")
Back to Journals » Patient Related Outcome Measures » Volume 9
Outcomes in adult pectus excavatum patients undergoing Nuss repair
Authors Ewais MM, Chaparala S , Uhl R , Jaroszewski DE
Received 4 July 2017
Accepted for publication 9 November 2017
Published 30 January 2018 Volume 2018:9 Pages 65—90
DOI https://doi.org/10.2147/PROM.S117771
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland

MennatAllah M Ewais, Shivani Chaparala, Rebecca Uhl, Dawn E Jaroszewski
Department of Cardiothoracic Surgery, Mayo Clinic Hospital, Phoenix, AZ, USA
Abstract: Pectus excavatum (PEx) is one of the most common congenital chest wall deformities. Depending on the severity, presentation of PEx may range from minor cosmetic issues to disabling cardiopulmonary symptoms. The effect of PEx on adult patients has not been extensively studied. Symptoms may not occur until the patient ages, and they may worsen over the years. More recent publications have implied that PEx may have significant cardiopulmonary implications and repair is of medical benefit. Adults presenting for PEx repair can undergo a successful repair with a minimally invasive “Nuss” approach. Resolution of symptoms, improved quality of life, and satisfying results are reported.
Keywords: complications, minimally invasive surgery, quality of life
Background
Pectus excavatum (PEx) is the most common congenital chest wall anomaly.1–4 The deformity is reported to occur more frequently in males than females; however, diagnosis in females may often be missed if obscured with breast tissue.5–7 Depending on the severity, presentation of PEx may range from a minor cosmetic issue to disabling cardiopulmonary symptoms.8–10 The internally displaced sternum can cause right-side heart compression and restrictive deficits.8,9 As the patient advances in age, the chest wall can become less flexible as a result of increased calcium accumulation in cartilage attachments of the anterior chest wall.11,12 Symptoms may occur or show progression as the patient ages.11–13 Kragten et al12 reported development of symptoms in the fourth and fifth decade in nearly half of their adult patients with significant improvement after surgical repair. The optimal surgical procedure for adult PEx patients has been controversial, and some surgeons recommend limiting the Nuss procedure to pediatrics and adolescents.14,15 We present a review of adult patients with PEx including outcomes after repair with Nuss (“Nuss”) or a minimally invasive repair of pectus excavatum (MIRPEx).
Cardiopulmonary outcomes
The cardiopulmonary effects of PEx have been debated for years, 16–18 and there is a paucity of reports evaluating adult patients.19,20 The inward deformity of the anterior chest wall has a negative cardiopulmonary consequence on patients with PEx, as supported by the most recent data.9,21 This can cause displacement of the heart into the left chest and varying degrees of heart compression (Figure 1). Decrease in atrial filling and venous return can result in diastolic dysfunction and reduction in cardiac output with significant compression to the chambers of the right heart.9,20–22 Mocchegiani et al23 reported that the right ventricular outflow tract in PEx patients was significantly narrower and right ventricle (RV) end-diastolic and-systolic areas were significantly smaller. Surgical correction of the PEx has been shown to relieve compression, allowing for a significant increase in right heart chamber size, increased flow velocities, and improved cardiac output9,21,24 (Figure 2A and B). Krueger et al25 also noted significant improvement in post-repair cardiac outputs that increased to 66.2% vs 58.4% and the end-diastolic RV volume that increased to a mean of 40.8 mL vs 21.7 mL preoperatively. There may be a greater impact on cardiac function and symptoms in patients over 30 years of age.12,24 In post-repair PEx patients ≥30 years, a mean increase in right ventricular output of 65% was documented by intraoperative transesophageal echocardiogram.24 Neviere et al26 found that PEx deformity was associated with reduction in the strength of the inspiratory muscle as evident by reduction in the maximal static respiratory pressure (PImax) and sniff nasal inspiratory pressure (SNIP) with significant increase of these values postoperatively which was reflected in enhanced efficacy of the respiratory pump and the cardiovascular function improvement.
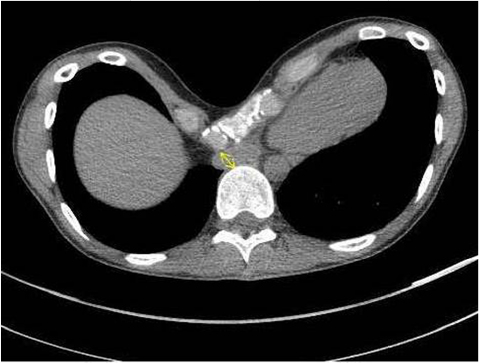 | Figure 1 Computerized tomographic scan of a patient with severe pectus excavatum and Haller index of 24.6. Sternal deformity with compression of the right heart and inflow are seen (arrow). |
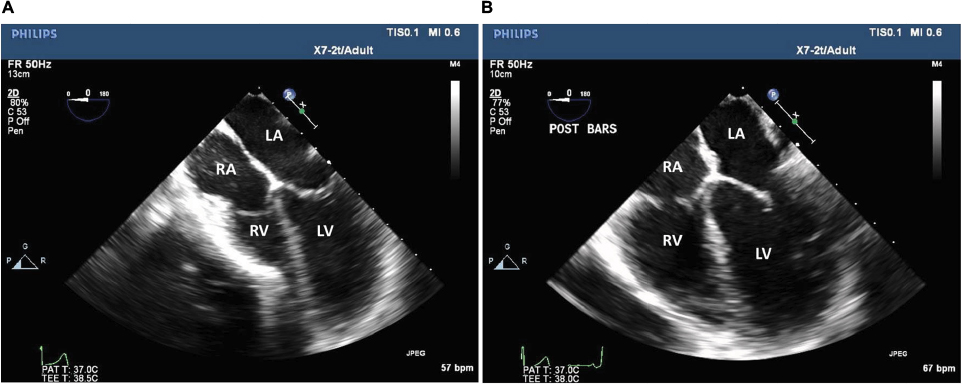 | Figure 2 Transesophageal echocardiographic images show preoperative effect (A) of pectus excavatum with compression on the right ventricle due to the inward sternal deformity and relief of the compression following surgical repair (B). Abbreviations: RV, right ventricle; LV, left ventricle; RA, right atrium; LA, left atrium. |
Long-term follow-up of corrected PEx patients and correlations between physiologic impact and symptoms are lacking.8,27–30 Table 1 reviews some of the major publications reporting cardiopulmonary impairments and postsurgical results. Only six of these represented a mean age of 18 years and older.9,19,25,26,31,32 Cardiopulmonary exercise testing has been used to assess exercise capacity and limitations in peak oxygen uptake and O2 pulse which can result as a consequence of the pectus deformity.18,19,33,34 Publications as to the benefits of surgical correction have varied.8,19,31,35 Several studies have reported that the cardiopulmonary function has improved significantly with increase in the oxygen consumption (VO2) and O2 pulse after surgical repair of PEx.8,19 Maagaard et al35 previously reported normalization of the decreased cardiopulmonary function in teenagers with PEx at 3 years following surgical repair; however, in a more recent evaluation of adult patients by Udholm et al31 (≥21 years), a significant improvement in the maximum oxygen consumption (VO2 max) was not seen 1 year after PEx repair. These results did show a trend of increased improvement in the VO2 max which could be more evident with a longer period of follow-up. Adult patients may also differ in their ability to return to normal after PEx repair. During assessment, the patient’s baseline exercise history must be considered. Cardiac output and deconditioning can occur with postoperative inactivity;36 therefore, the patient’s exercise history can affect the measurements of VO2 and may cause more impact on short-term testing results.34
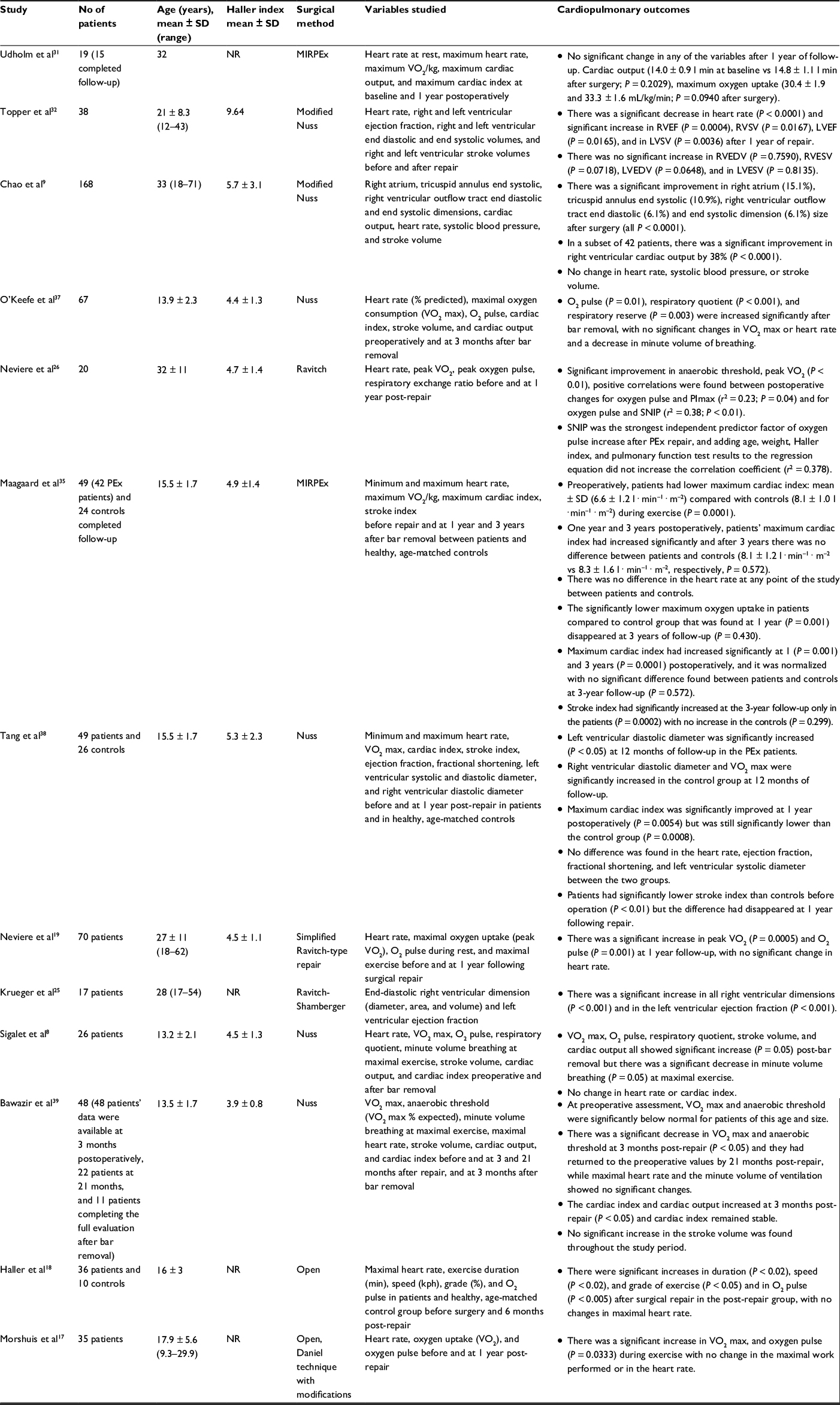 | Table 1 Review of major publications reporting cardiopulmonary outcomes and postsurgical results Abbreviations: MIRPEx, minimally invasive repair of pectus excavatum; RV, right ventricle; LV, left ventricle; EF, ejection fraction; SV, stroke volume; EDV, end-diastolic volume; ESV, end-systolic volume, PImax, maximal static respiratory pressure; SNIP, sniff nasal inspiratory pressure; PEx, pectus excavatum; NR, not reported. |
Quality of life and patient satisfaction
Both the exercise limitations and the cosmetic disfigurement with PEx may cause a decrease in quality of life and alteration of social behavior.37,40–44 There has been a greater recognition of the physiologic and psychologic impact of these patients.45 Lack of self-confidence, poor body image, avoidance of social activities, and emotional difficulties are noted in PEx patients. Feelings of anxiety, depression, sadness, and frustration are also reported.40 The importance of corrective surgery for improvement in psychological distress, quality of life, and exercise tolerance has been documented in the literature.37,41–44 The majority of these studies report a mixed population of children and adolescents with few adults; therefore, it is difficult to make broad-based assumptions as to their application to the adult population.46–50 Table 2 reviews some of the major publications44,48–50,53,54 reporting postsurgical quality of life and symptom outcomes.
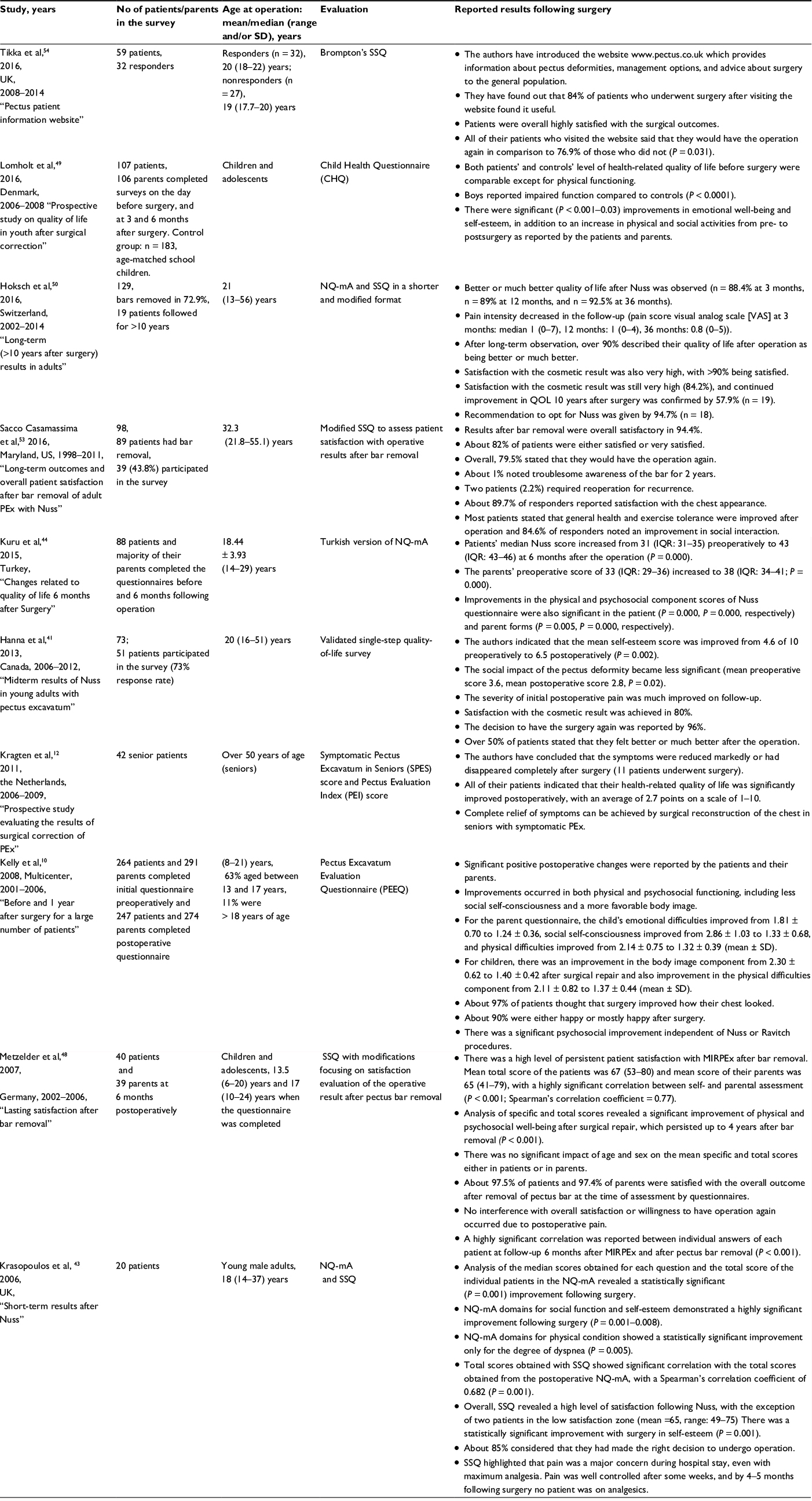 | Table 2 Review of major publications from 2006–2016 reporting quality of life and patient satisfaction after pectus excavatum repair Abbreviations: MIRPEx, minimally invasive repair of pectus excavatum; NQ-mA, Nuss questionnaire modified for Adults; SSQ, single-step questionnaire; QOL, quality of life; PEx, pectus excavatum; IQR, interquartile range. |
Kelly et al10 reported on 264 child patients and 291 parents from multiple centers using a validated Pectus Excavatum Evaluation Questionnaire. Children noted a dramatic improvement in the body image and physical difficulties after surgery. Parents also noticed an improvement in the child’s emotional, physical difficulties and social self-consciousness.10 Patient’s satisfaction with the chest appearance was found to be very good, with excellent to good results reported in over 95% of patients at the time of bar removal.51
In a 2016 study performed by Lomholt et al,49 107 patients and 106 parents completed the generic health-related quality-of-life measure. The Child Health Questionnaire was assessed preoperatively and at 3, 6 months following PEx repair. A control group of 183 school children completed the same measure on one occasion. In the postoperative study, patients and parents reported improved emotional well-being and self-esteem. Additionally, patients at both 3 and 6 months postoperatively reported increased physical and social activities.
There are very few major publications that documented symptoms and quality-of-life improvement after Nuss repair in adult patients. Kragten et al12 reported on symptomatic seniors with PEx. He found that in 45% of the patients with “serious and sometimes invalidating complaints”, symptoms did not start until the fourth or fifth decade of life and were often labeled as “unexplained cardiovascular complaints”. All patients that underwent surgery were repaired by the open Ravitch procedure and reported substantial or complete resolution of the symptoms postoperatively. Tikka et al52 used the Brompton’s single-step questionnaire (SSQ) to assess the postoperative patient satisfaction and confirmed that Nuss operation had positively impacted the psychological and physical status of their patients along with overall quality-of-life improvement. They reported that their pectus patient information website improved, additionally, their patient’s satisfaction and recovery after surgery.
Krasopoulos et al43 proposed the two-step Nuss Questionnaire modified for Adults (NQ-mA) and a SSQ. These questionnaires measured the disease-specific quality-of-life changes after surgery and assessed the effect of surgery on the physical and psychological well-being of postoperative patients. They noted that patients’ self-esteem, social functioning, and level of satisfaction were significantly improved following Nuss procedure. Their questionnaire also included the impact of surgical wounds/scars on the overall cosmetic result, consciousness of the presence of metallic bar, the decision to have the operation again, and questions about postoperative pain which may have limited the patient satisfaction after surgery. It was evident from the study that most of the patients were very satisfied with their scars and almost all of them were conscious of the presence of bar, but none of them considered that to be a major inconvenience. Pain was also noted as a concern in the immediate postoperative period; however, it decreased significantly after several weeks. By 4–5 months after surgery, no patient was still requiring analgesics.
Other surgeons have subsequently utilized this modified survey for assessing the patients postoperatively.48,50,53 Hoksch et al50 performed a prospective study to evaluate the long-term results of Nuss in adults using NQ-mA and SSQ in a shorter and modified format. Initially, a large adult cohort (n = 129) was included, but only19 patients were observed for >10 years after surgery. This has been the only study reporting outcomes for an adult population for more than 10 years after surgery. The results obtained initially after surgery were in the follow-up period of 3, 12 and 36 months showed high levels of satisfaction respectively reported at 97.6%, 97.2%, and 95.7%. Better or much better quality of life was reported at 3, 12, and 36 months in 88%, 89%, and increased to 92.5%, respectively, in the follow-up period. Even after observation for >10 years, continued improvement in quality of life was confirmed in 57.9% of patients. Surgical recommendation for Nuss was given by nearly 95% of patients. Mild pain occurring during specific bodily movements was reported in 31.6%, and 63.2% of patients had no pain.
Sacco Casamassima et al53 in 2016 reported long-term results of adults using modified SSQ. Satisfaction with the chest wall appearance was reported in 89% out of 43.8% of responders. Improvement in social interaction was reported by 84% of responders. About 94% of patients obtained overall satisfaction with the results post-bar removal. They also highlighted that the dissatisfaction observed by some patients was due to severe postoperative chest pain (that necessitates more aggressive analgesic regimen) and surgical scars. Willingness to have the operation again was reported by 79% of responders. Generalized conclusions cannot be drawn from this study as it is limited by small sample size. There is a compelling need for a large number of similar studies commenting on the long-term results in adults to identify the benefits of surgery in this group.
Hanna et al41 studied the midterm results in young adults who underwent Nuss repair and used the single-step quality-of-life survey for evaluation. With a 73% response rate, they noticed an improvement in both self-esteem and social life. Satisfaction with the cosmetic result was achieved in 80% and recommendation for the surgery was given by 96% of their patients. About 92% reported subjective improvement in the chest wall appearance. As stated by other authors, in-hospital pain despite aggressive analgesic usage was a major concern in the immediate postoperative period; however, in the follow-up it was significantly decreased, with almost all patients reporting minimal or no pain.
Most of the data available suggest that patients who had undergone Nuss showed an overall satisfaction with the cosmetic result, had a significant improvement in self-image, and felt that the surgery had a positive impact on their ability to exercise and well-being.
Surgical approaches and outcomes
The Nuss procedure or “MIRPEx” has become the standard of care for PEx repair in children and adolescents.64 There is an ongoing discussion in the literature regarding the success of this surgery in adults with PEx. Initial reports of Nuss procedure in adults were criticized due to higher complication rates vs the open Ravitch technique with most being related to bar migration, postoperative pain, and recurrences. 65–67 The recommendations of some surgeons were to limit the procedure to pediatrics and adolescents; however, their publications have been replaced with numerous series of successful repairs using a modified MIRPEx approach.24,68,69 Table 3 reviews publications reporting on 70 or more adults repaired using an MIRPEx procedure since 2008. The majority of authors considered patients aged 18 years and older as adults. 28,51,57,63,70,71 Several papers have stratified their results to differentiate younger vs older patients.24,30 There is evidence that older patients are more difficult to treat and the risk of complications may be greater.14 Despite this, excellent results are achieved with an MIRPEx approach even in older adult patients15,24,28–30,43,63,68,69,71–73 (Figure 3A–D).
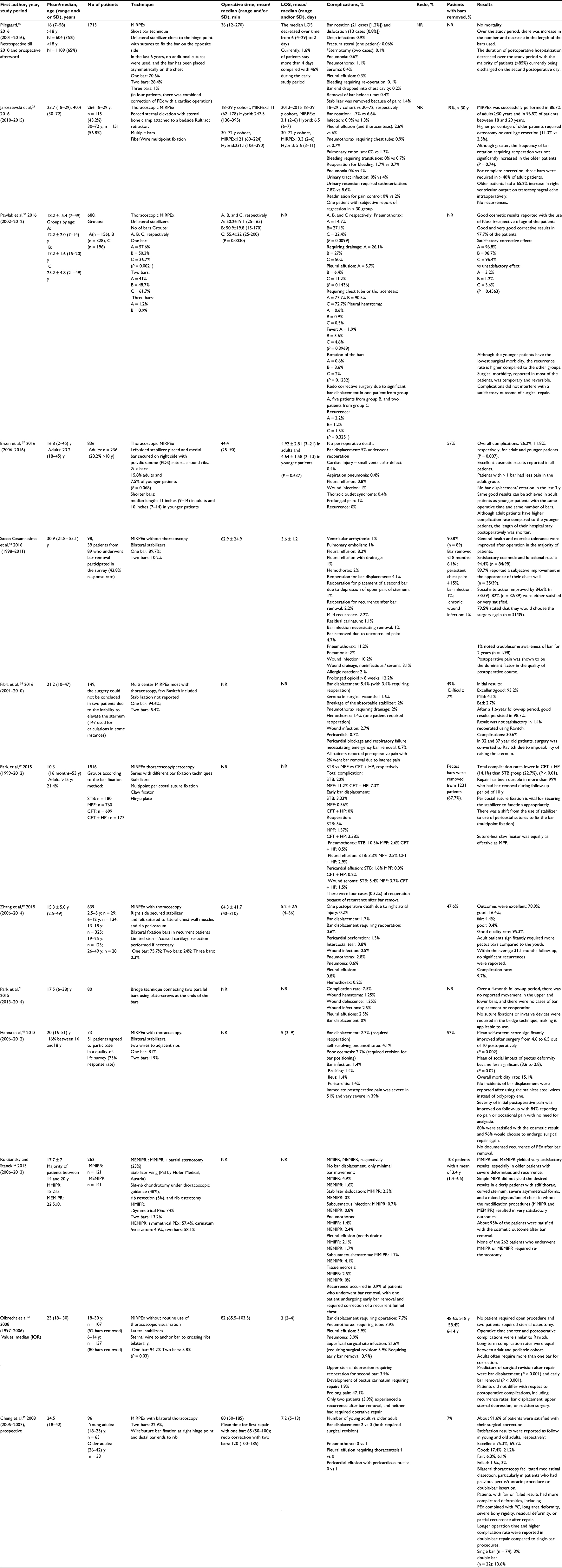 | Table 3 Review of some of the recent studies and reported results from 2008–2016 after Nuss procedure for pectus excavatum repair in adults Note: *Both sternotomies were done in re-do cases: one was due to inferior vena cava bleeding and one was due to right ventricle tear caused by an adhesion, from the primary Nuss correction. Abbreviations: NR, not reported; SD, standard deviation; LOS, length of stay; y, year; MIRPEx, minimally invasive repair of pectus excavatum; STB, stabilizer; MPF, multipoint pericostal fixation; CFT, claw fixator; HP, hinge plate; MIPR, minimally invasive pectus repair; MMIPR, modified minimally invasive pectus repair; MEMIPR, modified extended minimally invasive pectus repair; PEx, pectus excavatum; PC, pectus carinatum; QOL, quality of life; IQR, interquartile range; PSI, Pectus Security Implant. |
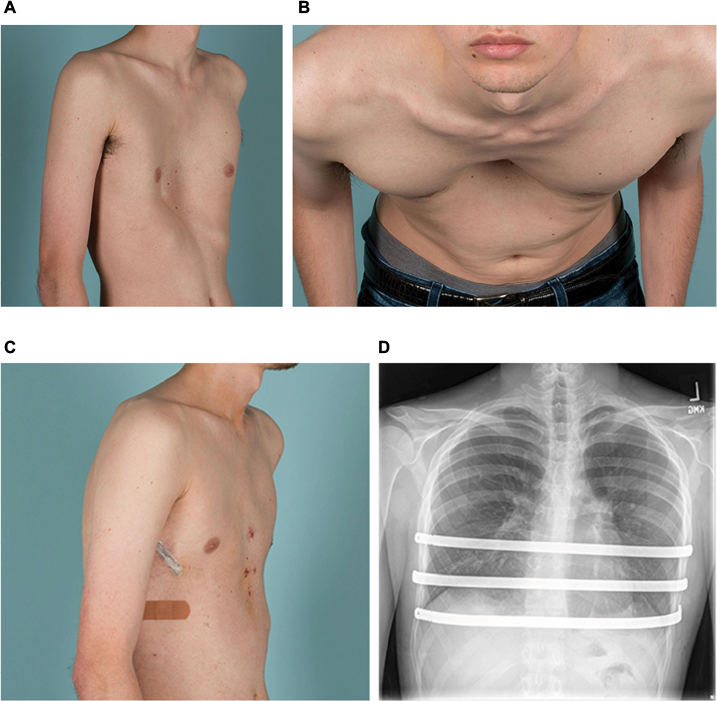 | Figure 3 Clinical photographs of a 22-year-old man with severe pectus excavatum are shown before surgery (A, B) and after (C) minimally invasive repair of pectus excavatum, with placement of three Nuss bars as shown in the chest roentgenogram (D). |
Since the introduction of the original Nuss technique for children in 1998,64 several changes have been made in the surgical technique and methods of bar stabilization which have improved the success of the procedure in adult patients.24,28,72,74–78 Important modifications include the use of forced sternal elevation,78 multiple support bars,24,77 and improved fixation methods to secure the bars and prevent rotation.24,28,72,74–78 These technical refinements enabled successful MIRPEx repair of older patients and are reviewed in Table 4.
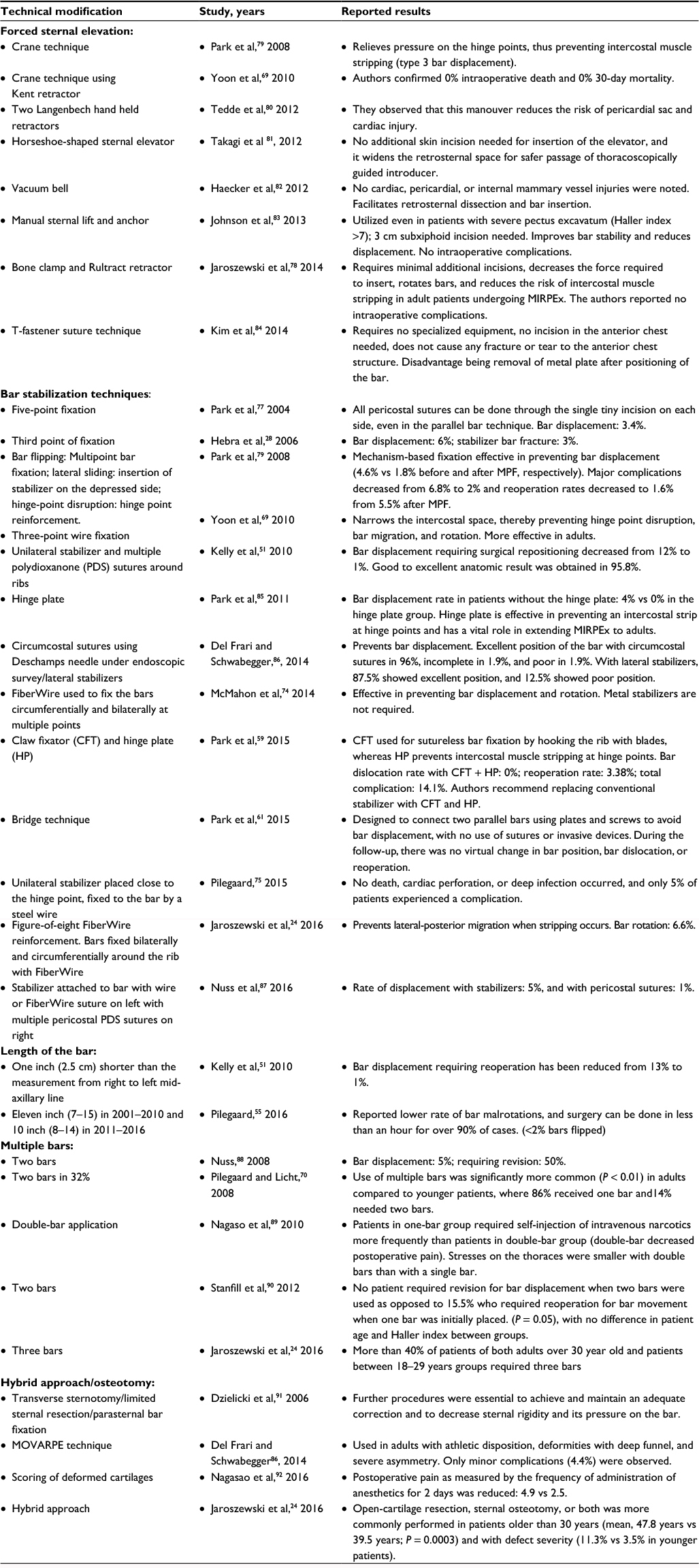 | Table 4 Review of several technical modifications reported for minimally invasive repair of pectus excavatum in adults Abbreviations: MIRPEx, minimally invasive repair of pectus excavatum; MPF, multipoint pericostal bar fixation; MOVARPE, minor open videoendoscopic assisted repair of pectus excavatum. |
The use of forced sternal elevation may help reduce the force required to insert and rotate bars (Figure 4). This may lessen, but not eliminate, lateral stripping of the intercostal muscles of the more rigid chest wall.69,78,79,81,82,84 Several techniques have been proposed for the forceful elevation of sternum. Park et al79 reported his Crane technique and discussed the benefits of its use in adult patients with heavier chests and severely asymmetric deformities including prevention of intercostal muscle tear and bar displacement. Similar variations of this technique have been reported by others with similar beneficial results.69,78,81,82,84 A more simplified aspect of handheld retractors can also be utilized, depending on the severity and rigidity of the defect.80,83
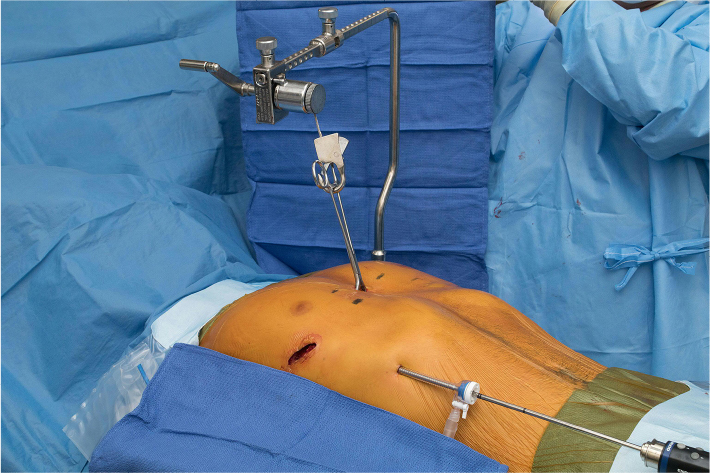 | Figure 4 The Rultract retractor can be utilized to forcefully elevate the sternum when attached by a bone clamp. |
Multiple bars may balance the increased pressure of the chest wall and in older patients, the use of two or more bars is frequently reported.24,70,77,90 The risk of bar rotation and malposition may also be decreased by distributing the pressure of a more rigid chest wall.70,77,90 Pilegaard68 reported that 70% of his patients over 30 years of age required two or more bars. In our own practice, two or more bars were utilized in 99% of patients over age 18 years,24 with 40% of patients over 30 years receiving three bars to achieve complete repair. Others have reported decreased risk of bar migration and the need of reoperation when multiple bars were utilized.70,77,90 In a study of PEx repair in 44 late adolescent and adult patients, 11.5% of those with single-bar repairs required reoperation for incomplete correction or bar rotation compared with 0% who had a double-bar repair. Double bar also decreases the postoperative pain as described by Nagaso et al.89 The risk of bar rotation may be lowered by the use of shorter bars as reported by several surgeons.93,94 In a publication reporting Nuss revision after procedure failure, too long bars were noted to be a factor related to failure.95
The biggest challenge in adult patients continues to be bar fixation. A higher rate of bar displacement is reported in older patients.14,24 There are multiple successful ways reported for securing of bars. Medial fixation with a hinge reinforcement plate,85 medially placed stabilizers,75 multipoint fixation,24,69,77 and the Bridge technique, which was more recently published,61 have all been successful methods for bar fixation in adult patients.72,79,87,96
Chondroplasty or open osteotomy may still be necessary to achieve adequate repair in some adult patients. Patients with complex combined deformities, extensively calcified chest walls, and significant asymmetry may require an open repair for optimal correction. The requirement for osteotomy or cartilage resection is more commonly reported in older patients.24,91,97,98 In our experience, over 88% of the patients ≥30 years were successfully repaired with MIRPEx; however, some required an osteotomy or open resection for fracture. Postoperative pain may also be reduced by scoring of deformed cartilages as illustrated by Nagasao et al.92 The use of a hybrid procedure may also be considered and is our procedure of choice for these more difficult deformities.24 Both surgical principles are utilized by incorporating osteotomy cuts and external fixation as well as pectus support bars. Achieving adequate postoperative pain control remains a concern for adults undergoing Nuss.99 Various analgesic regimens have been discussed by several authors.100 Perioperative pain can be well managed by current techniques.101 These include the use of thoracic epidurals, intravenous on-demand patient-administrated narcotics, local paravertebral blocks, and subcutaneous continuous flow catheters.102–106 We have had excellent results using a protocol including gabapentin, ibuprofen, acetaminophen, and narcotics along with subcutaneous continuous flow catheters for postoperative pain control.24,102,107 Adjuvant medications for postoperative pain management have included the use of ketorolac, diazepam, and gabapentin.103–106 Intraoperative use of methadone can also be advantageous.24,102
Discussion
The extension of the Nuss procedure to repair adults with PEx has been controversial in the past.14,65–67 There are now multiple publications that report successful repair of adults even beyond 50 years of age.9,12,24,55 The difficulty of repair and risk of complications do, however, increase with age.14,24,53 Adequate surgical experience with the Nuss procedure in younger patients that are easier to repair is critical prior to attempting the more difficult adult deformity. Bar rotation and migration can be a significant issue and techniques to minimize intercostal stripping, such as reinforcement of intercostal spaces24,59,87 and medially placed stabilizers, may be of benefit in reducing the risks.75 The use of forced sternal elevation can also decrease the forces required for bar insertion and positioning.69,78–84 The adult chest wall has additional complexities due to the decrease in flexibility and increase in weight. Multiple bars have been noted to decrease the weight supported by an individual bar and decrease the risk of rotation.24,70,88–90 Adequate stabilization of bars is also critical due to these factors, and medial and/or multipoint fixation has been shown to reduce bar displacement.24,28,51,59,61,69,75,86,87 We did not intend this publication to be an intensive review of surgical techniques in adult patients, and the majority of information presented was based on a larger case series which reported on primary Nuss repair in the adult population. Extension of the Nuss procedure to more complex repairs, such as patients with prior sternotomy or cardiac surgery, is beyond the scope of this paper and can be associated with catastrophic complications.55,108
Conclusion
MIRPEx can be extended to repair the majority of older adult patients. Although adults undergoing Nuss procedure may have a higher rate of complications, continuous technical refinements have significantly reduced the complication rates and contributed to the success of the procedure. As there is increased difficulty in performing this procedure in adult patients, the experience and expertise of surgeons at specialized centers is critical for successful outcomes. There is enough evidence to validate repair of adults with PEx. Published data support the benefits of repair with good outcomes and improvement of symptoms.
Disclosure
The authors report no conflicts of interest in this work.
References
Fokin AA, Steuerwald NM, Ahrens WA, Allen KE. Anatomical, histologic, and genetic characteristics of congenital chest wall deformities. Semin Thorac Cardiovasc Surg. 2009;21(1):44–57. | ||
Scherer LR, Arn PH, Dressel DA, Pyeritz RM, Haller JA, Jr. Surgical management of children and young adults with Marfan syndrome and pectus excavatum. J Pediatr Surg. 1988;23(12):1169–1172. | ||
Cobben JM, Oostra RJ, van Dijk FS. Pectus excavatum and carinatum. Eur J Med Genet. 2014;57(8):414–417. | ||
Chung CS, Myrianthopoulos NC. Factors affecting risks of congenital malformations. I. Analysis of epidemiologic factors in congenital malformations. Report from the Collaborative Perinatal Project. Birth Defects Orig Artic Ser. 1975;11(10):1–22. | ||
Fonkalsrud EW. Management of pectus chest deformities in female patients. Am J Surg. 2004;187(2):192–197. | ||
Ma IT, Rebecca AM, Notrica DM, McMahon LE, Jaroszewski DE. Pectus excavatum in adult women: repair and the impact of prior or concurrent breast augmentation. Plast Reconstr Surg. 2015;135(2):303e–312e. | ||
Park HJ, Gu JH, Jang JC, Dhong ES, Yoon ES. Correction of pectus excavatum with breast hypoplasia using simultaneous pectus bar procedure and augmentation mammoplasty. Ann Plast Surg. 2014;73(2):190–195. | ||
Sigalet DL, Montgomery M, Harder J, Wong V, Kravarusic D, Alassiri A. Long term cardiopulmonary effects of closed repair of pectus excavatum. Pediatr Surg Int. 2007;23(5):493–497. | ||
Chao CJ, Jaroszewski DE, Kumar PN, et al. Surgical repair of pectus excavatum relieves right heart chamber compression and improves cardiac output in adult patients – an intraoperative transesophageal echocardiographic study. Am J Surg. 2015;210(6):1118–1124. | ||
Kelly RE, Jr., Cash TF, Shamberger RC, et al. Surgical repair of pectus excavatum markedly improves body image and perceived ability for physical activity: multicenter study. Pediatrics. 2008;122(6):1218–1222. | ||
Jaroszewski DE, Fonkalsrud EW. Repair of pectus chest deformities in 320 adult patients: 21 year experience. Ann Thorac Surg. 2007;84(2):429–433. | ||
Kragten HA, Siebenga J, Hoppener PF, Verburg R, Visker N. Symptomatic pectus excavatum in seniors (SPES): a cardiovascular problem?: a prospective cardiological study of 42 senior patients with a symptomatic pectus excavatum. Neth Heart J. 2011;19(2):73–78. | ||
Jaroszewski D, Steidley E, Galindo A, Arabia F. Treating heart failure and dyspnea in a 78-year-old man with surgical correction of pectus excavatum. Ann Thorac Surg. 2009;88(3):1008–1010. | ||
Kim do H, Hwang JJ, Lee MK, Lee DY, Paik HC. Analysis of the Nuss procedure for pectus excavatum in different age groups. Ann Thorac Surg. 2005;80(3):1073–1077. | ||
Esteves E, Paiva KC, Calcagno-Silva M, Chagas CC, Barbosa-Filho H. Treatment of pectus excavatum in patients over 20 years of age. J Laparoendosc Adv Surg Tech A. 2011;21(1):93–96. | ||
Kaguraoka H, Ohnuki T, Itaoka T, Kei J, Yokoyama M, Nitta S. Degree of severity of pectus excavatum and pulmonary function in preoperative and postoperative periods. J Thorac Cardiovasc Surg. 1992;104(5):1483–1488. | ||
Morshuis WJ, Folgering HT, Barentsz JO, Cox AL, van Lier HJ, Lacquet LK. Exercise cardiorespiratory function before and one year after operation for pectus excavatum. J Thorac Cardiovasc Surg. 1994;107(6):1403–1409. | ||
Haller JA Jr, Loughlin GM. Cardiorespiratory function is significantly improved following corrective surgery for severe pectus excavatum. Proposed treatment guidelines. J Cardiovasc Surg (Torino). 2000;41(1):125–130. | ||
Neviere R, Montaigne D, Benhamed L, et al. Cardiopulmonary response following surgical repair of pectus excavatum in adult patients. Eur J Cardiothorac Surg. 2011;40(2):e77–e82. | ||
Malek MH, Fonkalsrud EW, Cooper CB. Ventilatory and cardiovascular responses to exercise in patients with pectus excavatum. Chest. 2003;124(3):870–882. | ||
Gurkan U, Aydemir B, Aksoy S, et al. Echocardiographic assessment of right ventricular function before and after surgery in patients with pectus excavatum and right ventricular compression. Thorac Cardiovasc Surg. 2014;62(3):231–235. | ||
Coln E, Carrasco J, Coln D. Demonstrating relief of cardiac compression with the Nuss minimally invasive repair for pectus excavatum. J Pediatr Surg. 2006;41(4):683–686; discussion 683–686. | ||
Mocchegiani R, Badano L, Lestuzzi C, Nicolosi GL, Zanuttini D. Relation of right ventricular morphology and function in pectus excavatum to the severity of the chest wall deformity. Am J Cardiol. 1995;76(12):941–946. | ||
Jaroszewski DE, Ewais MM, Chao CJ, et al. Success of minimally invasive pectus excavatum procedures (modified Nuss) in adult patients (±=30 years). Ann Thorac Surg. 2016;102(3):993–1003. | ||
Krueger T, Chassot PG, Christodoulou M, Cheng C, Ris HB, Magnusson L. Cardiac function assessed by transesophageal echocardiography during pectus excavatum repair. Ann Thorac Surg. 2010;89(1):240–243. | ||
Neviere R, Benhamed L, Duva Pentiah A, Wurtz A. Pectus excavatum repair improves respiratory pump efficacy and cardiovascular function at exercise. J Thorac Cardiovasc Surg. 2013;145(2):605–606. | ||
Kelly RE Jr, Mellins RB, Shamberger RC, et al. Multicenter study of pectus excavatum, final report: complications, static/exercise pulmonary function, and anatomic outcomes. J Am Coll Surg. 2013;217(6):1080–1089. | ||
Hebra A, Jacobs JP, Feliz A, Arenas J, Moore CB, Larson S. Minimally invasive repair of pectus excavatum in adult patients. Am Surg. 2006;72(9):837–842. | ||
Aronson DC, Bosgraaf RP, van der Horst C, Ekkelkamp S. Nuss procedure: pediatric surgical solution for adults with pectus excavatum. World J Surg. 2007;31(1):26–29; discussion 30. | ||
Cheng YL, Lee SC, Huang TW, Wu CT. Efficacy and safety of modified bilateral thoracoscopy-assisted Nuss procedure in adult patients with pectus excavatum. Eur J Cardiothorac Surg. 2008;34(5):1057–1061. | ||
Udholm S, Maagaard M, Pilegaard H, Hjortdal V. Cardiac function in adults following minimally invasive repair of pectus excavatum. Interact Cardiovasc Thorac Surg. 2016;22(5):525–529. | ||
Topper A, Polleichtner S, Zagrosek A, et al. Impact of surgical correction of pectus excavatum on cardiac function: insights on the right ventricle. A cardiovascular magnetic resonance studydagger. Interact Cardiovasc Thorac Surg. 2016;22(1):38–46. | ||
Albouaini K, Egred M, Alahmar A, Wright DJ. Cardiopulmonary exercise testing and its application. Heart. 2007;93(10):1285–1292. | ||
Malek MH, Coburn JW. Strategies for cardiopulmonary exercise testing of pectus excavatum patients. Clinics (Sao Paulo). 2008;63(2):245–254. | ||
Maagaard M, Tang M, Ringgaard S, et al. Normalized cardiopulmonary exercise function in patients with pectus excavatum three years after operation. Ann Thorac Surg. 2013;96(1):272–278. | ||
Perhonen MA, Franco F, Lane LD, et al. Cardiac atrophy after bed rest and spaceflight. J Appl Physiol (1985). 2001;91(2):645–653. | ||
O’Keefe J, Byrne R, Montgomery M, Harder J, Roberts D, Sigalet DL. Longer term effects of closed repair of pectus excavatum on cardiopulmonary status. J Pediatr Surg. 2013;48(5):1049–1054. | ||
Tang M, Nielsen HH, Lesbo M, et al. Improved cardiopulmonary exercise function after modified Nuss operation for pectus excavatum. Eur J Cardiothorac Surg. 2012;41(5):1063–1067. | ||
Bawazir OA, Montgomery M, Harder J, Sigalet DL. Midterm evaluation of cardiopulmonary effects of closed repair for pectus excavatum. J Pediatr Surg. 2005;40(5):863–867. | ||
Jaroszewski D, Notrica D, McMahon L, Steidley DE, Deschamps C. Current management of pectus excavatum: a review and update of therapy and treatment recommendations. J Am Board Fam Med. 2010;23(2):230–239. | ||
Hanna WC, Ko MA, Blitz M, Shargall Y, Compeau CG. Thoracoscopic Nuss procedure for young adults with pectus excavatum: excellent midterm results and patient satisfaction. Ann Thorac Surg. 2013;96(3):1033–1036; discussion 1037–1038. | ||
Jacobsen EB, Thastum M, Jeppesen JH, Pilegaard HK. Health-related quality of life in children and adolescents undergoing surgery for pectus excavatum. Eur J Pediatr Surg. 2010;20(2):85–91. | ||
Krasopoulos G, Dusmet M, Ladas G, Goldstraw P. Nuss procedure improves the quality of life in young male adults with pectus excavatum deformity. Eur J Cardiothorac Surg. 2006;29(1):1–5. | ||
Kuru P, Bostanci K, Ermerak NO, Bahadir AT, Afacan C, Yuksel M. Quality of life improves after minimally invasive repair of pectus excavatum. Asian Cardiovasc Thorac Ann. 2015;23(3):302–307. | ||
Steinmann C, Krille S, Mueller A, Weber P, Reingruber B, Martin A. Pectus excavatum and pectus carinatum patients suffer from lower quality of life and impaired body image: a control group comparison of psychological characteristics prior to surgical correction. Eur J Cardiothorac Surg. 2011;40(5):1138–1145. | ||
Kelly RE, Jr. Pectus excavatum: historical background, clinical picture, preoperative evaluation and criteria for operation. Semin Pediatr Surg. 2008;17(3):181–193. | ||
Krasopoulos G, Goldstraw P. Minimally invasive repair of pectus excavatum deformity. Eur J Cardiothorac Surg. 2011;39(2):149–158. | ||
Metzelder ML, Kuebler JF, Leonhardt J, Ure BM, Petersen C. Self and parental assessment after minimally invasive repair of pectus excavatum: lasting satisfaction after bar removal. Ann Thorac Surg. 2007;83(5):1844–1849. | ||
Lomholt JJ, Jacobsen EB, Thastum M, Pilegaard H. A prospective study on quality of life in youths after pectus excavatum correction. Ann Cardiothorac Surg. 2016;5(5):456–465. | ||
Hoksch B, Kocher G, Vollmar P, Praz F, Schmid RA. Nuss procedure for pectus excavatum in adults: long-term results in a prospective observational study. Eur J Cardiothorac Surg. 2016;50(5):934–939. | ||
Kelly RE, Goretsky MJ, Obermeyer R, et al. Twenty-one years of experience with minimally invasive repair of pectus excavatum by the Nuss procedure in 1215 patients. Ann Surg. 2010;252(6):1072–1081. | ||
Tikka T, Kalkat MS, Bishay E, Steyn RS, Rajesh PB, Naidu B. A 20-year review of pectus surgery: an analysis of factors predictive of recurrence and outcomes. Interact Cardiovasc Thorac Surg. 2016;23(6):908–913. | ||
Sacco Casamassima MG, Gause C, Goldstein SD, et al. Patient satisfaction after minimally invasive repair of pectus excavatum in adults: long-term results of Nuss procedure in adults. Ann Thorac Surg. 2016;101(4):1338–1345. | ||
Tikka T, Webb J, Agostini P, et al. Pectus patient information website has improved access to care and patient reported outcomes. J Cardiothorac Surg. 2016;11(1):69. | ||
Pilegaard HK. Single centre experience on short bar technique for pectus excavatum. Ann Cardiothorac Surg. 2016;5(5):450–455. | ||
Pawlak K, Gasiorowski L, Gabryel P, Galecki B, Zielinski P, Dyszkiewicz W. Early and late results of the Nuss procedure in surgical treatment of pectus excavatum in different age groups. Ann Thorac Surg. 2016;102(5):1711–1716. | ||
Ersen E, Demirkaya A, Kilic B, et al. Minimally invasive repair of pectus excavatum (MIRPE) in adults: is it a proper choice? Wideochir Inne Tech Maloinwazyjne. 2016;11(2):98–104. | ||
Fibla JJ, Molins L, Moradiellos J, et al. Experience with the Nuss technique for the treatment of pectus excavatum in Spanish thoracic surgery departments. Cir Esp. 2016;94(1):38–43. | ||
Park HJ, Kim KS, Lee S, Jeon HW. A next-generation pectus excavatum repair technique: new devices make a difference. Ann Thorac Surg. 2015;99(2):455–461. | ||
Zhang DK, Tang JM, Ben XS, et al. Surgical correction of 639 pectus excavatum cases via the Nuss procedure. J Thorac Dis. 2015;7(9):1595–1605. | ||
Park HJ, Kim KS, Moon YK, Lee S. The bridge technique for pectus bar fixation: a method to make the bar un-rotatable. J Pediatr Surg. 2015;50(8):1320–1322. | ||
Rokitansky AM, Stanek R. Modified minimally invasive pectus repair in children, adolescents and adults: an analysis of 262 patients. Pneumologia. 2013;62(4):224–231. | ||
Olbrecht VA, Arnold MA, Nabaweesi R, et al. Lorenz bar repair of pectus excavatum in the adult population: should it be done? Ann Thorac Surg. 2008;86(2):402–408; discussion 408–409. | ||
Nuss D, Kelly RE Jr, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg. 1998;33(4):545–552. | ||
Johnson WR, Fedor D, Singhal S. Systematic review of surgical treatment techniques for adult and pediatric patients with pectus excavatum. J Cardiothorac Surg. 2014;9:25. | ||
Hebra A, Swoveland B, Egbert M, et al. Outcome analysis of minimally invasive repair of pectus excavatum: review of 251 cases. J Pediatr Surg. 2000;35(2):252–257; discussion 257–258. | ||
Kanagaratnam A, Phan S, Tchantchaleishvili V, Phan K. Ravitch versus Nuss procedure for pectus excavatum: systematic review and meta-analysis. Ann Cardiothorac Surg. 2016;5(5):409–421. | ||
Pilegaard HK. Extending the use of Nuss procedure in patients older than 30 years. Eur J Cardiothorac Surg. 2011;40(2):334–337. | ||
Yoon YS, Kim HK, Choi YS, Kim K, Shim YM, Kim J. A modified Nuss procedure for late adolescent and adult pectus excavatum. World J Surg. 2010;34(7):1475–1480. | ||
Pilegaard HK, Licht PB. Routine use of minimally invasive surgery for pectus excavatum in adults. Ann Thorac Surg. 2008;86(3):952–956. | ||
Schalamon J, Pokall S, Windhaber J, Hoellwarth ME. Minimally invasive correction of pectus excavatum in adult patients. J Thorac Cardiovasc Surg. 2006;132(3):524–529. | ||
Park HJ, Jeong JY, Jo WM, et al. Minimally invasive repair of pectus excavatum: a novel morphology-tailored, patient-specific approach. J Thorac Cardiovasc Surg. 2010;139(2):379–386. | ||
Mansour KA, Thourani VH, Odessey EA, Durham MM, Miller JI Jr, Miller DL. Thirty-year experience with repair of pectus deformities in adults. Ann Thorac Surg. 2003;76(2):391–395; discussion 395. | ||
McMahon LE, Johnson KN, Jaroszewski DE, et al. Experience with FiberWire for pectus bar attachment. J Pediatr Surg. 2014;49(8):1259–1263. | ||
Pilegaard HK. Nuss technique in pectus excavatum: a mono-institutional experience. J Thorac Dis. 2015;7 (Suppl 2):S172–S176. | ||
Molik KA, Engum SA, Rescorla FJ, West KW, Scherer LR, Grosfeld JL. Pectus excavatum repair: experience with standard and minimal invasive techniques. J Pediatr Surg. 2001;36(2):324–328. | ||
Park HJ, Lee SY, Lee CS, Youm W, Lee KR. The Nuss procedure for pectus excavatum: evolution of techniques and early results on 322 patients. Ann Thorac Surg. 2004;77(1):289–295. | ||
Jaroszewski DE, Johnson K, McMahon L, Notrica D. Sternal elevation before passing bars: a technique for improving visualization and facilitating minimally invasive pectus excavatum repair in adult patients. J Thorac Cardiovasc Surg. 2014;147(3):1093–1095. | ||
Park HJ, Chung WJ, Lee IS, Kim KT. Mechanism of bar displacement and corresponding bar fixation techniques in minimally invasive repair of pectus excavatum. J Pediatr Surg. 2008;43(1):74–78. | ||
Tedde ML, de Campos JR, Wihlm JM, Jatene FB. The Nuss procedure made safer: an effective and simple sternal elevation manoeuvre. Eur J Cardiothorac Surg. 2012;42(5):890–891. | ||
Takagi S, Oyama T, Tomokazu N, Kinoshita K, Makino T, Ohjimi H. A new sternum elevator reduces severe complications during minimally invasive repair of the pectus excavatum. Pediatr Surg Int. 2012;28(6):623–626. | ||
Haecker FM, Sesia SB. Intraoperative use of the vacuum bell for elevating the sternum during the Nuss procedure. J Laparoendosc Adv Surg Tech A. 2012;22(9):934–936. | ||
Johnson WR, Fedor D, Singhal S. A novel approach to eliminate cardiac perforation in the nuss procedure. Ann Thorac Surg. 2013;95(3):1109–1111. | ||
Kim D, Idowu O, Palmer B, Kim S. Anterior chest wall elevation using a T-fastener suture technique during a nuss procedure. Ann Thorac Surg. 2014;98(2):734–736. | ||
Park HJ, Jeong JY, Kim KT, Choi YH. Hinge reinforcement plate for adult pectus excavatum repair: a novel tool for the prevention of intercostal muscle strip. Interact Cardiovasc Thorac Surg. 2011;12(5):687–691. | ||
Del Frari B, Schwabegger AH. How to avoid pectus bar dislocation in the MIRPE or MOVARPE technique: results of 12 years’ experience. Ann Plast Surg. 2014;72(1):75–79. | ||
Nuss D, Obermeyer RJ, Kelly RE. Nuss bar procedure: past, present and future. Ann Cardiothorac Surg. 2016;5(5):422–433. | ||
Nuss D. Minimally invasive surgical repair of pectus excavatum. Semin Pediatr Surg. 2008;17(3):209–217. | ||
Nagaso T, Miyamoto J, Kokaji K, et al. Double-bar application decreases postoperative pain after the Nuss procedure. J Thorac Cardiovasc Surg. 2010;140(1):39–44, 44.e1–2. | ||
Stanfill AB, DiSomma N, Henriques SM, Wallace LJ, Vegunta RK, Pearl RH. Nuss procedure: decrease in bar movement requiring reoperation with primary placement of two bars. J Laparoendosc Adv Surg Tech A. 2012;22(4):412–415. | ||
Dzielicki J, Korlacki W, Janicka I, Dzielicka E. Difficulties and limitations in minimally invasive repair of pectus excavatum – 6 years experiences with Nuss technique. Eur J Cardiothorac Surg. 2006;30(5):801–804. | ||
Nagasao T, Hamamoto Y, Tamai M, et al. Scoring of deformed costal cartilages reduces postoperative pain after Nuss procedure for pectus excavatum. Thorac Cardiovasc Surg. 2016;64(1):62–69. | ||
Pilegaard HK. Short Nuss bar procedure. Ann Cardiothorac Surg. 2016;5(5):513–518. | ||
Ghionzoli M, Ciuti G, Ricotti L, et al. Is a shorter bar an effective solution to avoid bar dislocation in a Nuss procedure? Ann Thorac Surg. 2014;97(3):1022–1027. | ||
Croitoru DP, Kelly RE Jr, Goretsky MJ, Gustin T, Keever R, Nuss D. The minimally invasive Nuss technique for recurrent or failed pectus excavatum repair in 50 patients. J Pediatr Surg. 2005;40(1):181–186; discussion 186–187. | ||
Fallon SC, Slater BJ, Nuchtern JG, et al. Complications related to the Nuss procedure: minimizing risk with operative technique. J Pediatr Surg. 2013;48(5):1044–1048. | ||
Al-Assiri A, Kravarusic D, Wong V, Dicken B, Milbrandt K, Sigalet DL. Operative innovation to the “Nuss” procedure for pectus excavatum: operative and functional effects. J Pediatr Surg. 2009;44(5):888–892. | ||
Ravenni G, Actis Dato GM, Zingarelli E, Flocco R, Casabona R. Nuss procedure in adult pectus excavatum: a simple artifice to reduce sternal tension. Interact Cardiovasc Thorac Surg. 2013;17(1):23–25. | ||
Papic JC, Finnell SM, Howenstein AM, Breckler F, Leys CM. Postoperative opioid analgesic use after Nuss versus Ravitch pectus excavatum repair. J Pediatr Surg. 2014;49(6):919–923; discussion 923. | ||
Muhly WT, Maxwell LG, Cravero JP. Pain management following the Nuss procedure: a survey of practice and review. Acta Anaesthesiol Scand. 2014;58(9):1134–1139. | ||
Kelly RE, Jr., Shamberger RC, Mellins RB, et al. Prospective multicenter study of surgical correction of pectus excavatum: design, perioperative complications, pain, and baseline pulmonary function facilitated by internet-based data collection. J Am Coll Surg. 2007;205(2):205–216. | ||
Jaroszewski DE, Temkit M, Ewais MM, et al. Randomized trial of epidural vs. subcutaneous catheters for managing pain after modified Nuss in adults. J Thorac Dis. 2016;8(8):2102–2110. | ||
Gebhardt R, Mehran RJ, Soliz J, Cata JP, Smallwood AK, Feeley TW. Epidural versus ON-Q local anesthetic-infiltrating catheter for post-thoracotomy pain control. J Cardiothorac Vasc Anesth. 2013;27(3):423–426. | ||
Ried M, Schilling C, Potzger T, et al. Prospective, comparative study of the On-Q(R) PainBuster(R) postoperative pain relief system and thoracic epidural analgesia after thoracic surgery. J Cardiothorac Vasc Anesth. 2014;28(4):985–990. | ||
Weber T, Matzl J, Rokitansky A, Klimscha W, Neumann K, Deusch E. Superior postoperative pain relief with thoracic epidural analgesia versus intravenous patient-controlled analgesia after minimally invasive pectus excavatum repair. J Thorac Cardiovasc Surg. 2007;134(4):865–870. | ||
Futagawa K, Suwa I, Okuda T, et al. Anesthetic management for the minimally invasive Nuss procedure in 21 patients with pectus excavatum. J Anesth. 2006;20(1):48–50. | ||
Hall Burton DM, Boretsky KR. A comparison of paravertebral nerve block catheters and thoracic epidural catheters for postoperative analgesia following the Nuss procedure for pectus excavatum repair. Paediatr Anaesth. 2014;24(5):516–520. | ||
Jaroszewski DE, Gustin PJ, Haecker F-M, et al. Pectus excavatum repair after sternotomy: the Chest Wall International Group experience with substernal Nuss bars. European Journal of Cardio-Thoracic Surgery. 2017;52(4):710–717. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.