")
Back to Journals » Clinical Ophthalmology » Volume 11
Pain perception description after advanced surface ablation
Authors Sobas EM , Videla S, Vázquez A, Fernández I, Maldonado MJ , Pastor JC
Received 15 February 2017
Accepted for publication 28 February 2017
Published 7 April 2017 Volume 2017:11 Pages 647—655
DOI https://doi.org/10.2147/OPTH.S134542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eva M Sobas,1,2 Sebastián Videla,3,4 Amanda Vázquez,1 Itziar Fernández,1,5 Miguel J Maldonado,1 José-Carlos Pastor1,6,7
1Instituto Universitario de Oftalmobiología Aplicada (IOBA), Universidad de Valladolid, Valladolid, Spain; 2Facultad de Enfermería, Universidad de Valladolid, Valladolid Spain; 3Laboratorios Dr. Esteve S.A., Barcelona, Spain; 4Department of Experimental and Health Sciences, Facultad de Ciencias de la Salud y de la Vida, Universidad Pompeu Fabra, Barcelona, Spain; 5Networking Research Center on Bioengineering, Biomaterials and Nanomedicine (CIBER-BBN), Valladolid, Spain; 6Department of Ophthalmology, Hospital Clínico Universitario, Valladolid, Spain; 7Department of Surgery, Ophthalmology, Otorhinolaryngology and Physiotherapy, Facultad de Medicina, Universidad de Valladolid, Valladolid, Spain
Purpose: The objective of this study was to characterize the evolution of ocular pain after advanced surface ablation (ASA) to improve strategies in postoperative pain management.
Methods: This was a multicenter, prospective, descriptive, cohort study. The inclusion criteria were healthy individuals ≥18 years old receiving bilateral alcohol-assisted surface ablation with epithelial removal. Pain intensity was evaluated with the visual analog scale (VAS) and the numeric pain rating scale before and after surgery. Comorbidities (photophobia, burning, tearing, and foreign body sensation) and Hospital Anxiety and Depression (HAD) questionnaire were evaluated before and at 6 hours after surgery. Postoperative treatments included cold patch, topical cold antibiotics, topical steroids, and benzodiazepines.
Results: Thirty-two consecutive patients having similar profiles of postoperative pain evolution were included. At 0.5 hour after ASA, the pain score by VAS was 37±20 mm, and the maximum pain, 61±31 mm, occurred at 24 hours. Afterward, it decreased progressively until 72 hours after surgery (19±20 mm). Most patients (81%) scored >60 mm, and 44% required rescue medication. Among the comorbidities, all patients had photophobia and 84% had burning sensation. At 6 hours, the HAD score was 5.4±3.9, within the range of values considered as normal.
Conclusion: Postoperative acute ocular pain after ASA showed a characteristic evolution over time. Recognition of the pattern could be important for improving the acceptance of ASA and for improving strategies in pain management in the postoperative period.
Keywords: ocular pain, advanced surface ablation, model acute surgical pain
Introduction
Refractive surgery procedures such as advanced surface ablation (ASA), photorefractive keratectomy, and others are safe and effective to correct refractive errors, although they always produce some wounding of the cornea.1 Nevertheless, these procedures are gaining popularity because they diminish the risk of ectasia and eliminate flap complications that can occur after laser in situ keratomileusis. Indeed, ASA has gained popularity at the expense of laser in situ keratomileusis.1 One of the most important limitations of these procedures is the presence of postoperative pain and discomfort. Therefore, the management of these complications is a matter of great importance, and there are few specific reports on this subject.2
Improvement of postoperative pain management after ASA requires an understanding of the injury and of the inflammatory response of the corneal epithelial and stromal cells and the sensory nerves running through the wounded issues.3 The cornea is innervated by sensory fibers that have their origin in different functional types of trigeminal ganglion neurons. A majority (about 70%) of the sensory afferent fibers are polymodal nociceptors activated by mechanical forces, exogenous chemical irritants, endogenously released chemical mediators, and extreme temperatures.4 About 20% are pure mechanoreceptors, responding only to noxious mechanical force, and the remaining 10% are cold-sensitive receptors that respond primarily to temperature reductions on the corneal surface.5 After injury, nociceptor fibers are often the source of spontaneous pain sensation.6 In addition, inflammatory mediators released by the injured tissues activate intact and damaged nociceptor endings, further contributing to spontaneous pain and development of hyperalgesia and neurogenic inflammation. However, the effects of surgical injury on the distinctive response of the various functional classes of corneal sensory fibers are unknown.7
Postoperative pain after ASA is not well characterized, and there is little information regarding the duration, intensity, and peak of pain after ASA in clinical practice.8 Consequently, there is an unmet research need for the study of acute ocular pain. The purpose of this study is to characterize the evolution of the postoperative pain and discomfort after ASA, so that a more effective management can be developed.
Patients and methods
Study design
A multicenter (two sites), prospective, cohort study, based on patients who were treated with alcohol-assisted surface ablation with epithelial removal, was conducted.9 The ethics committee of the Universidad de Valladolid reviewed and approved the study protocol for both centers participating in this study. The study complied with the updated Declaration of Helsinki and the Spanish biomedical research regulatory requirements, and the protection of confidentiality concerning personal data was ensured as required by the Spanish law (LOPD 15/1999). All subjects provided their written informed consent before participation in the study.
Study population
The patients included in this study fulfilled the following inclusion criteria: both genders, between 18 and 60 years of age, Caucasian, free from ocular pain of any origin, no ocular disease, receiving ASA on both eyes, myopia between 0.75 and 9 D or hyperopia between 0.25 and 5 D, with or without astigmatism. The exclusion criteria included having pain in other part of the body in the preceding 7 days; having undergone ocular surgeries within the last 12 months; diagnosed with an autoimmune disease; receiving treatment with pain killers (including anti-inflammatories), psychotropics, anticonvulsants, or antidepressants; or having difficulties in communication. All ASA surgeries were performed by two experienced surgeons.
Data were collected regarding gender, pain intensity, ocular comorbidities, and rescue medication in the first 72 h after ASA. Questionnaires of Hospital Anxiety and Depression (HAD) and quality of life (QoL) were evaluated before ASA and at 6 h afterward, and adverse events up to 7 days after ASA were assessed.
ASA procedure
Preoperative
Each patient took one tablet of 0.5 mg alprazolam (Trankimazin®; Pfizer S.A., Puurs, Belgium) 30 min before ASA surgery. Twenty minutes before surgery, one drop of 5% lidocaine was applied topically. It was applied again 10 min later and once again just before surgery.
Intraoperative
An ethyl alcohol solution (17%) was placed on the cornea within an 8.5 mm solution cone and left in place for 30 s. Then, a merocel sponge (Medtronic Xomed Ophthalmics, Inc., Jacksonville, FL, USA) was placed to absorb the excess. After that, the corneal surface was rinsed with topical cold balanced salt solution and the epithelium was removed with a blunt spatula. This maneuver was followed by stromal ablation using the excimer laser MEL 70 G (Carl Zeiss Meditec, Jena, Germany), which incorporates an eye tracking system. The diameter of the treated area was always at least 6 mm with a transition to 9 mm. After the ablation, the surface was rinsed copiously with cold balanced salt solution. Then a drop of 0.3% ofloxacin (Exocin®; Allergan SA, Madrid, Spain) and a drop of 0.18% sodium hyaluronate (Vismed®; Thea Laboratories, SA, Barcelona, Spain) were applied. A therapeutic contact lens (Acuvue Oasis®; Johnson & Johnson, Limerick, Ireland) kept at 4°C was placed on to the cornea at the end of the procedure.
Postoperative
Immediately after surgery, patients received a cold patch for 15 min (Fredo Kit; KRZ, Barcelona, Spain). Patients were given topical cold antibiotics (ofloxacin, Exocin; Allergan SA; four times daily for 2 weeks), topical cold steroids (dexamethasone, Dexafree®; Thea Laboratories, SA; three times daily for 2 weeks), oral alprazolam 0.5 mg (Trankimazin; Pfizer SA, for the two first postoperative nights), oral vitamin C tablets (1 g/tablet, Redoxon®; Bayer, Barcelona, Spain; once daily for a month), topical 0.18% sodium hyaluronate (Vismed®; Thea Laboratory SA; four times daily for 2 weeks), and artificial tears (Viscofresh® 0.5%; Allergan SA; as needed, for several months).
All patients stayed in the surgical facilities for 4 or 6 h after ASA. They were instructed to apply the same medications to both eyes and to keep all eye drops at 4°C (refrigerator temperature). Initially, no other painkillers were prescribed, unless pain was deemed unbearable. In those cases, the patient was given a protocol to use a rescue medication.
Rescue medication for unbearable pain was initiated with one drop of cyclopentolate hydrochloride 10 mg/1 mL (Cyclopejico®; Allergan SA) three times a day for 2 or 3 days. If discomfort or pain continued after 30 min, then tramadol/paracetamol 37.5 mg/325 mg (Zaldiar®; Grünenthal Pharma, Aachen, Germany) was administered every 6 h for the first 36 h. If pain persisted, 0.2% or 0.4% oxybuprovacaine (Prescaína Colirio®; Laboratory Llorens SA, Barcelona, Spain) or tetracaine and oxybuprovacaine (Anestesico Doble; Alcon Cusi, Barcelona, Spain) was added. Patients were allowed to use any of the suggested drugs, but were not allowed to use more than four times a day for 4 days.
Postoperative pain assessment
Pain intensity was evaluated by means of the visual analog scale (VAS) and the numeric pain rating scale (NPRS).9 The VAS consisted of a horizontal line, 100 mm in length, where 0 mm corresponded to “no pain” and 100 mm to “the worst imaginable pain”. The NPRS was an 11-point scale from 0 to 10, where 0 corresponded to “no pain” and 10 to “the worst imaginable pain”. Pain intensity was evaluated before and 0.5, 1, 2, 3, 4, 5, 6, 9, 12, 24, 36, 48 (second day), 60, 72 (third day), 96 (fourth day), 120 (fifth day), and 144 (sixth day) h after surgery. Each patient was also given a diary to record his/her medication usage and pain and depression observations at home.
Other ocular symptoms, HAD questionnaire, QoL questionnaire, and Visual Function 25 (VF25) questionnaire
Other ocular symptoms
Based on a previous questionnaire developed by Sobas et al,10 the presence and intensity of the following ocular symptoms were recorded: photophobia, burning sensation, tearing, foreign body, itching, and headache. The intensity of each item was rated on a Likert scale of 4 points (range 0–3, where 0 corresponded to no symptom and 3 to the worst imaginable symptom).11 These ocular symptoms were evaluated before and at 1, 6, 48, and 120 h after surgery. The patient’s diary included this information.
HAD questionnaire
The HAD scale, validated in Spanish,12 was used to assess pre- and postsurgical anxiety and depression. HAD was evaluated before and at 6, 48, and 120 h after ASA. This self-administered questionnaire consisted of 14 items, divided into two 7-item subscales, one for anxiety and one for depression. Both subscales had the same cutoffs: 0–7, normal; 8–10, doubtful; and ≥11, existence of a clinical problem.
QoL questionnaire
The QoL short form-12 (SF12) health survey was evaluated before and at 24 and 72 h after surgery. This self-administered questionnaire consisted of 12 questions to measure the physical and mental health status: the physical component summary and the mental component summary. The score was computed from the scores of the 12 questions and ranged from 0 to 100. A score of 0 indicated the lowest level of physical and mental health and a score of 100 indicated the highest level.13
VF25 questionnaire
The VF25 questionnaire was evaluated before and at 24 and 72 h after surgery. This self-administered questionnaire consisted of a base set of 25 vision-targeted questions representing eleven vision-related constructs, plus an additional single-item general health rating question. Each item was converted to a 0–100 scale, so that 0 represented the lowest visual function and 100 represented the highest.13
Statistical analysis
Sample size was based on our previously published study in which 97% had postoperative pain10 Subsequent to that study, clinical records suggested that 99% of patients had postoperative pain after ASA (unpublished data). Thus, we assumed that 98% of the participants would have ocular pain. A representative sample should include 32 subjects, assuming the normal distribution and a range of ±2.5% for a two sided 95% confidence interval (95% CI). The P-values <0.05 were considered significant.
Baseline characteristics were summarized with standard descriptive statistics, and descriptive analyses were carried out. The postoperative incidence of pain and symptoms was estimated and the 95%CI was calculated. Analysis of variance (ANOVA) with repeated measures was used to evaluate mean differences over time. Sphericity assumption was checked by Mauchly’s test and, in case of violation of sphericity, the Greenhouse-Geisser correction was used. Post-hoc test using Benjamini and Hochberg correction for multiple comparisons was performed. Normality assumptions were checked by the Shapiro-Wilk test and, when this assumption was not valid; Friedman’s test was used, followed by the post-hoc analysis based on Wilcoxon-Nemenyi-McDonald-Thompson test.
Functional data analysis (FDA) was used for analyzing the temporal evolution of VAS scores. The eighteen VAS measurements for the 32 patients were transformed into 32 continuous smooth curves by spline smoothing with B-splines basis functions. The optimal smoothing parameters were found using cross validation criterion. In the sample of VAS curves, the mean curve was used descriptively. Differences between shapes of the mean curves for sex, age or rescue medication category were checked by a permuted t-test.
Functional principal component analysis (FPCA)14 to extract the most important features of the temporal evolution of VAS scores was used. We tried to extract a limited number of functional principal components (FPC) curves that represent independent parts of the overall variation observed in the sample of curves. The first component, PCA1, would explain the maximum amount of variability observed in the sample. Second and lower level components, PCA2 and others, would each explain elements that accounted for smaller amounts of variability. Thus, we reduced our original data to a small number of independent variables.
Data analysis was carried out using R Statistical Software version 3.2.4 (Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
A total of 32 consecutive patients (19 men and 13 women) were included between June 2015 and June 2016. The median (range) age was 28 (18–47) years, and all patients received surgery on both eyes.
Pain evolution after ASA procedure
All patients reported postoperative ocular pain (VAS ≥20 mm) from 0.5 to 60 h after surgery. For seven patients, the VAS score was <20 mm at 0.5 and 2 h after surgery, with no pain reported at 1 h. During that same time, the NRPS scores were <2 for four patients at 0.5 h, for one patient at 1 h, and for two patients at 2 h. For all patients, the peak pain occurred at 24 h after surgery with VAS and NPRS scores of 61±31 mm and 6.0±2.8, respectively.
There was great variability among patients in the intensity of pain experienced during the follow-up period (Figure 1). The average pain intensity for all of the participants increased sharply during the first 9 h after surgery, and then peaked at 24 h with a 6-point difference between pre- and postsurgical VAS at that time. After that, the pain intensity was approximately stable until 36 h, when it started declining until 96 h after surgery. The VAS score at 72 h was 19±20 mm. The evolution of pain intensity scored by VAS and NPRS was similar. It is important to highlight that the average pain intensities were ≥40 mm and 4 points for VAS and NPRS, respectively, in the period between 1 h and 48 h. Nevertheless, the size of the sample does not allow us to perform an appropriate subgroup analysis. But it would be interesting to analyze as a separate subgroup those patients referring high values of postoperative pain.
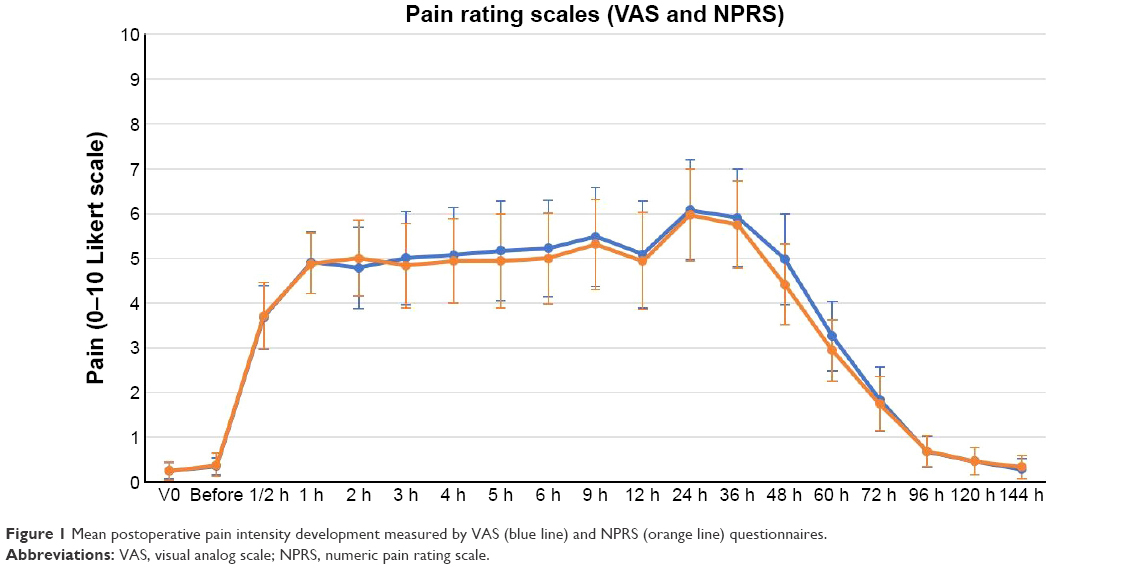 | Figure 1 Mean postoperative pain intensity development measured by VAS (blue line) and NPRS (orange line) questionnaires. |
There were no differences between females and males (Figure 2, P=0.862) (PCA) or among the different age groups (PCA, P=0.179; Figure 3) for the evolution of postoperative pain or age. Nevertheless, patients older than 30 years tended to experience greater pain intensity between 6 and 48 h after ASA, in comparison to younger patients. No relationship was found between the feeling of pain and the amount of ablation.
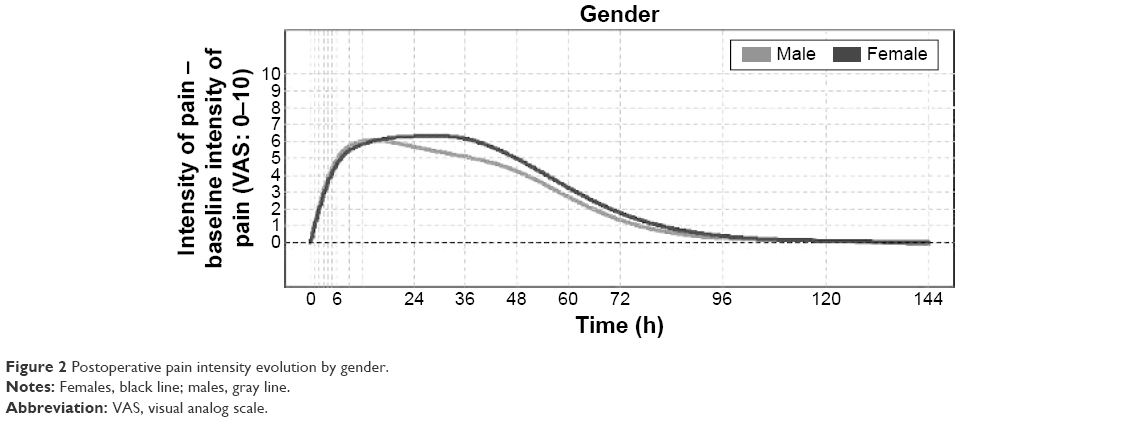 | Figure 2 Postoperative pain intensity evolution by gender. |
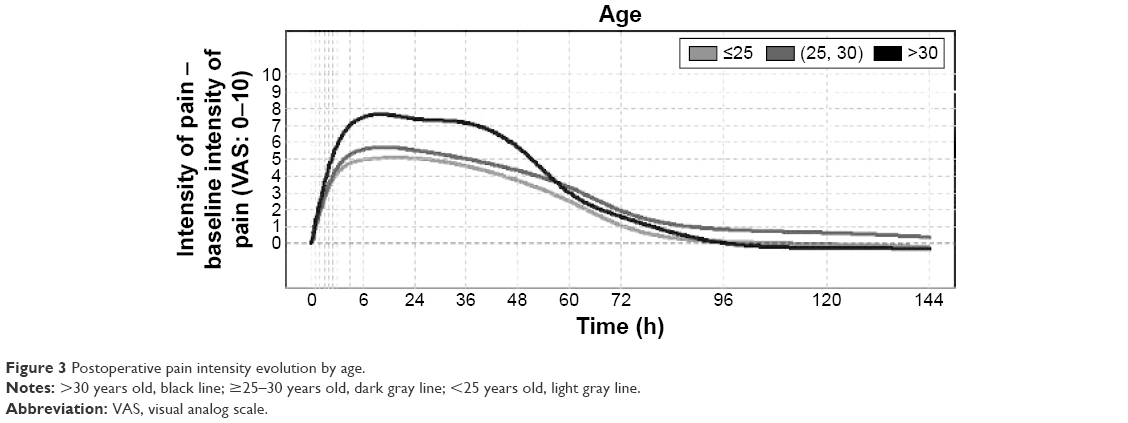 | Figure 3 Postoperative pain intensity evolution by age. |
PCA1, the first function of PCA, represents the overall pain level. This component showed that subjects with higher VAS and NPRS scores had more pain than average during the study period. The highest and lowest scores corresponded to scores that were far from the mean postoperative pain intensity evolution. PCA1 explained 78% of the total variability of the sample (Figure 4). PCA2, the second function of PCA, represents the recovery time (Figure 5). Subjects with high scores in this component took longer time to recover. Subjects with low scores reached the peak of pain 24–36 h after surgery, and they also had a faster recovery time after 48 h. PCA2 explained 12% of the total variability of the sample. Thus, PCA1 and PCA2 accounted for 90% of the total variability of the data.
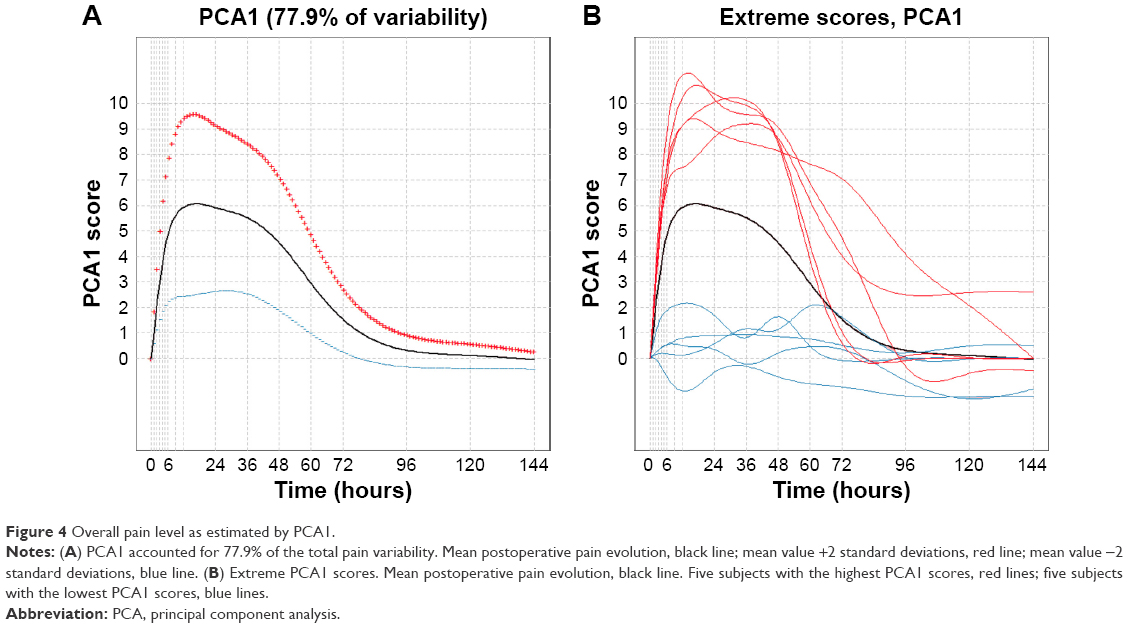 | Figure 4 Overall pain level as estimated by PCA1. |
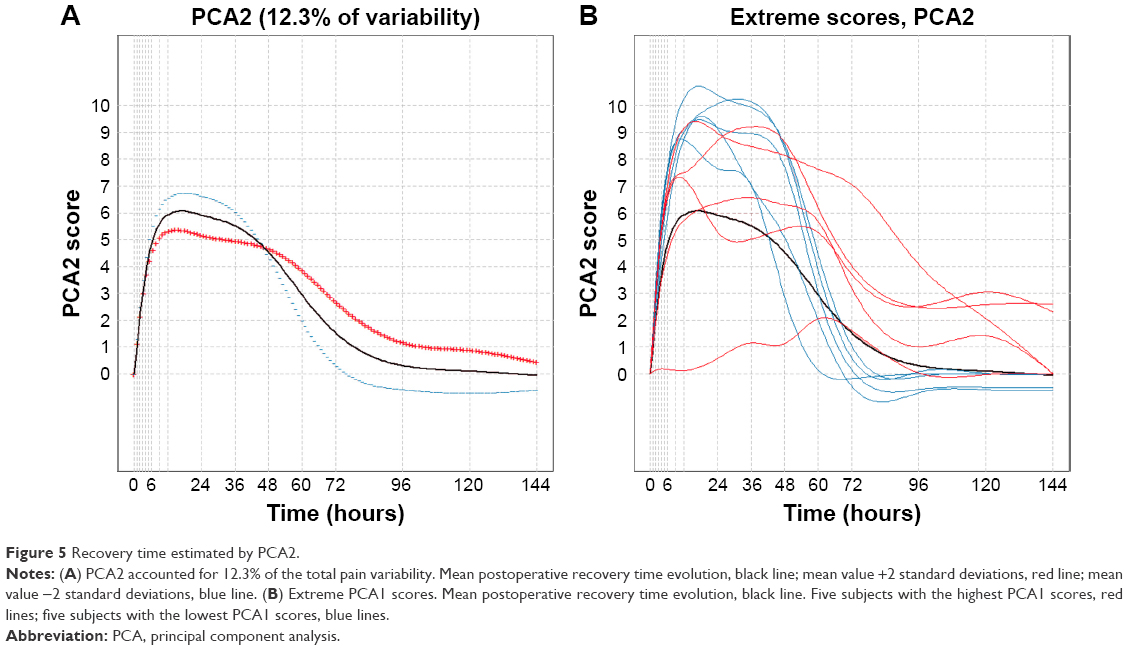 | Figure 5 Recovery time estimated by PCA2. |
All patients took oral acetaminophen (1 g) between 4 and 6 h after ASA, and then, every 8 h up to 72 h. Fourteen (44%) patients needed rescue medication. These patients presented greater pain intensity, although the difference between the VAS scores before and after ASA for patients requiring rescue medication and those not requiring the medication was not statistically significant (P=0.107, Figure 6).
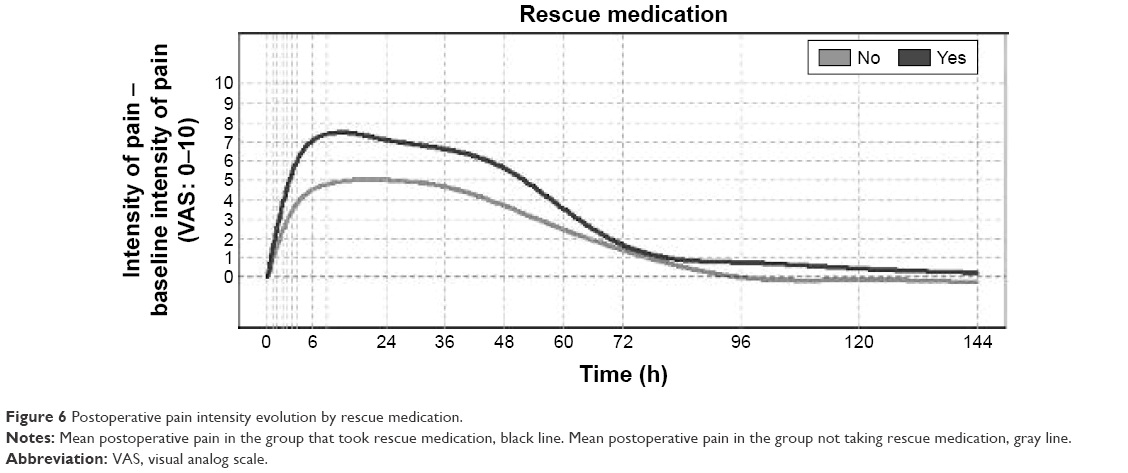 | Figure 6 Postoperative pain intensity evolution by rescue medication. |
Other ocular symptoms after ASA
Regarding other postoperative symptoms such as photophobia, burning, itching, tearing, foreign body sensation, and headache, the results are shown in Table 1. All patients had photophobia and 27 (84%) had burning sensation.
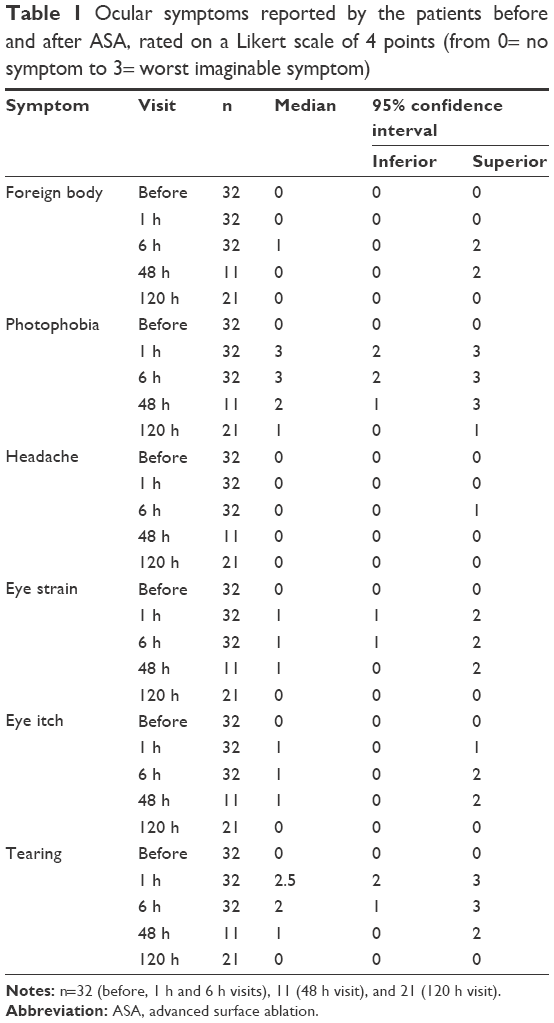 | Table 1 Ocular symptoms reported by the patients before and after ASA, rated on a Likert scale of 4 points (from 0= no symptom to 3= worst imaginable symptom) |
HAD questionnaire
Before ASA, the overall score for the HAD questionnaire was 4.4±3.6 (Figure 7). At 6 h after surgery, it was 5.4±3.9. Before surgery, 29 (91%) of the patients scored between 0 and 7, 1 (3%) scored 10, and 1 (3%) scored ≥11 in the anxiety subscale. At 6 h after surgery, all patients had anxiety scores between 0 and 7. For the depression subscale, all patients scored between 0 and 8 before surgery. Six hours after ASA, the results were similar.
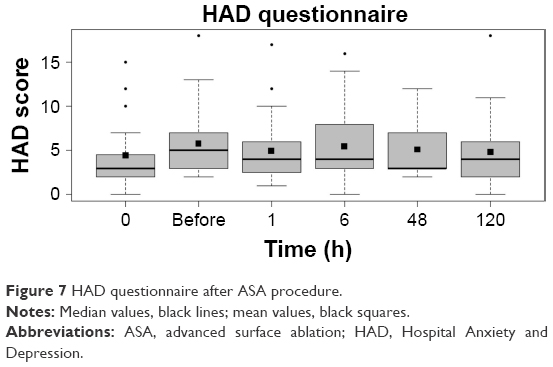 | Figure 7 HAD questionnaire after ASA procedure. |
QoL questionnaire SF12
The QoL questionnaire score was lowest at 24 h after surgery (SF12 physical component summary 38±15.9, SF12 mental component summary 50.4±11.9). At that time, it was lower than both the baseline value (P<0.0001) and the value at 72 h (P<0.008).
VF25 questionnaire
Before surgery, the score for the self-administered VF25 questionnaire was 92.4±9.6. At 24 h after surgery, the lowest score, 59.7±27.6, was recorded (P<0.001).
Adverse events
No adverse events related to the ASA procedure or the medication used in this study were reported.
Discussion
Pain from corneal origin is very severe and stressful to patients and their surgeons.2 No method of pain control has been considered ideal or universally accepted.15 Also, in our series of patients, we found that 44% of the subjects needed rescue medication. Therefore, these results deserve further research to develop new and more efficient postoperative analgesic protocols.
To the best of our knowledge, this study is the first to assess pain for 6 days following ASA and to describe the natural history of its evolution in the postoperative period. Some other studies determined if several drugs could decrease the rate of corneal re-epithelialization, but assessment of pain was not the main outcome.2,16
There were no significant differences in pain scores between males and females, and although patients over 30 years of age tended to report more pain than younger patients, the differences were not statistically significant. The pain curve measured by the VAS questionnaire increased rapidly during the first 9 h after surgery. It peaked at 24 h in the moderate to severe range, with a VAS value of 6 mm. It was then stable until 36 h, before it began to decrease until 72 h. This finding is in agreement with other studies.16–18 To avoid delayed epithelialization, our postoperative analgesic protocol did not utilize either topical nonsteroidal anti-inflammatory or other drugs. It is clear that ASA produces a direct injury of the nerves of the treated corneal area, including those of the epithelium and upper stromal layers,19,20 and pain is associated with the corneal healing process.5 Gallar et al showed that in cats, the corneal sensory fibers innervating the wounded area and surroundings are functionally altered after ASA, becoming more sensitive to pain stimuli 24–48 h after surgery.5 Thus, our clinical findings, in which the pain continued after 72 h when the cornea was healed, differ from the experimental results of Gallar et al regarding the intensity and duration of pain.
The importance of our study lies in the assessment of pain during the 6-day follow-up period in which we obtained new findings. We identified two types of responses. Some patients experienced severe pain, which reached a peak at 24–36 h after surgery. These patients had a fast recovery time from 48 h onward. The other type of patients reported light pain and a prolonged recovery. The differences between these two types of patients could be an important point to understand, so that new customized postoperative treatments can be designed.
Another important finding is that individuals with higher pain scores had higher average pain throughout the entire follow-up period. Therefore, two types of patients can be described: those more sensitive to the overall wound healing process and those more insensitive to the same. Not surprisingly, the individuals taking rescue medications had higher levels of postoperative pain than did the patients not taking rescue medication, though the differences in pain level measured by the VAS and NRPS questionnaires were not significant.
Sher et al established a distinction between pain and discomfort.21 They described discomfort as a group of symptoms characterized by photophobia, burning, tearing, and foreign body sensation. We included itching and headache to this collection of symptoms, and each was individually evaluated. Most studies only assess some of these symptoms, with photophobia being the most frequently reported. We found that after postoperative pain, photophobia was the most prevalent symptom present in all of our subjects and it reached the highest scores among all the discomfort symptoms. These results are in line with those from other reports.21–23
While the primary objective of this study was to characterize postoperative pain after ASA, we also sought to propose new clinical models for evaluating postsurgical pain. In turn, we hope that these new models would lead to improvement in the pain management protocols for patients undergoing ASA and other invasive surface treatments. ASA as a possible clinical model has some interesting features. First, the induced injury is quite homogeneous in all subjects. Second, postoperative acute ocular pain after ASA has a characteristic and reproducible evolution. Third, postoperative pain is moderate, but the relative increase is significant (0–6 on the VAS scoring system). Finally, this surgery is performed in pain-free, healthy subjects of all ages. These characteristics suggest that ASA surgery could be a useful and novel human model of acute surgical pain and, therefore, to test new pain control protocols or drugs.
Our study is subject to a series of methodological limitations. The observational design and the sample size might underestimate or overestimate the ability to generalize the results beyond the population and the conditions studied. Sample size was relatively small for some analysis, a fact that could introduce bias in our results; pain perception is highly heterogeneous and it is possible that by including larger number of patients, the results might be different. Another limitation is that all patients took oral acetaminophen (1 g) between 4 and 6 h after ASA and then every 8 h up to 72 h, and 44% of patients took rescue medication. Likewise, all patients took an anxiolytic before and after surgery. The potential impact of these analgesic and anxiolytic drugs on pain evolution was not considered in our analysis. Therefore, it is likely that pain evolution between 4 and 6 h after ASA would have been greater without these drugs. Consequently, our results might underestimate the ocular pain after ASA. In addition, we detected that demographic and psychologic factors have been identified as being important for postoperative pain in other surgical disciplines. Therefore, these should be included in future research.24 However, despite these limitations, our results support the predictable evolution of postsurgical pain after ASA as a new model for the study of acute postoperative pain and describe two patterns of painful responses.
Conclusion
Our results suggest that postoperative acute ocular pain after ASA presents a characteristic evolution with two types of patient profiles. One type experienced severe pain with rapid recovery after 48 h. The other type had light to moderate pain and a prolonged recovery time. These two types should be considered when designing new customized postoperative treatments. ASA could be a useful novel human model of acute pain for the prediction of clinical analgesia. These results justify the search for a more efficient postoperative analgesic protocol and additional research to develop personalized postoperative treatments.
Acknowledgments
This work has been supported by a grant from Instituto Universitario de Oftalmobiología Aplicada (IOBA).
Disclosure
SV received fees for collaborating with Laboratorios del Dr Esteve on pain research. The authors report no other conflicts of interest in this work.
References
Moisseiev E, Sela T, Minkev L, Varssano D. Increased preference of surface ablation over laser in situ keratomileusis between 2008–2011 is correlated to risk of ecatasia. Clin Ophthalmol. 2013;7:93–98. | ||
Woreta FA, Gupta A, Hochstetler B, Bower KS. Management of post-photorefractive keratectomy pain. Surv Ophthalmol. 2013;58(6):529–535. | ||
Netto MV, Mohan RR, Ambrosio R Jr, Hutcheon AE, Zieske JD, Wilson SE. Wound healing in the cornea: a review of refractive surgery complications and new prospects for therapy. Cornea. 2005;24(5):509–522. | ||
El-Maghraby A, Salah T, Waring GO 3rd, Klyce S, Ibrahim O. Randomized bilateral comparison of excimer laser in situ keratomileusis and photorefractive keratectomy for 2.50 to 8.00 diopters of myopia. Ophthalmology. 1999;106(3):447–457. | ||
Gallar J, Acosta MC, Gutierrez AR, Belmonte C. Impulse activity in corneal sensory nerve fibers after photorefractive keratectomy. Invest Ophthalmol Vis Sci. 2007;48(9):4033–4037. | ||
Gracely RH, Lynch SA, Bennett GJ. Painful neuropathy: altered central processing maintained dynamically by peripheral input. Pain. 1992;51(2):175–194. | ||
Beuerman RW, McDonald MB, Zhang D, Varnell RJ, Thompson HW. Diclofenac sodium attenuates neural activity after photorefractive keratectomy in rabbits. J Refract Surg. 1996;12(7):783–791. | ||
Breivik H, Borchgrevink PC, Allen SM, et al. Assessment of pain. Br J Anaesth. 2008;101(1):17–24. | ||
Lopez-Miguel A, Martinez-Almeida L, Mateo ME, Coco-Martin MB, Alio JL, Maldonado MJ. Dependability of pachymetry measurements after myopic advanced surface ablation using scanning-slit topography and specular microscopy. Invest Ophthalmol Vis Sci. 2013;54(2):1054–1060. | ||
Sobas EM, Videla S, Maldonado MJ, Pastor JC. Ocular pain and discomfort after advanced surface ablation: an ignored complaint. Clin Ophthalmol. 2015;9:1625–1632. | ||
McMonnies CW. Measurement of symptoms pre- and post-treatment of dry eye syndromes. Optom Vis Sci. 2016;93(11):1431–1437. | ||
Herrero MJ, Blanch J, Peri JM, De Pablo J, Pintor L, Bulbena A. A validation study of the Hospital Anxiety and Depression Scale (HADS) in a Spanish population. Gene Hosp Psychiatry. 2003;25(4):277–283. | ||
Mangione CM, Lee PP, Gutierrez PR, et al. Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol. 2001;119(7):1050–1058. | ||
Ramsay JO, Silverman BW. Principal components analysis for functional data. Functional Data Analysis. 2nd ed. New York: Springer; 2005:147–172. | ||
Nissman SA, Tractenberg RE, Babbar-Goel A, Pasternak JF. Oral gabapentin for the treatment of postoperative pain after photorefractive keratectomy. Am J Ophthalmol. 2008;145(4):623–629. | ||
Hong JP, Nam SM, Im CY, et al. Comparison of analgesic effect of preoperative topical diclofenac and ketorolac on postoperative pain after photorefractive keratectomy. J Cataract Refract Surg. 2014;40(10):1689–1696. | ||
Autrata R, Rehurek J. Laser-assisted subepithelial keratectomy and photorefractive keratectomy for the correction of hyperopia. Results of a 2-year follow-up. J Cataract Refract Surg. 2003;29(11):2105–2114. | ||
Blake CR, Cervantes-Castaneda RA, Macias-Rodriguez Y, Anzoulatous G, Anderson R, Chayet AS. Comparison of postoperative pain in patients following photorefractive keratectomy versus advanced surface ablation. J Cataract Refract Surg. 2005;31(7):1314–1319. | ||
Tervo K, Latvala TM, Tervo TM. Recovery of corneal innervation following photorefractive keratoablation. Arch Ophthalmol. 1994;112(11):1466–1470. | ||
Erie JC, McLaren JW, Hodge DO, Bourne WM. Recovery of corneal subbasal nerve density after PRK and LASIK. Am J Ophthalmol. 2005;140(6):1059–1064. | ||
Sher NA, Golben MR, Bond W, Trattler WB, Tauber S, Voirin TG. Topical bromfenac 0.09% vs. ketorolac 0.4% for the control of pain, photophobia, and discomfort following PRK. J Refract Surg. 2009;25(2):214–220. | ||
Sher NA, Frantz JM, Talley A, et al. Topical diclofenac in the treatment of ocular pain after excimer photorefractive keratectomy. Refract Corneal Surg. 1993;9(6):425–436. | ||
Caldwell M, Reilly C. Effects of topical nepafenac on corneal epithelial healing time and postoperative pain after PRK: a bilateral, prospective, randomized, masked trial. J Refract Surg. 2008;24(4):377–382. | ||
Lesin M, Domazet Bugarin J, Puljak L. Factors associated with postoperative pain and analgesic consumption in ophthalmic surgery: a systematic review. Surv Ophthalmol. 2015;60(3):196–203. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.