")
Back to Journals » International Journal of General Medicine » Volume 14
Oxidative Stress (Malondialdehyde) in Adults Beta-Thalassemia Major and Intermedia: Comparison Between Before and After Blood Transfusion and Its Correlation with Iron Overload
Authors Atmakusuma TD , Nasution IR, Sutandyo N
Received 1 September 2021
Accepted for publication 27 September 2021
Published 7 October 2021 Volume 2021:14 Pages 6455—6462
DOI https://doi.org/10.2147/IJGM.S336805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tubagus Djumhana Atmakusuma,1 Intan Russiana Nasution,2 Noorwati Sutandyo3
1Division of Hematology-Medical Oncology, Department of Internal Medicine, Dr. Cipto Mangunkusumo General Hospital/Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 2Division of Hematology-Medical Oncology, Department of Internal Medicine, Gatot Soebroto Army Hospital Jakarta/Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia; 3Division of Hematology-Medical Oncology, Department of Internal Medicine, Dharmais National Cancer Hospital Jakarta/Faculty of Medicine Universitas Indonesia, Jakarta, Indonesia
Correspondence: Tubagus Djumhana Atmakusuma
Division of Hematology-Medical Oncology, Department of Internal Medicine, Dr. Cipto Mangunkusumo General Hospital/Faculty of Medicine Universitas Indonesia, Jalan Diponegoro No. 71, Jakarta Pusat, DKI, Jakarta, Indonesia
Email [email protected]
Background: Iron overload is a major problem in both transfusion-dependent (TDT) and non-transfusion-dependent thalassemia (NTDT). It has been known to increase oxidative stress. Meanwhile, blood transfusion as main therapy for thalassemia increases iron overload. One of the markers of oxidative stress is malondialdehyde (MDA). This study aims to provide data on MDA levels in adult thalassemia patients, and to compare the levels before and after transfusion in patients with TDT and NTDT.
Methods: This is a cross-sectional, pre-post study in adult patients with thalassemia major and intermedia that received blood transfusion with or without iron-chelating agents in Cipto Mangunkusumo Hospital. Blood samples were taken immediately before the transfusion and one day after. Serum ferritin (SF) assays were conducted by electrochemiluminescence immunoassay method, while transferrin saturation (TS) was calculated by dividing serum iron by the binding capacity. Subsequently, plasma MDA levels assays were performed using the Wills method, and data analysis was conducted using the t-test/Mann–Whitney and Pearson/Spearman correlation test, depending on the data distribution.
Results: The 63 respondents recruited consist of 51 TDT and 12 NTDT patients, and their median plasma MDA level before and after transfusion was 0.49 μmol/L and 0.45 μmol/L, respectively. Before transfusion, there was no correlation between SF and MDA, and TS and MDA levels. After the transfusion, there was no correlation between, SF and MDA, or TS and MDA levels.
Conclusion: There is no significant difference in MDA levels before and after transfusion. Although blood transfusion increases the iron load in thalassemia patients, there was no increase in median MDA level after transfusion. Meanwhile, there was no correlation between markers of iron overload and MDA level in thalassemia patients both before and after transfusion.
Keywords: iron overload, malondialdehyde, oxidative stress, non-transfusion dependent thalassemia, transfusion-dependent thalassemia
Background
Thalassemia is a hereditary disease caused by a defect in globin synthesis. This results in erythrocyte membrane fluidity. Thalassemia allows erythrocytes to be broken down easily, thereby lowering the level of hemoglobin in the blood. This phenomenon will result in chronic non-immune hemolytic anemia.1–3 Indonesia is one of the countries with a high prevalence number of thalassemia. Data from the Thalassemia Center, Cipto Mangunkusumo Hospital (RSCM) in 2016, showed that there were 9.031 patients with thalassemia major, and this number is expected to be higher since we have high prevalence of thalassemia gene carriers which are asymptomatic and have not conducted any premarital screening.4
Thalassemia major (TM) is characterized by severe anemia requiring red blood cell transfusions regularly for growth and survival.5 Meanwhile, thalassemia intermedia (TI) has a clinical spectrum or phenotype which varies widely from requiring regular blood transfusions (transfusion-dependent thalassemia/TDT) to not requiring regular transfusions (non-transfusion-dependent thalassemia/NTDT). Generally, complications of excess iron load in TM are due to transfusion of red blood cells, which may result in organ toxicity caused by free radicals, reactive oxygen species (ROS). People with TI are also at risk of iron overload due to the increased absorption of iron from the digestive tract.6
Excessive iron overload forms non-transferrin-bound iron (NTBI) with the most toxic labile plasma iron (LPI) fraction. However, the NTBI examination has not been standardized and does not yet exist in Indonesia. Transferrin saturation (TS) can be used as a surrogate marker for NTBI examination.7 Furthermore, NTBI ferrous iron (Fe II) induces the increased production of ROS, especially hydroxyl radicals (OH•) by the Fenton and Haber Weiss reaction.8,9 The formed ROS will cause lipid peroxidation (PL) cell membrane with one of the products namely malondialdehyde (MDA), which is toxic and mutagenic. MDA is used as a biomarker of oxidative stress examination.10
Existing study on oxidative stress shows conflicting results. Some studies in pediatric and adults with beta-thalassemia found correlation between SF and MDA levels.11,12 However, different results were obtained by Al-Hakeim et al13 and Gunarsih et al, who found no correlation between SF and MDA. Meanwhile, results from the study by Cighetti et al14 showed a correlation between NTBI and MDA. On the contrary, Al-Hakeim, et al13 and Walter et al15 did not obtain the correlation between NTBI with MDA. These warrant further study, especially in adult thalassemia patients since most studies were conducted in pediatric population.
Regular blood transfusion therapy of thalassemia causes iron overload that will induce the formation of ROS. However, there is no published data about the effect of transfusion on changes in oxidative stress. MDA was selected as a marker of oxidative stress because the sampling and examination techniques are relatively easy. Therefore, this study aims to measure the change of MDA levels as a biomarker of oxidative stress related to the provision of blood transfusion therapy. Furthermore, we also aim to analyze the relationship of iron overload and MDA level in thalassemia patients both before and after transfusion.
Methods
Population
The targeted population is adult patients with beta-thalassemia in RSCM at the Thalassemia and Hematology Polyclinic, Department of Internal Medicine. They received blood transfusions either regularly (thalassemia major or TDT-phenotype thalassemia intermedia) or as required (thalassemia minor or NTDT-phenotype thalassemia intermedia). Furthermore, the selected subjects were a those who met the inclusion criteria of the study.
Inclusion Criteria
The subjects recruited were aged 18 years or more and were diagnosed with beta-thalassemia with high-performance liquid chromatography (HPLC) or microcapillary method. They were willing to participate in the study after signing a written consent form. Furthermore, the subjects that fulfilled inclusion criteria were categorized into TDT and NTDT groups.
Exclusion Criteria
The patients who experienced acute medical conditions (heart failure, liver failure), acute inflammation (temperature>38°C), chronic inflammation or infection, pregnant woman, and malignancy were excluded.
Recruitment of Subjects
The subjects were recruited consecutively from at the Thalassemia and Hematology Polyclinic, Department of Internal Medicine, Cipto Mangunkusumo National Referral Hospital, Jakarta. Furthermore, the demographic data and the volume of blood and frequency of red cell transfusions in the past year were recorded from the medical records of patients, and they were categorized into TDT and NTDT.
Laboratory Procedures
The patients underwent venous blood sampling twice, ie, before and after blood transfusion. Subsequently, blood samples were taken each as much as 12 mL and 5 mL, and the test for the value of hemoglobin, serum ferritin, hsCRP, transferrin saturation, and malondialdehyde (MDA) was then conducted.
Measurement of MDA was conducted by spectrophotometric method (Wills) using the principle of the reaction with thiobarbituric acid. This procedure uses 3 mL of blood serum mixed with trichloroacetic acid and was centrifuged to form a supernatant. Furthermore, the supernatant or protein deposits were added with acetic acid, thiobarbituric acid, and n-butanol to produce colors. The color formed is read at a wavelength of 532 nm by spectrophotometry.
Ethics
This study has been reviewed and approved by The Ethics Committee of the Faculty of Medicine, Universitas Indonesia, and the subjects provided appropriate consent to participate. This study was conducted following the declaration of Helsinki, and all participants were informed about the purpose of the study.
Data Analysis
The collected data were processed using SPSS 20 for Windows. Data analysis was conducted using the t-test/Mann–Whitney and Pearson/Spearman correlation test, depending on the data distribution.
Results
Demographic Data
A total of 63 adult patients with beta-thalassemia were recruited during this study period, and it consisted of 51 TDT and 12 NTDT patients. There were 37 females (58%) and 26 males (42%) subjects, and the median age was 25 years with a range from 18 to 67 years. Furthermore, the number of patients with beta-thalassemia was 21 (33%) and beta-thalassemia/HbE was 42 people (67%). Clinical characteristics of subjects with TDT were almost equal to patients with NTDT in terms of the gender ratio, age, hemoglobin level and body mass index (BMI). Patients with TDT received much larger and more frequent blood transfusions than NTDT (Table 1).
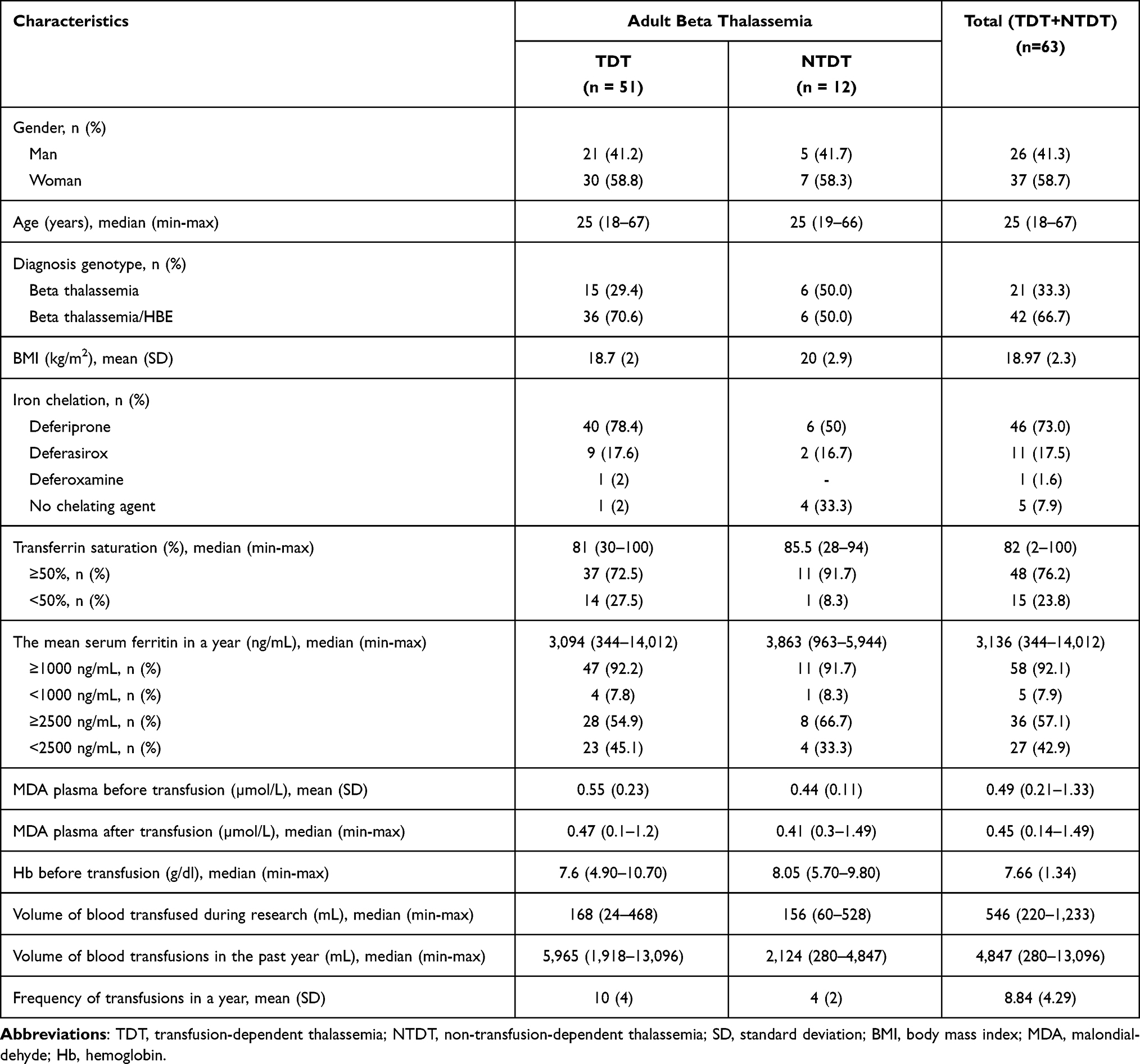 |
Table 1 Characteristics of the Subjects Study According TDT and NTDT Groups Before Transfusion |
Measurement of MDA Plasma
The median plasma MDA level on the subjects before transfusion was 0.49 µmol/L with the lowest and the highest value of 0.21 µmol/L and 1.33 µmol/L. Meanwhile, the median plasma MDA level after transfusion was 0.45 µmol/L with the lowest and highest value of 0.14 µmol/L and 1.49 µmol/L, respectively.
Differences in Plasma MDA Levels Between TDT and NTDT Groups
There were no significant differences in plasma MDA levels before and after transfusion in adult patients with beta-thalassemia TDT and NTDT (Table 2).
 |
Table 2 Plasma MDA Levels Before and After Transfusion in Adult Patients with Beta-Thalassemia TDT and NTDT |
Plasma MDA Level in Adult Patients with Beta-Thalassemia TDT and NTDT Between Before and After Transfusion
The analysis showed that there was no significant difference in the change (delta) median plasma MDA levels before and after transfusion in adult patients with beta-thalassemia TDT and NTDT (Table 3).
 |
Table 3 Change (Delta) Plasma MDA Levels in Adult Patients with Beta-Thalassemia TDT and NTDT Between Before and After Transfusion |
Correlation Between Serum Ferritin and Transferrin Saturation with Plasma MDA Levels Before and After Transfusion in Adult Patients with Beta-Thalassemia TDT and NTDT
Before transfusion, there was no correlation between SF and MDA, and TS and MDA levels. After the transfusion, there was no correlation between, SF and MDA, or TS and MDA levels in adult patients with beta-thalassemia (TDT and NTDT) (Table 4).
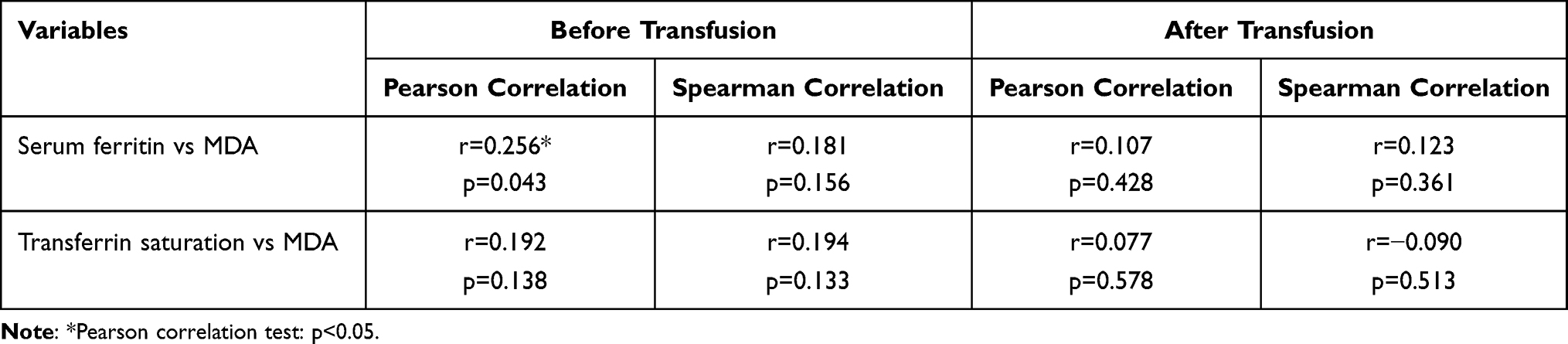 |
Table 4 The Correlation Between Serum Ferritin and Transferrin Saturation with Plasma MDA Levels Before and After Transfusion |
Although Pearson correlation test showed significant correlation between SF and MDA before transfusion, the data distribution was not normal. Hence, Spearman correlation was used and resulted in no correlation.
Changes in Plasma MDA
The changes in plasma MDA levels in these two groups can be seen in Table 5 and Figure 1.
 |
Table 5 The Proportion of Subjects According to Changes of Plasma MDA Levels Before and After Transfusion in Adult Patients with Thalassemia Beta TDT and NTDT |
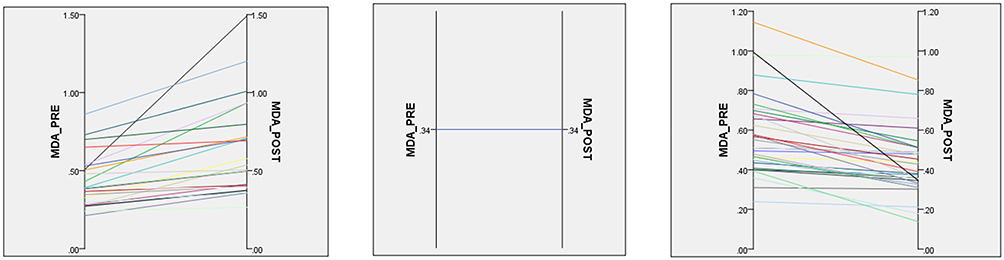 |
Figure 1 Line graph depicting the increase (left), stagnation (middle), and decrease (right) in MDA levels between study subjects, pre and post transfusion. |
Discussion
A total of 63 patients were included in this study, consisting of 51 TDT and 12 NTDT patients with a median age of 25 years old. Furthermore, the median levels of MDA were 0.49 (min 0.21; max 1.33) µmol/L and were not significantly different between before and after transfusion. Differences in the results of plasma MDA levels with previous studies can be assumed to be caused by different subject characteristics. This includes the use of iron chelation therapy and antioxidant supplementation as well as the methods used in the measurement of MDA levels. Plasma MDA level tends to be increased in thalassemia and this reflects the oxidative stress status of the patients.16 Compared to healthy controls, patients with thalassemia show increased MDA levels.16,17 The increase in this lipid peroxidation product is considered to be closely related to the degree of oxidative stress as reported by Ozturk et al.18
The subjects used iron chelation therapy and antioxidant supplementation regularly. Several studies have been conducted on the effect of iron chelation and antioxidants on changes in MDA levels as a marker of oxidative stress. Plasma MDA levels were decreased on the subject approaching the levels in healthy controls after receiving iron chelation therapy and antioxidants for 6–12 months.19,20 A study conducted by Nasseri, et al21 showed that administration of antioxidants in thalassemia patients decreases MDA levels. Therefore, plasma MDA levels obtained in this study were likely to be influenced by routine supplementation of antioxidants and iron chelation therapy.
Median levels of MDA was not significantly different in patients with TDT and NTDT (0.55 vs 0.44 µmol/L; p = 0.100; Mann–Whitney test). The NTDT group consists of patients with thalassemia that received blood transfusions, but not regularly with a mean frequency of 4 transfusions per year. On the contrary, TDT patients consist of beta-thalassemia major and TDT-phenotype thalassemia intermedia patients that require regular blood transfusions. However, this study shows that the difference of MDA levels between TDT and NTDT groups was not significant.
There was no correlation between SF and MDA levels before transfusion. Although Pearson test showed a significant weak correlation, since our data distribution was abnormal, nonparametric test should be used. Spearman correlation test showed that there was no correlation between SF and MDA as well as TS and MDA before and after transfusion.
Similar results have been reported Gunarsih et al1 in children with thalassemia major in the same center where our study was conducted. In their study, the correlation between serum ferritin and plasma MDA concentration was not obtained (r=0.147; p=0.285). In addition, a study conducted by Al-Hakeim, et, al13 on 118 patients with beta-thalassemia major in children age 4–12 years also showed no correlation between serum ferritin levels of plasma MDA. On the contrary, another study by Cighetti et al14 on 21 patients with beta-thalassemia major age 19–30 years and 13 with beta-thalassemia intermedia 23–46 years of age obtained a positive correlation between total MDA and NTBI (r=0.45; p=0.037). However, in our study, we found no correlation between total MDA and serum ferritin level.
Malondialdehyde (MDA) is a well-established marker for oxidative stress and cellular damage. Oxidative stress happens in many disease states such as cancer, chronic inflammation, and thalassemia.22 Oxidative stress is a result from the imbalance of oxidants and antioxidants. When the balance tip towards oxidants (ie, insufficient antioxidant activity), cellular damage occurs. Furthermore, the formation of reactive oxygen species (ROS) contributes to DNA damage, cellular injury, and even carcinogenesis.22 In thalassemia, iron overload plays a major role in mediating oxidative stress.
There was no previous study which correlated serum ferritin levels and plasma MDA in serial pattern before and after transfusion. In 58% of TDT patients, MDA levels decreased after transfusion. Meanwhile, in NTDT, 55.6% had increased MDA levels. The absence of plasma MDA increase after transfusion in some subjects might be related to routine supplementation of antioxidants, which could attenuate the rise in MDA levels. A study by Ezzat, et al23 showed that patients with thalassemia have reduced antioxidant activity and vitamin E levels. Therefore, routine supplementation of vitamin E or other antioxidants should be considered a rational approach. In subjects with increased MDA levels after transfusion, the supplementation of antioxidants may not be sufficient to suppress the oxidative stress damage. Therefore, antioxidants such as vitamin E can be used to attenuate this process.21 In this study, the majority of patients were routinely prescribed antioxidants.
In Islamic countries such as the Middle East and Indonesia, there is a practice of blood cupping called Al-hijamah. Even though there is no data on the proportion of thalassemia patients that received this treatment, a lot of Indonesians follow the practice. Blood cupping is scientifically proven to reduce iron overload, serum ferritin, and oxidative stress.24 It removes MDA from circulating blood to reduce oxidative stress.25 Therefore, this method can be considered in select thalassemia patients, especially in those without thrombocytopenia due to hypersplenism. If thrombocytopenia has already occurred, blood cupping might induce massive blood loss which will increases the transfusional requirement.
Another concern of measuring plasma MDA level after transfusion is the possibility of interference from the donor’s MDA. However, since leukodepleted or washed-packed red cells are only used for routine transfusion, the plasma content of MDA should be negligible.
Furthermore, the transferrin saturation did not correlate with plasma MDA levels either before or after transfusion. Transferrin saturation is a surrogate marker for NTBI. NTBI is the gold standard for measuring iron overload, although the examination is not available in Indonesia. Therefore, transferrin saturation was employed instead of NTBI, and there was no correlation between FS and TS with MDA levels. Therefore, further study should measure NTBI instead of FS and TS as markers of iron overload. In terms of oxidative stress, in addition of malondialdehyde, activity of other aldehydes can be measured by using assay for thiobarbituric acid reactive species.26
The sample size used is larger than similar studies conducted in Pakistan and Egypt.23,27 Moreover, the novelty of this study is the fact the MDA levels were measured pre- and post-transfusion. This is the first study that employed serial measurements of MDA levels. Limitation of this study is the limited number of participants due to the short study period and budget restrictions since MDA-level assay are not covered by national health insurance. Further studies involving a larger sample size is encouraged to confirm our findings. Moreover, it should involve patients with thalassemia major, intermedia, minor, and normal control group to compare the relationship between blood transfusion, iron overload, and oxidative stress. In addition, the subjects should be stratified based on baseline SF and TS to detect the difference in MDA levels.
Conclusion
Median plasma MDA levels in adult beta-thalassemia major and intermedia before and after transfusion were 0.49 µmol/L and 0.45 µmol/L, respectively. There was no significant difference between MDA levels and between TDT and NTDT patients. Furthermore, there was no correlation between FS and TS with MDA before and after transfusion. The routine administration of antioxidants, especially vitamin E, might play a role in ameliorating MDA in thalassemia patients. Therefore, although blood transfusion increases iron load in thalassemia patients, there was no increase in median MDA level after transfusion.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Gunarsih A, Amalia P, Boediman I. Variables associated with malondialdehyde level in patients with thalassemia major. Paediatr Indones. 2012;52:125–131. doi:10.14238/pi52.3.2012.125-31
2. Cappellini MD, Cohen A, Porter J, et al. Guidelines for the Management of Transfusion-Dependent Thalassemia. Thalassemia International Federation; 2014.
3. Gamberini MR, De Sanctis V, Gilli G. Hypogonadism, diabetes mellitus, hypothyroidism, hypoparathyroidism: incidence and prevalence related to iron overload and chelation therapy in patients with thalassaemia major followed from 1980 to 2007 in the Ferrara Centre. Pediatr Endocrinol Rev. 2008;6(Suppl 1):158–169.
4. Thalassemia Center Cipto Mangunkusumo Hospital. Thalassemia major patients data. Jakarta; 2016. [unpublished document].
5. Wood B, Molecular Higgs D. Basis of thalassemia syndromes. Disorders of erythropoiesis, erythrocytes and iron metabolism. Eur Sch Hematol. 2009;35:406
6. Taher AT, Vichinsky E, Musallam Ea K. Guidelines for the Management of Non-Transfusion Dependent Thalassemia (NTDT). Thalassemia International Federation; 2013.
7. Kohgo Y, Ikuta K, Ohtake T, et al. Body iron metabolism and pathophysiology of iron overload. Int J Hematol. 2008;88(1):7–15. doi:10.1007/s12185-008-0120-5
8. Hershko C. Pathogenesis and management of iron toxicity in thalassemia. Ann N Y Acad Sci. 2010;1202:1–9. doi:10.1111/j.1749-6632.2010.05544.x
9. Kalpravidh RW, Siritanaratkul N, Insain P, et al. Improvement in oxidative stress and antioxidant parameters in beta-thalassemia/Hb E patients treated with curcuminoids. Clin Biochem. 2010;43(4–5):424–429. doi:10.1016/j.clinbiochem.2009.10.057
10. Nielsen F, Mikkelsen BB, Nielsen JB, et al. Plasma malondialdehyde as biomarker for oxidative stress: reference interval and effects of life-style factors. Clin Chem. 1997;43(7):1209–1214. doi:10.1093/clinchem/43.7.1209
11. Sengsuk C, Tangvarasittichai O, Chantanaskulwong P, et al. Association of iron overload with oxidative stress, hepatic damage and dyslipidemia in transfusion-dependent β-Thalassemia/HbE patients. Indian J Clin Biochem. 2014;29(3):298–305. doi:10.1007/s12291-013-0376-2
12. Naithani R, Chandra J, Bhattacharjee J, et al. Peroxidative stress and antioxidant enzymes in children with beta-thalassemia major. Pediatr Blood Cancer. 2006;46(7):780–785. doi:10.1002/pbc.20669
13. Al-Hakeim HK, Auda FM, Ali BM. Lack of correlation between non-labile iron parameters, total carbonyl and malondialdehyde in major thalassemia. J Clin Biochem Nutr. 2014;55(3):203–206. doi:10.3164/jcbn.14-24
14. Cighetti G, Duca L, Bortone L, et al. Oxidative status and malondialdehyde in beta-thalassaemia patients. Eur J Clin Invest. 2002;32(Suppl 1):55–60. doi:10.1046/j.1365-2362.2002.0320s1055.x
15. Walter PB, Macklin EA, Porter J, et al. Inflammation and oxidant-stress in beta-thalassemia patients treated with iron chelators deferasirox (ICL670) or deferoxamine: an ancillary study of the Novartis CICL670A0107 trial. Haematologica. 2008;93(6):817–825. doi:10.3324/haematol.11755
16. Boudrahem-Addour N, Izem-Meziane M, Bouguerra K, et al. Oxidative status and plasma lipid profile in β-Thalassemia patients. Hemoglobin. 2015;39(1):36–41. doi:10.3109/03630269.2014.979997
17. Abduljabbar A, Mehmetçik G. Malondialdehyde and C-Reactive protein values in transfusion dependent thalassemia patients; 2018.
18. Ozturk Z, Genc GE, Kupesiz A, et al. Thalassemia major patients using iron chelators showed a reduced plasma thioredoxin level and reduced thioredoxin reductase activity, despite elevated oxidative stress. Free Radic Res. 2015;49(3):309–316. doi:10.3109/10715762.2015.1004327
19. Yanpanitch OU, Hatairaktham S, Charoensakdi R, et al. Treatment of β-Thalassemia/Hemoglobin E with antioxidant cocktails results in decreased oxidative stress, increased hemoglobin concentration, and improvement of the hypercoagulable state. Oxid Med Cell Longev. 2015;2015:537954. doi:10.1155/2015/537954
20. Tesoriere L, D’Arpa D, Maggio A, et al. Oxidation resistance of LDL is correlated with vitamin E status in beta-thalassemia intermedia. Atherosclerosis. 1998;137(2):429–435. doi:10.1016/s0021-9150(97)00300-6
21. Nasseri E, Mohammadi E, Tamaddoni A, et al. Benefits of curcumin supplementation on antioxidant status in β-thalassemia major patients: a double-blind randomized controlled clinical trial. Ann Nutr Metab. 2017;71(3–4):136–144. doi:10.1159/000479634
22. Maurya RP, Prajapat MK, Singh VP, et al. Serum malondialdehyde as a biomarker of oxidative stress in patients with primary ocular carcinoma: impact on response to chemotherapy. Clin Ophthalmol. 2021;15:871–879. doi:10.2147/OPTH.S287747
23. Ezzat AM, Abdelmotaleb GS, Shaheen AM, et al. Peroxidative stress and antioxidant enzymes in children with beta-thalassemia major. Med Res J. 2016;15(2):57–62. doi:10.1097/01.MJX.0000511315.53248.78
24. El-Shanshory M, Hablas NM, Shebl Y, et al. Al-hijamah (wet cupping therapy of prophetic medicine) significantly and safely reduces iron overload and oxidative stress in thalassemic children: a novel pilot study. J Blood Med. 2018;9:241–251. doi:10.2147/JBM.S170523
25. Almaiman AA. Proteomic effects of wet cupping (Al-hijamah). Saudi Med J. 2018;39(1):10–16. doi:10.15537/smj.2018.1.21212
26. Ondei L, Estevão I, Rocha MIP, et al. Oxidative stress and antioxidant status in beta-thalassemia heterozygotes. Rev Bras Hematol Hemoter. 2013;35(6):409–413. doi:10.5581/1516-8484.20130122
27. Rasool M, Malik A, Jabbar U, et al. Effect of iron overload on renal functions and oxidative stress in beta thalassemia patients. Saudi Med J. 2016;37(11):1239–1242. doi:10.15537/smj.2016.11.16242
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.