")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
Pancreatic ductal adenocarcinoma and chronic pancreatitis may be diagnosed by exhaled-breath profiles: a multicenter pilot study
Authors Uslu HI , Dölle AR, Dullemen HM , Aktas H, Kolkman JJ, Venneman NG
Received 10 October 2018
Accepted for publication 9 July 2019
Published 14 August 2019 Volume 2019:12 Pages 385—390
DOI https://doi.org/10.2147/CEG.S189102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Koulaouzidis
HI Uslu,1,2 AR Dölle,1 HM Dullemen,2 H Aktas,3 JJ Kolkman,1,2 NG Venneman1
1Department of Gastroenterology and Hepatology, Medisch Spectrum Twente, Enschede, The Netherlands; 2Department of Gastroenterology and Hepatology, University Medical Center Groningen (UMCG), Groningen, The Netherlands; 3Department of Gastroenterology and Hepatology, Ziekenhuisgroep Twente (ZGT), Almelo, The Netherlands
Background: The diagnosis of pancreatic adenocarcinoma and chronic pancreatitis often rely on expensive and invasive diagnostic approaches, which are not always discriminative since patients with chronic pancreatitis and pancreatic adenocarcinoma may present with similar symptoms. Volatile organic compounds (VOCs) in expired breath, could be used as a non-invasive diagnostic biological marker for detection of pancreatic pathology. Detection and discrimination of pancreatic pathology with an electronic nose has not yet been reported.
Purpose: The objective of this pilot study was to determine the diagnostic potential of an electronic nose to identify pancreatic adenocarcinoma and chronic pancreatitis by analyzing volatile organic compoundg (VOC) profiles in exhaled air.
Patients and methods: In a multicenter study, the exhaled air of 56 chronic pancreatitis patients, 29 pancreatic adenocarcinoma patients, and 74 disease controls were analyzed using an electronic nose based on 3 metal oxide sensors (MOS). The measurements were evaluated utilizing an artificial neural network.
Results: VOC profiles of chronic pancreatitis patients could be discriminated from disease controls with an accuracy of 0.87 (AUC 0.95, sensitivity 80%, specificity 92%). Also, VOC profiles of patients with pancreatic adenocarcinoma differed from disease controls with an accuracy of 0.83 (AUC 0.87, sensitivity 83%, specificity 82%). Discrimination between chronic pancreatitis and pancreatic adenocarcinoma showed an accuracy of 0.75 (AUC 0.83, sensitivity 83%, specificity 71%).
Conclusion: An electronic nose may be a valuable diagnostic tool in diagnosis of pancreatic adenocarcinoma and chronic pancreatitis. The current study shows the potential of an electronic nose for discriminating between chronic pancreatitis, pancreatic adenocarcinoma and healthy controls. The results from this proof-of-concept study warrant external validation in larger cohorts.
Keywords: pancreatic adenocarcinoma, chronic pancreatitis, electronic nose, exhaled breath
Introduction
Pancreatic adenocarcinoma is the seventh most common cause of cancer-related deaths worldwide.1 In patients with chronic pancreatitis, the risk of developing pancreatic carcinoma is increased.2 The majority of patients with pancreatic adenocarcinoma have locally advanced or metastatic disease when diagnosed. Therefore, diagnosis in an asymptomatic stage could improve prognosis. Also, it is known that chronic pancreatitis can mimic pancreatic carcinoma.3 Discrimination between pancreatic adenocarcinoma and chronic pancreatitis is important, since the two diseases have different treatment strategies and prognoses.
Volatile organic compounds (VOC) in exhaled breath could be used as a non-invasive diagnostic biological marker for detection of pancreatic pathology. Previously, numerous disorders have been linked to unique breath profiles, including tuberculosis, lung cancer, asthma and cystic fibrosis, head and neck cancer and amyotrophic lateral sclerosis.4–8 In 2016, Mayerle and co-workers identified biomarker signatures which may differentiate between pancreatic adenocarcinoma and chronic pancreatitis, showing the potential value of using metabolic markers.9 Most studies were performed with a laborious and expensive gas chromatography-mass spectroscopy (GC-MS) set-up. Analysis of VOC breath patterns using an electronic nose is a promising technology to discriminate between chronic pancreatitis and pancreatic adenocarcinoma.
Therefore, we aimed to determine the diagnostic potential of an electronic nose (Aeonose, The eNose Company, the Netherlands) to differentiate between individuals with chronic pancreatitis, pancreas adenocarcinoma and disease controls based on exhaled air analysis. By using artificial neural network (ANN) software, exhaled-breath patterns can be distinguished.
A detailed description of patient selection and methods is available in the Methods section.5 Briefly, the diagnostic accuracy of the electronic nose was examined in a multicenter, prospective design in 56 participants with chronic pancreatitis and 29 patients with pancreatic adenocarcinoma. In patients with chronic pancreatitis, the diagnosis was confirmed in 19 patients by endoscopic ultrasound (EUS) according to the Rosemont criteria and in 37 patients with computed tomography (CT)/Magnetic Resonance Imaging (MRI) only. The diagnosis in patients with pancreatic adenocarcinoma was confirmed by histology after surgery in 15 patients, by EUS-FNA in 12 patients and by CT-scan only in 2 patients. These patients were recruited from the outpatient clinics and clinical wards of the Department of Gastroenterology & Hepatology and Department of Surgery, at Medisch Spectrum Twente (MST), University Medical Centre Groningen (UMCG), and Ziekenhuisgroep Twente (ZGT), the Netherlands.
For five minutes, the subjects gently breathed through a mouthpiece which was attached to the electronic nose. Baseline characteristics of these groups are shown in Table 1. The breath profiles and classifications were used to train ANN, and subsequently cross-validated using the “Leave-10%-Out” method.5
 |
Table 1 Baseline characteristics of study participants |
Methods
Study design
The study concerns a multicenter, prospective, case-disease control design in subjects with confirmed diagnosis of chronic pancreatitis or pancreatic adenocarcinoma. The study was conducted between April 2015 and July 2017.
Subjects
Patients with chronic pancreatitis (CP), pancreatic adenocarcinoma and disease controls were recruited sequentially during a single visit at the outpatient clinic of Department of Gastroenterology & Hepatology and Department of Surgery at Medisch Spectrum Twente (MST), University Medical Center Groningen (UMCG) and Ziekenhuisgroep Twente (ZGT), or in the respective clinical wards, all in the Netherlands.
In patients with chronic pancreatitis, 46 patients were in remission and 10 were analyzed during an exacerbation. The disease control group consisted of subjects without relevant disease states, which were referred for colonoscopy because of changed bowel habit or rectal bleeding. They were included as disease controls when colonoscopy and pathological analysis excluded colorectal cancer or advanced adenoma. Subjects with (hyperplastic) polyps as well as non-advanced adenomas were accepted as disease controls. Individuals with an unclear diagnosis were excluded from the study. In patients with pancreas cancer, 23 carcinomas were located in the head, 5 in the body and 1 in the tail.
69 subjects were excluded from the analyses, largely due to other active malignancies, infections, inflammations or inability to provide exhaled air. 6 subjects were excluded due to technical problems. Exhaled air was analyzed in 56 subjects with chronic pancreatitis, 29 subjects with pancreatic adenocarcinoma and 74 disease controls.
Inclusion criteria for the subjects were: age ≥18 years, written informed consent, no breathing problems. Exclusion criteria were hemodynamic instability, severe pulmonary or cardiovascular disease, liver and/or renal insufficiency, unstable diabetes mellitus, systemic inflammatory disease, unstable thyroid function, oral corticosteroid use, active treatment with radiotherapy and/or chemotherapy, active primary malignancy other than pancreatic adenocarcinoma. All recorded personal information was anonymized, including age, gender, body mass index, tobacco and alcohol history, medication, hyperbilirubinemia (>30 mmol/L), tumor stage, tumor localization and major comorbidities including DM, diseases of heart, lung, kidneys or liver, and history of malignancies. Current medication except prednisolone <10 mg daily was allowed. In order to prevent systematic errors caused by disturbing smells, no flowers or vegetables were allowed in the rooms during breath measurement. During the measurements, none of the patients was receiving any special therapy which potentially could affect the results. No patients were included in the study with prednisolone> 10 mg, active treatment by radiotherapy and/or chemotherapy, hemodynamic instability, severe pulmonary or cardiovascular disease, liver and/or renal insufficiency, unstable diabetes mellitus, systemic inflammatory disease, unstable thyroid function. Initial treatment after the measurements in patients with cancer was resection in 15 patients, neoadjuvant therapy in 1, palliative chemotherapy in 9 and best supportive care in 5 patients.
Baseline characteristics
Chronic pancreatitis versus controls: Patients with chronic pancreatitis were comparable to disease controls concerning gender, age, structural alcohol intake, history of pulmonary disease, history of malignancy and hyperbilirubinemia. Current smokers and subjects with diabetes mellitus were more frequent in chronic pancreatitis patients (see Table 1).
Pancreatic adenocarcinoma versus controls: Patients with pancreatic adenocarcinoma were comparable to disease controls concerning gender, body mass index, current smokers, structural alcohol intake and history of pulmonary disease. Patients with pancreatic adenocarcinoma were significantly older than disease controls. A history of diabetes mellitus, malignancy and hyperbilirubinemia was also higher in subjects with pancreatic adenocarcinoma, as shown in Table 1
Chronic pancreatitis versus pancreatic adenocarcinoma: Patients diagnosed with pancreatic adenocarcinoma were significantly older, had higher BMI, a more frequent history of malignancy or hyperbilirubinemia than subjects with chronic pancreatitis. There were no significant differences observed in gender, structural alcohol intake, diabetes mellitus and history of pulmonary disease between the two groups, as seen in Table 1.
Exhaled-breath collection
To minimize confounding factors, participants were requested to rest and refrain from food and drinking for at least three hours prior to the measurement, with the exception of water. The subjects breathed through a mouthpiece with a carbon filter, which was attached to the electronic nose. Also, a HEPA filter was mounted in the mouthpiece to prevent contamination of the inner structure of the electronic nose. Inhaled air passed through a carbon filter; the valve to the Aeonose was then closed. Exhaled air passed through the bacterial filter into the Aeonose; the valve to the outside of the mouthpiece was then closed. A nose clamp was used to force patients to breathe through the Aeonose. Patients were requested to exhale through the electronic nose for 5 mins. During the study, 3 electronic nose devices were randomly used to rule out potential inter-device differences.
System descriptions; the electronic nose
The integrated device technology in the current study is based on an array of three metaloxide sensors attached to a micro hotplate. The sensors act as semiconductors at different temperatures ranging 230–340°C. VOCs in exhaled air interact with these sensors, resulting in redox reactions changing the conductivity of the sensors. The response of redox reactions depends on the surface material of the sensor, temperature cycle and the gas composition. Different organic compounds express various responses at different temperatures for the same sensor type. These reactions then result in changing the conductivity of each sensor surface that can be recorded as electronic signal and quantified as unique smell-print. The information obtained was transferred from the device to a notebook for assessment. Consequently, the smell-prints recorded from different samples were arranged in groups by pattern recognition algorithms.
Pattern recognition and data analysis
A breath profile consists of approx. 7000 data points for each patient. First, the data are pre-processed (eg, standardized) in order to compensate for deterioration in time of the sensors. Then the data are compressed using a Tucker3-like algorithm, as it is too large to analyze. In this way, redundant data and noise are removed. This data reduction process does not result in loss of significant data. It turns out that the breath profile can be represented by a vector with 6–15 elements.5
Together with the classification obtained from other diagnostic techniques, the compressed vectors are used for training ANN. In this way, the ANN settings for a specific disease can be fixed.
In order to check whether the ANN is actually capable of classifying on the disease and not on some artifact, “leave-10%-Out“ cross-validation is applied: In this method, 90% of the dataset is used for training the ANN, while the remaining 10% is predicted. Next, another 10% of the dataset is classified on the remaining 90% used for training. This process is being repeated 10 times and in that way, in fact, all patients can be classified based on a model from the other measurements. Once an ANN model has been fixed, unknown vectors representing breath profiles can be classified without needing the availability of additional diagnostic information.
During the data analysis, multiple ANNs can be derived using different sensor combinations (A, B, C, AB, AC, BC, ABC), pre-processing techniques, vector lengths and ANN topologies.
The models were all evaluated in terms of sensitivity and specificity and ranked in that way. For this data-analysis process, proprietary software package Aethena was used. Additionally, IBM SPSS Statistics, version 22 for Windows (IBM SPSS Statistics, IBM Corporation, Armonk, NY) was utilized to create receiver operating characteristic (ROC) curves to establish the area under the curve (AUC). Two-tailed t-tests were executed to analyze continuous data after evaluation of symmetric distribution in statistics. Chi-square tests (χ2 test) were used for distributions of categorical data. Fisher’s exact test was utilized with small sample sizes.
Results
The electronic nose was able to distinguish between chronic pancreatitis and disease controls with an accuracy of 87% (Figure 1A), sensitivity 80% (95% CI: 67–89%), specificity 92% (95% CI: 83–96%), negative predictive value of 86% (95% CI: 76–93%) and a positive predictive value of 88% (95% CI: 75–95%).
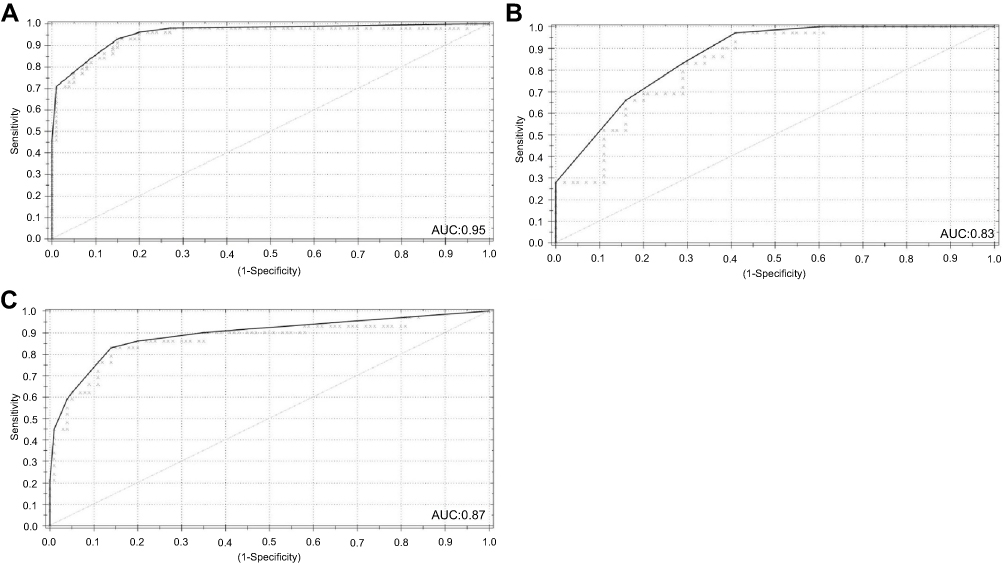 |
Figure 1 (A) ROC curve in chronic pancreatitis versus healthy controls; (B) ROC curve in pancreatic adenocarcinoma versus controls; and (C) ROC curve in chronic pancreatitis versus pancreatic adenocarcinoma. |
Pancreatic adenocarcinoma was distinguished from disease controls with an accuracy of 83% (Figure 1B), sensitivity 83% (95% CI: 64–93%), specificity 82% (95% CI: 71–90%), negative predictive value of 92% (95% CI: 82–97%) and a positive predictive value of 65% (95 CI: 47–79%).
The electronic nose discriminated pancreatic adenocarcinoma from chronic pancreatitis with an accuracy of 75% (Figure 1C), sensitivity 83% (95% CI: 64–93%), specificity 71% (95% CI: 58–82%), negative predictive value of 89% (95% CI: 75–96%) and a positive predictive value of 60% (95% CI: 43% 75%).
Discussion
Our study has a number of limitations. Firstly, it is unclear which VOCs are responsible for detection of pancreatic pathology by an electronic nose. Secondly, detection of pancreatic adenocarcinoma may be stage-dependent. Thus, it remains unknown whether early pancreatic cancer could be detected as well. Also, localization of the lesion may effect metabolism, which in turn may effect VOC patterns. Although the disease control group was not screened for pancreatic pathology, disease controls were assumed not to suffer from pancreatic pathology, considering its low incidence. Furthermore, various patients with adenocarcinoma were cholestatic. Cholestasis may have profound effects on metabolism, and therefore on exhaled VOCs. In chronic pancreatitis patients, exacerbation of complaints may also affect metabolism, and therefore exhaled VOCs. Finally, smoking habits and/or alcohol intake may have affected our findings.
Our results suggest that chronic pancreatitis patients, pancreatic adenocarcinoma patients and disease controls exhibit differences in metabolism reflected by differences in measured VOC patterns. The current study reflects the potential of an electronic nose for detecting chronic pancreatitis and pancreatic adenocarcinoma. The major advantage of the Aeonose is that it allows for easy measurement within minutes, in contrast to the laborious standard VOC-techniques using gas chromatography. The classification of VOC patterns by extensive neural network modeling may improve with a larger number of subjects. With increased sensitivity and specificity, the Aeonose may be a useful tool in the workup of patients with suspected pancreatic disease. It may also have a role in non-invasive screening of high-risk subjects, or follow-up after pancreatic surgery for pancreatic adenocarcinoma. The results in our study need validation in a larger multicenter blinded cohort with pre-diagnosed subjects, stratified for cholestasis, localization, stage and exacerbation, in line with STARD Statement.10
Ethical considerations
The current study was authorized by the local medical ethics committee, Medische Ethische Toetsingscommussie (METC) Twente (no. K15-36) and was conducted in accordance with the Helsinki Declaration. All patients were informed both verbally and on paper, and they had given their written informed consent before taking part in measurements. The staff of participating hospitals received written information and they were orally informed fully about the study.
Acknowledgments
We thank all patients for participating in this study. We also like to give special thanks to all members of departments of gastroenterology and surgery at the participating hospitals. We are thankful to L Wymenga (medical doctor) and I Ertugrul (medical student) for helping to recruit the patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ilic M, Ilic I. Epidemiology of pancreatic cancer. World J Gastroenterol. 2016;22(44):9694–9705. doi:10.3748/wjg.v22.i44.9694.
2. Kudo Y, Kamisawa T, Anjiki H, Takuma K, Egawa N. Incidence of and risk factors for developing pancreatic cancer in patients with chronic pancreatitis. Hepatogastroenterology. 2011;58(106):609–611.
3. Lowenfels AB, Maisonneuve P, Cavallini G, et al. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med. 1993;328(20):1433–1437. doi:10.1056/NEJM199305203282001
4. Zetola NM, Modongo C, Matsiri O, et al. Diagnosis of pulmonary tuberculosis and assessment of treatment response through analyses of volatile compound patterns in exhaled breath samples. J Infect. 2017;74(4):367–376. doi:10.1016/j.jinf.2016.12.016
5. Kort S, Brusse-keizer M, Gerritsen JW, Van der Palen J. Data analysis of electronic nose technology in lung cancer: generating prediction models by means of Aethena. J Breath Res. 2017;11(2):026006. doi:10.1088/1752-7163/aa6b08
6. Bannier MA, Van de Kant KD, Jöbsis Q, Dompeling E. Feasibility and diagnostic accuracy of an electronic nose in children with asthma and cystic fibrosis. J Breath Res. 2019;13(3):036009. doi:10.1088/1752-7163/aae158.
7. Van Hooren MRA, Leunis N, Brandsma DS, Dingemans A-MC, Kremer B, Kross KW. Differentiating head and neck carcinoma from lung carcinoma with an electronic nose: a proof of concept study. Eur Arch Oto-Rhino-Laryngol. 2016;273(11):3897–3903. doi:10.1007/s00405-016-4038-x.
8. Dragonieri S, Quaranta VN, Carratu P, et al. An electronic nose may sniff out amyotrophic lateral sclerosis. Respir Physiol Neurobiol. 2016;232:22–25. doi:10.1016/j.resp.2016.06.005
9. Mayerle J, Kalthoff H, Reszka R, et al. Metabolic biomarker signature to differentiate pancreatic ductal adenocarcinoma from chronic pancreatitis. Gut. 2017. doi:10.1136/gutjnl-2016-312432
10. Bossuyt PM, Reitsma JB, Bruns DE, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ. 2015;351:h5527. doi:10.1136/bmj.h5527.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.