")
Back to Journals » Journal of Pain Research » Volume 13
Pain Intensity and Functional Outcomes for Activities of Daily Living, Gait and Balance in Older Adults Accessing Outpatient Rehabilitation Services: A Retrospective Study
Authors Pelletier R , Purcell-Levesque L, Girard MC , Roy PM , Leonard G
Received 3 April 2020
Accepted for publication 17 June 2020
Published 7 August 2020 Volume 2020:13 Pages 2013—2021
DOI https://doi.org/10.2147/JPR.S256700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Schatman
R Pelletier,1 L Purcell-Levesque,2 M-C Girard,2 P-M Roy,2 G Leonard2,3
1School of Rehabilitation, Faculty of Medicine, Université de Montréal, Montreal, Quebec, Canada; 2Research Center on Aging, Centre intégré universitaire de santé et de services sociaux de l’Estrie - Centre hospitalier universitaire de Sherbrooke (CIUSSS de l’Estrie - CHUS), Sherbrooke, Quebec, Canada; 3School of Rehabilitation, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, Quebec, Canada
Correspondence: G Leonard Email [email protected]
Purpose: Older adults are referred for outpatient physical therapy to improve their functional capacities. The goal of the present study was to determine if pain had an influence on functional outcomes in older adults who took part in an outpatient physical rehabilitation program.
Patients and Methods: A retrospective study was performed on the medical records of patients aged 65 and over referred for outpatient physical therapy to improve physical functioning (n=178). Pain intensity (11-point numeric pain scale) and results from functional outcome measures (Timed Up and Go [TUG], Berg Balance Scale [BBS], 10-meter walk test, 6-minute walk test and Functional Autonomy Measuring System [SMAF]) were extracted at initial (T1) and final (T2) consultations. Paired t-tests were performed to determine if there were differences in functional outcome measures between T1 and T2 in all the patients. Patients were stratified to those with pain (PAIN, n=136) and those without pain (NO PAIN, n=42). Differences in functional outcome measures between T1 and T2 (delta scores) were compared between groups with independent t-tests with Welch corrections for unequal variances. Pearson correlation coefficients between initial pain intensity and changes in functional outcome measures (T2-T1) were also performed. Correcting for multiple comparisons, a p-value of p≤ 0.01 was considered as statistically significant.
Results: The TUG, BBS, 10-meter walk test, 6-minute walk test all demonstrated improvement between T1 and T2 (all p< 0.01). There was no difference between groups for delta scores for TUG (p=0.14), BBS (p=0.03), 10-meter walk test (p=0.54), 6-minute walk test (p=0.94) and SMAF (p=0.23). Pearson correlation coefficients were weak between initial pain intensity and changes in functional outcome scores between T1 and T2 (r= − 0.16 to 0.15, all p-values > 0.10).
Conclusion: These results suggest that pain is not an impediment to functional improvements in older individuals who participated in an outpatient physical rehabilitation program.
Keywords: pain, function, physical therapy, older adults, disability
Introduction
Musculoskeletal conditions are a leading cause of pain and disability.1 The ICD-11 defines chronic musculoskeletal pain as “persistent or recurrent pain that arises as part of a disease process directly affecting bone(s), joint(s), muscle(s) or related soft tissue”.2 Chronic pain is a major public health problem affecting almost one-third of older adults in Canada.3 Older adults living with chronic pain experience greater levels of depression and anxiety and decreased quality of life when compared with those living without pain.4–6 In older adults, chronic musculoskeletal conditions and pain are also associated with important health implications, including decreased physical activity and mobility, reduced cognitive function and an increased risk of falls.7
Pain intensity has been associated with an increased risk of falls,8 altered movement patterns,9 and an increased risk of chronic pain.10 Pain is associated with changes in motor control and activation. These changes include altered muscular activity, both within agonist and between synergistic muscles, increased co-contraction, decreased maximum voluntary contraction, and decreased muscular endurance.11–14 There is evidence that pain may affect corticospinal projections and interfere with motor learning15–20 important for improving functional outcomes in rehabilitation.21,22 Pain, motor learning, altered movement patterns, and function appear to be interrelated variables that impact motor performance and are targeted in physical rehabilitation treatments.
As pain affects motor control and motor learning, it is also possible that it could impede functional gains. If pain affects motor control and motor learning and results in poorer functional outcomes, we should observe that patients with pain who participated in a physical rehabilitation outpatient program demonstrate decreased functional gains when compared to individuals with no pain. The goal of the present study was to determine if pain impacted functional improvement in older adult patients who engaged in an outpatient physical rehabilitation program. We hypothesized that all older patients having participated in an outpatient physical therapy program would demonstrate improvement in functional outcomes. However, we also hypothesized that patients with pain would demonstrate less functional improvement compared to patients without pain.
Patients and Methods
Study Design
This is a descriptive retrospective study of information extracted from the medical records of patients who attended the outpatient rehabilitation facility at the Integrated University Health and Social Services Centre – University Institute of Geriatrics of Sherbrooke (CIUSSS-IUGS), Youville Pavilion, in Sherbrooke, Quebec, Canada. All the medical records of patients treated at the outpatient clinic in 2014 were examined by a member of the research team. Inclusion criteria were to have participated in an outpatient physical therapy program after referral by a physician for difficulty in performing functional activities of daily living and to be over 65 years of age. Exclusion criteria were a Mini Mental State Exam (MMSE) score of <24. Although several persons referred for outpatient rehabilitation experience pain, the goal of physical therapy treatments provided in the outpatient facility for the older adults were to improve function as well as to maintain functional levels of autonomy. Physical therapy treatments were typically offered 1–2 times per week over a 12-week period. Physical therapy treatments were individually adapted and tailored to functional limitations revealed when establishing medical history and during the physical examination, as well as from the information provided by the referring physician. Typically, physical therapy treatments consisted in exercises to improve motor control, strength and conditioning, balance, and functional abilities. In compliance with the Declaration of Helsinki and with the Canadian Tri-Council Policy Statement (TPCS-2 2018) the research protocol was evaluated and approved by the institutional research ethics committee of the CIUSSS-IUGS review board (CER#2016-638). The ethics review board waived the obligation to obtain consent from participants due to the retrospective nature of the study. In Quebec, the Act respecting health services and social services provides that the director of professional services of an institution can authorize a professional to examine a medical record for research purposes. To ensure patient confidentiality access to the medical records was limited to only one member of the research team who transcribed the necessary data for the study. Furthermore, the data were linked to a participant number and no identifiable information was recorded.
Study Variables
Information was extracted from the patients’ medical records by the research assistant (MCG), including: age at the start of rehabilitation, gender, average and maximum pain intensity (on a 0–10 numeric scale; 0=no pain; 10=worst possible pain) during the last 24 hours,23 pain localisation, and number of physical therapy treatments.
A series of functional measures commonly utilized by rehabilitation professionals were extracted from the patients’ medical records. Information regarding walking aids used when performing functional tests was also recorded. The functional measures included:
- Physical function related to walking was the main outcome variable and was evaluated with the 10-meter walk test measured in seconds and the 6-minute walk test measured in meters.24,25 The 10-meter walk test (ICC=0.82)26 and the 6-minute walk test (ICC=0.95–0.97)25 have excellent test–retest reliability in older adults. There is adequate validity for the 10-meter walk test (r=0.54–0.58)27 and the 6-minute walk test (r=0.52–0.73)24 with measures of physical function. Minimal clinically significant differences for the 10-meter walk test and 6-minute walk test are 0.5 m/sec and 19–22 meters, respectively.28
- Balance was measured with Berg Balance Scale (BBS) and Timed Up and Go (TUG) test, two frequently utilized tests in clinical rehabilitation settings with older adults.25 The BBS is comprised of 14 items and measures static balance and risk of falls. Total score ranges from 0 to 56, with a higher scores indicating better function (0–56). Validity (r=0.67) and reliability (ICC=0.91–0.97) of the BBS are well established29,30 and its use to assess balance generates consensus.31 The TUG test assesses mobility and is measured in seconds. Values greater than 12 seconds indicate an elevated risk of falls. Validity (r=−0.61 to −0.81) and reliability (ICC=0.97) of the TUG test are also well documented.32,33 Minimal clinically significant differences for the BBS and the TUG are 6.534 and 0.8 to 3.0 seconds,35 respectively. Values on the BBS below 4037 and TUG values greater than 13.5 seconds36 are associated with an increased risk of falling in older adults.
- Functional autonomy was measured with the Functional Autonomy Measuring System (SMAF). The SMAF is a measuring tool developed from the World Health Organisation classification of disabilities and assesses functional abilities across 29 items, including activities of daily living (7 items), mobility (6 items), communication (3 items), mental functions (5 items) and instrumental activities of daily living (8 items).37 This tool provides a total score, as well as sub-scores for each domain. The SMAF utilizes a negative scoring system with scores closer to zero indicative of better functioning. SMAF’s validity (r=0.88) and reliability (ICC=0.78–0.96) are established.37–39
Statistical Analysis
Data were analyzed with GraphPad Prism 8 (GraphPad Software Inc., La Jolla, CA, USA) software. To test for improvement in functional outcomes (TUG, BBS, 10-meter walk test, 6-minute walk test and SMAF), the differences in outcome measures in all patients between T1 and T2 were compared with paired t-tests. Patients were stratified into two groups, those with pain (PAIN) and those without pain (NO PAIN). Baseline values for age, gender, number of physical therapy treatments and measures of function were compared with independent t-tests with Welch corrections for unequal variances. To determine if there were differences between groups for improvement in the functional measures taken before discharge (T2) and baseline measures (T1), values were compared with independent t-tests with Welch corrections for unequal variances. As there was a substantial difference in the number of participants between the PAIN and NO PAIN groups, within-group analyses were not performed for outcome measures between T2 and T1 to avoid any misinterpretation related to issues of statistical power. Pearson correlation coefficients were also performed for all patients between measures of pain severity and changes in functional outcome measures between T2 and T1.
Adjustments for multiple comparisons were made using the False Discovery Rate Benjamini-Hochberg procedure with an α<0.05.40,41 After making corrections for multiple comparisons, only p values ≤0.01 were considered to be statistically significant.
Results
One hundred and seventy-eight (178) files were retrieved. There were 103 females and 75 males (see baseline measures for all participants in Table 1). Comparisons between functional outcome measures between T1 and T2 in all patients indicated that TUG, BBS, 10-meter walk test, and 6-minute walk test all demonstrated statistically significant improvement (Table 2). There was no improvement in the SMAF scores. The differences between initial and final scores for the 10-meter walk test and the 6-minute walk test were greater than minimal clinically significant differences in both groups; however, these were considered as small.28 Differences between initial and final scores for the BBS were less than the minimal clinically significant difference in older adults34 and values remained above mean values and cut-off values for a greater risk of falls in this population.42 The differences between initial and final scores for the TUG were greater than the minimal clinically significant differences in older age clinical populations in both groups35 but values at T2 still were associated with a greater risk of falling36 and above normative values for this population.25
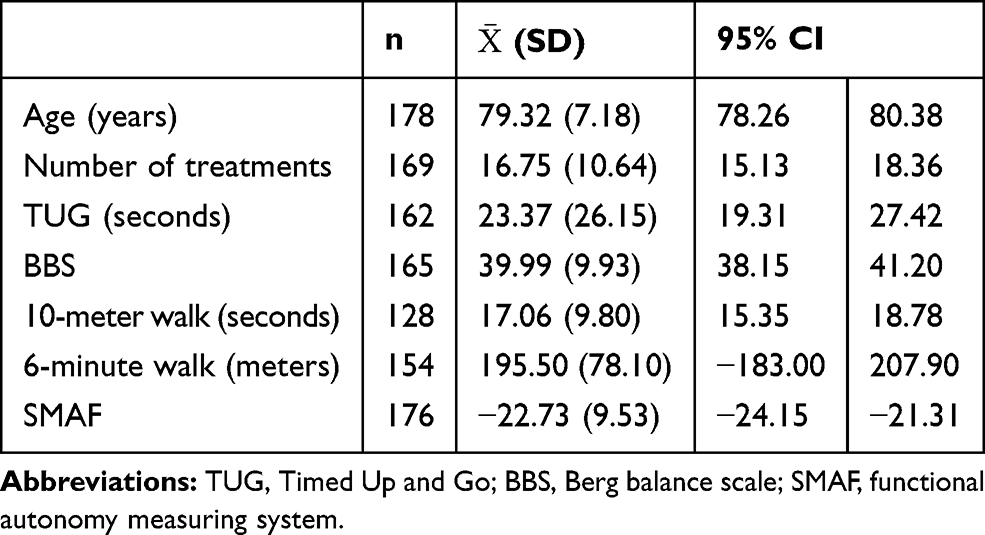 |
Table 1 Baseline Measures and Number of Treatments for All Participants |
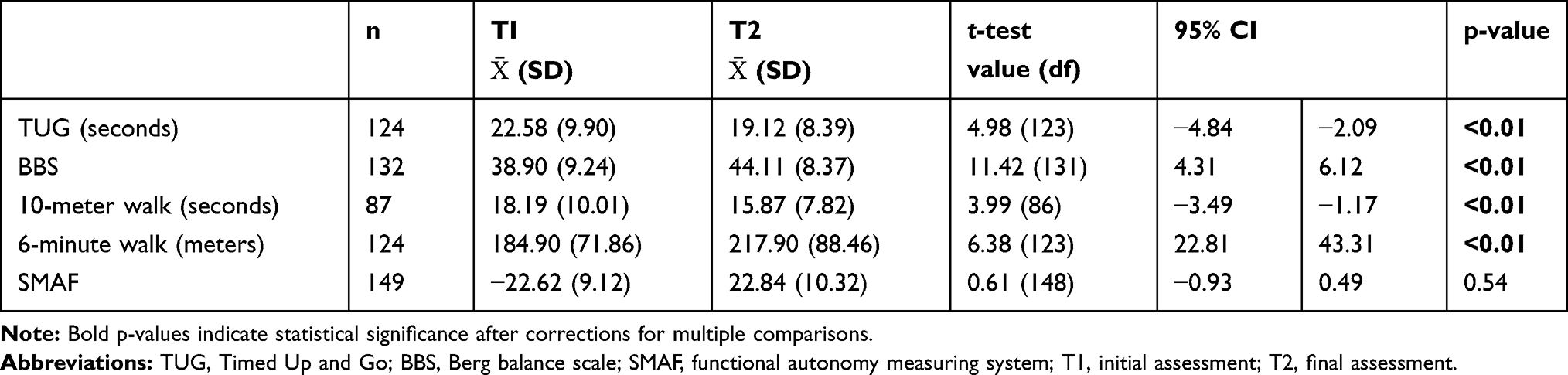 |
Table 2 Differences Between Final and Initial Outcome Measures in All Patients |
Patient data were stratified into two groups, PAIN and NO PAIN. Baseline values were similar for both groups (Table 3). Patients in the PAIN group had more physical therapy sessions than the NO PAIN group and better SMAF scores. Pain intensity levels did not change in the PAIN group between baseline (T1; 6.47 ± 2.31) and prior to discharge (T2; 6.11 ± 2.27) over the period of treatment (t = 0.98, df = 69, p=0.33).
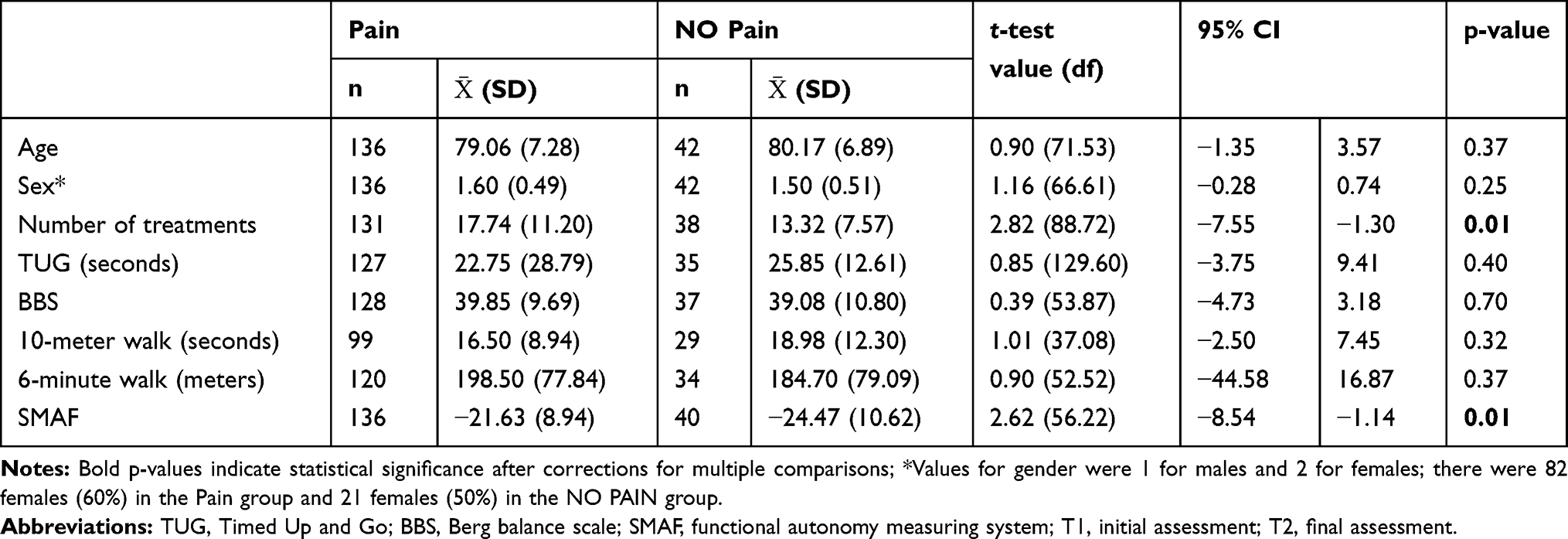 |
Table 3 Baseline Measures and Number of Treatments with Participants Stratified into those with Pain (PAIN) and those without Pain (NO PAIN) |
There were no differences between baseline and final measurements (T2-T1) between groups after correcting for multiple comparisons (Table 4). Correlations between pain intensity and changes in functional outcome scores were weak and not statistically significant (see Table 5).
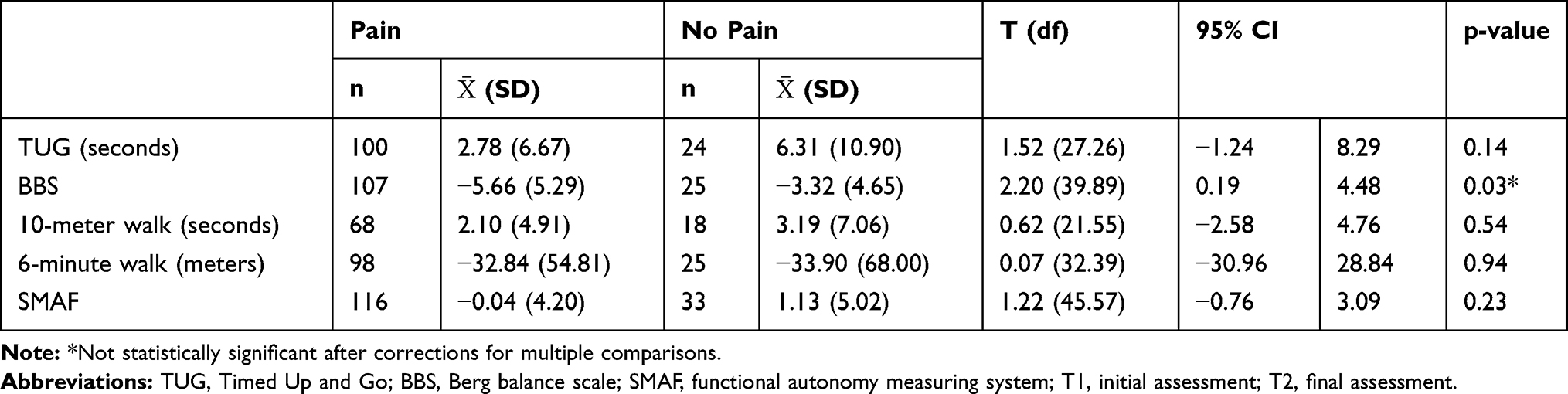 |
Table 4 Differences Between Final (T2) and Initial (T1) Measures Between Groups |
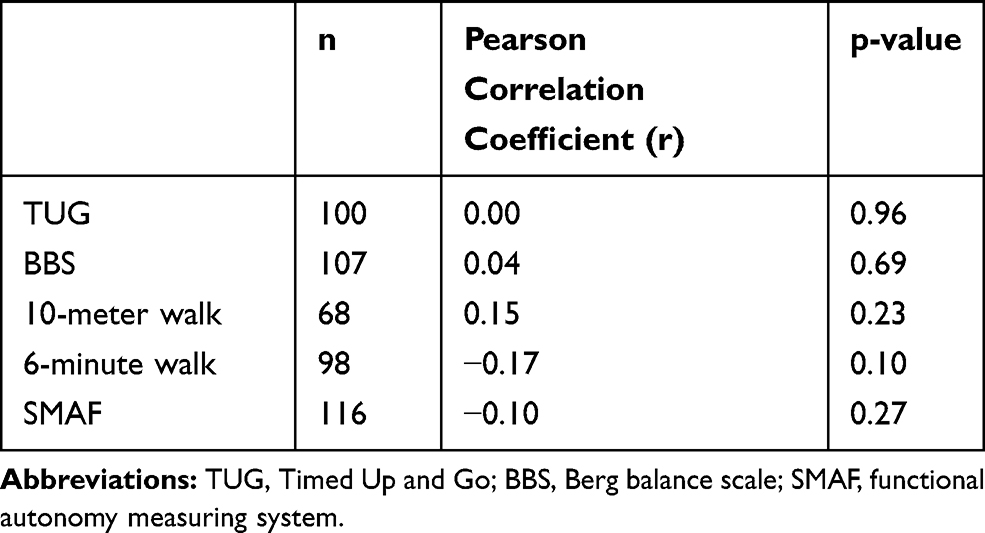 |
Table 5 Pearson Product Correlations Between Pain Intensity and Changes in Functional Outcome Measures Between Final (T2) and Baseline (T1) Evaluations for Patients in the PAIN Group |
Discussion
The purpose of the study was to determine if initial pain intensity was associated with poorer functional outcomes in older patients who participated in an outpatient physical rehabilitation program. It was hypothesized that older persons with pain who participated in such a program would demonstrate less improvement in measures of balance, gait, and functional abilities compared to older persons without pain. Collectively, all patients demonstrated small but statistically significant changes in the outcome measures. Baseline measures were similar between persons with and without pain except for the SMAF scores (patients without pain had lower scores, suggesting slightly better function). The number of treatments received were grearter in the PAIN group. There were no statistically significant differences in the improvement of outcome measures between persons with pain and those without pain. Contrary to the hypothesis, initial pain intensity levels were not associated with decreased improvement in functional outcomes. These findings have important clinical implications, as initial pain intensity levels do not appear to be a prognostic factor of clinical functional improvement and do not appear to hinder performance gains in functional measures of gait and balance.
Pain Intensity and Functional Outcomes
Research has clearly demonstrated that pain results in altered movement and behaviors that range from subtle differences to complete avoidance.9 There is evidence to suggest that pain intensity may be a prognostic factor for negative outcomes in persons with musculoskeletal conditions.10 In a pooled analysis of studies involving adults of various ages with non-specific low back pain, greater baseline pain intensity was associated with a poorer prognosis for long-term pain outcomes and increased activity limitations and participation restrictions.43 Persons with poorer outcomes associated with non-specific low back pain (pain maintenance, increased activity limitations and participation restriction) were 1.45 times more likely to have had higher baseline pain intensity levels, suggesting a relatively weak, but nonetheless negative relationship between pain intensity and long-term outcomes. In older adult patients, greater pain intensity levels have also been associated with higher fall rates.8,44 Foot pain has also been associated with decreased balance and changes in gait parameters, including the 6-meter walk test in community-dwelling older adults.45 Even neck pain in older persons has been associated with decreases in gait parameters, including decreased walking speed and cadence and increased time to complete the 10-meter walk test.46 In a study investigating the effect of a behavioral medicine approach of physical therapy that addresses physical function and psychosocial factors for older adults with chronic pain, it was noted that such a program resulted in a greater decrease in pain severity, as well as greater improvements in physical activity, health-related quality of life and self-efficacy in the intervention group, compared to the control group.47 Interestingly, and similar to the results in the present study, both persons in the intervention and control group demonstrated significant improvements in physical function.47 In the present study, the functional gains measured for gait, balance and functional autonomy following outpatient rehabilitation were not associated with initial pain levels. The changes in the values of the outcome measures between T1 and T2 were similar between the groups. Collectively, these findings suggest that pain does not hinder improvements in functional outcomes for older individuals who participated in the outpatient physical therapy program. However, addressing pain in older adults remains important to improve quality of life and increase physical activity.47
Pain, Motor Learning and Functional Outcomes
We hypothesized that pain would impact functional outcomes in older persons referred for physical therapy to improve function. We had hypothesized that pain would interfere with functional progressions as experimental and clinical pain is associated with motor control and performance changes.11–14 Motor control changes associated with pain include a decrease in maximal voluntary contractions, reorganisation of muscle recruitment both within and between muscles, and decreased muscle endurance during submaximal contractions.11–14 Furthermore, pain may affect motor learning16–22 that appears to be important to improve functional outcomes in rehabilitation.21
A lack of association between pain intensity and functional outcomes in the present study suggest that pain intensity was not an impediment to motor learning. Although several studies in participants with experimentally induced pain have suggested that pain may interfere with motor learning,15–22 there are studies that also suggest that acute pain has no effect49 or may actually enhance motor learning.50–52 In one of these studies, young adults were assessed in the performance of a complex motor task involving tracing sequences of sinusoidal wave functions of different amplitudes and varying frequencies.52 One group had capsaicin (experimental pain) applied to the elbow during motor learning practice while the control group did not. Motor task performance was improved in both groups after initial motor learning practice and when assessing motor retention 24–48 hours later. However, the group with capsaicin applied to the elbow demonstrated greater performance gains compared to the control group. It was suggested by the researchers that experimentally induced pain could increase attention to the body part utilized in the task, which resulted in a better performance.52 Indeed, the importance of attention in motor learning is well documented in the literature.53 Attentional bias has been found towards both pain-related words/pictures54 and towards painful sensory stimuli in persons with chronic pain.55 It is possible that chronic musculoskeletal pain mobilises attentional resources,54 having a positive effect on motor learning in some circumstances.56
There are also studies indicating that clinical pain may not hinder motor learning. A study assessing motor skill learning in participants with hand osteoarthritis found that the participants performed more poorly at the onset of the motor skill task, but had greater improvement over time compared to participants in the control group (no pain), suggestive of increased motor skill learning.57 Although the most painful hand was utilized for the motor skill task, neither pain intensity values before or during the training of the hand in the participants were recorded, so the association of pain intensity with motor performance was not elaborated. However, results from the study do indicate that older persons with arthritic pain are capable of motor learning and improved motor performance.57 In another study by Krebs et al (2007) with older adults, progressive resistance and functional training were associated with better performance and reduced fall‐related behaviors compared to a placebo control group that did not receive balance and functional training.58 Functional training resulted in greater improvement in gait parameters than strength training.58 In a study conducted by Heuninckx et al (2008) involving complex interlimb coordination tasks, there was increased activation in higher sensorimotor and frontal brain areas compared to younger adults, and these activation changes were associated with improved performance.59 Here again, the studies of Krebs et al (2007) and Heuninckx et al (2008) did not include pain measures, limiting any conclusion about the impact of pain on functional and sensorimotor changes. However, their results suggest that the acquisition of complex motor tasks in older adults is associated with the increased neural activation of sensorimotor and cognitive areas and functional improvement in gait and balance, highlighting the beneficial effect that this type of training can have in older adults.
Strength, Self-Efficacy, and Functional Outcomes
The finding from the present study that pain was not an impediment to improved functional outcomes for gait and balance may also suggest that other factors besides learning and attention allocation were involved. For example, in the study by Krebs et al (2007) described above, the authors found both strength training and functional training to be associated with improvement gains in gait parameters in older adult patients,58 suggesting that strength gains alone can be sufficient to enhance function. Strength gains have also been associated with improved gait speed and chair rising,60 as well as a decreased risk of falls in older adults.61 Importantly, the presence of pain does not appear to prevent strength gains, as studies have demonstrated that resistance exercises can increase strength in older adults suffering from clinical pain conditions.62,63 The relationship between pain and disability also appears to be weaker in older than in younger adults, and may, therefore, interfere less with functional performance gains.64 Increased self-efficacy, the perceived ability to manage their condition, has also been associated with better gait performance in older persons with knee osteoarthritis.65 Self-efficacy, measured with the self-efficacy for exercise scale, has been found to partially mediate the relationship between rehabilitation and functional outcomes following hip fractures,66 and between physical activity and function in general in older adults.67 A behavioral medicine physical therapy intervention in older adults with chronic pain resulted in significantly increased self-efficacy in relation to goal behavior to improve function and physical activities.47 Taken together, these observations suggest that alternative mechanisms, which are independent of motor learning and presumably unaffected by pain levels, could be involved in the functional improvements found within the present study.
Limitations
Several limitations should be considered when interpreting the data. This was a retrospective study where information was extracted from patients’ medical files. No pain measures were captured while performing the physical therapy treatments. It is also important to acknowledge that interventions likely varied across physical therapists. No direct measure of motor learning was performed. However, these limitations do not alter the findings that functional improvements were equally present in persons with and without pain, which was the principal objective of the study. There is no indication of which factors were responsible for the improvements in function. That was, however, not the focus of the study. Given that differences between functional outcome measures for all participants were statistically significant, but the effects were clinically small, the possibility of Type II errors cannot be discarded. The absence of a statistically significant difference between groups suggests that the study may have been underpowered. However, the differences in means between the delta scores on the outcome measures would have remained small and non-clinically significant.
Future studies should be prospective in design, have determined protocols for physical rehabilitation, measure pain intensity during the performance of functional movements,68 involve the measurement of motor learning, and assess other related measures that may be associated with functional improvement (i.e. attention allocation, strength and self-efficacy) and with pain that have been shown to impact movement and function (i.e. fear-avoidance and pain catastrophizing).
Conclusion
The study found that the presence of pain did not hinder improvements in functional measures of balance and gait in older individuals having received physical therapy treatments to improve function and autonomy. These findings have clinical implications. Initial pain intensity does not appear to be a useful measure in determining the prognosis in older adults with chronic musculoskeletal conditions accessing outpatient physical rehabilitation. Improvements in physical functioning, including in gait and balance, can occur in the presence of pain and may not be associated with changes in pain intensity.
Abbreviations
BBS, Berg Balance Scale; SMAF, Functional Autonomy Measuring System; TUG, Timed UpP and Go; T1, initial assessment; T2, final assessment.
Disclosure
This work was supported by a grant from the Fondation Vitae of the CIUSSS de l’Estrie - CHUS. Guillaume Léonard is supported by FRQS (Quebec). The authors report no other conflicts of interest in this work.
References
1. Briggs AM, Cross MJ, Hoy DG, et al. Musculoskeletal health conditions represent a global threat to healthy aging: a report for the 2015 world health organization world report on ageing and health. Gerontologist. 2016;56:S243–55. doi:10.1093/geront/gnw002
2. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
3. Ramage-Morin PL. Chronic pain in Canadian seniors. Health Rep. 2008;19(1):37–52.
4. Creighton AS, Davison TE, Kissane DW. The correlates of anxiety among older adults in nursing homes and other residential aged care facilities: a systematic review. Int J Geriatr Psychiatry. 2017;32(2):141–154. doi:10.1002/gps.4604
5. Zis P, Daskalaki A, Bountouni I, Sykioti P, Varrassi G, Paladini A. Depression and chronic pain in the elderly: links and management challenges. Clin Interv Aging. 2017;12:709–720. doi:10.2147/CIA.S113576
6. Goffaux P, Leonard G, Levesque M. Perception de la douleur et santé mentale. In: Marchand S, Saravane D, Gaumond I, editors. Santé mentale et douleur. Paris: Springer; 2013:37–52.
7. Blyth FM, Noguchi N. Chronic musculoskeletal pain and its impact on older people. Best Pract Res Clin Rheumatol. 2017;31(2):160–168. doi:10.1016/j.berh.2017.10.004
8. Leveille SG, Jones RN, Kiely DK, et al. Chronic musculoskeletal pain and the occurrence of falls in an older population. JAMA. 2009;302(20):2214–2221. doi:10.1001/jama.2009.1738
9. Hodges PW, Smeets RJ. Interaction between pain, movement, and physical activity: short-term benefits, long-term consequences, and targets for treatment. Clin J Pain. 2015;31(2):97–107. doi:10.1097/AJP.0000000000000098
10. Potter RG, Jones JM, Boardman AP. A prospective study of primary care patients with musculoskeletal pain: the identification of predictive factors for chronicity. Br J Gen Pract. 2000;50(452):225–227.
11. Graven-Nielsen T, Arendt-Nielsen L. Impact of clinical and experimental pain on muscle strength and activity. Curr Rheumatol Rep. 2008;10(6):475–481. doi:10.1007/s11926-008-0078-6
12. Arendt-Nielsen L, Graven-Nielsen T. Muscle pain: sensory implications and interaction with motor control. Clin J Pain. 2008;24(4):291–298. doi:10.1097/AJP.0b013e31815b608f
13. Hodges PW, Tucker K. Moving differently in pain: a new theory to explain the adaptation to pain. Pain. 2011;152(3 Suppl):S90–8. doi:10.1016/j.pain.2010.10.020
14. Bank PJ, Peper CE, Marinus J, Beek PJ, van Hilten JJ. Motor consequences of experimentally induced limb pain: a systematic review. Eur J Pain. 2013;17(2):145–157. doi:10.1002/j.1532-2149.2012.00186.x
15. Martel M, Harvey MP, Houde F, Balg F, Goffaux P, Leonard G. Unravelling the effect of experimental pain on the corticomotor system using transcranial magnetic stimulation and electroencephalography. Exp Brain Res. 2017;235(4):1223–1231. doi:10.1007/s00221-017-4880-0
16. Masse-Alarie H, Beaulieu LD, Preuss R, Schneider C. Corticomotor control of lumbar multifidus muscles is impaired in chronic low back pain: concurrent evidence from ultrasound imaging and double-pulse transcranial magnetic stimulation. Exp Brain Res. 2016;234(4):1033–1045. doi:10.1007/s00221-015-4528-x
17. Pelletier R, Higgins J, Bourbonnais D. Is neuroplasticity in the central nervous system the missing link to our understanding of chronic musculoskeletal disorders? BMC Musculoskelet Disord. 2015;16:25. doi:10.1186/s12891-015-0480-y
18. Bouffard J, Bouyer LJ, Roy JS, Mercier C. Tonic pain experienced during locomotor training impairs retention despite normal performance during acquisition. J Neurosci. 2014;34(28):9190–9195. doi:10.1523/JNEUROSCI.5303-13.2014
19. Lamothe M, Roy JS, Bouffard J, Gagne M, Bouyer LJ, Mercier C. Effect of tonic pain on motor acquisition and retention while learning to reach in a force field. PLoS One. 2014;9(6):e99159. doi:10.1371/journal.pone.0099159
20. Boudreau S, Romaniello A, Wang K, Svensson P, Sessle BJ, Arendt-Nielsen L. The effects of intra-oral pain on motor cortex neuroplasticity associated with short-term novel tongue-protrusion training in humans. Pain. 2007;132(1–2):169–178. doi:10.1016/j.pain.2007.07.019
21. Snodgrass SJ, Heneghan NR, Tsao H, Stanwell P, Rivett DA, van Vliet PM. Recognising neuroplasticity in musculoskeletal rehabilitation: A basis for greater collaboration between musculoskeletal and neurological physiotherapists. Man Ther. 2014;19(6):614–617. doi: 10.1016/j.math.2014.01.006
22. Boudreau SA, Farina D, Falla D. The role of motor learning and neuroplasticity in designing rehabilitation approaches for musculoskeletal pain disorders. Man Ther. 2010;15(5):410–414. doi:10.1016/j.math.2010.05.008
23. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
24. Harada ND, Chiu V, Stewart AL. Mobility-related function in older adults: assessment with a 6-minute walk test. Arch Phys Med Rehabil. 1999;80(7):837–841. doi:10.1016/S0003-9993(99)90236-8
25. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: six-minute walk test, berg balance scale, timed up & go test, and gait speeds. Phys Ther. 2002;82(2):128–137. doi:10.1093/ptj/82.2.128
26. Hollman JH, Beckman BA, Brandt RA, Merriwether EN, Williams RT, Nordrum JT. Minimum detectable change in gait velocity during acute rehabilitation following hip fracture. J Geriatr Phys Ther. 2008;31(2):53–56. doi:10.1519/00139143-200831020-00003
27. Latham NK, Mehta V, Nguyen AM, et al. Performance-based or self-report measures of physical function: which should be used in clinical trials of hip fracture patients? Arch Phys Med Rehabil. 2008;89(11):2146–2155. doi:10.1016/j.apmr.2008.04.016
28. Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743–749. doi:10.1111/j.1532-5415.2006.00701.x
29. Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health. 1992;83(Suppl 2):S7–11.
30. Berg KO, Maki BE, Williams JI, Holliday PJ, Wood-Dauphinee SL. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil. 1992;73(11):1073–1080.
31. Tremblay LE, savard J, Casimiro L, Tremblay M. Répertoire des outils d’évaluation en français pour la réadaptation. Ottawa (ON): Centre franco-ontarien de ressources pédagogiques; 2004.
32. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the “get-up and go” test. Arch Phys Med Rehabil. 1986;67(6):387–389.
33. Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
34. Romero S, Bishop MD, Velozo CA, Light KE. Minimum detectable change of the berg balance scale and dynamic gait index in older persons at risk for falling. J Geriatr Phys Ther. 2011;34(3):131–137. doi:10.1519/JPT.0b013e3182048006
35. Flansbjer UB, Holmback AM, Downham D, Patten C, Lexell J. Reliability of gait performance tests in men and women with hemiparesis after stroke. J Rehabil Med. 2005;37(2):75–82. doi:10.1080/16501970410017215
36. Shumway-Cook S, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys Ther. 2000;80(9):896–903. doi:10.1093/ptj/80.9.896
37. Hébert R, Carrier R, Bilodeau A. The functional autonomy measurement system (SMAF): description and validation of an instrument for the measurement of handicaps. Age Ageing. 1988;17(5):293–302. doi:10.1093/ageing/17.5.293
38. Desrosiers J, Bravo G, Hebert R, Dubuc N. Reliability of the revised functional autonomy measurement system (SMAF) for epidemiological research. Age Ageing. 1995;24(5):402–406. doi:10.1093/ageing/24.5.402
39. Hebert R, Guilbault J, Desrosiers J, Dubuc N. The functional autonomy measurement system (SMAF): a clinical-based instrument for measuring disabilities and handicaps in older people. J Can Geriatr Soc. 2001;4:141–147.
40. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Series B. 1995;57:289–300. doi:10.1111/j.2517-6161.1995.tb02031.x
41. Verhoeven KJF, Simonsen KL, McIntyre LM. Implementing false discovery rate control: increasing your power. Oikos. 2005;108(3):643–647. doi:10.1111/j.0030-1299.2005.13727.x
42. Shumway-Cook A, Baldwin M, Polissar NL, Gruber W. Predicting the probability for falls in community-dwelling older adults. Phys Ther. 1997;77(8):812–819. doi:10.1093/ptj/77.8.812
43. Kent PM, Keating JL. Can we predict poor recovery from recent-onset nonspecific low back pain? A systematic review. Man Ther. 2008;13(1):12–28. doi:10.1016/j.math.2007.05.009
44. Stubbs B, Binnekade T, Eggermont L, Sepehry AA, Patchay S, Schofield P. Pain and the risk for falls in community-dwelling older adults: systematic review and meta-analysis. Arch Phys Med Rehabil. 2014;95(1):175–87 e9. doi:10.1016/j.apmr.2013.08.241
45. Menz HB, Lord SR. Foot pain impairs balance and functional ability in community-dwelling older people. J Am Podiatr Med Assoc. 2001;91(5):222–229. doi:10.7547/87507315-91-5-222
46. Poole E, Treleaven J, Jull G. The influence of neck pain on balance and gait parameters in community-dwelling elders. Man Ther. 2008;13(4):317–324. doi:10.1016/j.math.2007.02.002
47. Cederbom S, Leveille SG, Bergland A. Effects of a behavioral medicine intervention on pain, health, and behavior among community-dwelling older adults: a randomized controlled trial. Clin Interv Aging. 2019;14:1207. doi:10.2147/CIA.S208102
48. Pelletier R, Higgins J, Bourbonnais D. Addressing neuroplastic changes in distributed areas of the nervous system associated with chronic musculoskeletal disorders. Phys Ther. 2015;95(11):1582–1591. doi:10.2522/ptj.20140575
49. Ingham D, Tucker KJ, Tsao H, Hodges PW. The effect of pain on training-induced plasticity of the corticomotor system. Eur J Pain. 2011;15(10):1028–1034. doi:10.1016/j.ejpain.2011.04.006
50. Dancey E, Murphy B, Srbely J, Yielder P. The effect of experimental pain on motor training performance and sensorimotor integration. Exp Brain Res. 2014;232(9):2879–2889. doi:10.1007/s00221-014-3966-1
51. Dancey E, Murphy BA, Andrew D, Yielder P. The effect of local vs remote experimental pain on motor learning and sensorimotor integration using a complex typing task. Pain. 2016;157(8):1682–1695. doi:10.1097/j.pain.0000000000000570
52. Dancey E, Murphy B, Andrew D, Yielder P. Interactive effect of acute pain and motor learning acquisition on sensorimotor integration and motor learning outcomes. J Neurophysiol. 2016;116(5):2210–2220. doi:10.1152/jn.00337.2016
53. Jueptner M, Stephan KM, Frith CD, Brooks DJ, Frackowiak RS, Passingham RE. Anatomy of motor learning. I. Frontal cortex and attention to action. J Neurophysiol. 1997;77(3):1313–1324. doi:10.1152/jn.1997.77.3.1313
54. Crombez G, Van Ryckeghem DM, Eccleston C, Van Damme S. Attentional bias to pain-related information: a meta-analysis. Pain. 2013;154(4):497–510. doi:10.1016/j.pain.2012.11.013
55. Todd J, van Ryckeghem DML, Sharpe L, Crombez G. Attentional bias to pain-related information: a meta-analysis of dot-probe studies. Health Psychol Rev. 2018;12(4):419–436. doi:10.1080/17437199.2018.1521729
56. Tsao H, Druitt TR, Schollum TM, Hodges PW. Motor training of the lumbar paraspinal muscles induces immediate changes in motor coordination in patients with recurrent low back pain. J Pain. 2010;11(11):1120–1128. doi:10.1016/j.jpain.2010.02.004
57. Parker RS, Lewis GN, Rice DA, McNair PJ. The association between corticomotor excitability and motor skill learning in people with painful hand arthritis. Clin J Pain. 2017;33(3):222–230. doi:10.1097/AJP.0000000000000392
58. Krebs DE, Scarborough DM, McGibbon CA. Functional vs. strength training in disabled elderly outpatients. Am J Phys Med Rehabil. 2007;86(2):93–103. doi:10.1097/PHM.0b013e31802ede64
59. Heuninckx S, Wenderoth N, Swinnen SP. Systems neuroplasticity in the aging brain: recruiting additional neural resources for successful motor performance in elderly persons. J Neurosci. 2008;28(1):91–99. doi:10.1523/JNEUROSCI.3300-07.2008
60. Chandler JM, Duncan PW, Kochersberger G, Studenski S. Is lower extremity strength gain associated with improvement in physical performance and disability in frail, community-dwelling elders? Arch Phys Med Rehabil. 1998;79(1):24–30. doi:10.1016/S0003-9993(98)90202-7
61. Buchner DM, Cress ME, de Lateur BJ, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol a Biol Sci Med Sci. 1997;52(4):M218–M24. doi:10.1093/gerona/52A.4.M218
62. Knutzen KM, Pendergrast BA, Lindsey B, Brilla LR. The effect of high resistance weight training on reported pain in older adults. J Sports Sci Med. 2007;6(4):455–460.
63. Latham N, Liu CJ. Strength training in older adults: the benefits for osteoarthritis. Clin Geriatr Med. 2010;26(3):445–459. doi:10.1016/j.cger.2010.03.006
64. Houde F, Cabana F, Léonard G. Does age affect the relationship between pain and disability? A descriptive study in individuals suffering from chronic low back pain. J Geriatr Phys Ther. 2016;39(3):140–145. doi:10.1519/JPT.0000000000000055
65. Maly MR, Costigan PA, Olney SJ. Self-efficacy mediates walking performance in older adults with knee osteoarthritis. J Gerontol a Biol Sci Med Sci. 2007;62(10):1142–1146. doi:10.1093/gerona/62.10.1142
66. Chang FH, Latham NK, Ni P, Jette AM. Does self-efficacy mediate functional change in older adults participating in an exercise program after hip fracture? A randomized controlled trial. Arch Phys Med Rehabil. 2015;96(6):1014–20 e1. doi:10.1016/j.apmr.2015.02.009
67. McAuley E, Szabo A, Gothe N, Olson EA. Self-efficacy: implications for physical activity, function, and functional limitations in older adults. Am J Lifestyle Med. 2011;5(4):361–369. doi:10.1177/1559827610392704
68. Corbett DB, Simon CB, Manini TM, George SZ, Riley JL, Fillingim RB. Movement-evoked pain: transforming the way we understand and measure pain. Pain. 2019;160(4):757–761. doi:10.1097/j.pain.0000000000001431
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.