")
Back to Journals » Research and Reports in Urology » Volume 13
Outcome of Delayed Perineal Anastomotic Urethroplasty in Children with Post-Traumatic Urethral Stricture in a Tertiary Center, Addis Ababa, Ethiopia
Authors Setato T , Mammo TN, Wondemagegnehu B
Received 5 June 2021
Accepted for publication 3 August 2021
Published 29 August 2021 Volume 2021:13 Pages 631—637
DOI https://doi.org/10.2147/RRU.S322980
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Jan Colli
Temesgen Setato, Tihitena Negussie Mammo, Belachew Wondemagegnehu
Department of Surgery, Pediatric Surgery Division, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Temesgen Setato Tel +251-913-393-457
Email [email protected]
Background: Urethral stricture is a challenging urologic problem resulting from congenital, idiopathic, traumatic, iatrogenic,and inflammatory causes. Road traffic accidents and falling-down accidents are the most common traumatic causes. Although most management principles are extrapolated from adults, stricture in children has a unique anatomic challenge. The outcome of urethroplasty is reported to be good in nearly all patients according to different studies. Since there is no study from Ethiopia on this subject, our work will show our experience with the problem.
Patients and Methods: We conducted a retrospective study of children who underwent delayed urethroplasty for post-traumatic urethral stricture from November 2011 to November 2019. A retrospective study was conducted on boys for whom delayed perineal anastomotic urethroplasty was performed after they sustained trauma. Sociodemographic data, pre-operative presentation of patients, and intraoperative conditions were assessed. The need of any further procedure to micturate, stream of urine and urethral caliber on post-operative cystourethrography were parameters used to measure the outcome. Data were entered into SPSS version 24 and analyzed, taking a p-value of 0.05 as statistically significant.
Results: Nineteen boys had delayed perineal anastomotic urethroplasty in the study period, with a mean age at the time of surgery being 9.8 years. Out of these 19 patients, nine had been involved in road traffic accidents, eight had fallen from a height, and two had bullet injuries. The membranous urethra was the most commonly affected part and, in seven of them, associated pelvic bone fracture was documented. The affected urethral segment length ranged from 1– 3 cm, with a mean of 1.77 cm. For all of them delayed perineal urethroplasty was performed after a minimum of 3 months. Successful outcome after primary surgery and re-do surgery was 58% and 82%, respectively.
Conclusion: Urethral stricture is an uncommon condition in children but is one of the challenging conditions a pediatric urologist faces. Our study showed that perineal urethroplasty can be done safely in most children with urethral stricture, but unless adequate pre-operative evaluation and strict surgical principles are followed the outcome will be poor.
Keywords: urethroplasty, urethral stricture, trauma
Introduction
Urethral stricture in children an uncommon but challenging urologic problem. There are various reasons why children develop urethral stricture; these include congenital, idiopathic, traumatic, iatrogenic and inflammatory issues. Road traffic accidents remain the most common traumatic cause, followed by straddle injury from falling accidents.1,2 Among children who sustained a pelvic fracture, the incidence of associated urethral injury is reported to be as high as 30%, and boys are more commonly affected than girls.3 According to the Société Internationale d’Urologie and the International Consultation on Urological Diseases guidelines drafted in 2014, the term “urethral stricture” is used to describe narrowing of the anterior urethra surrounded by spongiosum. Posterior urethral narrowing is described as “stenosis” (if not associated with pelvic fracture) or “Pelvic fracture urethral distraction injury” (if associated with pelvic fracture).4
Although most management principles are the same and are actually extrapolated from adults, there are still certain differences between urethral strictures in adult and pediatric populations. In children ≤15 years, pelvic fracture tends to cause urethral injury more commonly than in adults.5 According to Devine and Devine,6 unlike in adults, children have a thin rudimentary prostate gland that provides poor support to the posterior urethra, and injury resulting from trauma tends to cause more proximal injury to the level of the bladder neck or prostatic urethra. This will in turn hamper access from the perineal approach. Apart from this, in children the bladder is intra-abdominal, and the pubo-prostatic ligaments are immature, which easily transmit shearing force to the prostate and result in injury.7 Though delayed anastomotic urethroplasty is considered a gold standard approach by most surgeons, there are still some authors who prefer primary re-alignment. The perineal approach is preferred whenever possible, while the perineal trans-pubic approach and abdominoperineal approaches are reserved for long or more proximal injuries where a tension-free anastomosis is not possible. According to Basiri et al,10 symphysiotomy is the preferred approach of repair of pediatric urethral stricture, because of anatomic difficulty.8–10
Despite the challenges of urethroplasty in children, successful urethroplasty can be achieved in nearly all children with post-traumatic urethral stricture.11 We did not come across any study done in low income countries, including Ethiopia. So, this will be a benchmark paper aimed to show our experience with this problem. It is also our aim to show further challenges which may affect the outcome, in addition to those which are mentioned in other studies.
Patients and Method
A retrospective study was conducted on patients who underwent delayed anastomotic urethroplasty for post-traumatic urethral stricture in the study period, November 2011 to November 2019. Charts of 22 patients were reviewed. Of them three patients either defaulted from follow-up, had incomplete charts, or we could not trace them through their registered phone number. Therefore, we analyzed the data of the remaining 19 patients.
A data collection tool was designed by the investigators and pretested. Data cleaning and analysis were done using SPSS version 24. Chi-squared tests and Fisher's exact test for categorical and independent t-test analysis for continuous variables were used to report outcomes, and the two-sided significance level was set to be 0.05 (5%).
Sociodemographic data (age), pre-operative evaluation findings (etiology, diagnostic modality, part of affected urethra, associated pelvic fracture), intraoperative assessment (length of affected urethra, duration of surgery, intraoperative complication), and the outcome of the procedure were studied. Post-op outcome was followed for a minimum of 1 year. The outcome of urethroplasty was assessed using three parameters, which were; need of any further procedure to micturate, stream of urine (observation by a physician), and urethral caliber on post-operative cystourethrography (CUG).
The operational definitions used were:
- Delayed urethroplasty: Urethroplasty done after at least 3 months from the date of trauma.
- Successful outcome: If the patient does not need a further procedure to micturate and passes full stream urine as it was in the pre-trauma state and/or normal urethral caliber on post-operative cystourethrography (CUG).
- Poor Outcome: If the patient is unable to pass urine or has a poor urinary stream, if an additional procedure is needed to achieve normal micturition, or if CUG shows remnant stricture.12
In all patients the procedure was done on lithotomy position, with a Mercedes Benz incision made on the perineum. Proximal urethra was identified by a bougie dilator inserted into the bladder and posterior urethra through suprapubic cystostomy site and pushing the proximal end downwards. All scar tissue excised and end-to-end mucosa to mucosa anastomosis was done over foley catheter using interrupted vicryl stitches and a glove drain was left around the anastomosis. The length of the affected urethral segment was measured intraoperatively using a tape meter. The procedures were done by four surgeons who apply similar techniques.
Ethical Consideration
The study was conducted after getting approval from the Institutional Review Board (IRB) of Addis Ababa University, College of Health Sciences and Medicine. Parents/legal guardians were contacted through phone and were asked for verbal consent. Written consent was taken by the time they came for a clinic visit, this was also the time when evaluation for the outcome was made.
We confirm that every procedure of this study was under the guidelines of the Declaration of Helsinki.
Results
All 19 patients who had delayed urethroplasty were male and their age ranged from 6 years to 12 years, with a mean age of 9.8 years. Retrograde urethrography has not been done in an emergency setting, rather in all patients with blood on urethral meatus or other findings, suggestive of urethral injury catheterization, was deferred and suprapubic cystostomy was done. A definitive diagnosis of urethral stricture was made with cystourethrography in all patients. Road traffic accidents and straddle injury were the two most common causes of urethral stricture (9/19, and 8/19, respectively) and in two of the patients, the cause of stricture was a direct gunshot wound. Seven patients (37%) had pelvic bone fracture documented (Table 1).
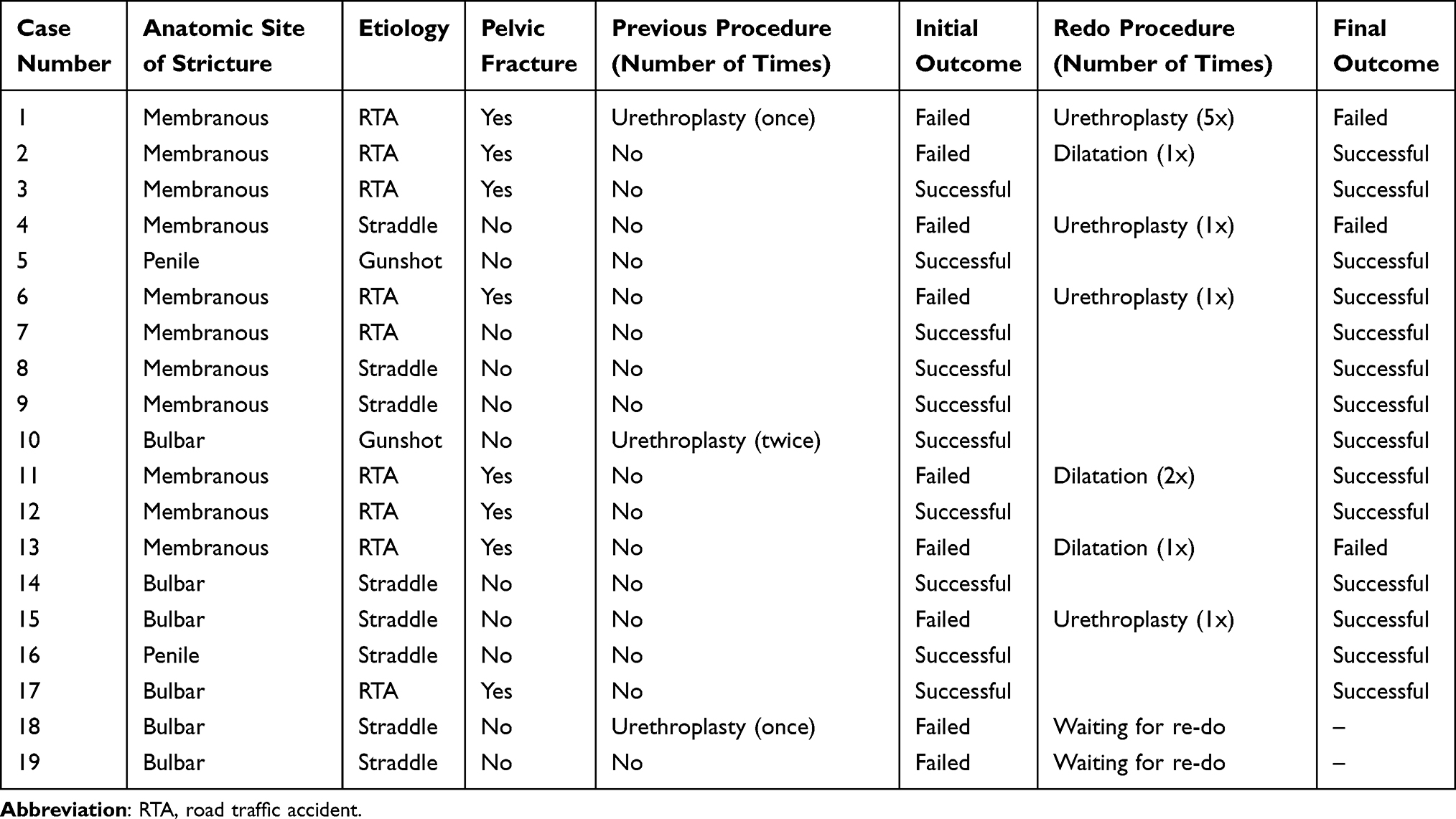 |
Table 1 Etiology, Anatomic Site of Affected Urethra, Treatment History, and Outcome |
Three patients had a previous urethroplasty and came for recurrent stricture, of which two underwent the surgery in the same institution before the study period and one came from another center. Two of them were operated on twice and one was operated on once, all were trans-perineal anastomotic urethroplasty (Table 1).
Delayed perineal anastomotic urethroplasty was done in all patients after a minimum of 3 months from trauma. All patients had suprapubic cystostomy done after urethral injury was diagnosed clinically at the time of trauma.
The length of the affected urethral segment was mentioned intraoperatively in 11 of the patients and it ranged from 1 cm to 3 cm with a mean of 1.77 cm. The mean duration of surgery was 112 minutes, and there were no intra-operative surgical or anesthetic complications reported. Glove drainage was left in 17 (89%) patients and a drain was not needed for two patients with penile urethral stricture.
All patients were put on intravenous antibiotics up to the day of discharge and were put on oral antibiotics on discharge, except one patient with penile urethral stricture who was given only intravenous antibiotics for 7 days. The total duration of antibiotics ranged between 7 days, for those with penile urethral stricture, to 28 days, with a mean of 16 days. A trans-urethral catheter was kept in place from 7 to 24 days, with a median of 21 days. Except for penile repairs, for whom catheters were removed early, the rest get it removed on the 21st day post-op day unless they delay two to three days to show up.
Out of the nine (47%) patients who developed recurrent stricture after initial urethroplasty, bouginage was done for three, urethroplasty was done for four and the other two are still on suprapubic cystostomy waiting for a redo procedure. Four patients became symptom-free after the salvage procedure and four remained unsuccessful, with this our final success rate became 82% (14/17).
The part of the urethra involved, length of strictured segment, etiology, presence of associated pelvic fracture, and previous surgery were assessed to see if they affect the success of urethroplasty and none of these factors showed a statistically significant association with the outcome on chi-square and independent t-test analysis (P=0.515, 0.860, 0.755, 0.576, 0.331).
Discussion
Delayed perineal anastomotic urethroplasty was done on 19 boys who had post-traumatic urethral stricture with a mean stricture length of 1.77 cm. The initial surgery was successful in 58% and the final outcome after repeat surgery was 82%.
Unlike in adults, urethral stricture in children is less common and less studied. With this scarcity of cases on top of demanding anatomy and more complicated stricture type children usually have, it is difficult to handle these cases.6,13
In our study, the mean age at the time of surgery was 9.7 years, which goes in line with similar studies.11,14 A road traffic accident is by far the most common reported cause of urethral disruption in similar studies whereas, in our study a nearly equal number of patients sustained straddle injury, which may be because more rural area children sustain a fall from a height, like from trees.14,15
The gold standard treatment for post-traumatic urethral stricture is delayed anastomotic urethroplasty which is done after 3 months at which time local healing is thought to be complete and hematoma contracts well. If there are conditions necessitating emergency repair, such as associated rectal, vaginal or bladder neck injury, a primary repair can be done.16 Regarding the approach, whenever possible perineal approach should be used first, whereas the trans-pubic (trans-perineal or abdominoperineal) approach is reserved for longer and more complex strictures. According to Podesta,17 the abdominoperineal approach has even superior results on top of better exposure and easier repair. However, others suggest that a simple perineal approach is enough in most cases as the imagined difficulty of the proximal location of stricture and difficult access is compensated by the shorter overall length of the pediatric pelvis.12,18
Pelvic fracture associated urethral injury usually involves membranous urethra or an even more proximal part in children, whereas bulbar urethra is commonly associated with straddle injury as in falling accidents.19 In our series, three patients sustained straddle injury and sustained a membranous urethral injury with no pelvic fracture. The likely reason is these patients may have associated stable pelvic fracture which is overlooked on a pelvic x-ray or not documented. There is also one patient who sustained a road traffic accident and pelvic fracture with bulbar urethral injury. This may be because in our study the site of injury is documented only on the intra-operative note which may be liable for bias since the report is based on the distal-most part affected.
Antegrade and retrograde urethrography with or without urethroscopy is considered a key pre-operative evaluation technique. In an acute setting, extravasation of contrast will confirm the urethral injury and will also show the site of injury while in an established stricture cystourethrogram helps to assess length and site of urethral distraction and it also can give us information regarding bladder neck status. However, both overestimation and underestimation of the length of distraction are possible. Underestimation occurs when an incompletely absorbed hematoma cavity is filled with extravasated contrast just like the urethra does, whereas, overestimation occurs when the proximal urethra is incompletely filled with contrast making the gap wider.18,20 All of our cases had antegrade and retrograde urethrography done before definitive surgery, however, the length and site were not clearly described. Urethroscopy is favored by some surgeons as it complements the information one gets from cystourethrography. Ultrasound and MRI are also indicated if further information is needed but ultrasound cannot be utilized in the case of posterior urethral injury.11,13,21
The mean length of the strictured segment in our study is 1.77 cm, which is comparable with reports of Koushik et al, Rouke et al, and Orabi et al, but lower than reports of Hafez et al, Podesta et al, and Singla et al.8,11,13,22–24 In our study, the length of the affected segment was reported on an intra-operative note which is said to be more reliable than pre-operative radiologic estimation. Given the maximum estimated length in our study, 3 cm, it is justifiable to use the perineal approach only. The actual length that determines tension on anastomosis is the one measured after excision of all scar tissue and refreshing the ends of both the proximal and distal urethra, however, as the gap described by different authors is not this final one, there may be over- or underestimation.16,24
After perineal urethroplasty, we kept the catheters for 3 weeks, while across the literature there are variable practices. In studies from India and China the catheter is kept for 3–4 weeks but others kept it for just 2 weeks unless the trans-abdominal approach was used. No study has compared the advantage of one over the other, but cystourethrography should be done either before removal or just after removal to see any narrowing or extravasation.12,19,24–26
When compared with similar studies on the overall outcome of perineal anastomotic urethroplasty, our outcome is significantly low (P=0.004) (Table 2). However, Koushik et al24 from India, a comparable setup, reported a similar success rate on both primary and redo surgery.5,8,11,14,23,24 Given the relative rarity of cases in our setting and the absence of a dedicated center to pool these cases, there is limited experience on the subject matter. Across the literature the outcome of urethroplasty is assessed in a non-uniform way and unless there is a scoring system by which all outcomes are uniformly assessed, it may be vulnerable to subjectivity.
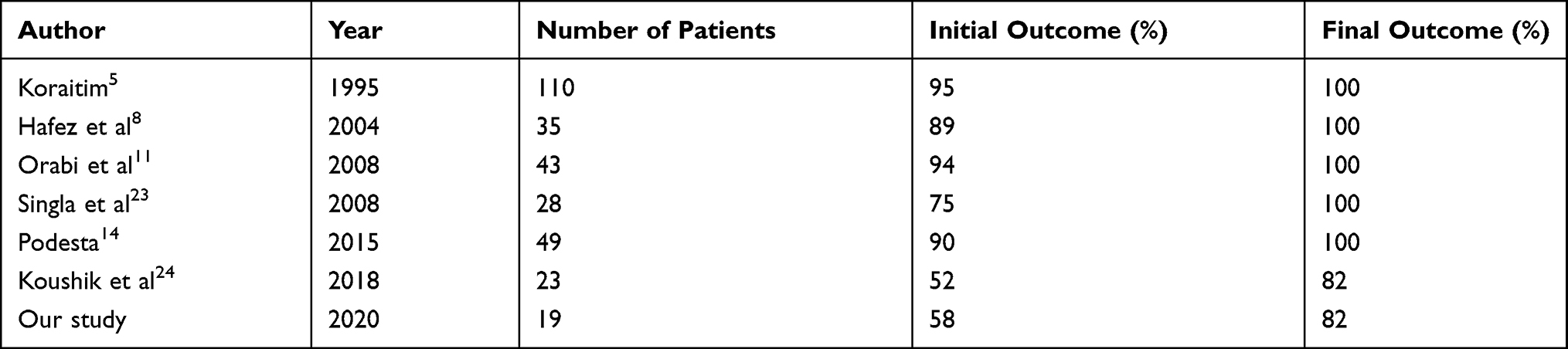 |
Table 2 Outcome of Urethroplasty in Different Studies |
The success of urethroplasty is dependent on various factors starting from the proper pre-operative evaluation which helps one to know the exact image of the patient. Every effort should be made to achieve a tension-free mucosa-to-mucosa anastomosis despite utilizing different approaches including mobilizing the anterior urethra to the extent of corporal separation and depending on the posterior extent of stricture using trans-pubic or abdominoperineal approaches. In addition, complete excision of scar tissue is suggested by most authors but others claim to have a comparable result and relatively lower risk of incontinence, with limited scar excision. The anastomosis should be widened by spatulating proximal and distal ends, though some question its importance.11,12,16,25
Visual Internal Urethrotomy (VIU) is also considered good alternative management in selected cases. Tamer E. Helmy27 reported a high success rate (77% primary urethrotomy and 90% in the second urethrotomy) of VIU when used in short strictures and as a complement for anastomosis site stricture after open urethroplasty. It seems an attractive option as it reduces injuries associated with open approaches, however, patient selection is very important; as its use is shown in short stricture, less than 1 cm, and when passing a guidewire is possible.
Another very important factor that may affect variations in outcome may be a non-uniform way of assessing postoperative outcome. Unless there is a scoring system by which all outcomes are uniformly assessed, it may be prone to subjectivity.12,28
Conclusion
Perineal anastomotic urethroplasty is the first-line treatment for post-traumatic pediatric urethral stricture. The outcome of urethroplasty in our setup is lower as compared to others, which needs to be improved by focusing on proper pre-operative evaluation and sticking to surgical principles to achieve tension-free mucosa to mucosa anastomosis.
Limitation of the Study
This study has all problems inherent to retrospective studies such as incomplete charts and non-uniform follow-ups. We did not study incontinence, erectile dysfunction, or chordae, which may occur post-surgery. The non-objective measurement of outcome due to the lack of a urodynamic study also remains a limitation of our study.
Abbreviations
CUG, Cysto-urethrography; RTA, Road traffic accident; VIU, Visual internal urethrotomy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Frank JD, Pocock RD, Stower MJ. Urethral strictures in childhood. Br J Urol. 1988;62(6):590–592. doi:10.1111/j.1464-410X.1988.tb04432.x
2. Vetterlein MW, Weisbach L, Riechardt S, Fisch M. Anterior urethral stricture in children: disease etiology and comparative effectiveness of endoscopic treatment vs. open surgical reconstruction. Front Pediatr. 2019;7:5. doi:10.3389/fped.2019.00005
3. Tarman GJ, Steven GWK, Lerman SL, McAleer IM, Losasso BE. Lower genitourinary injury and pelvic fractures in pediatric patients. Pediatr Urol. 2002;59(1):123–126. doi:10.1016/S0090-4295(01)01526-6
4. Latini JM, McAninch JW, Brandes SB, Chung JY, Rosenstein D. SIU/ICUD consultation on urethral strictures: epidemiology, etiology, anatomy, and nomenclature of urethral stenoses, strictures, and pelvic fracture urethral disruption injuries. Urology. 2014;83(3):S1–S7. doi:10.1016/j.urology.2013.09.009
5. Koraitim MM. The lessons of 145 posttraumatic posterior urethral strictures treated in 17 years. J Urol. 1995;153(1):63–66. doi:10.1097/00005392-199501000-00024
6. Devine PC, Devine CJ. Posterior urethral injuries associated with pelvic fractures. Urology. 1982;20(5):467–470. doi:10.1016/0090-4295(82)90114-5
7. Morra MN, Das S. Traumatic stricture of prostatic urethra in ten-year-old boy. Pediatr Urol. 1991;38(6):552–553. doi:10.1016/0090-4295(91)80177-9
8. Hafez AT, Osama Sarhan -AE-A, El-Hefnawy AS, Ghoneim MA. Perineal anastomotic urethroplasty for managing post-traumatic urethral strictures in children: the long-term outcome. Br J Urol. 2004;95(3):403–406. doi:10.1111/j.1464-410X.2005.05309.x
9. Koraitim MM. Post-traumatic posterior urethral strictures: preoperative decision making. Adult Urol. 2004;64(2):228–231. doi:10.1016/j.urology.2004.03.019
10. Basiri A, Shadpour P, Moradi MR, Ahmadinia H, Madaen K. Symphysiotomy: a viable approach for delayed management of posterior urethral injuries in children. J Urol. 2002;168(5):2166–2169. doi:10.1016/S0022-5347(05)64345-5
11. Orabi HB, Saad A, Youssef M, Hanno A, Hanno A. Post-traumatic posterior urethral stricture in children: how to achieve a successful repair. J Pediatr Urol. 2008;4(4):290–294. doi:10.1016/j.jpurol.2008.01.209
12. Zhou FJ, Xiong YH, Zhang XP, Shen PF. Transperineal end-to-end anastomotic urethroplasty for traumatic posterior urethral disruption and strictures in children. Asian J Surg. 2001;25(2):134–138. doi:10.1016/S1015-9584(09)60161-5
13. Hagedorn JC, Voelzke BB. Pelvic-fracture urethral injury in children. Arab J Urol. 2019;13(1):37–42. doi:10.1016/j.aju.2014.11.007
14. Podesta M. Delayed surgical repair of posttraumatic posterior urethral distraction defects in children and adolescents: long-term results. J Pediatr Urol. 2015;11:67–e1.
15. Shenfeld OZ, Ran Katz JG, Gofrit ON, Pode D, Landau EH. Urethroplasty, by perineal approach, for bulbar and membranous urethral strictures in children and adolescents. Pediatr Urol. 2007;71(3):430–433. doi:10.1016/j.urology.2007.09.072
16. Podesta M, Miguel P
17. Podesta ML. Use of the perineal and perineal-abdominal (transpubic) approach for delayed management of pelvic fracture urethral obliterative strictures in children: long-term outcome. J Urol. 1998;160(1):160–164. doi:10.1016/S0022-5347(01)63078-7
18. Priyadarshi Ranjan MSA, Manmeet Singh SS, Chipde RS, Kapoor R. Post-traumatic urethral strictures in children: what have we learned over the years? J Pediatr Urol. 2012;8(3):234–239. doi:10.1016/j.jpurol.2011.06.004
19. Bryan B, Voelzkea B, Benjamin N, Breyera B, Jack W. Blunt pediatric anterior and posterior urethral trauma: 32-year experience and outcomes. J Pediatr Urol. 2011;8:258–263.
20. Pichler R, Fritsch H, Skradski V. Diagnosis and management of pediatric urethral injuries. Urol Int. 2012;89(2):136–142. doi:10.1159/000336291
21. Pavlica P, Barozzi L, Menchi I. Imaging of male urethra. Eur Radiol. 2002;13:1583–1596.
22. Rourke KF, Joel KAM, Sumfest M, Gerald H. Jordan, open reconstruction of pediatric and adolescent urethral strictures: long-term followup. J Urol. 2003;169(5):1818–1821. doi:10.1097/01.ju.0000056035.37591.9f
23. Singla MSJ, Muruganandam K, Aneesh Srivastava MS, Ansari AM, Dubey D, Kapoor A. Posttraumatic posterior urethral strictures in children—management and intermediate-term follow-up in tertiary care center. Pediatr Urol. 2008;72(3):540–543. doi:10.1016/j.urology.2008.02.078
24. Koushik H, Jehangir S, Thomas RJ. Stricture urethra in children: an Indian perspective. J Indian Assoc Pediatr Surg. 2018;23(4):192–197. doi:10.4103/jiaps.JIAPS_146_17
25. Koraitim MM. Posttraumatic posterior urethral strictures in children: a 20-year experience. J Urol. 1997;157(2):641–645. doi:10.1016/S0022-5347(01)65239-X
26. Garg G, Singh MK,M, Sankhwar SN, Sankhwar SN. Spectrum of management options for pediatric pelvic fracture urethral injury and outcome analysis: 12-year tertiary center experience. J Pediatr Urol. 2018;15(4):
27. Tamer E, Helmy ATH. Internal urethrotomy for recurrence after perineal anastomotic urethroplasty for posttraumatic pediatric posterior urethral stricture: could it be sufficient? J Endourol. 2013;27(6):693–696. doi:10.1089/end.2012.0592
28. Abdurrahman Onen HÖ, Kaya M, Otcu S, Otçu S. Long-term outcome of posterior urethral rupture in boys: a comparison of different surgical modalities. Pediatr Urol. 2005;65(6):1202–1207. doi:10.1016/j.urology.2005.01.039
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.