persons with postherpetic neuralgia: results from a population-based survey. J Pain. 2005;6(6):356–363. doi:10.1016/j.jpain.2005.01.359
5. Mehta P, Maher P, Singh JR. Treatment of postherpetic neuralgia using a thoracic transforaminal epidural steroid injection. Pm R. 2015;7(4):443–446. doi:10.1016/j.pmrj.2014.11.009
6. Head H, Campbell AW, Kennedy PG. The pathology of herpes zoster and its bearing on sensory localisation. Rev Med Virol. 1997;7(3):131–143.
7. Oaklander AL, Romans K, Horasek S, Stocks A, Hauer P, Meyer RA. Unilateral postherpetic neuralgia is associated with bilateral sensory neuron damage. Ann Neurol. 1998;44(5):789–795. doi:10.1002/ana.410440513
8. Laird JM, Bennett GJ. An electrophysiological study of dorsal horn neurons in the spinal cord of rats with an experimental peripheral neuropathy. J Neurophysiol. 1993;69(6):2072–2085. doi:10.1152/jn.1993.69.6.2072
9. Mayer DJ, Mao J, Holt J, Price DD. Cellular mechanisms of neuropathic pain, morphine tolerance, and their interactions. Proc Natl Acad Sci U S A. 1999;96(14):7731–7736.
10. Palecek J, Dougherty PM, Kim SH, et al. Responses of spinothalamic tract neurons to mechanical and thermal stimuli in an experimental model of peripheral neuropathy in primates. J Neurophysiol. 1992;68(6):1951–1966. doi:10.1152/jn.1992.68.6.1951
11. Argoff CE, Katz N, Backonja M. Treatment of postherpetic neuralgia: a review of therapeutic options. J Pain Symptom Manage. 2004;28(4):396–411. doi:10.1016/j.jpainsymman.2004.01.014
12. Amjad M, Mashhood AA. The efficacy of local infiltration of triamcinolone acetonide with lignocaine compared with lignocaine alone in the treatment of postherpetic neuralgia. J Coll Physicians Surg Pak. 2005;15(11):683–685. doi:11.2005/JCPSP.683685
13. Dubinsky RM, Kabbani H, El-Chami Z, Boutwell C, Ali H. Quality standards subcommittee of the American Academy of N. Practice parameter: treatment of postherpetic neuralgia: an evidence-based report of the quality standards subcommittee of the American Academy of Neurology. Neurology. 2004;63(6):959–965.
14. Rowbotham MC, Petersen KL. Zoster-associated pain and neural dysfunction. Pain. 2001;93(1):1–5.
15. van Wijck AJ, Opstelten W, Moons KG, et al. The PINE study of epidural steroids and local anaesthetics to prevent postherpetic neuralgia: a randomised controlled trial. Lancet. 2006;367(9506):219–224. doi:10.1016/S0140-6736(06)68032-X
16. Forrest JB. Management of chronic dorsal root pain with epidural steroid. Can Anaesth Soc J. 1978;25(3):218–225.
17. Forrest JB. The response to epidural steroid injections in chronic dorsal root pain. Can Anaesth Soc J. 1980;27(1):40–46.
18. Kwak S, Nahm FS, Choi EJ, Lee PB. Transformainal epidural steroid injections within 3 months; better outcome in the postherpetic neuralgia. 2016. Available from:
19. Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J Med. 2005;352(22):2271–2284. doi:10.1056/NEJMoa051016
20. Opstelten W, Zuithoff NP, van Essen GA, et al. Predicting postherpetic neuralgia in elderly primary care patients with herpes zoster: prospective prognostic study. Pain. 2007;132(Suppl 1):S52–59. doi:10.1016/j.pain.2007.02.004
21. Schmader KE. Epidemiology and impact on quality of life of postherpetic neuralgia and painful diabetic neuropathy. Clin J Pain. 2002;18(6):350–354.
22. Arani RB, Soong SJ, Weiss HL, et al. Phase specific analysis of herpes zoster associated pain data: a new statistical approach. Stat Med. 2001;20(16):2429–2439.
23. Heinze G, Schemper M. A solution to the problem of separation in logistic regression. Stat Med. 2002;21(16):2409–2419. doi:10.1002/sim.1047
24. Drolet M, Brisson M, Schmader KE, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. Cmaj. 2010;182(16):1731–1736. doi:10.1503/cmaj.091711
25. Watson CP, Oaklander AL. Postherpetic neuralgia. Pain Pract. 2002;2(4):295–307. doi:10.1046/j.1533-2500.2002.02039.x
26. Johnson RW, Dworkin RH. Treatment of herpes zoster and postherpetic neuralgia. BMJ. 2003;326(7392):748–750. doi:10.1136/bmj.326.7392.748
27. Kotani N, Kushikata T, Hashimoto H, et al. Intrathecal methylprednisolone for intractable postherpetic neuralgia. N Engl J Med. 2000;343(21):1514–1519. doi:10.1056/NEJM200011233432102
28. Kikuchi A, Kotani N, Sato T, Takamura K, Sakai I, Matsuki A. Comparative therapeutic evaluation of intrathecal versus epidural methylprednisolone for long-term analgesia in patients with intractable postherpetic neuralgia. Reg Anesth Pain Med. 1999;24(4):287–293.
29. Baron R, Wasner G. Prevention and treatment of postherpetic neuralgia. Lancet. 2006;367(9506):186–188. doi:10.1016/S0140-6736(06)68010-0
30. Abram SE. Intrathecal steroid injection for postherpetic neuralgia: what are the risks? Reg Anesth Pain Med. 1999;24(4):283–285.
31. Rutgers MJ, Dirksen R. The prevention of postherpetic neuralgia: a retrospective view of patients treated in the acute phase of herpes zoster. Br J Clin Pract. 1988;42(10):412–414.
32. Perkins HM, Hanlon PR. Epidural injection of local anesthetic and steroids for relief of pain secondary to herpes zoster. Arch Surg. 1978;113(3):253–254.
33. Opstelten W, van Wijck AJ, Moons KG, et al. Treatment of patients with herpes zoster by epidural injection of steroids and local anaesthetics: less pain after 1 month, but no effect on long-term postherpetic neuralgia–a randomised trial. Ned Tijdschr Geneeskd. 2006;150(48):2649–2655.
34. Hardy D. Relief of pain in acute herpes zoster by nerve blocks and possible prevention of post-herpetic neuralgia. Can J Anaesth. 2005;52(2):186–190. doi:10.1007/BF03027727
35. Shakir A, Kimbrough DA, Mehta B. Postherpetic neuralgia involving the right C5 dermatome treated with a cervical transforaminal epidural steroid injection: a case report. Arch Phys Med Rehabil. 2007;88(2):255–258. doi:10.1016/j.apmr.2006.11.001
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.