")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Overcoming barriers to effective management of tardive dyskinesia
Authors Caroff SN
Received 13 January 2019
Accepted for publication 20 February 2019
Published 4 April 2019 Volume 2019:15 Pages 785—794
DOI https://doi.org/10.2147/NDT.S196541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Stanley N Caroff
Corporal Michael J Crescenz VA Medical Center, and the Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
Abstract: Tardive dyskinesia (TD) is a heterogeneous syndrome of involuntary hyperkinetic movements that is often persistent and occurs belatedly during treatment with antipsychotics. Recent approval of two dopamine-depleting analogs of tetrabenazine based on randomized controlled trials offers an evidence-based therapeutic approach to TD for the first time. These agents are optimally used within the context of a comprehensive approach to patient management that includes a practical screening and monitoring program, sensitive and specific criteria for the diagnosis of TD, awareness of the severity and impact of the disorder, informed discussions with patients and caregivers, and a rational basis for prescribing decisions about continued antipsychotic and adjunctive agents. Areas of limited or inconclusive data, bias and misunderstandings about key aspects, and neglect of training about TD in recent years contribute to barriers in providing effective care and promoting patient safety.
Keywords: tardive dyskinesia, valbenazine, deutetrabenazine, tetrabenazine vesicular monoamine transporter inhibitors, antipsychotics, schizophrenia, bipolar disorder, major depressive disorder, drug-induced movement disorders
Introduction
The introduction of specific antipsychotic drugs over a half century ago ushered in an era of renewed therapeutic optimism and revitalized interest in understanding the neurobiology of severe mental illness. However, a troubling drawback of this class of agents that are dependent on dopamine-receptor blocking properties was their impact on basal ganglia functions underlying drug-induced movement disorders.1,2 Although most of these adverse effects were acute in onset and reversible after medication cessation, the movements of tardive dyskinesia (TD) that were persistent and associated with prolonged treatment were most concerning.
Until the recent approval of two new tetrabenazine analogs, there was no evidence-based treatments for TD. Even so, there are several areas of misunderstanding, bias, or gaps in knowledge that may limit the effective and safe application of these new drugs. Now that approved treatments are available, it becomes even more important to be aware of the clinical features of TD and when and how these new treatments can be applied to enhance successful outcomes and quality of life.
Frequency and risk of TD
The relative significance of TD as a clinical problem and the need for treatment have been questioned since the initial recognition of the disorder. Following early reports, several authorities questioned whether TD was related to treatment, how common it was and whether it was clinically significant.3–8 Early observers assumed that TD was rare and found primarily among elderly women with chronic conditions and brain damage, but this clearly reflected a skewed, selection bias based on studies of long-term residents in institutionalized settings.4,9 Although this bias that TD was uncommon and restricted to chronic mental illness was refuted by many reports among younger people who received dopamine-receptor blocking drugs for pain, gastrointestinal symptoms, or anxiety,3,10–12 it may once again become a concern as antipsychotics are widely marketed to an ever-expanding and more functional population of nonpsychotic patients with mood disorders and other indications. It is important to understand that anyone exposed to dopamine-receptor blocking drugs, not just those with chronic mental illness, may be at risk for TD.
In subsequent years, the frequency of TD has been convincingly demonstrated and repeatedly shown.13–15 Depending on the risk of the sample population studied and methodology of case detection, studies have shown a cumulative incidence of TD of about 4%–5% annually, with a prevalence rate of 20%–30%.16 Although younger patients are at risk for TD and may be particularly susceptible to more generalized and dystonic movements, older age has consistently been shown to be a major risk factor for TD. The annual incidence of TD in patients over the age of 45 years has been reported as 15%–30% after 1 year of treatment with a prevalence rate of up to 50%–60%.17 Previous studies on TD risk have less consistently suggested an association with female gender, race, higher ratings of negative symptoms and thought disorder, greater cognitive impairments, acute drug-induced movement disorders, substance abuse, and diabetes.18,19 Since both older adults and patients with schizophrenia have been found historically to have a predisposition for spontaneous dyskinesias,3 it is not surprising that they may be at greatest risk for TD.20 However, patients with mood disorders are also at risk and have been considered to be at high risk, although data supporting elevated risk for these patients from early studies may be confounded by the older age of depressed patients, gender bias, and the intermittent use of antipsychotics during sporadic episodes, all known risk factors for TD in their own right.21–23 The conclusion for practical purposes must be that regardless of diagnosis, TD is not rare and that anyone exposed to treatment with antipsychotics is at risk.
Differences in liability for TD between older first-generation antipsychotics (FGAs) and newer second-generation antipsychotics (SGAs) have been studied extensively. Comparing the incidence of TD with haloperidol, industry-sponsored trials of SGAs found a 6- to 12-fold reduction in risk for TD with newer agents.24–26 Subsequent trials using comparators with less potent dopamine-receptor binding affinity than haloperidol indicated that the advantages of SGAs in reducing risk of TD were diminished.27–30 But more recent studies confirmed that the relative risk (RR) of TD with SGAs is significantly less on average than that with FGAs (RR =0.47–0.68 of SGAs vs FGAs).14,31 The risk of TD associated with clozapine is probably least of all.32 The SGAs retain some risk, and since they are more broadly marketed, the absolute number of cases of TD is likely to increase. Thus, while there is some differential risk of TD among antipsychotics depending on dopamine-receptor binding affinity, no currently available antipsychotic is free of liability for TD. Longer duration of antipsychotic treatment and greater cumulative drug doses are considered additional risk factors for the development and persistence of TD.
Seriousness and impact of TD
Dismissal or neglect of TD and the need for treatment also derive from the impression in early studies that patients seemed unaware of or denied concern about TD.3,33,34 The resulting conventional wisdom that TD is unimportant may be an artifact of patient selection bias or the lack of rigorous investigations. Early reports that patients were indifferent to TD were based on older patients with chronic illnesses confined to institutions who were limited by psychosis and negative symptoms and impoverished by cognitive impairments, lack of insight, denial, and few opportunities for social engagement. While up to two thirds of these patients seemed unaware of TD movements, others admitted to being embarrassed by them.35–37 By contrast, a recent survey of outpatients with possible TD revealed that 70%–80% were aware of their movements and 50%–60% felt self-conscious or embarrassed by them.20
In assessing the seriousness of TD and need for treatment, clinicians should consider the objective severity of the movements and the functional impact on affected patients.3 Mild cases of TD may be suppressed, acceptable to the patient, or not readily noticeable apart from everyday habits, tics, and mannerisms that are commonly ignored even by normal individuals. However, moderate to severe movements may be intolerable, painful, physically disabling and eventuate in depression and even suicide.38,39 As antipsychotics are prescribed for more functional patients, however, TD is likely to be experienced as intolerable even in mild cases as a result of social embarrassment. Early impressions in chronic schizophrenia, that patients are unconcerned about TD, may be outdated given the evidence that it has physical, emotional, and social consequences that bear directly on clinical outcomes, functional recovery, and survival.40,41
A recent review summarized correlations between TD and impaired cognition, poor response to treatment, risk of relapse, longer hospital stays, lower quality of life, and increased mortality.42 However, these correlations are confounded by the effect of the underlying psychiatric illness, the severity of which contributes to the risk of both TD and poor outcomes. In other words, the association between TD, psychopathology, and poor response could be an artifact of treatment reflecting the fact that patients with severe psychoses and poor prognoses receive higher doses of antipsychotics for longer periods with poor adherence, resulting secondarily in a greater incidence of TD.3,42 There remains a pressing need to assess the psychological, physical, social, and economic burden of TD.43,44 This requires asking concrete, descriptive questions to patients and caregivers regarding specific circumstances in social situations where odd postures and movements invite ridicule and ostracism, and induce shame and withdrawal.3 Complacency is unacceptable regarding even mild cases of TD which can seriously impede social rehabilitation and recovery.
Onset of TD and screening methods
Given that TD may become persistent and irreversible, prevention by conservative use of antipsychotics and early detection is critical. Early diagnosis leading to antipsychotic drug cessation may increase the chances that movements will be transient and reversible.33,45,46 Therefore, the frequency and methods for screening should reflect the biology and time of onset of TD. Although evidence suggests that most cases of TD develop over months to years, with the risk correlating with duration and cumulative dose of antipsychotic treatment,47,48 there are reports of persistent movements arising within days to weeks after starting antipsychotics particularly among susceptible patients such as the elderly.49,50 Delineation of the time of onset of TD is confounded by the fact that TD could be masked or suppressed by antipsychotics and may first become apparent or worsen only after drug withdrawal in 5%–67% of patients.3,51,52 Although not accepted as a completely valid model for TD,53 dopamine-receptor supersensitivity in animal models usually develops quickly after 1 week of treatment and has occurred even after a single injection of an antipsychotic.54,55
By contrast, some criteria for the diagnosis of TD suggest a minimum duration of antipsychotic treatment of at least 3 months.56,57 Even less consistent with biological findings, guidelines for screening of TD suggest clinical assessment every 6 or 12 months for patients receiving FGAs or SGAs, respectively, reduced to 3 or 6 months for patients at heightened risk.58,59 But assessments conducted every 3 months or more are likely to miss a percentage of early cases of TD, preventing timely intervention and reducing chances of reversal. Paradoxically, the same guidelines recommend clinical assessment at every clinical visit to detect acute drug-induced movement disorders, for example, akathisia. These contradictions led the majority of experts in a recent Delphi consensus project on guidelines for managing TD to suggest that the lower limit of exposure to antipsychotics for TD to develop may be unknown but could reasonably be set at 1 month and that screening assessments therefore should be conducted at every clinical encounter.60
Regarding instruments for assessing the severity and extent of TD, the Abnormal Involuntary Movement Scale (AIMS) has achieved widespread acceptance as an easy-to-use and objective measure.61 The AIMS has been effective at enhancing compliance with routine monitoring and screening for TD and at fostering standardization and comparability between research trials.62,63 Of note, a recent expert consensus process on reporting outcomes of clinical trials based on AIMS data in clinically relevant terms concluded that no single analysis can be considered the standard of clinical efficacy and multiple analytic approaches are recommended.62 For clinicians, the complete AIMS examination can be time-consuming to conduct formally in a busy office practice, and efforts have been suggested to develop an abridged, simpler AIMS or other semi-structured examination and screening instrument that could be used more frequently and routinely during all clinical encounters.20,60
Diagnosis of TD
Research criteria for the diagnosis of TD based on AIMS scores developed by Schooler and Kane, which require a rating of moderate movements in at least one body area or ratings of at least mild in two body areas, played an invaluable role in standardizing the diagnosis across virtually all subsequent clinical and epidemiologic studies.56 A modification suggested by Glazer et al, which required only a total score of three with at least one body area rated as mild, offered a lower threshold but never gained currency in research studies.64 However, observation of even mild movements in one body area (ie, an AIMS score of 2) in a clinical practice setting may be significant and sufficient for the diagnosis of TD. For example, patients who become aware of and embarrassed by mild lip-smacking cannot be ignored. Recognition of incipient signs of TD such as tic-like orofacial or lingual movements or increased eye blink frequency may be critical in allowing early treatment intervention and prevention of worsening or generalization of movements.
Before selecting treatment options for TD, it is essential to distinguish TD from other movement disorders which may require very different management. In general, the differential diagnosis of movement disorders is complex with a long list of primary and secondary neurodegenerative disorders, structural abnormalities of the brain, and metabolic and toxic etiologies, many of which are quite rare and require collaboration with movement disorder specialists for in-depth evaluation.1 Potential clues to underlying disorders and the need for consultation include sudden onset or atypical or progressive course, positive family history, and associated systemic medical, neurological, laboratory or neuroimaging findings.
For the psychiatrist, the most likely disorders to differentiate from TD are spontaneous dyskinesias and other drug-induced movement disorders. Older people are at risk for spontaneous dyskinesias, especially involving orofacial muscles which may be associated with edentulousness or ill-fitting dentures.65,66 Psychomotor disorders are a core symptom dimension in schizophrenia and were recognized decades before antipsychotics were introduced.3,67–71 While TD may present in a variety of forms simulating classical neurological movement disorders (eg, chorea or dystonia), spontaneous movements found among psychiatric patients include a wide range of hyperkinetic (eg, mannerisms, stereotypies, compulsions) or hypokinetic behaviors (eg, psychomotor retardation, mutism, catalepsy).72 Clinicians and supporting staff may be misled by the fact that neurological movement disorders including TD often fluctuate with anxiety, arousal, and distraction, disappear during sleep, and can be suppressed by voluntary exertion, which often leads to misinterpreting drug-induced movement disorders as intentional “acting out” or attention-seeking behaviors.
It is also important to differentiate TD from acute drug-induced movement disorders. For example, drug-induced parkinsonism characterized by bradykinesia and tremor begins days to weeks after antipsychotic initiation and generally improves after antipsychotic discontinuation or with anticholinergic medications.73 Dopamine-depleting agents would significantly worsen parkinsonism. Similar considerations apply to acute drug-induced dystonic reactions and akathisia. Although movement disorders have been associated with other drug classes, TD-like movements that persist are unusual with drugs that do not block dopamine receptors.74
Treatment of TD
Once TD is detected, a practical management strategy entails a progressive series of steps consistent with standard patient care (Table 1).2,73,75 First, after visual inspection, a complete AIMS examination should be performed to document the severity and distribution of movements which could be monitored during subsequent treatment. Although not recorded on the AIMS, it would be prudent to also record the character or subtype of movements observed (eg, dystonia versus stereotyped movements). Second, a differential diagnosis should be considered to rule out spontaneous dyskinesias or other acute drug-induced movements, with neurological consultation if other less common disorders are suspected. Once TD is confirmed, a discussion should take place with patients and caregivers to inform them of the diagnosis, prognosis, and treatment options.58
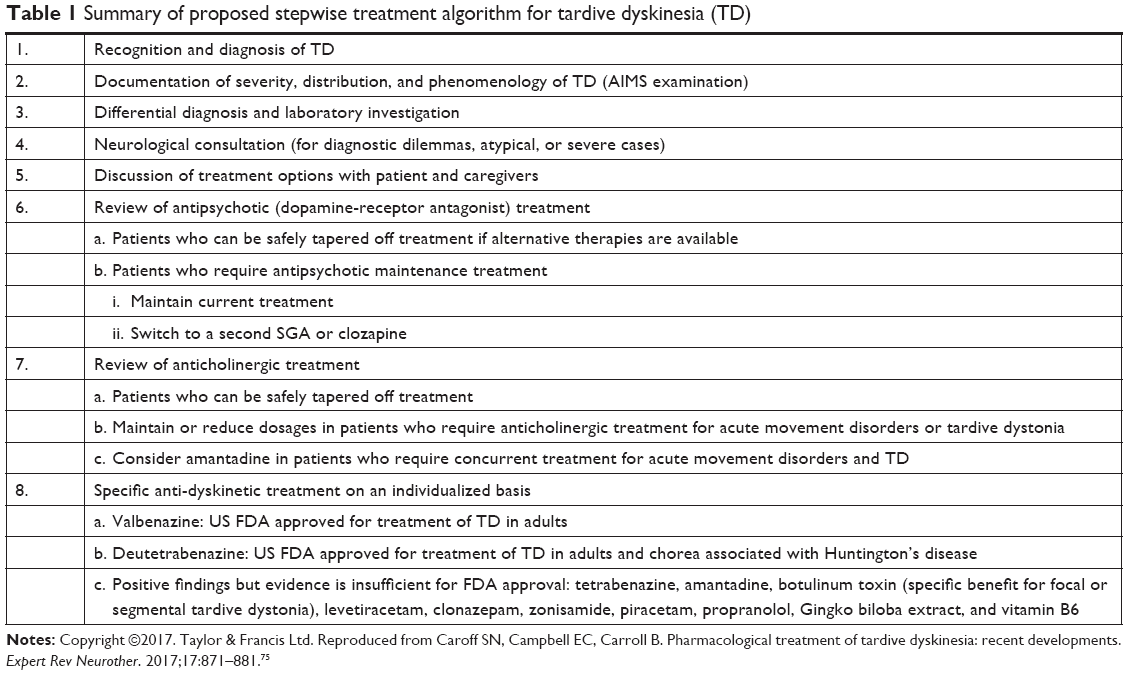 | Table 1 Summary of proposed stepwise treatment algorithm for tardive dyskinesia (TD) |
A number of pharmacological decisions then follow that are not necessarily mutually exclusive. Re-evaluating antipsychotic treatment is the first priority. Should the current antipsychotic be maintained, discontinued, reduced, or switched? In a patient with severe psychiatric illness at high risk for damaging relapse who is well-managed on current antipsychotic therapy but observed to have mild, localized TD with minimal subjective impact, maintenance of current treatment may be justified. In most cases, TD is not progressive even with continued antipsychotic treatment, although symptoms may worsen in some cases.42,76 Patients should provide informed consent with this plan and should be carefully monitored for any signs of progression. Alternatively and ideally, antipsychotics could be tapered off; in patients without an underlying psychotic disorder, such as those who develop TD while taking adjunctive dopamine antagonists for depression or for medical conditions, antipsychotics may be difficult to justify and could be safely discontinued. However, patients with schizophrenia or some cases of bipolar disorder may incur a significant risk of psychotic relapse and require ongoing maintenance treatment.77 Although drug withdrawal had been routinely recommended in past guidelines, about 33%–53% of patients were reported to experience worsening of dyskinesias initially, while 36%–55% may have shown improvement over time after FGAs were discontinued.78 But potential reversibility of TD after drug cessation has been controversial. While recent surveys suggest a grim prognosis with as few as 2% of patients showing resolution of TD several years after drug withdrawal in some studies,79,80 older reports found remission from TD a few months after drug cessation occurring in 50%–75% of patients if detected early.45,46 While these early cases may represent reversible withdrawal dyskinesias, they nevertheless support the potential efficacy of drug withdrawal in nonpsychotic patients as a management option.
Another recommended option has been dose reduction of antipsychotics. However, there is no evidence that this maneuver improves TD which in fact may temporarily worsen on decreased dosages. In addition, recent evidence suggests that dose reduction like drug cessation may contribute to symptom relapses and possible re-hospitalization, further eliminating this action as a reasonable treatment option for TD without additional evidence.81 Another alternative is to switch antipsychotics if maintenance treatment is necessary or if the patient requests a change from the agent that caused TD. A change to more potent antipsychotics or FGAs may suppress symptoms of TD in up to 67% of patients, although limiting remission of TD and potentially exacerbating parkinsonism and other acute drug-induced movements.82–84 One early study of the effects of FGAs on TD suggested that the suppressive effect was only temporary and TD symptoms may re-emerge during follow-up.85 Similarly, several studies of SGAs have shown reduction in TD severity, with some studies showing greater suppression, lesser suppression, or no difference compared with FGAs.42,86–88 In fact, studies of SGAs in suppressing TD have shown about a 3–4 point average decrease in the total AIMS severity scores which is comparable to decreases in recent trials of dopamine-depleting analogs of tetrabenazine,42,87 but at a cost of continued dopamine-receptor blockade which perpetuates the etiologic mechanism of TD and presumably restricts chances of remission.
If anticholinergic drugs have been prescribed, a decision should also be made about whether continuation is necessary or gradual tapering could be considered. Anticholinergic drugs probably worsen TD generally, such that improvement in TD severity ratings have been noted in up to 60% of patients withdrawn from these agents.75,82,84,89,90 But caution should be taken in decisions to reduce or taper anticholinergics if acute drug-induced movements (eg, parkinsonism, dystonia) or tardive dystonia are present as these disorders could re-emerge or worsen after withdrawal. Amantadine may be a reasonable alternative to anticholinergics in patients with TD and parkinsonism; it is now marketed in a long-acting formulation and evidence suggests it may have beneficial effects on both the movement disorder types.90–94
If TD remains a significant problem once antipsychotic treatment is optimized, specific anti-dyskinetic drugs should then be considered. A broad range of agents have been proposed as treatments for TD derived from theories of the underlying pathophysiology that identify potential targets. For example, the prevailing heuristic theory is the dopamine-receptor supersensitivity hypothesis which posits that prolonged dopamine-receptor blockade results in an increase in numbers or sensitivity of post-synaptic receptors.1,53–55 While helpful in understanding the causative and suppressive effects of drugs that affect dopaminergic neurotransmission at the clinical level, animal models of dopamine-receptor supersensitivity in rodents and primates are inexact; dyskinesias observed after drug administration in animals may develop sooner than TD, may not be age-related, and invariably resolve after drug cessation. Cholinergic compounds have been tried based on a theorized opposing balance between dopamine and acetylcholine in the basal ganglia and the finding of cholinergic cell loss in the striatum after administration of antipsychotics in rats.95 Similarly, animal studies revealing loss of striatal neurons containing gamma-aminobutyric acid (GABA) after antipsychotic treatment suggested that GABA-ergic compounds may alleviate TD.1 Findings in animal models which showed that dopaminergic blockade results in excess dopamine turnover and oxidative free radical formation formed the basis for trials of antioxidants.1 To synthesize these disparate effects of supersensitivity and interneuronal dysfunction underlying TD, animal models have been invoked to show that these abnormalities may in concert affect synaptic plasticity of glutaminergic synapses on striatal interneurons, resulting in an imbalance of the direct and indirect pathways, and abnormal output to the sensorimotor cortex.1,96,97
The record of clinical trials of agents to treat TD is extensive. Virtually all reviews and meta-analyses of these trials have concluded that the evidence on effectiveness for most of these agents remains preliminary and inconclusive.75,86,98,99 However, these reviews have been of limited usefulness to clinicians because they focus on trial design and statistical validity but less so on tolerability, reliability, and availability of products, while antipsychotics and anticholinergics are analyzed equally with specific antidyskinetics, apart from their psychiatric necessity. They conclude that treatments studied have limited evidence, based on small trials that are often underpowered, uncontrolled, unblinded, from single sites, or unreplicated. Though most agents did not meet the threshold of evidence to justify approval, some may have efficacy for subgroups of patients with TD if more definitive trials could be conducted, that is, absence of evidence is not evidence of absence!
In contrast, recent state-of-the-art randomized controlled trials have provided robust evidence on the efficacy and tolerability of two tetrabenazine analogs, valbenazine, and deutetrabenazine. These drugs act to deplete dopamine and thereby reduce the severity of TD, by inhibiting vesicular monoamine transporter-2 (VMAT-2) in nerve terminals, which ordinarily protects dopamine from metabolic breakdown by sequestering monoamines in protective vesicles. Tetrabenazine was initially synthesized as an antipsychotic and subsequently shown to suppress TD.100–102 Despite a lack of controlled trials of tetrabenazine, it is generally regarded as efficacious for the treatment of TD symptoms based on historical, open-label, observational studies, but is limited by a short half-life and side effects of sedation, parkinsonism, akathisia, and depression.103 Valbenazine and deutetrabenazine were designed with improved pharmacokinetics to allow for a longer half-life and reduced fluctuations associated with differences in genetic metabolic rate and drug interactions. Rigorous trials have confirmed that both drugs are more effective than placebo in reducing severity of TD and are better tolerated than tetrabenazine.75,101,102,104 The management of TD is, therefore, likely to be transformed with the introduction of these VMAT-2 inhibitors as approved treatments for TD. These agents have also renewed interest in many questions about the biology and management of TD. For example, although recent short-term and year-long extension trials of VMAT-2 inhibitors offer clear evidence of efficacy and tolerability in suppressing the severity of TD, even in patients continuing antipsychotic treatment, their impact on real-world, long-term outcomes remains to be investigated. There are as yet no head-to-head comparative trials of tetrabenazine and its analogs, so their relative effectiveness cannot be addressed. Similarly, comparisons between the VMAT-2 inhibitors and SGAs or other antidyskinetic agents have not been conducted, although tetrabenazine at least was shown to be more effective than haloperidol in suppressing TD.85 In addition, the relative cost-effectiveness of approved treatments remains controversial;105 ongoing studies of the social, psychological, and economic impact of TD are likely to provide crucial evidence to better inform cost–benefit treatment decisions in the near future.20
The interaction between the VMAT-2 inhibitors and antipsychotics has also raised interesting questions about synergistic antipsychotic effects. For example, if VMAT-2 inhibitors were added early in treatment in first-episode patients, would that allow lower doses of antipsychotics to be used and therefore possibly reduce the risk of TD? However, there are no animal or human data on the efficacy and safety of VMAT-2 inhibitors used for prophylactic purposes in preventing TD, such that this use is not advisable at this time. On the contrary, dopamine depletion, like denervation, may theoretically add to the risk of supersensitivity, synaptic dysplasticity, and TD from antipsychotic-induced dopamine-receptor blockade.97,106–109 But the risk of VMAT-2 inhibitors independently causing TD seems slight given the scarcity of such reports of TD associated with VMAT-2 inhibitors, despite recent and ongoing long-term studies of tetrabenazine and novel VMAT-2 inhibitors. While tetrabenazine may have dopamine-receptor blocking properties associated with a potential risk of TD and other drug-induced movement disorders, the risk may be lower with valbenazine, which was developed specifically without significant off-target receptor-binding properties, and with deutetrabenazine as a result of the lower doses that can be used effectively. Finally, the determination of risk for causing or contributing to TD attributed to VMAT-2 inhibitors is confounded by the fact that patients receiving these agents already have TD and are usually receiving concomitant antipsychotic medications.
To what extent might these agents facilitate remission or reversibility of TD long-term? By suppressing TD symptoms without blocking dopamine receptors, these agents might allow patients who do not require maintenance antipsychotics to tolerate drug withdrawal and therefore facilitate natural reversal of the mechanisms underlying TD, that is, as a “bridge to recovery”? As suggestive evidence, approximately 25%–30% of patients enrolled in long-term extension studies of valbenazine continued to show strong response in the reduction of TD even 4 weeks after withdrawal from valbenazine.110 Long-term withdrawal studies may provide answers in the future.
Conclusion
The availability of the VMAT-2 inhibitors may transform the treatment of TD, both in patients who may not require continued antipsychotic treatment and could be withdrawn from antipsychotics and in those with psychotic disorders who require maintenance antipsychotic treatment. Even so, these findings need to be tested in real-world settings over the long-term and taken into consideration as part of a broader, practical treatment algorithm (Table 1) that provides a stepwise approach to the management of patients affected by TD. Availability of these treatments may also rekindle interest in TD and the need for re-education and development of standardized practice guidelines. Additional research into TD should include investigations of underlying pathophysiological mechanisms, genetic predisposition, and the efficacy of other potential antidyskinetic drugs, especially those targeting non-dopaminergic mechanisms, with the ultimate goal of achieving true reversibility and remission of TD.
Disclosure
Dr Caroff served as a consultant for Neurocrine Biosciences, Teva Pharmaceuticals, Osmotica Pharmaceuticals, and DisperSol Technologies and received a research grant from Neurocrine Biosciences. The author reports no other conflicts of interest in this work.
References
Owens DGC. A Guide to the Extrapyramidal Side-Effects of Antipsychotic Drugs. 2nd ed. Cambridge (UK): Cambridge University Press; 2014. | ||
Caroff SN, Campbell EC. Drug-induced extrapyramidal syndromes: implications for contemporary practice. Psychiatr Clin North Am. 2016;39:391–411. doi:10.1016/j.psc.2016.04.003 | ||
Caroff SN, Ungvari GS, Cunningham Owens DG. Historical perspectives on tardive dyskinesia. J Neurol Sci. 2018;389:4–9. doi:10.1016/j.jns.2018.02.015 | ||
Kline NS. On the rarity of “irreversible” oral dyskinesias following phenothiazines. Am J Psychiatry. 1968;124:48–54. doi:10.1176/ajp.124.8S.48 | ||
Anonymous. The London letter. A side effect of phenothiazines. Can Med Assoc J. 1964;91:1081. | ||
Anonymous. Side-effects of phenothiazine drugs. Br J Med. 1964;2:1412. doi:10.1136/bmj.2.5422.1412 | ||
Anonymous. Irreversible side effects of phenothiazines. JAMA. 1965;191:333–334. | ||
Turek IS. Drug induced dyskinesia: reality or myth? Dis Nerv Syst. 1975;36:397–399. | ||
Brandon S, McClelland HA, Protheroe C. A study of facial dyskinesia in a mental hospital population. Br J Psychiatry. 1971;118:171–184. | ||
Evans JH. Persistent oral dyskinesia in treatment with phenothiazine derivatives. Lancet. 1965;1:458–460. | ||
Crane GE. Tardive dyskinesia in patients treated with major neuroleptics: a review of the literature. Am J Psychiatry. 1968;124(8S):40–48. doi:10.1176/ajp.124.8S.40 | ||
Klawans HL, Bergen D, Bruyn GW, Paulson GW. Neuroleptic-induced tardiave dyskinesias in nonpsychotic patients. Arch Neurol. 1974;30:338–339. | ||
Kane JM, Smith JM. Tardive dyskinesia: prevalence and risk factors, 1959 to 1979. Arch Gen Psychiatry. 1982;39:473–481. | ||
Carbon M, Kane JM, Leucht S, Correll CU. Tardive dyskinesia risk with first- and second-generation antipsychotics in comparative randomized controlled trials: a meta-analysis. World Psychiatry. 2018;17:330–340. doi:10.1002/wps.20579 | ||
Carbon M, Hsieh C-H, Kane JM, Correll CU. Tardive dyskinesia prevalence in the period of second-generation antipsychotic use: a meta-analysis. J Clin Psychiatry. 2017;78:e264–e278. doi:10.4088/JCP.16r10832 | ||
Kane JM. Tardive dyskinesia: epidemiological and clinical presentation. In: Bloom FE, Kupfer DJ, editors. Psychopharmacology: The Fourth Generation of Progress. New York: Raven Press; 1995:1485–1495. | ||
Jeste DV. Tardive dyskinesia in older patients. J Clin Psychiatry. 2000;61(Suppl 4):27–32. | ||
Miller DD, McEvoy JP, Davis SM, et al. Clinical correlates of tardive dyskinesia in schizophrenia: baseline data from the CATIE schizophrenia trial. Schizophr Res. 2005;80:33–43. doi:10.1016/j.schres.2005.07.034 | ||
Solmi M, Pigato G, Kane JM, Correll CU. Clinical risk factors for the development of tardive dyskinesia. J Neurol Sci. 2018;389:21–27. doi:10.1016/j.jns.2018.02.012 | ||
Caroff SN, Cutler AJ, Tanner CM, et al. Awareness and Impact of Possible Tardive Dyskinesia by Primary Psychiatric Diagnosis in Patients Prescribed Antipsychotics: Results from the RE-KINECT Study. Orlando (FL): Academy of Managed Care Pharmacy (AMCP) Nexus 2018; 2018. | ||
Keck PE Jr, McElroy SL, Strakowski SM, Soutullo CA. Antipsychotics in the treatment of mood disorders and risk of tardive dyskinesia. J Clin Psychiatry. 2000;61(Suppl 4):33–38. | ||
Coplan J, Gugger JJ, Tasleem H. Tardive dyskinesia from atypical antipsychotic agents in patients with mood disorders in a clinical setting. J Affect Disord. 2013;150:868–871. doi:10.1016/j.jad.2013.04.053 | ||
Rajan TM, Bharadwaj B, Rajkumar RP, Adole PS. Frequency and correlates of tardive dyskinesia in Indian patients with type I bipolar disorder. Asian J Psychiatr. 2018;32:92–98. doi:10.1016/j.ajp.2017.12.001 | ||
Correll CU, Leucht S, Kane JM. Lower risk for tardive dyskinesia associated with second-generation antipsychotics: a systematic review of 1-year studies. Am J Psychiatry. 2004;161:414–425. doi:10.1176/appi.ajp.161.3.414 | ||
Beasley CM, Dellva MA, Tamura RN, et al. Randomised double-blind comparison of the incidence of tardive dyskinesia in patients with schizophrenia during long-term treatment with olanzapine or haloperidol. Br J Psychiatry. 1999;174:23–30. | ||
Jeste DV, Lacro JP, Bailey A, Rockwell E, Harris MJ, Caligiuri MP. Lower incidence of tardive dyskinesia with risperidone compared with haloperidol in older patients. J Am Geriatr Soc. 1999;47:716–719. | ||
Correll CU, Schenk EM. Tardive dyskinesia and new antipsychotics. Curr Opin Psychiatry. 2008;21:151–156. doi:10.1097/YCO.0b013e3282f53132 | ||
Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209–1223. doi:10.1056/NEJMoa051688 | ||
Miller DD, Caroff SN, Davis SM, et al. Extrapyramidal side-effects of antipsychotics in a randomised trial. Br J Psychiatry. 2008;193:279–288. doi:10.1192/bjp.bp.108.050088 | ||
Leucht S, Wahlbeck K, Hamann J, Kissling W. New generation antipsychotics versus low-potency conventional antipsychotics: a systematic review and meta-analysis. Lancet. 2003;361:1581–1589. doi:10.1016/S0140-6736(03)13306-5 | ||
Woods SW, Morgenstern H, Saksa JR, et al. Incidence of tardive dyskinesia with atypical versus conventional antipsychotic medications: a prospective cohort study. J Clin Psychiatry. 2010;71:463–474. doi:10.4088/JCP.07m03890yel | ||
Kane JM, Woerner MG, Pollack S, Safferman AZ, Lieberman JA. Does clozapine cause tardive dyskinesia? J Clin Psychiatry. 1993;54:327–330. | ||
Crane GE. Prevention and management of tardive dyskinesia. Am J Psychiatry. 1972;129:466–467. doi:10.1176/ajp.129.4.466 | ||
Alexopoulos GS. Lack of complaints in schizophrenics with tardive dyskinesia. J Nerv Ment Dis. 1979;167:125–127. | ||
Macpherson R, Collis R. Tardive dyskinesia. Patients’ lack of awareness of movement disorder. Br J Psychiatry. 1992;160:110–112. | ||
Marsden CD, Tarsy D, Baldessarini RJ. Spontaneous and drug-induced movement disorders in psychotic patients. In: Benson DF, Blumer D, editors. Psychiatric Aspects of Neurologic Disease. New York: Grune & Stratton; 1975:219–253. | ||
Sandyk R, Kay SR, Awerbuch GI. Subjective awareness of abnormal involuntary movements in schizophrenia. Int J Neurosci. 1993;69:1–20. | ||
Yassa R. Functional impairment in tardive dyskinesia: medical and psychosocial dimensions. Acta Psychiatr Scand. 1989;80:64–67. | ||
Tarsy D. History and definition of tardive dyskinesia. Clin Neuropharmacol. 1983;6:91–99. | ||
Ascher-Svanum H, Zhu B, Faries D, Peng X, Kinon BJ, Tohen M. Tardive dyskinesia and the 3-year course of schizophrenia: results from a large, prospective, naturalistic study. J Clin Psychiatry. 2008;69:1580–1588. | ||
Browne S, Roe M, Lane A, et al. Quality of life in schizophrenia: relationship to sociodemographic factors, symptomatology and tardive dyskinesia. Acta Psychiatr Scand. 1996;94:118–124. | ||
Caroff SN, Davis VG, Miller DD, et al. Treatment outcomes of patients with tardive dyskinesia and chronic schizophrenia. J Clin Psychiatry. 2011;72:295–303. doi:10.4088/JCP.09m05793yel | ||
Strassnig M, Rosenfeld A, Harvey PD. Tardive dyskinesia: motor system impairments, cognition and everyday functioning. CNS Spectr. 2018;23:370–377. | ||
Cloud LJ, Zutshi D, Factor SA. Tardive dyskinesia: therapeutic options for an increasingly common disorder. Neurotherapeutics. 2014;11:166–176. doi:10.1007/s13311-013-0222-5 | ||
Quitkin F, Rifkin A, Gochfeld L, Klein DF. Tardive dyskinesia: are first signs reversible? Am J Psychiatry. 1977;134:84–87. doi:10.1176/ajp.134.1.84 | ||
Jeste DV, Potkin SG, Sinha S, Feder S, Wyatt RJ. Tardive dyskinesia–reversible and persistent. Arch Gen Psychiatry. 1979;36:585–590. | ||
Crane GE. Persistent dyskinesia. Br J Psychiatry. 1973;122:395–405. | ||
Faurbye A, Rasch PJ, Petersen PB, Brandborg G, Pakkenberg H. Neurological symptoms in pharmacotherapy of psychoses. Acta Psychiatr Scand. 1964;40:10–27. | ||
Schonecker M. [Paroxysmal dyskinesia as the effect of megaphen]. Nervenarzt. 1957;28:550–553. | ||
Uhrbrand L, Faurbye A. Reversible and irreversible dyskinesia after treatment with perphenazine, chlorpromazine, reserpine, and electroconvulsive therapy. Psychopharmacologia. 1960;1:408–418. doi:10.1007/BF00441188 | ||
Kane JM, Woerner M, Lieberman J. Tardive dyskinesia: prevalence, incidence, and risk factors. J Clin Psychopharmacol. 1988;8:52S–56S. | ||
Turek I, Kurland AA, Hanlon TE, Bohm M. Tardive dyskinesia: its relation to neuroleptic and antiparkinson drugs. Br J Psychiatry. 1972;121:605–612. | ||
Jeste DV, Lohr JB, Kauffmann CA, Wyatt RJ. Pathophysiology of tardive dyskinesia; Evaluation of supersensitivity theory and alertnative hypotheses. In: Casey DE, Gardos G, editors. Tardive Dyskinesia and Neuroleptics: From Dogma to Reason. Washington (DC): American Psychiatric Press, Inc.; 1986:15–32. | ||
Moore KE. Dyskinesia: animal experimental correlates. Acta Psychiatr Scand. 1981;63:88–102. doi:10.1111/j.1600-0447.1981.tb02461.x | ||
Christensen AV, Fjalland B, Nielsen IM. On the supersensitivity of dopamine receptors, induced by neuroleptics. Psychopharmacology. 1976;48:1–6. | ||
Schooler NR, Kane JM. Research diagnoses for tardive dyskinesia. Arch Gen Psychiatry. 1982;39:486–487. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington (DC): American Psychiatric Press, Inc.; 1994. | ||
American Psychiatric Association. Tardive Dyskinesia: A Task Force Report of the American Psychiatric Association. American Psychiatric Press. Inc. Washington (DC); 1992. | ||
Lehman AF, Lieberman JA, Dixon LB, et al. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry. 2004;161:1–56. | ||
Caroff SN, Citrome L, Meyer J, et al. A Modified Delhi Consensus Approach to Clinical Guidelines for Tardive Dyskinesia. New York: Annual Meeting of the American Psychiatric Association; 2018. | ||
Guy W. Abnormal Involuntary Movement Scale (AIMS). ECDEU Assessment Manual for Psychopharmacology Revised: Alcohol, Drug Abuse and Mental Health Administration. National Institute of Mental Health. Rockville, MD; 1976:534–537. | ||
Kane JM, Correll CU, Nierenberg AA, Caroff SN, Sajatovic M. Tardive Dyskinesia Assessment Working Group. Revisiting the abnormal involuntary movement scale: proceedings from the tardive dyskinesia assessment workshop. J Clin Psychiatry. 2018;79(3):17cs11959. | ||
Munetz MR, Schulz SC. Screening for tardive dyskinesia. J Clin Psychiatry. 1986;47:75–77. | ||
Glazer WM, Morgenstern H, Doucette JT. Predicting the long-term risk of tardive dyskinesia in outpatients maintained on neuroleptic medications. J Clin Psychiatry. 1993;54:133–139. | ||
Lieberman J, Kane JM, Woerner M, Weinhold P. Prevalence of tardive dyskinesia in elderly samples. Psychopharmacol Bull. 1984;20:22–26. | ||
Kane JM, Weinhold P, Kinon B, Wegner J, Leader M. Prevalence of abnormal involuntary movements (“spontaneous dyskinesias”) in the normal elderly. Psychopharmacology. 1982;77:105–108. | ||
Manschreck TC, Kopala LC, Honer WG. Neurological comorbidity and features in schizophrenia. In: Meyer JM, Nasrallah HA, editors. Medical Illness and Schizophrenia. Arlington (VA): American Psychiatric Publishing, Inc.; 2003:185–214. | ||
Peralta V, Cuesta MJ. Motor abnormalities: from neurodevelopmental to neurodegenerative through “functional” (neuro)psychiatric disorders. Schizophr Bull. 2017;43:956–971. doi:10.1093/schbul/sbx089 | ||
Pappa S, Dazzan P. Spontaneous movement disorders in antipsychotic-naive patients with first-episode psychoses: a systematic review. Psychol Med. 2009;39:1065–1076. doi:10.1017/S0033291708004716 | ||
Khot V, Wyatt RJ. Not all that moves is tardive dyskinesia. Am J Psychiatry. 1991;148:661–666. doi:10.1176/ajp.148.5.661 | ||
Fenton WS. Prevalence of spontaneous dyskinesia in schizophrenia. J Clin Psychiatry. 2000;61(Suppl 4):10–14. | ||
Richard I, O’Brien C, Kurlan R. Spontaneous movement disorders in psychiatric patients. In: Factor SA, Lang AE, Weiner WJ, editors. Drug Induced Movement Disorders. 2nd ed. Malden (MA): Blackwell Publishing, Inc.; 2005:30–52. | ||
Citrome L. Reprint of: clinical management of tardive dyskinesia: five steps to success. J Neurol Sci. 2018;389:61–66. doi:10.1016/j.jns.2018.02.037 | ||
D’Abreu A, Friedman JH. Tardive dyskinesia-like syndrome due to drugs that do not block dopamine receptors: rare or non-existent: literature review. Tremor Other Hyperkinet Mov (New York, NY). 2018;8:570. | ||
Caroff SN, Campbell EC, Carroll B. Pharmacological treatment of tardive dyskinesia: recent developments. Expert Rev Neurother. 2017;17:871–881. doi:10.1080/14737175.2017.1358616 | ||
Margolius A, Fernandez HH. Current treatment of tardive dyskinesia. Parkinsonism Relat Disord. 2018. [Epub Dec 19]. doi:10.1016/j.parkreldis.2018.12.022 | ||
Gilbert PL, Harris MJ, McAdams LA, Jeste DV. Neuroleptic withdrawal in schizophrenic patients. A review of the literature. Arch Gen Psychiatry. 1995;52:173–188. doi:10.1001/archpsyc.1995.03950150005001 | ||
Casey DE, Gerlach J. Tardive dyskinesia: what is the long-term outcome? In: Casey DE, Gardos G, editors. Tardive Dyskinesia and Neuroleptics: From Dogma to Reason. Washington (DC): American Psychiatric Press, Inc.; 1986:76–97. | ||
Zutshi D, Cloud LJ, Factor SA. Tardive syndromes are rarely reversible after discontinuing dopamine receptor blocking agents: experience from a university-based movement disorder clinic. Tremor Other Hyperkinet Mov (N Y). 2014;4:266. | ||
Glazer WM, Moore DC, Schooler NR, Brenner LM, Morgenstern H. Tardive dyskinesia. A discontinuation study. Arch Gen Psychiatry. 1984;41:623–627. | ||
Caroff SN, Mu F, Ayyagari R, Schilling T, Abler V, Carroll B. Hospital utilization rates following antipsychotic dose reductions: implications for tardive dyskinesia. BMC Psychiatry. 2018;18:306. doi:10.1186/s12888-018-1889-2 | ||
Egan MF, Apud J, Wyatt RJ. Treatment of tardive dyskinesia. Schizophr Bull. 1997;23:583–609. | ||
Mentzel CL, Bakker PR, van Os J, et al. Effect of antipsychotic type and dose changes on tardive dyskinesia and parkinsonism severity in patients with a serious mental illness: the curacao extrapyramidal syndromes study XII. J Clin Psychiatry. 2017;78:e279–e285. doi:10.4088/JCP.16m11049 | ||
Soares-Weiser K, Fernandez HH. Tardive dyskinesia. Semin Neurol. 2007;27:159–169. doi:10.1055/s-2007-971169 | ||
Kazamatsuri H, Chien CP, Cole JO. Long-term treatment of tardive dyskinesia with haloperidol and tetrabenazine. Am J Psychiatry. 1973;130:479–483. doi:10.1176/ajp.130.4.479 | ||
Bhidayasiri R, Fahn S, Weiner WJ, Gronseth GS, Sullivan KL, Zesiewicz TA. Evidence-based guideline: treatment of tardive syndromes: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;81:463–469. doi:10.1212/WNL.0b013e31829d86b6 | ||
Mentzel TQ, van der Snoek R, Lieverse R, et al. Clozapine monotherapy as a treatment for antipsychotic-induced tardive dyskinesia: a meta-analysis. J Clin Psychiatry. 2018;79(6):17r11852. doi:10.4088/JCP.su17023ah3c | ||
Tarsy D, Baldessarini RJ, Tarazi FI. Effects of newer antipsychotics on extrapyramidal function. CNS Drugs. 2002;16:23–45. doi:10.2165/00023210-200216010-00003 | ||
Greil W, Haag H, Rossnagl G, Ruther E. Effect of anticholinergics on tardive dyskinesia. A controlled discontinuation study. Br J Psychiatry. 1984;145:304–310. | ||
Ward KM, Citrome L. Antipsychotic-related movement disorders: drug-induced parkinsonism vs. tardive dyskinesia-key differences in pathophysiology and clinical management. Neurol Ther. 2018;7:233–248. doi:10.1007/s40120-018-0105-0 | ||
Pappa S, Tsouli S, Apostolou G, Mavreas V, Konitsiotis S. Effects of amantadine on tardive dyskinesia: a randomized, double-blind, placebo-controlled study. Clin Neuropharmacol. 2010;33:271–275. | ||
Elkurd MT, Bahroo LB, Pahwa R. The role of extended-release amantadine for the treatment of dyskinesia in Parkinson’s disease patients. Neurodegener Dis Manag. 2018;8:73–80. doi:10.2217/nmt-2018-0001 | ||
Fann WE, Lake CR. Amantadine versus trihexyphenidyl in the treatment of neuroleptic-induced parkinsonism. Am J Psychiatry. 1976;133:940–943. doi:10.1176/ajp.133.8.940 | ||
DiMascio A, Bernardo DL, Greenblatt DJ, Marder JE. A controlled trial of amantadine in drug-induced extrapyramidal disorders. Arch Gen Psychiatry. 1976;33:599–602. | ||
Margolese HC, Chouinard G, Kolivakis TT, Beauclair L, Miller R. Tardive dyskinesia in the era of typical and atypical antipsychotics. Part 1: pathophysiology and mechanisms of induction. Can J Psychiatry. 2005;50:541–547. doi:10.1177/070674370505000907 | ||
Teo JT, Edwards MJ, Bhatia K. Tardive dyskinesia is caused by maladaptive synaptic plasticity: a hypothesis. Mov Disord. 2012;27:1205–1215. doi:10.1002/mds.25107 | ||
Borgkvist A, Lieberman OJ, Sulzer D. Synaptic plasticity may underlie l-DOPA induced dyskinesia. Curr Opin Neurobiol. 2018;48:71–78. doi:10.1016/j.conb.2017.10.021 | ||
Bhidayasiri R, Jitkritsadakul O, Friedman JH, Fahn S. Updating the recommendations for treatment of tardive syndromes: a systematic review of new evidence and practical treatment algorithm. J Neurol Sci. 2018;389:67–75. doi:10.1016/j.jns.2018.02.010 | ||
Soares-Weiser K, Rathbone J, Ogawa Y, Shinohara K, Bergman H. Miscellaneous treatments for antipsychotic-induced tardive dyskinesia. Cochrane Database Syst Rev. 2018;3:Cd000208. | ||
Brandrup E. Tetrabenacine treatment in persisting dyskinesia caused by psychopharmaca. Am J Psychiatry. 1961;118:551–552. doi:10.1176/ajp.118.6.551 | ||
Caroff SN, Aggarwal S, Yonan C. Treatment of tardive dyskinesia with tetrabenazine or valbenazine: a systematic review. J Comp Eff Res. 2018;7:135–148. doi:10.2217/cer-2017-0065 | ||
Scorr LM, Factor SA. VMAT2 inhibitors for the treatment of tardive dyskinesia. J Neurol Sci. 2018;389:43–47. doi:10.1016/j.jns.2018.02.006 | ||
Jankovic J, Clarence-Smith K. Tetrabenazine for the treatment of chorea and other hyperkinetic movement disorders. Expert Rev Neurother. 2011;11:1509–1523. doi:10.1586/ern.11.149 | ||
Citrome L. Tardive dyskinesia: placing vesicular monoamine transporter Type 2 (VMAT2) inhibitors into clinical perspective. Expert Rev Neurother. 2018;18:323–332. doi:10.1080/14737175.2018.1455504 | ||
Atlas SJ, Agboola F, Curfman G. Effectiveness and value of 2 novel treatments for tardive dyskinesia. JAMA Intern Med. 2018;178:1110–1112. doi:10.1001/jamainternmed.2018.2463 | ||
LeWitt PA. Tardive dyskinesia caused by tetrabenazine. Clin Neuropharmacol. 2013;36:92–93. doi:10.1097/WNF.0b013e318290cd41 | ||
Mandel RJ, Hartgraves SL, Severson JA, Woodward JJ, Wilcox RE, Randall PK. A quantitative estimate of the role of striatal D-2 receptor proliferation in dopaminergic behavioral supersensitivity: the contribution of mesolimbic dopamine to the magnitude of 6-OHDA lesion-induced agonist sensitivity in the rat. Behav Brain Res. 1993;59:53–64. | ||
Moy SS, Criswell HE, Breese GR. Differential effects of bilateral dopamine depletion in neonatal and adult rats. Neurosci Biobehav Rev. 1997;21:425–435. | ||
Kostrzewa RM, Brus R. Lifelong rodent model of tardive dyskinesia-persistence after antipsychotic drug withdrawal. Curr Top Behav Neurosci. 2016;29:353–362. doi:10.1007/7854_2015_395 | ||
Caroff SN, Lindenmayer JP, Farahmand K, Burke J, Siegert S. Characteristics of patients with tardive dyskinesia who maintain treatment response after discontinuing long-term valbenazine: pooled analysis of two trials. The American College of Neuropsychopharmacology Annual Meeting; 2018; Hollywood, FL. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.