")
Back to Journals » Patient Preference and Adherence » Volume 13
Overcoming barriers to the use of metformin: patient and provider perspectives
Authors Flory JH, Keating S , Guelce D, Mushlin AI
Received 9 April 2019
Accepted for publication 25 July 2019
Published 22 August 2019 Volume 2019:13 Pages 1433—1441
DOI https://doi.org/10.2147/PPA.S211614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
James H Flory,1 Scott Keating,2 Dominique Guelce,2 Alvin I Mushlin2
1Endocrinology Service, Department of Subspecialty Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA; 2Department of Healthcare Policy and Research, Weill Cornell Medical College, New York, NY, USA
Correspondence: James H Flory
Endocrinology Service, Department of Subspecialty Medicine, Memorial Sloan Kettering Cancer Center, 205 E 64th Street
, New York, NY 10021, USA
Tel +1 347 638 3235
Email [email protected]
Background: Metformin is the first-line treatment for type 2 diabetes mellitus. Observational studies show lower rates of use than would be expected from clinical guidelines.
Objective: We undertook a qualitative study of barriers to metformin use from the patient and provider perspective.
Design: Patient focus group, patient individual interviews, provider interviews, and chart review. Purposive sampling of patients and providers in New York State.
Participants: Seven one-on-one patient interviews, one focus group with 13 patients, 10 provider interviews, and manual review of 1259 charts.
Approach: Grounded theory.
Results: Both providers and patients cited potential health benefits as strong reasons to take metformin and describe it as the first-line drug for diabetes. Patients and providers both cited gastrointestinal side effects as the primary barrier to metformin use. Patients described adapting to these side effects and taking metformin at a time that minimizes them. In contrast, providers emphasized dose titration and the use of extended-release formulation as tools for minimizing side effects but were uncertain about the effectiveness of these strategies.
Conclusion: Metformin is positively viewed by patients and providers, but gastrointestinal side effects are a barrier to its use. There is some consensus on basic measures to improve its tolerability, but these measures are not consistently applied and lack evidence establishing their effectiveness. Pragmatic clinical trial research on optimal dose, formulation, and counseling for new metformin users should be considered.
Keywords: metformin, diabetes, qualitative research, pharmacology, adherence
Background
Metformin is a first-line drug for type 2 diabetes (T2DM), and evidence also supports its off-label use for obesity and prediabetes.1,2 Yet, even among patients with T2DM, only half take metformin, with both overall utilization and long-term persistence of approximately 50%,3–5 consistent with most patients being offered the medication but roughly half of them not taking it long term. However, the reason for such low rates of long-term use is not known. Given metformin’s low cost, excellent safety profile, and effectiveness, such high rates of non-use warrant explanation.
Failure to continue to take metformin might reflect lack of need for the drug, for example if T2DM is well controlled with diet alone. In other cases, despite a clear clinical need, patients may lack motivation to adhere to chronic medication, be unable to afford the cost, or have concerns about drug safety or stigma.6 A third possibility is that patients may have a contraindication to metformin – such as alcoholism or severe kidney, liver, or heart disease, all of which are thought to increase the risk of lactic acidosis as a side effect – although the total prevalence of these conditions is unlikely to account for a 50% rate of non-use.3,7,8
A fourth potential factor in metformin non-persistence is intolerance. Metformin is widely described as poorly tolerated due to gastrointestinal side effects, and providers are advised to use low starting doses and consider extended-release formulations to curb these side effects.9,10 Although significant in clinical practice, metformin’s gastrointestinal side effects are not well understood, with some evidence linking them to pre-existing gastrointestinal conditions, but little direct data on their mechanism.11–14
Although conventional wisdom is that gastrointestinal intolerance is a common problem with metformin use, and that strategies for addressing such intolerance are important, the evidence base supporting these assumptions is limited. There have been few quantitative or qualitative studies of the reasons for metformin non-use. One quantitative study found that side effects were the most commonly cited reason for early metformin discontinuation, but rates of missing data were very high.15 A qualitative study of two provider focus groups also identified gastrointestinal side effects as a challenge to using metformin, but placed a greater emphasis on concern about safety in patients with contraindications (renal insufficiency, heart failure, hepatic dysfunction, and alcohol use).16 However, this study did not include the patient perspective and used a guided discussion format that included multiple specific questions about contraindications, potentially leading participants to overemphasize their role.
Because metformin is a cornerstone of diabetes management, understanding the reasons for metformin non-use in T2DM is an important step for identifying effective interventions to improve diabetes care. From a grounded theory perspective, we conducted a qualitative study of patients, providers, and electronic-health record documentation to gain insight into why patients take metformin, why they stop, and what potential interventions might appropriately increase the effective use of metformin.
Methods
One-on-one semi-structured patient interviews, a semi-structured focus group with patients, semi-structured provider interviews, and manual chart review were used. In this qualitative study, free text from transcripts of interviews and focus groups, and from charts, was coded in a hypothesis-free, non-quantitative fashion as detailed below.17,18
Study participants
Focus group participants were recruited from the Weill Cornell Internal Medicine clinic; any adult patient (age ≥18) with a history of T2DM was eligible. Additional one-on-one interview participants were identified through a database search for metformin users seen at endocrinology or internal medicine practices affiliated with Weill Cornell Medical College (WCMC), and eligible patients were contacted by phone after we obtained permission from their primary care providers. Patients were eligible if they were age ≥18 and had at least one electronic prescription for metformin documented in the WCMC electronic-health record. Of note, patients did not have to be current users of metformin to be eligible, and did not have to have any particular duration of prior use; these broad inclusion criteria were intended to maximize the variety of experience captured in this qualitative study. Key-informant interviews were conducted with ten health care providers recruited from the principal investigator’s professional network; providers were eligible if they were able to prescribe medications and routinely cared for patients with T2DM. For all of these groups, recruitment continued concurrently with iterative analysis of collected data until thematic saturation was reached.
Chart review data were taken from a related quantitative study in which 1259 charts of patients aged >18 with at least one electronic prescription for metformin documented in the WCMC electronic-health record were manually reviewed.15 Although saturation would likely have been reached with a smaller number of charts, all 1259 charts were used in this study as it was cost-effective to include qualitative analysis with the systematic chart review done for the quantitative study.
Human subject protections
This study was approved by the Institutional Review Board of WCMC. Written informed consent was obtained from participants in the one-on-one patient interviews, while oral informed consent was obtained from participants in the focus groups and key-informant interviews. Patients who participated in the focus group or in the one-on-one interviews received a $25 cash card as an incentive.
Data collection and analysis
After providing informed consent, a facilitator with training in qualitative research led a focus group, following a set of pre-written questions and probes. The same facilitator conducted seven one-on-one patient interviews based on a set of guide questions, as well as ten key-informant interviews, all also consisting of pre-written questions and probes. All sessions were recorded and field notes were kept. Transcripts were created from the recordings.
Analysis consisted of open coding of the transcript and chart review data by three authors identifying emergent themes, following a grounded theory approach.17,18 One author was a fellowship-trained diabetes specialist; one was a second-year medical student without specialized diabetes training; and one had a non-medical background and no special experience with diabetes. Three authors (Flory, Guelce, and Keating) independently conducted coding of transcripts from the focus groups and from the first half of the individual interviews, with review and consolidation of code lists. Two authors (Flory and Guelce) then coded the remaining transcripts, subsequently again undergoing joint review and consolidation of the code list. “Component themes” were only identified if those component themes were expressed by at least three different individuals or found in at least three different chart reviews.
Chart review was facilitated by limiting review to notes containing the word “metformin” or a common commercial name (“Glucophage”,“Fortamet“). These notes were independently reviewed by two authors (Flory and Keating), followed by joint review and consolidation of the code list. Chart review was limited to patients for whom diabetes was the indication for metformin use. Data had been de-identified at the time of analysis, so that charts could not be linked directly to the much smaller cohort of individuals who were interviewed; there likely was some overlap between these cohorts but the amount of overlap cannot be assessed.
Coding was initially conducted manually without the use of specialized software; coded data was then analyzed using R statistical software (R-3.5.2 for Windows). Focus group and interview questions are summarized in the Table S1.
Results
A total of 20 patients (13 in the focus group and 7 in one-on-one interviews) were included. Eleven were male and 9 were female; all identified as having type 2 diabetes. Further clinical and demographic data were not collected on focus group participants. One-on-one interview patients ranged in age from 32 to 81 years. All had been taking metformin for at least 1 year and at the time of the interview were taking metformin at doses ranging from 500 to 2000 mg daily. Ten providers were recruited from four different clinics in New York State and consisted of four endocrinologists, one nurse-practitioner, and five general internists. All had been in independent practice for at least 5 years. Fifty percent were female and the rest male. Two were in private practice while the rest practiced in an academic setting. In addition, 1259 charts were reviewed, all belonging to patients with type 2 diabetes. The charts were drawn from a cohort described in a previous quantitative publication.15
Major recurrent themes across all data sources were the reasons to take metformin (Motivations), barriers to taking it (Barriers), and strategies to overcome these barriers (Strategies). A theme unique to providers was uncertainty about key facts, meaning lack of either confidence or consistency, or both, in expressed views (Uncertainty).
Motivations to use metformin range from simple glucose lowering to its broadly positive reputation
Both patients and providers cited specific benefits of metformin, including glucose (or HbA1c) lowering as well as weight loss and possible anti-cancer benefits, as reasons to use it: “It’s helped me keep my A1c under six” (Table 1). In addition to these specific motives, both patients and providers often made less specific statements about metformin’s general reputation: “all the doctors seem to feel that metformin is like the miracle drug for diabetes”.
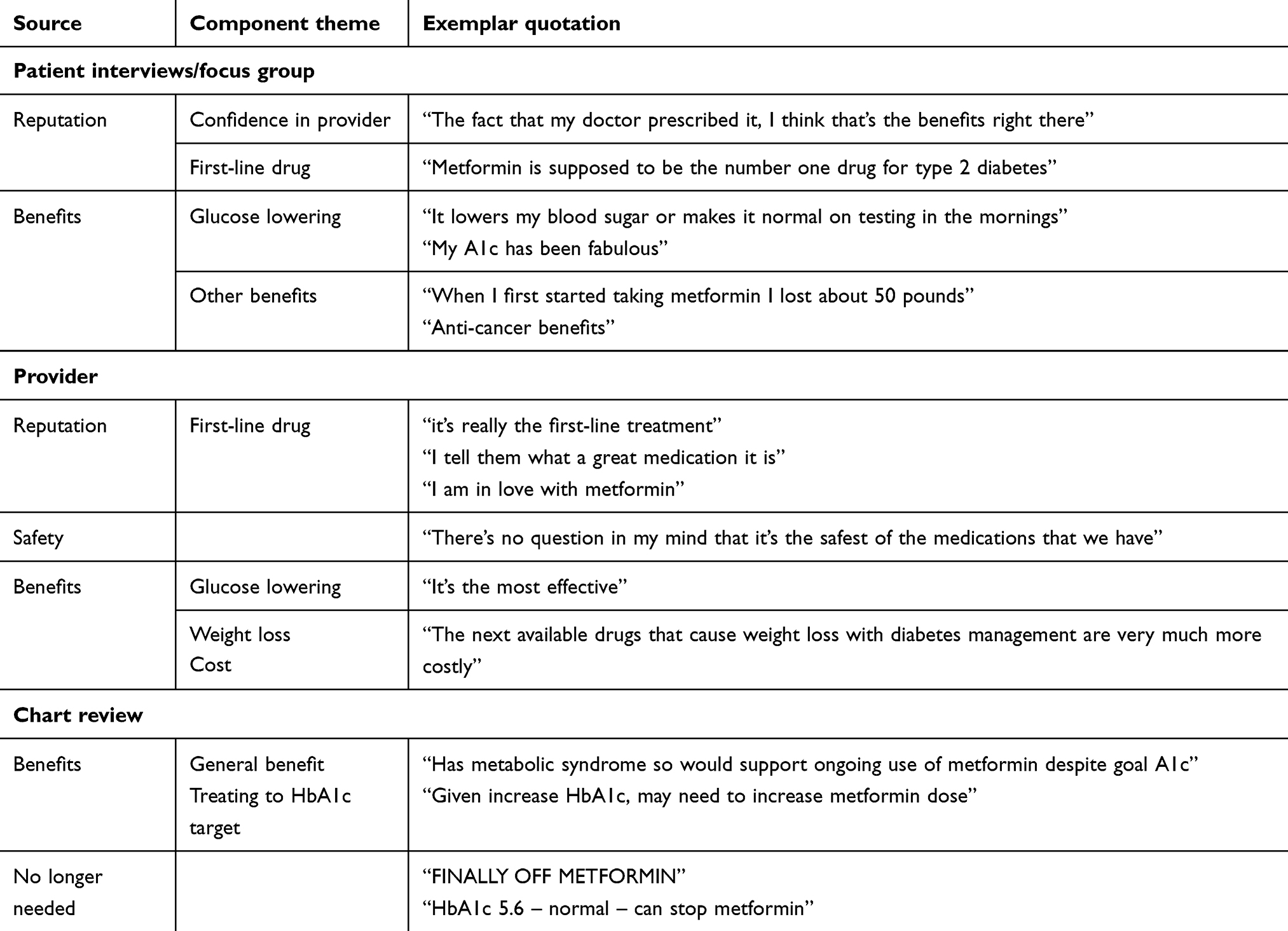 |
Table 1 Motivations to use metformin |
While safety was not a component theme for patients, it was for providers. Providers typically viewed its safety very favorably: “it’s such a great medication … it’s so safe relative to some of the others for the long-term”. Two of the 10 providers mentioned contraindications to metformin, but both did so noting that the impact of the contraindications was limited – “the only time that I will really stop it or decrease the dose if the kidney function is getting really bad” and "it actually is turning out that lactic acidosis is more infrequent and the caveat whereby one is prescribing it with a heart failure, liver failure, renal failure, I think that those have been somewhat overblown".
Chart review also exhibited the benefit component theme. An additional component theme which seldom appeared in interviews but was prominent in chart review was “no longer needing metformin” in patients who had already achieved a clinical goal (usually HbA1c reduction).
Gastrointestinal side effects are a major barrier to metformin use
For the theme of “barriers”, patients, providers, and chart review were all dominated by the sub-theme of side effects, particularly the component of gastrointestinal side effects: “people complain about bloating and it just upsets their stomach. Some people get diarrhea with it”. All providers spontaneously brought up gastrointestinal side effects as a concern in their interviews. On patient and chart review, an additional sub-theme was the absence of side effects in certain individuals (Table 2).
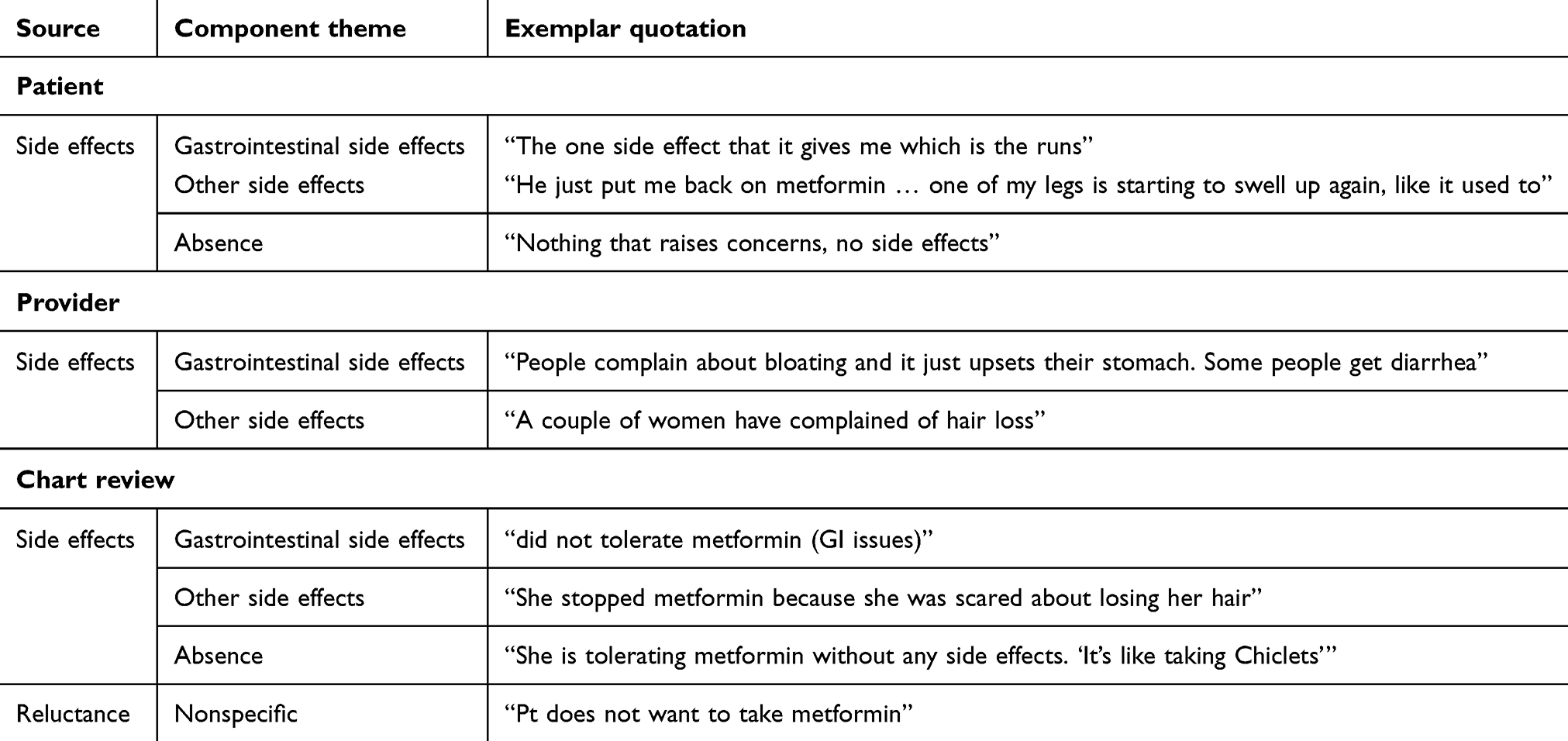 |
Table 2 Barriers to metformin use |
Patients and physicians have different strategies for improving metformin tolerance
Strategies for staying on metformin focused on addressing gastrointestinal side effects but differed considerably between patients and providers (Table 3). For patients, the only theme was adaptation through lifestyle, for example by avoiding taking the drug near mealtimes. Of interest, one patient-interviewee was adamant that taking metformin apart from a meal was essential to tolerate it, although other patients and providers felt that taking metformin with a meal was beneficial. This interviewee described a routine of taking the medication at times when the side effects would not be disruptive:
I realized I didn’t have to take it with a meal per se, or I would just take it first thing in the morning when I woke up knowing I would be home for at least the next two hours or so. And then, taking the second dose before going to bed. Or once I get home knowing that I’m not going back out. That way, if anything happens, at least I’m home where I’m comfy and I don’t have to run into a restaurant or a store or something and say, “I need to make a potty run, please,” type thing.
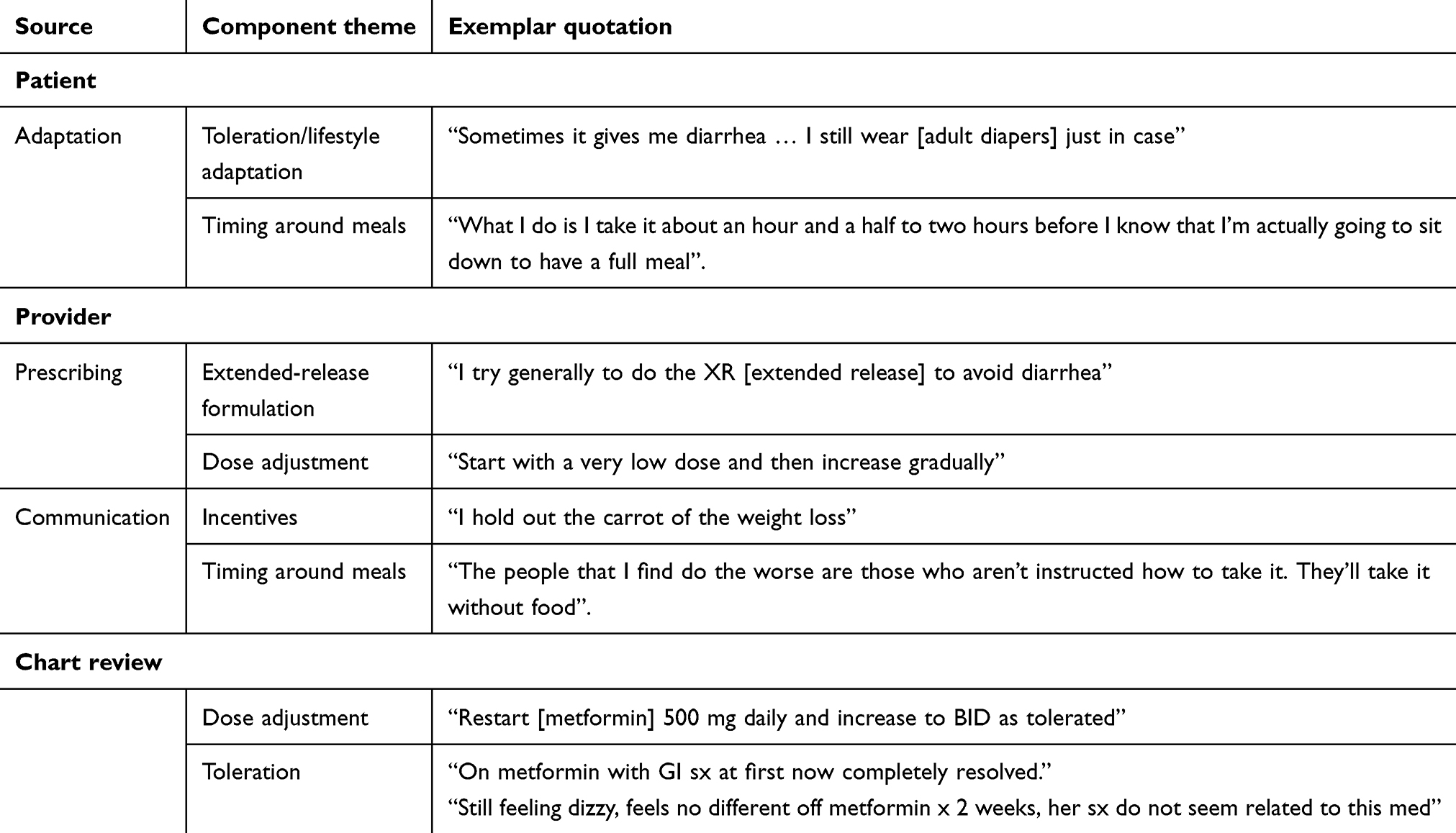 |
Table 3 Strategies for improving metformin tolerance |
Providers in contrast focused on the component theme of prescribing practices, specifically through dose adjustment and use of extended-release formulations. These approaches were frequently mentioned together: “I either switch to XR [extended-release] if I didn’t start them on an extended-release form, and I decrease the dose, and I ask them to go really, really slowly on titrating it up”. Providers also noted communication and counseling as a component theme, and often described their approach in some detail:
I read them the whole act beforehand and say “listen this is going to bother your stomach. We’re going to start at a pretty low dose, and we’ll build up. You may notice that it really does decrease your appetite, and you get some bloating.” You give them the whole nine yards, and then I see them next time. They’re like, “Oh really? It wasn’t that bad at all.”
Chart review also revealed the “prescribing” component-theme, primarily dose adjustment.
Strategies for improving metformin tolerance are of uncertain effectiveness
A final theme was uncertainty/inconsistency, although it emerged only from the provider interviews (Table 4). It had three component themes. First was “prevalence”: while all providers provided a quantitative estimate of how many patients stopped metformin, these estimates ranged from “close to 5%” to “maybe half”. Second was challenges in always attributing side effects to metformin as opposed to other causes. Finally, providers voiced uncertainty about the effectiveness of either extended-release formulations or dose adjustment in minimizing metformin’s side effects (Table 4).
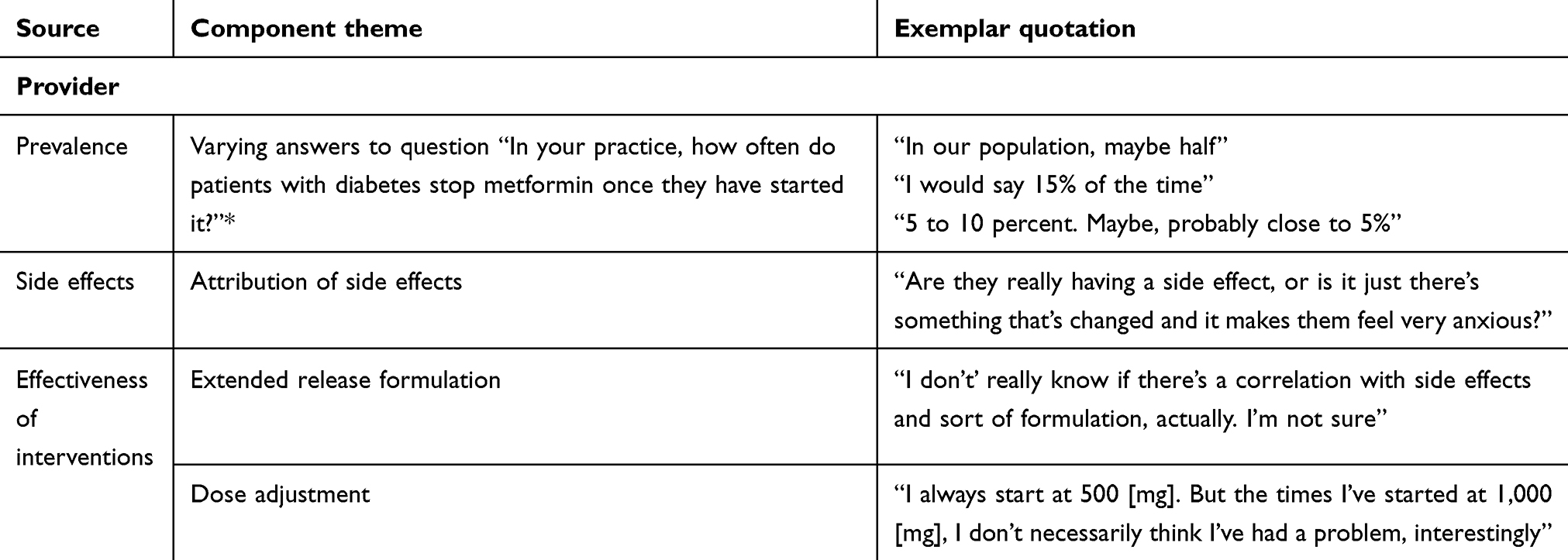 |
Table 4 Uncertainty, meaning lack of confidence or consistency, about key facts and effectiveness of interventions |
Conclusion
This study finds that providers and patients included in this study were strongly motivated to use metformin but that gastrointestinal side effects were perceived as a major disadvantage and barrier to the use of the drug. Both groups cite several widely known strategies for dealing with metformin’s side effects, with patients emphasizing adaptation and providers emphasizing the use of dose and formulation to prevent side effects. The providers expressed a lack of confidence in the tools available to them to reduce metformin side effects.
Patients, and particularly providers, cited strong motivation to use metformin, describing it as the “first-line” drug for type 2 diabetes with many potential health benefits. Providers were particularly positively disposed toward the drug, emphasizing its safety profile and using dramatic language (“I am in love with metformin”). Some, however, suspected that large numbers of patients stopped using the drug and attributed this to gastrointestinal side effects.
The finding that both providers and patients commonly cited gastrointestinal side effects as a barrier is consistent with the empirical literature on metformin side effects, as well as with two other qualitative studies.16,19 It contrasts with the qualitative literature on other medications, for example statins, in which other considerations such as cost and safety were much more prominent.20 Of note, contraindications such as chronic kidney disease were not a prominent theme in these interviews, in contrast to another qualitative study of metformin users.16
Proposed strategies for overcoming barriers focused on gastrointestinal side effects and were consistent with the conventional wisdom that gastrointestinal side effects are a potential barrier to metformin use, and that providers can help prevent or relieve side effects with careful counseling, dose titration, and potentially use of extended-release formulations. But, these findings also reveal how little evidence supports the conventional wisdom. Providers offered very different estimates of the frequency of metformin side effects, suggesting that this phenomenon is not consistently measured or reported to providers in routine practice.
Providers’ limited confidence in the effectiveness of manipulating dose and formulation is consistent with uncertainty in the literature. Meta-analyses have failed to confirm a dose-dependency of metformin’s side effects.21 Extended-release formulations have advantages in clinical trials but have never been shown to improve adherence by rigorous study in a pragmatic setting.22–24 Some authors have argued that extended-release metformin should be routinely used instead of immediate release.25 In actual practice, some providers do routinely start their patients on extended-release while others routinely start patients on immediate release, suggesting uncertainty and equipoise on this issue.15
This research has limitations. As in any qualitative research, subjectivity in interpretation of data is impossible to avoid. Sample size, although seemingly sufficient to reach saturation, was small, and the fact that all participants were from New York State and the majority had a connection to a single academic medical center limits the generalizability of these findings. The study captures limited information on parameters, such as duration of metformin use, that would be particularly important in follow-up quantitative research on specific risk factors and the effects of specific interventions for metformin intolerance. The greater emphasis on gastrointestinal side effects over contraindications seen in this study might reflect methodological differences from other work, or true differences between study populations.16
Given metformin’s ubiquity in the health care system, any opportunity to optimize the way it is prescribed deserves consideration. Dissemination of the limited existing evidence about how best to prescribe metformin to maximize adherence is warranted, but it is important to note that most of the existing advice is not evidence based. Pragmatic clinical trial research on optimal dose, formulation, and counseling for new metformin users should be considered. One example would be a study to assess whether adherence and outcomes are superior among when patients are routinely started on extended release as opposed to immediate-release metformin.
Acknowledgment
This work was funded by Agency for Healthcare Research and Quality, K08-HS023898.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sanchez-Rangel E, Inzucchi SE. Metformin: clinical use in type 2 diabetes. Diabetologia. 2017;60:1586–1593. doi:10.1007/s00125-017-4336-x
2. American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S90–S102. doi:10.2337/dc19-S009
3. Flory JH, Hennessy S. Metformin use reduction in mild to moderate renal impairment: possible inappropriate curbing of use based on food and drug administration contraindications. JAMA Intern Med. 2015;175:458–459. doi:10.1001/jamainternmed.2015.0324
4. Hampp C, Borders-Hemphill V, Moeny DG, Wysowski DK. Use of antidiabetic drugs in the U.S., 2003–2012. Diabetes Care. 2014;37(5):1367–1374. doi:10.2337/dc13-2289
5. Flory J, Gerhard T, Stempniewicz N, Keating S, Rowan CG. Comparative adherence to diabetes drugs: an analysis of electronic health records and claims data. Diabetes Obes Metab. 2017;19:1184–1187. doi:10.1111/dom.2017.19.issue-8
6. Hugtenburg JG, Timmers L, Elders PJ, et al. Definitions, variants, and causes of nonadherence with medication: a challenge for tailored interventions. Patient Prefer Adherence. 2013;7:675–682. doi:10.2147/PPA.S29549
7. Metformin hydrochloride [product label]. U.S. Food and Drug Administration website. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/020357s037s039,021202s021s023lbl.pdf. Accessed August 7, 2019
8. Crowley MJ, Diamantidis CJ, McDuffie JR, et al. Clinical outcomes of metformin use in populations with chronic kidney disease, congestive heart failure, or chronic liver disease: a systematic review. Ann Intern Med. 2017;166(3):191–200. doi:10.7326/M16-1901
9. Florez H, Luo J, Castillo-Florez S, et al. Impact of metformin-induced gastrointestinal symptoms on quality of life and adherence in patients with type 2 diabetes. Postgrad Med. 2010;122:112–120. doi:10.3810/pgm.2010.03.2128
10. Bonnet F, Scheen A. Understanding and overcoming metformin gastrointestinal intolerance. Diabetes Obes Metab. 2016;19(1):473–481. doi:10.1111/dom.12854
11. Bouchoucha M, Uzzan B, Cohen R. Metformin and digestive disorders. Diabetes Metab. 2011;37:90–96. doi:10.1016/j.diabet.2010.11.002
12. Dujic T, Zhou K, Donnelly LA, et al. Association of organic cation transporter 1 with intolerance to metformin in type 2 diabetes: a GoDARTS study. Diabetes. 2015;64:1786–1793. doi:10.2337/db14-1560
13. Huang Y, Sun J, Wang X, et al. Helicobacter pylori infection decreases metformin tolerance in patients with type 2 diabetes mellitus. Diabetes Technol Ther. 2015;17:128–133. doi:10.1089/dia.2014.0203
14. Okayasu S, Kitaichi K, Hori A, et al. The evaluation of risk factors associated with adverse drug reactions by metformin in type 2 diabetes mellitus. Biol Pharm Bull. 2012;35:933–937. doi:10.1248/bpb.35.933
15. Flory JH, Keating SJ, Siscovick D, Mushlin AI. Identifying prevalence and risk factors for metformin non-persistence: a retrospective cohort study using an electronic health record. BMJ Open. 2018;8(7):e021505. doi:10.1136/bmjopen-2018-021505
16. Trinkley KE, Malone DC, Nelson JA, Saseen JJ. Prescribing attitudes, behaviors and opinions regarding metformin for patients with diabetes: a focus group study. Ther Adv Chronic Dis. 2016;7(5):220–228. doi:10.1177/2040622316657328
17. Pope C, Ziebland S, Mays N. Qualitative research in health care: analysing qualitative data. BMJ. 2000;320(7227):114–116. doi:10.1136/bmj.320.7227.114
18. Leung L. Validity, reliability, and generalizability in qualitative research. J Family Med Prim Care. 2015;4(3):324–327. doi:10.4103/2249-4863.161306
19. Guénette L, Lauzier S, Guillaumie L, Giguère G, Grégoire JP, Moisan J. Patients’ beliefs about adherence to oral antidiabetic treatment: a qualitative study. Patient Prefer Adherence. 2015;10(9):413–420. doi:10.2147/PPA.S78628
20. Ju A, Hanson CS, Banks E, et al. Patient beliefs and attitudes to taking statins: systematic review of qualitative studies. Br J Gen Pract. 2018;68(671):e408–e419. doi:10.3399/bjgp18X696365
21. Hirst JA, Farmer AJ, Ali R, et al. Quantifying the effect of metformin treatment and dose on glycemic control. Diabetes Care. 2012;35:446–454. doi:10.2337/dc11-1465
22. Schwartz S, Fonseca V, Berner B, et al. Efficacy, tolerability, and safety of a novel once-daily extended-release metformin in patients with type 2 diabetes. Diabetes Care. 2006;29:759 64. doi:10.2337/diacare.29.04.06.dc05-1967
23. Gao H, Xiao W, Wang C, et al. The metabolic effects of once daily extended-release metformin in patients with type 2 diabetes: a multicentre study. Int J Clin Pract. 2008;62:695–700. doi:10.1111/j.1742-1241.2008.01733.x
24. Donnelly LA, Morris AD, Pearson ER. Adherence in patients transferred from immediate release metformin to a sustained release formulation: a population-based study. Diabetes Obes Metab. 2009;11:338–342. doi:10.1111/j.1463-1326.2008.00973.x
25. Alsultan M, Al-Omar H, Vandewalle B, et al. Metformin extended versus immediate release in Saudi Arabia: a cost-effectiveness analysis. Value Health. 2017;20(9):A479. doi:10.1016/j.jval.2017.08.456
Supplementary material
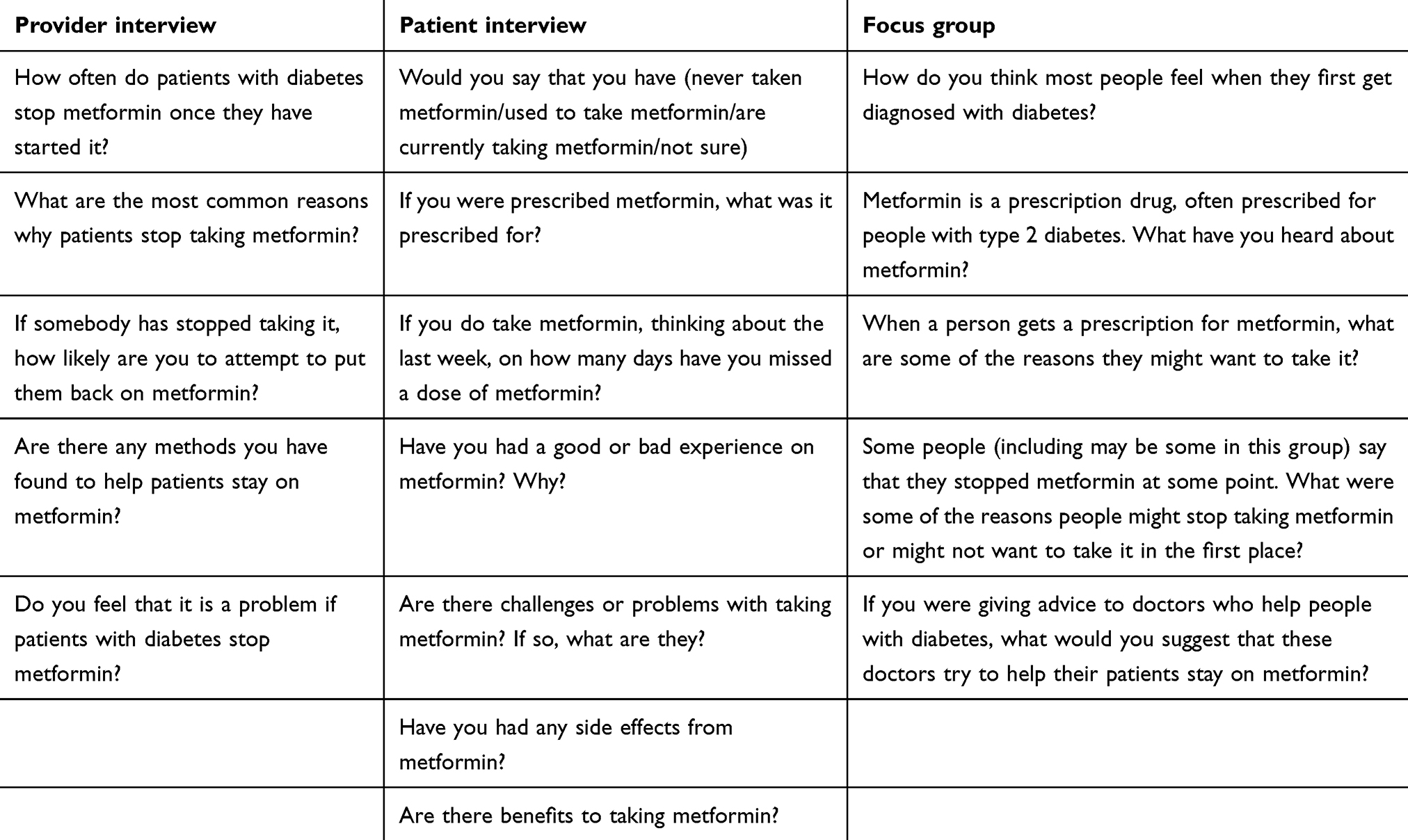 |
Table S1 Interview and focus group questions |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.