")
Back to Journals » Open Access Journal of Sports Medicine » Volume 6
Overuse injuries in youth basketball and floorball
Authors Leppänen M, Pasanen K, Kujala UM, Parkkari J
Received 5 February 2015
Accepted for publication 31 March 2015
Published 22 May 2015 Volume 2015:6 Pages 173—179
DOI https://doi.org/10.2147/OAJSM.S82305
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Freddie H Fu
Mari Leppänen,1 Kati Pasanen,1 Urho M Kujala,2 Jari Parkkari,1
1Tampere Research Center of Sports Medicine, UKK Institute for Health Promotion Research, Tampere, 2Department of Health Sciences, University of Jyväskylä, Jyväskylä, Finland
Background: The popularity of team sports is growing among young people. High training volume and intensity may predispose young athletes to overuse injuries. Research to date has tended to focus on acute injuries rather than overuse injuries. The purpose of this study was to examine the occurrence, nature, and severity of overuse injuries in youth basketball and floorball, with the hypothesis that overuse injuries are frequent in youth team sports.
Methods: The study comprised a total of 401 Finnish team sports athletes (207 basketball and 194 floorball players). The data were collected using a detailed questionnaire. The participants (mean age 15.8±1.9 years) responded to the questionnaire covering information on overuse injuries during the previous 12 months.
Results: A total of 190 overuse injuries was reported (97 in basketball and 93 in floorball). In both sports, most of the injuries involved the lower extremities (66% and 55% of all injuries in basketball and floorball, respectively). In basketball, the most commonly injured site was the knee (44 cases, 45%). In floorball, the most commonly injured sites were the lower back/pelvis (36 cases, 39%) and knee (32 cases, 34%). Overuse injuries caused an average time loss from full participation of 26±50 (median 7) days in basketball and 16±37 (median 5) days in floorball.
Conclusion: Overuse injuries are a common problem in youth team sports, and often cause long-term absence from full participation. The findings suggest that injury reduction and training load monitoring strategies are needed in the field. More research using explicit prospective data collection is needed to better understand the problem.
Keywords: overuse injuries, sports injuries, epidemiology, adolescence, team sports
Introduction
Sports participation among the young is associated with multiple health benefits.1,2 However, compared with less physically active adolescents, highly active adolescents seem to suffer more musculoskeletal pain,3 such as a higher incidence of Osgood–Schlatter disease4 and low back pain.5 Overuse injuries in youth sports are of particular concern because they may cause long-term disability, negatively affect sports participation, and impact on performance and even daily activities.6 Furthermore, repetitive physical overloading of the physis may in some cases result in growth disturbances and deformities.7 Intensive training with a high training volume at an early age may predispose young athletes to overuse injuries.8 Overuse injuries are common in endurance sports9–11 and technical sports12 that require long monotonous training sessions or repetitious movement patterns. However, overuse injuries may also be a substantial problem in team sports due to the high training volume and competition load.13–15 Although interest in sports injury research has increased over the past decade,16 there is little research on the incidence, prevalence, and prevention of overuse injuries.12
Basketball is a globally popular team sport.17 Several earlier studies have investigated the epidemiology of basketball injuries in various populations, mainly among adult,17 professional,18–20 collegiate,21,22 and high school23,24 basketball players, but also more recently among children.25–27 Regardless of the large number of studies published, analyses on the incidence and nature of overuse injuries in basketball are scarce. In addition, most of the studies published have been conducted outside Europe, and knowledge about basketball-related injuries in Europe is still insufficient.17
Floorball is a team sport that has become very popular in Europe, and is also one of the most popular team sports among the youth of Finland. In 2009–2010, there were 144,000 leisure-time floorball players among Finnish adolescents aged 3–18 years.28 Floorball is a form of hockey played indoors on a court (20×40 m) surrounded by a low board. The players use sticks of graphite compounds to score goals with a hollow, dimpled plastic ball. A team usually consists of 15–20 players, and six players (a goalkeeper and five outfield players) are on the court at the same time. The playing time is three periods of 20 minutes. While the goalkeeper wears a helmet and padded clothes, the other players usually wear no protection or eye protection only. Although rough body contact is not allowed, floorball is associated with sudden accelerations, stops and turns, uncontrolled contacts with the boards, and strikes by sticks or the ball.2 Thus far, only a few studies have investigated floorball injuries,29–34 and these studies have focused mostly on adult players. Moreover, little information exists on overuse injuries in this sport.
Basketball and floorball are popular sports among young people in Finland. These sports are both played indoors and include similar movements, such as rapid turns, stops, and accelerations. Most epidemiological studies on basketball and floorball have focused on acute injuries. Thus, the purpose of this retrospective study of young basketball and floorball players was to examine the occurrence, nature, and severity of overuse injuries. The study hypothesis is that although most of the injuries in these sports are acute in nature, overuse injuries are common and often restrict normal training and playing for a long time.
Materials and methods
Participants
Study participants were recruited from basketball and floorball teams of the Tampere region. Altogether, 20 teams (with 475 junior players) were invited (ten basketball and ten floorball teams), and 18 teams (nine basketball and nine floorball teams) agreed to participate in the study. Of the participating teams, 37 players refused to take part in the study. Players were included if they were official members of the participating teams and had played official junior games (U16–U20) during the previous season. Players were excluded (n=3) if they had not participated in training and games during the previous season. A total of 401 players (207 basketball players and 194 floorball players) agreed to participate in the study. Participation in the study was based on written informed consent from each player, and the consent of a parent for subjects younger than 18 years was required. The study was approved by the ethics committee of the Pirkanmaa Hospital District, Tampere, Finland (ETL code R10169).
Data collection
This retrospective analysis is part of a large 3-year (2011–2014) follow-up study on sports injury risk factors. Injury occurrence in this report was analyzed retrospectively over a preceding 12-month period. The data used are based on a detailed questionnaire, which subjects completed when they entered the study (baseline). The questionnaire was based on a previous study of sports injuries,32 and covered information on personal data, sports participation, and the history of sports injuries. The athletes were asked to evaluate as precisely as possible the number of weekly training sessions, the number of hours spent per session, and the number of games they played during the previous season. One part of the questionnaire concerned injury occurrence during participation in the player’s sport. This part was completed if the athlete had sustained a sports injury in the preceding 12 months. For each injury that had occurred over the period of interest, the anatomic location, type of injury, the nature of injury (acute or overuse), context (contact or non-contact, training or competition), date of occurrence, and recovery time were registered. The collected data were systematically cross-checked with the athlete face-to-face to ensure the accuracy of the completed questionnaire.
Injury definitions and severity
An injury was defined as any physical complaint related to a game or practice that resulted in the player being unable to take full part in a game or practice session for at least one day. Any significant pain or discomfort that restricted normal training was taken into consideration. An overuse injury was defined as being caused by repetitive microtrauma without a single, identifiable event being responsible for injury. The severity of the injuries was defined according to Fuller et al,35 using time loss from full participation in the usual training program or competition: a minimal injury, an injury causing an absence from full participation of 1–3 days; a mild injury, an injury causing an absence from full participation of 4–7 days; a moderate injury, an injury causing an absence from full participation of 8–28 days; and a severe injury, an injury causing an absence from full participation of 29 or more days.
Exposure hours
Total hours of exposure were calculated as the sum of training and game hours per year. The total training hours per year for each player were calculated by the individually reported weekly training hours over the 45-week active period. Total exposure time during the games was calculated using an average of 60 minutes’ active exposure time (including time spent in warm-up, playing, and cool-down) per game.
Injury rate and injury incidence
The injury rate was calculated as the number of injured players divided by the number of exposed players. Injury incidence per 1,000 hours of exposure was calculated by dividing the number of injuries by the total number of hours of exposure and then multiplying that figure by 1,000.
Statistical analysis
Means ± standard deviations were calculated to describe continuous variables, and frequencies and percentages were used for categorical variables. Differences in injury occurrence, injured body site, and injury severity between the boys and girls were analyzed using the chi-squared test. The independent samples t-test was used to compare group differences in characteristics of the participants. P-values <0.05 were considered to be statistically significant.
Results
Characteristics of the participants
A total of 401 junior players (213 boys and 188 girls) completed the questionnaire in the year they entered the study. The study population consisted of 207 basketball players (101 boys and 106 girls) and 194 floorball players (112 boys and 82 girls). The characteristics of the participants are shown in Table 1. The mean age of the participants at the time they entered the study was 15.8±1.9 (range 12–21) years. The boys were significantly older than the girls (P=0.001). The boys reported having started playing at a significantly (P<0.001) younger age than the girls (8.1±2.6 years versus 9.1±2.7 years, respectively). The average training volume per week was significantly (P=0.001) higher for the boys (10.2±3.9 hours per week) than the girls (9.0±3.0 hours per week).
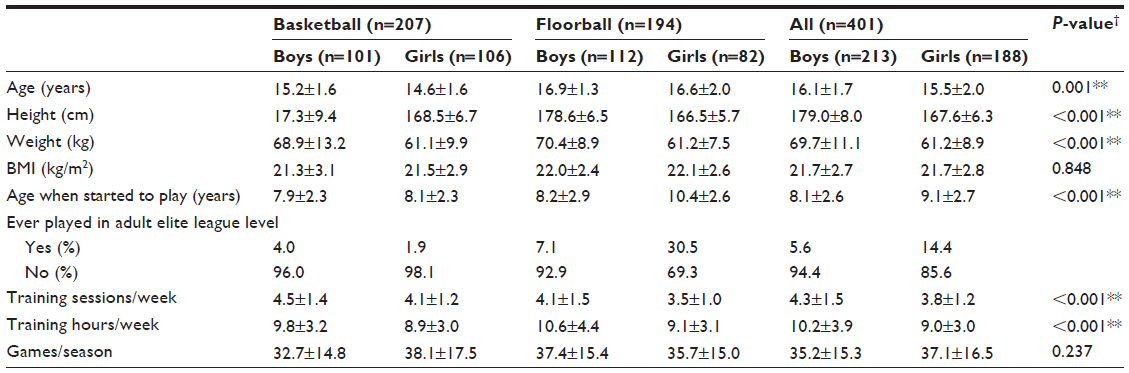 | Table 1 Characteristics of the participants |
Overall injury characteristics
In all, the 401 players included in the study reported a total of 629 injuries, comprising 439 acute injuries (70%) and 190 overuse injuries (30%). In basketball, the proportion of overuse injuries was 31% and in floorball the proportion was 30%. The incidence of overuse injury was 1.0 per 1,000 hours of exposure in both sports. The injured population consisted of 91 (60%) male players and 61 (40%) female players, of whom 80 (53%) were basketball players and 72 (47%) were floorball players. In addition, players reported a total of 150 overuse conditions that caused no time loss from training or competition; these were not included in the present analysis.
Basketball
Of the 207 basketball players participating in the study, 80 (39%) had sustained at least one overuse injury in the preceding 12 months. The boys had sustained 44 (45%) overuse injuries and the girls 53 (55%), giving a total of 97 overuse injuries among the basketball players. The injury rate was 0.47 overuse injuries per athlete per year.
Most of the overuse injuries in basketball involved the lower extremities (64 cases, 66%), with the knee being the most commonly injured site (44 cases, 45%, Table 2). Overuse injuries caused an average time loss from full participation of 26±50 (median 7) days. The severity of injuries is presented in Table 3. In basketball, there were no differences for the anatomic location (Figure 1) or severity of overuse injuries between the boys and the girls.
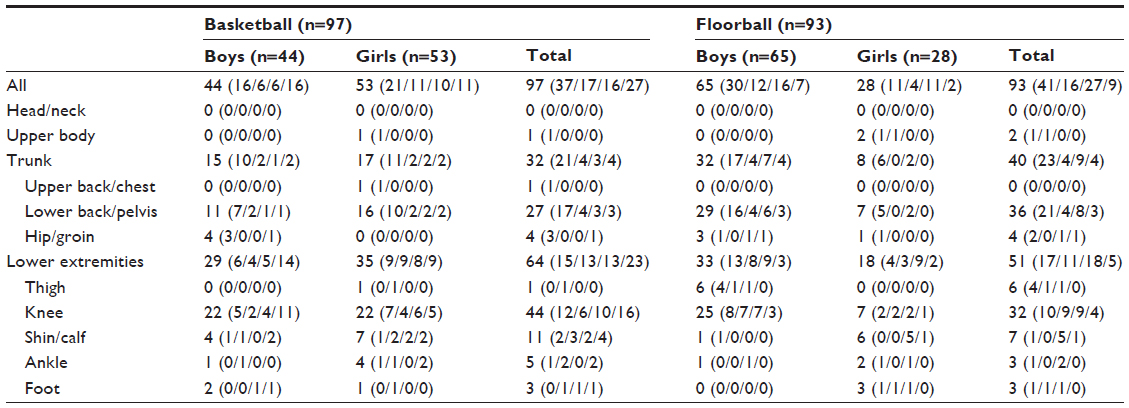 | Table 2 Frequency (n) and anatomical distribution of overuse injuries according to game and sex, with distribution of overuse injuries according to injury severity |
 | Table 3 Severity of overuse injuries (n=190) according to sports and sex |
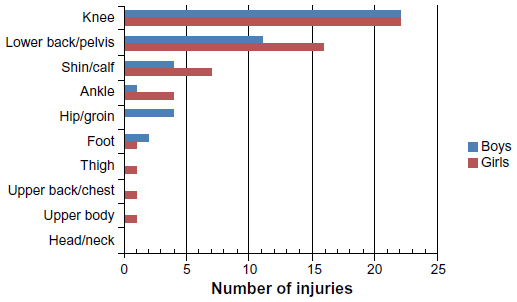 | Figure 1 Overuse injuries in basketball according to anatomic location and sex. |
Floorball
Of the 194 floorball players, 72 (37%) reported having had at least one overuse injury in the preceding 12 months. Significantly more boys (51 players) reported overuse injury/injuries than girls (21 players, P=0.005). Floorball players sustained a total of 93 overuse injuries, of which the boys sustained 65 (70%) overuse injuries and the girls 28 (30%) overuse injuries. The injury rate in floorball was 0.48 overuse injuries per athlete per year.
Most of the overuse injuries involved the lower extremities (51 cases, 55%). The most commonly injured site was the lower back/pelvis (36 cases, 39%), and the second most common site was the knee (32 cases, 34%, Table 2). There were differences in anatomic location of overuse injuries between the boys and girls; the boys reported significantly more lower back and knee overuse injuries compared with the girls (P<0.001, Figure 2). Most of the injuries were classified as minimal (Table 3). There was no difference in severity of overuse injuries between the boys and girls (P=0.544). The average time loss from full participation due to an overuse injury was 16±37 (median 5) days.
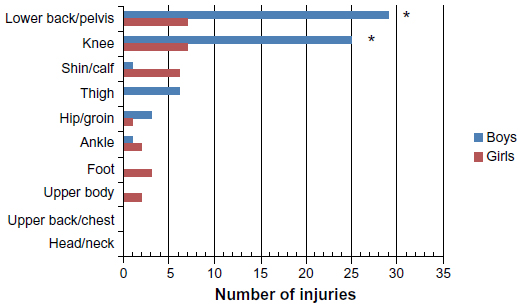 | Figure 2 Overuse injuries in floorball according to anatomic location and sex. |
Discussion
The main finding of this retrospective study was that 39% of basketball players and 37% of floorball players reported having had at least one overuse injury during the preceding 12-month period. Overuse injuries caused long absences from full participation in training and playing in both sports. Most of the overuse injuries in these sports affected the lower extremities, with the knee and lower back/pelvis being the most commonly injured sites.
Epidemiological studies of overuse injuries in team sports are scarce, especially among young people. Previous studies in older populations of floorball players have reported that approximately 17%–24% of all floorball injuries are overuse injuries.30,31 In a study of female players only,33 the percentage of overuse injuries was 30%. In our study, the proportion of overuse injuries among young floorball players was similar (30%). According to previous studies among professional basketball players,18,19,36 overuse injuries and inflammatory conditions account for 15%–27% of all injuries. In our study, 31% of all basketball injuries were overuse injuries. However, Clarsen et al37 recently found that overuse injuries tend to be underreported, so the actual proportion of overuse injuries is probably much higher than these rates suggest. Our results, which show that the most common injury location causing long-term losses in playing time was the knee, are in accordance with previous findings that growing athletes commonly suffer from Osgood–Schlatter disease,4 patellofemoral pain, or other long-lasting but self-limiting unspecified knee pain.38
When describing the occurrence of overuse injuries, the definition used to record these injuries is important. We used the definition “time lost from full participation in the usual training program or competition” and found an overuse injury incidence of 1.0 injuries per 1,000 hours of exposure in both sports. Unfortunately, we were not able to find a reference incidence for either youth sport. In their prospective cohort study of senior basketball players, Cumps et al17 used an injury definition based on physical discomfort rather than time loss, and found an overuse injury incidence of 3.8 per 1,000 hours of exposure, which is considerably higher than the incidence in youth basketball in our study. Although these rates are not comparable due to different study designs and methods, it can be speculated that the injury definition we used may have underestimated the true extent of overuse injuries. Standard injury surveillance methods (time loss) are not able to register all overuse injuries because overuse problems often have a gradual onset and athletes tend to train and compete despite their symptoms.37 It is worth noting that players in our study reported 150 overuse conditions that caused no time loss and hence were not defined as injuries, but it is most likely that these injuries were still harmful. Including these conditions in the present analysis would give an overuse injury incidence of 1.8 per 1,000 hours of exposure.
The present finding that most of the overuse injuries in both basketball and floorball are located in the lower extremities, with the knee being the most common site of an overuse injury, is consistent with previous research.17,30,31,33 There is evidence in the literature that overuse knee conditions, such as patellofemoral pain, are common, especially in elite-level basketball.17,19,20,36 In team sports that require jumping (volleyball, basketball), the high training load is commonly reported as a risk factor for patellar tendinopathy.15,17,39 Furthermore, recent findings indicate that smaller tendon cross-sectional area might also be related to patellar tendinopathy.40 While adolescent athletes rapidly increase their muscle strength, tendon stiffness and cross-sectional area are not similarly developed, and this may predispose adolescent athletes to tendon overuse injuries.41 Pains in the tendon insertions and associated tendon-related problems are common in youth team sports that involve repetitious impact movements such as landing from a jump and sudden stops.4 Surprisingly, according to our results, overuse conditions of the lower back were almost as common as knee problems in basketball, and in floorball they were even more common. In floorball, a plausible explanation for this might be the low playing position, which causes strain to the lower back.
It is well known that injury profiles vary by sport,10 but there is insufficient evidence regarding whether male and female team sport athletes have different risks for overuse conditions. Many authors have found that patellar tendinopathy is far more common in male athletes than in female athletes.13,15,42 However, this is not the case in all sports and overuse conditions. Cumps et al17 reported that female basketball players are at a higher risk for all overuse injuries and for patellofemoral pain. Snellman et al32 reported overuse injuries in floorball being more common in females, whereas Wikström and Andersson31 found the opposite. In the current study, there were no sex differences in basketball, but in floorball the boys seemed to have sustained overuse injuries more often than the girls. Sex differences might partly be explained by differences in training volumes.43 More studies are therefore needed to determine the possible role of sex as a risk factor for overuse injuries in team sports as well as in other sports.
This study has some limitations. First, there is recall bias affecting the reliability of the retrospectively collected injury history. In addition, we were not able to confirm detailed diagnoses. Second, we calculated exposure hours based on individually reported data and by using average values for training and playing. Thus, it is possible that some players played less and some more than our estimation. Further, the injury definition based on time loss, although emphasizing time loss from full participation in training or competition, might have left aside injuries that caused no time loss or were transient in nature. It is possible that this might have resulted in underestimation of the frequency and severity of overuse injuries. These results should therefore be interpreted with caution. In addition, in our study, the age of the participants ranged from 12 to 21 years, and these findings cannot be extrapolated to immature adolescent athletes or to adult athletes.
The strengths of this study are the accuracy of the completed questionnaire and the high response rate. We collected the data on the day the player entered the study, and completed the questionnaire on the spot, meaning that a study researcher was able to carefully check the completed questionnaire with the player. All participating players completed the questionnaire.
Conclusion
Overuse injuries among growing athletes in youth team sports have not been well studied. The present findings provide evidence that overuse injuries are quite a common problem among youth basketball and floorball players, and overuse injuries often have a long-term injurious effect on the player’s ability to practice and compete at full capacity. Notwithstanding the limitations of retrospectively collected data, our findings suggest that development of injury reduction and training load monitoring strategies is needed in the field. Prospective analyses of risk factors for overuse injuries in popular youth team sports are also needed. In order to understand the true extent of the problem, future studies should use standardized methods to register overuse problems.
Acknowledgments
The study was supported by the Finnish Ministry of Education and Culture and the Medical Research Fund of Tampere University Hospital. We thank the players and their coaches for their cooperation with our research.
Disclosure
The authors declare that there are no conflicts of interests regarding the publication of this paper.
References
Pate RR, Trost SG, Levin S, Dowda M. Sports participation and health-related behaviors among US youth. Arch Pediatr Adolesc Med. 2000;154:904–911. | |
Bäckmand H, Kujala U, Sarna S, Kaprio J. Former athletes’ health-related lifestyle behaviours and self-rated health in late adulthood. Int J Sports Med. 2010;31:751–758. | |
Kujala UM, Taimela S, Viljanen T. Leisure physical activity and various pain symptoms among adolescents. Br J Sports Med. 1999;33:325–328. | |
Kujala UM, Kvist M, Heinonen O. Osgood-Schlatter’s disease in adolescent athletes. Retrospective study of incidence and duration. Am J Sports Med. 1985;13:236–241. | |
Kujala UM, Taimela S, Erkintalo M, Salminen JJ, Kaprio J. Low-back pain in adolescent athletes. Med Sci Sports Exerc. 1996;28:165–170. | |
Kettunen JA, Kvist M, Alanen E, Kujala UM. Long-term prognosis for jumper’s knee in male athletes. A prospective follow-up study. Am J Sports Med. 2002;30:689–692. | |
Caine D, DiFiori J, Maffulli N. Physeal injuries in children’s and youth sports: reasons for concern? Br J Sports Med. 2006;40:749–760. | |
DiFiori JP, Benjamin HJ, Brenner J, et al. Overuse injuries and burnout in youth sports: a position statement from the American Medical Society for Sports Medicine. Clin J Sport Med. 2014;24:3–20. | |
Clarsen B, Krosshaug T, Bahr R. Overuse injuries in professional road cyclists. Am J Sports Med. 2010;38:2494–2501. | |
Ristolainen L, Heinonen A, Turunen H, et al. Type of sport is related to injury profile: a study on cross country skiers, swimmers, long-distance runners and soccer players. A retrospective 12-month study. Scand J Med Sci Sports. 2010;20:384–393. | |
Andersen CA, Clarsen B, Johansen TV, Engebretsen L. High prevalence of overuse injury among iron-distance triathletes. Br J Sports Med. 2013;47:857–861. | |
Jacobsson J, Timpka T, Kowalski J, et al. Injury patterns in Swedish elite athletics: annual incidence, injury types and risk factors. Br J Sports Med. 2013;47:941–952. | |
Lian ØB, Engebretsen L, Bahr R. Prevalence of jumper’s knee among elite athletes from different sports. A cross-sectional study. Am J Sports Med. 2005;33:561–567. | |
Myklebust G, Hasslan L, Bahr R, Steffen K. High prevalence of shoulder pain among elite Norwegian female handball players. Scand J Med Sci Sports. 2011;23:288–294. | |
Visnes H, Bahr R. Training volume and body composition as risk factors for developing jumper’s knee among young elite volleyball players. Scand J Med Sci Sports. 2013;23:607–613. | |
Leppänen M, Aaltonen S, Parkkari J, Heinonen A, Kujala UM. Interventions to prevent sports injuries: a systematic review and meta-analysis of randomized controlled trials. Sports Med. 2014;44:473–486. | |
Cumps E, Verhagen E, Meeusen R. Prospective epidemiological study of basketball injuries during one competitive season: ankle sprains and overuse knee injuries. J Sports Sci Med. 2007;6:204–211. | |
Deitch JR, Starkey C, Walters SL, Moseley JB. Injury risk in professional basketball players: a comparison of Women’s National Basketball Association and National Basketball Association Athletes. Am J Sports Med. 2006;34:1077–1083. | |
Drakos MC, Domb B, Starkey C, Callahan L, Allen AA. Injury in the National Basketball Association. A 17-year overview. Sports Health. 2010;2:284–290. | |
McCarthy MM, Voos JE, Nguyen JT, Callahan L, Hannafin JA. Injury profile in elite female basketball athletes at the Women’s National Basketball Association combine. Am J Sports Med. 2013;41:645–651. | |
Agel J, Olson DE, Dick R, Arendt EA, Marshall SW, Sikka RS. Descriptive epidemiology of collegiate women’s basketball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42:202–210. | |
Dick R, Hertel J, Agel J, Grossman J, Marshall SW. Descriptive epidemiology of collegiate men’s basketball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42:194–201. | |
Messina DF, Farney WC, DeLee JC. The incidence of injury in Texas high school basketball. A prospective study among male and female athletes. Am J Sports Med. 1999;27:294–299. | |
Borowski LA, Yard EE, Fields SK, Comstock RD. The epidemiology of US high school basketball injuries, 2005–2007. Am J Sports Med. 2008;36:2328–2335. | |
Randazzo C, Nelson NG, McKenzie LB. Basketball-related injuries in school-aged children and adolescents in 1997–2007. Pediatrics. 2010; 126:727–733. | |
Pappas E, Zazulak BT, Yard EE, Hewett TE. The epidemiology of pediatric basketball injuries presenting to US emergency departments 2000–2006. Sports Health. 2011;3:331–335. | |
Vanderlei FM, Bastos FN, de Lemes íR, Vanderlei LC, Júnior JN, Pastre CM. Sports injuries among adolescent basketball players according to position on the court. Int Arch Med. 2013;6:5. | |
National exercise survey 2009–2010 (2010): Kansallinen liikuntatutkimus 2009–2010. Lapset ja nuoret. Nuori Suomi ry, Suomen Liikunta ja Urheilu, Suomen Kuntourheiluliitto ry, Suomen Olympiakomitea, Helsingin kaupunki, Opetus- ja kulttuuriministeriö. SLU:n julkaisusarja 7/2010 [Children and young people. Finnish Sports Federation SLU Association, the Young Finland Association, the Finnish Sport Federation, Finnish Olympic Committee and the City of Helsinki. The research was conducted in collaboration with the Ministry of Education and the Ministry of Culture]. Available at: ISBN: 978-952-5828-24-5 (pdf). Finnish. | |
Pasanen K, Parkkari J, Kannus P, et al. Injury risk in female floorball: a prospective one-season follow-up. Scand J Med Sci Sports. 2008;18:49–54. | |
Löfgren O, Andersson N, Björnstig U, Lorantzon R. Incidence, nature and causes of floorball injuries. Scand J Med Sci Sports. 1994;4:211–214. | |
Wikström J, Andersson C. A prospective study of injuries in licensed floorball players. Scand J Med Sci Sports. 1997;7:38–42. | |
Snellman K, Parkkari J, Kannus P, Leppälä J, Vuori I, Järvinen M. Sports injuries in floorball: a prospective one-year follow-up study. Int J Sports Med. 2001;22:531–536. | |
Leivo T, Puusaari I, Mäkitie T. Sports-related eye injuries: floorball endangers the eyes of young players. Scand J Med Sci Sports. 2007;17:556–563. | |
Maxen M, Kühl S, Krasti G, Filippi A. Eye injuries and orofacial traumas in floorball? A survey in Switzerland and Sweden. Dent Traumatol. 2011;27:95–101. | |
Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40:193–201. | |
Starkey C. Injuries and illnesses in the National Basketball Association: a 10-year perspective. J Athl Train. 2000;35:161–167. | |
Clarsen B, Myklebust G, Bahr R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: the Oslo Sports Trauma Research Centre (OSTRC) Overuse Injury Questionnaire. Br J Sports Med. 2013;47:495–502. | |
Kujala UM, Kvist M, Österman K. Knee injuries in athletes. Review of exertion injuries and retrospective study of outpatient sports clinical material. Sports Med. 1986;3:447–460. | |
van der Worp H, van Ark M, Zwerver J, van den Akker-Scheek I. Risk factors for patellar tendinopathy in basketball and volleyball players: a cross-sectional study. Scand J Med Sci Sports. 2012;22:783–790. | |
Couppé C, Kongsgaard M, Aagaard P, et al. Differences in tendon properties in elite badminton players with or without patellar tendinopathy. Scand J Med Sci Sports. 2013;23:e89–e95. | |
Mersmann F, Bohm S, Schroll A, Boeth H, Duda G, Arampatzis A. Evidence of imbalanced adaptation between muscle and tendon in adolescent athletes. Scand J Med Sci Sports. 2014;24:e283–e289. | |
Zwerver J, Bredeweg SW, van den Akker-Scheek I. Prevalence of jumper’s knee among nonelite athletes from different sports. A cross-sectional survey. Am J Sports Med. 2011;39:1984–1988. | |
Ristolainen L, Heinonen A, Waller B, Kujala UM, Kettunen JA. Gender differences in sport injury risk and types of injuries: a retrospective twelve-month study on cross-country skiers, swimmers, long-distance runners and soccer players. J Sports Sci Med. 2009;8:443–451. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.