")
Back to Journals » Infection and Drug Resistance » Volume 14
Outbreak of Multidrug-Resistant OXA-232-Producing ST15 Klebsiella pneumoniae in a Teaching Hospital in Wenzhou, China
Authors Jia H, Zhang Y, Ye J , Xu W, Xu Y, Zeng W, Liao W, Chen T, Cao J, Wu Q, Zhou T
Received 16 July 2021
Accepted for publication 13 October 2021
Published 24 October 2021 Volume 2021:14 Pages 4395—4407
DOI https://doi.org/10.2147/IDR.S329563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Huaiyu Jia,1 Ying Zhang,2 Jianzhong Ye,1 Wenya Xu,1 Ye Xu,1 Weiliang Zeng,2 Wenli Liao,1 Tao Chen,1 Jianming Cao,2 Qing Wu,1 Tieli Zhou1
1Department of Clinical Laboratory, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang Province, People’s Republic of China; 2Department of Medical Laboratory Science, School of Laboratory Medicine and Life Science, Wenzhou Medical University, Wenzhou, Zhejiang Province, People’s Republic of China
Correspondence: Tieli Zhou; Qing Wu
Department of Clinical Laboratory, the First Affiliated Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
Tel/Fax +86-0577-8668-9885
Email [email protected]; [email protected]
Background: OXA-232-producing carbapenem-resistant Klebsiella pneumoniae (CRKP) has the potential to become the “third epidemic” of carbapenem-resistant Klebsiella strain after KPC-2 and NDM in China. We investigated the first outbreak of CRKP in the First Affiliated Hospital of Wenzhou Medical University.
Methods: We collected 610 clinical isolates of CRKP from the First Affiliated Hospital of Wenzhou Medical University between January 2019 and September 2020 and screened them by Polymerase Chain Reaction (PCR). The multilocus sequence typing and pulsed-field gel electrophoresis were used to determine the genetic relatedness of the strains. The antimicrobial susceptibility test was performed to determine the drug resistance of the clinical isolates. The molecular mechanism underlying carbapenem resistance was elucidated by performing PCR and conjugation experiments. The virulence potential of the strains was determined by the string test, detection of virulence-associated genes and capsular serotypes, and Galleria mellonella larval infection model.
Results: Between September 2019 and May 2020, 26 OXA-232-producing CRKP were obtained from 12 patients in our hospital. Ten patients were hospitalized in the intensive care units (ICU) and the overall mortality of the inpatients involved in the outbreak was 50% (6/12). Epidemiological investigations reported that all the OXA-232-producing CRKP strains belonged to the sequence type ST15 and can be clonally transmitted among the inpatients in the ICU. All the strains had low virulence and were resistant to commonly used clinical antibiotics except for ceftazidime/avibactam, colistin, and tigecycline. The OXA-232-producing CRKP was sensitive to triclosan and chlorhexidine, and its eradication from our hospital can be achieved by the use of disinfectants in the ICU.
Conclusion: In our study, OXA-232-producing CRKP isolates appeared to be clonally transmitted and the sequence type ST15 was responsible for the outbreak. Therefore, effective measurements for the infection control of CRKP are urgently needed to prevent its epidemic in the nearby region in the future.
Keywords: Klebsiella pneumoniae, carbapenem-resistance, virulence, OXA-232, outbreak
Introduction
Data from the global surveillance programs report that OXA-48-like carbapenemases are the most common carbapenemases among the Enterobacterales strains in various countries (eg, the Middle East, North Africa, and European countries such as Belgium and Spain).1–3 More than a dozen different variants of OXA-48-like carbapenemase have been reported and OXA-232 is currently the 3rd most common OXA-48-like derivative globally.1 OXA-232 was produced in the Escherichia coli and K. pneumoniae strains isolated from three French patients traveling to India in 2013.4 Since then, along with the co-production of New Delhi metallo-beta-lactamase-1, the OXA-232-producing Enterobacteriaceae especially K. pneumoniae had spread to many hospitals around the world due to international travels, leading to a huge challenge in the clinical diagnosis and treatment.5–8
Since the initial isolation of OXA-232-producing CRKP in five neonatal patients in China in 2017, several nosocomial outbreaks of the OXA-232-producing CRKP at a small scale have been reported in children and elderly patients.5,7 The main sequence type (ST) in the OXA-232-producing CRKP from China is ST15; but recent studies have reported that the OXA-232 is also present in ST437 K. pneumoniae clinical isolates, a newly discovered clone of high-risk multidrug-resistant (MDR) CC11.5–7,9 Currently, a few studies have reported the virulence of OXA-232-producing CRKP. Although researchers from China have reported the OXA-232-producing CRKP with a plVPK-like virulent plasmid, its virulence level was not high.5 Mukherjee, S. et al reported a case of neonatal septicemia caused by the ST23 hypervirulent K. pneumoniae (hvKP) producing OXA-232 carrying pLVPK-like plasmids in India, suggesting that the ST23 hvKP strains may have obtained the resistance gene blaOXA-232 during evolution.10,11 Since K. pneumoniae has a remarkable ability to take up exogenous resistance-encoding and hypervirulence-encoding genetic elements, we need to inhibit the evolution of OXA-232-producing K. pneumoniae ST15 towards hypervirulence and high resistance.10
In the present retrospective study, we investigated the first outbreak of ST15 OXA-232-producing CRKP in a teaching hospital, which occurred from September 2019 to May 2020. The study was designed to explore the characteristics of clinical, microbiological, and molecular epidemiology of OXA-232-producing CRKP, and to provide the theoretical basis for controlling the transmission.
Materials and Methods
Bacterial Isolates
The study site was the First Affiliated Hospital of Wenzhou Medical University in Wenzhou, China. It is one of the largest healthcare centers in southern Zhejiang province that bears the responsibility for the medical care and treatment of critical and difficult diseases for an estimated 30 million population, with approximately 3300 hospital beds. From January 2019 to September 2020, a group of 610 CRKP isolates was collected from outpatients or inpatients in the First Affiliated Hospital of Wenzhou Medical University. All isolates were tested for the presence of the blaOXA-232 by polymerase chain reaction (PCR) amplification with primers suggested elsewhere.12 Then, the positive products were sequenced by the BGI Technology Co., Ltd. The sequencing results exhibited a total of 25 CRKP strains carried the blaOXA-232 (Table S1). Isolates that were found to be positive for blaOXA-232 were further analyzed. Moreover, an OXA-232-producing CRKP (FK-LW) recovered from the first people’s Hospital of Longwan district in Wenzhou was included in this research for epidemiological investigation. The identification of all isolates was performed by employing the Matrix-Assisted Laser Desorption/Ionization Time-Of-Flight Mass Spectrometry (MALDI-TOF/MS, Bruker Daltonics, US) as per the manufacturer’s instructions. The subjects of all subsequent experiments included these 26 OXA-232-producing CRKP clinical isolates.
Clinical Data Collection
Clinical data were acquired from the Electronic Medical Records of the inpatient including patient demographics data, brief hospital course, clinical diagnosis, type of infection, isolation site, ICU admission, antimicrobial treatment, invasive treatments, and the outcome of hospitalization. The study and consent procedure were approved by the Ethical Committee of the First Affiliated Hospital of the Wenzhou Medical University.
Molecular Epidemiology Analysis
The genetic relatedness of 26 OXA-232-producing CRKP strains was evaluated by molecular typing by using pulsed-field gel electrophoresis (PFGE). Plugs containing Xba I-digested genomic DNA were prepared and the DNA fragments were dispersed for 17.5 h at 6 V/cm at 14°C on the Bio-Rad® CHEF-Mapper XA machine (Bio-Rad, California, USA). The initial and final pulse times were 6 s and 36 s, respectively. Salmonella enterica serotype Braenderup H9812 served as the marker. The reports-phylogenetic tree (UPGAMA) was established to determine the genetic level homology between the strains. The chromosomal DNA restriction patterns were explicated by employing a previously built criteria,12 with a phylogenetic dendrogram analysis demonstrating 85% strain relatedness. Multilocus sequence typing (MLST) was performed in the light of the protocols on the Pasteur Institute MLST website for K. pneumoniae (https://bigsdb.pasteur.fr/klebsiella/klebsiella.html).
Antibiotic Susceptibility Test
The minimum inhibitory concentrations (MICs) of common antibacterial drugs and disinfectants (triclosan and chlorhexidine)13 were tested by agar dilution method or broth microdilution method (ceftazidime/avibactam, tigecycline, and colistin). The breakpoints were set in the light of Clinical and Laboratory Standards Institute (CLSI 2020)14 (except for colistin and tigecycline), European Committee on Antimicrobial Susceptibility Testing (EUCAST v.11.0) (http://www.eucast.org/) (for colistin), and the US Food and Drug Administration (for tigecycline) recommendation. E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were adopted as the quality control strains.
Detection of Carbapenem-Resistance Genes and Virulence Genes
All isolates positive for blaOXA-232 were analyzed through PCR examination with particular primers and amplification setups in order to identify the existence of carbapenemases (blaKPC, blaVIM, blaIMP, and blaNDM), ESBLs genes (blaCTX-M, blaSHV, blaTEM), and virulence genes (rmpA, rmpA2, iucA, wcaG, uge, magA, aerobactin, iucA, ybtA, iroN, kfuBC, iroB, mrkD, and ureA) as previously described.12 Subsequently, the positive PCR products were sequenced.
Plasmid Analyses
The transferability of blaOXA-232-encoding plasmids was assayed by conjugation. The donor for the conjugal transfer of blaOXA-232 gene was found to be OXA-232-producing CRKP, and the recipient was rifampicin-resistant E. coli EC600 or sodium azide-resistant E. coli J53. Donor or recipient strain was routinely grown at 37°C with shaking (180 rpm) in Luria–Bertani broth (10 g/L tryptone, 5 g/L yeast extract, 5 g/L NaCl) until they reached their exponential growth phase (OD600 = 0.4–0.6). Then, overnight cultures of donor and the recipient strains were mixed in a 1:1 ratio and incubated at 37°C for 16–20 h. After incubation, 100-μL of the sample was spread onto MH agar plates containing ertapenem (4 μg/mL) or ceftazidime (16 μg/mL) and rifampicin (600 μg/mL) or sodium azide (100 μg/mL). The blaOXA-232-positive transconjugants were confirmed by PCR.
Hyperviscous Phenotype Detection (String Test)
The experimental strain was inoculated on the plate and incubated in an incubator at 35°C for 18–24 h. The inoculation ring gently touched the surface of a single colony and then pulled upward. If the mucus filament was formed and the length of the mucus filament was >5 mm, it was judged to be positive for the string test, that is, to indicate a hyperviscous phenotype.15
Determination of Capsular Serotype of K. pneumoniae
First, the gene wzi (wzi-For, 5ʹ-GTGCCGCGAGCGCTTTCTATCTTGGTATTCC-3ʹ; and wzi-Rev, 5ʹ-GAGAGCCACTGGTTCCAGAACTTGACCGC-3ʹ) of all tested strains were amplified by PCR and then sequenced. Then, the PCR sequencing results were submitted to the Pasteur Institute website for K. pneumoniae (https://bigsdb.pasteur.fr/klebsiella/klebsiella.html) for comparison purposes, and the capsular serotype of K. pneumoniae was determined.
Galleria Mellonella in vivo Infection Model
Five experimental strains (ie, FK-LW, FK-7859, FK-7779, FK-8190, and FK-7853) were selected according to the PFGE results. A total of 26 strains of OXA-232-producing CRKP were categorized into four clusters (ie, A, B, C, and D). One strain of K. pneumoniae was randomly selected from cluster A, cluster B, and cluster C, and two strains of K. pneumoniae were randomly selected from cluster D. The virulence of OXA-232-producing CRKP was evaluated by the Galleria mellonella in vivo infection mode. Briefly, K. pneumoniae suspension at a concentration of 104 to 107 CFU/mL was prepared in phosphate-buffered saline (PBS). Then, 10 μL of the bacterial suspension was injected into the larvae and maintained at 37°C in the dark. The number of dead larvae was recorded 24, 48, 72, 96, and 120 h after the injection. The experiments were repeated thrice using 10 larvae in each group for each experiment.
Results
Outbreak Description
Between September 2019 and May 2020, a university hospital in the south Zhejiang province, China was affected by an outbreak of OXA-232-producing K. pneumoniae. A total of 26 OXA-232-producing K. pneumoniae isolates were obtained from the 12 inpatients. The complete hospitalization data of all the cases were available (Table 1). None of the patients had a recent medical history or a recent international travel experience. Of the 12 patients, two were female and 10 were male, with a median age of 70.5 years (range: 42–89 years). With the outbreak, all the patients reported clinical symptoms such as sepsis, pneumonia, or urinary tract infection with severe underlying diseases, which became a major concern for the infection control department in the hospital.
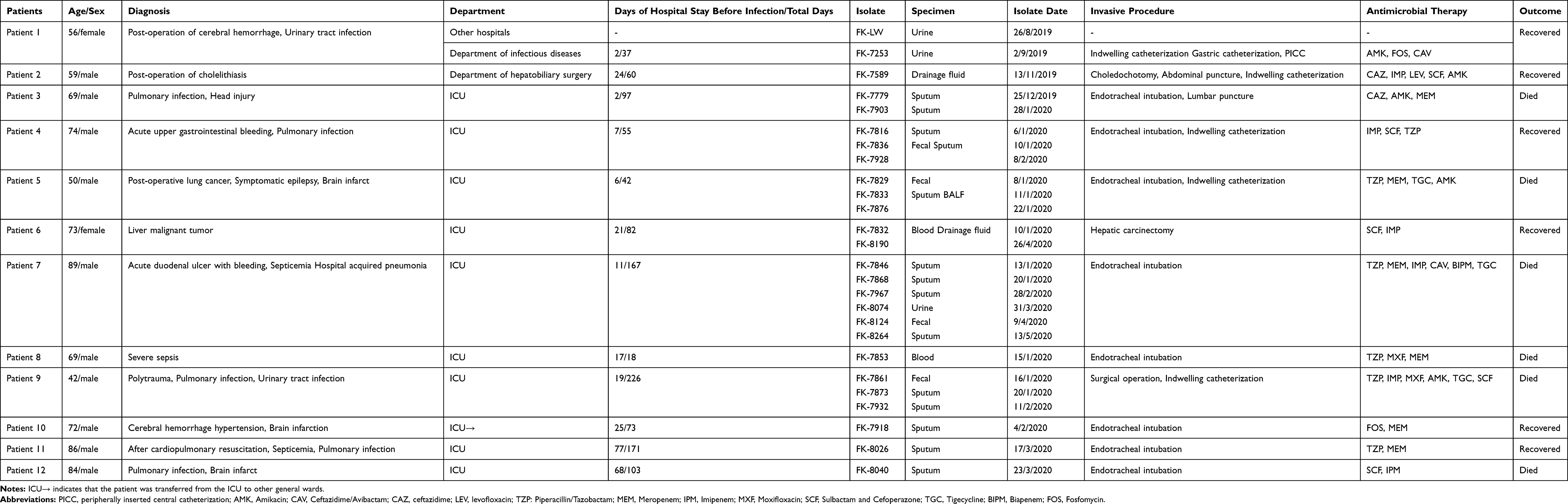 |
Table 1 Clinical Features of Patients Infected with OXA-232-Producing K. Pneumoniae Isolates |
The cases were arranged based on the date when the first OXA-232-producing CRKP was isolated. A retrospective analysis of the clinical information of the 12 patients indicated that the index patient (Patient 1) was a 56-year-old female who was in a comatose condition after a craniocerebral surgery because of intracerebral hemorrhage and had been indwelling a urinary catheter after discharge. On August 20, 2019, she went to a secondary hospital (the First People’s Hospital in Longwan district in Wenzhou, China) because of a urinary tract infection, and a strain of OXA-232-producing CRKP was isolated from the urine sample. Because it was difficult to control the infection, patient 1 was admitted to the Department of Urology in our hospital on September 1, 2019. On the second day of hospitalization, ST15 OXA-232-producing K. pneumoniae (FK-7253) was isolated from the urine sample. After a long-term antibiotic treatment (Amikacin, Fosfomycin, and Ceftazidime) and a transfer to the department of infectious disease for more advanced treatment, the patient recovered and was discharged. Patient 2, a male, was admitted to the Hepatobiliary surgical ward on March 21, 2019, with the diagnosis of acute cholangitis after cholelithiasis. On the 24th day post-hospitalization, ST15 K. pneumoniae (FK-7589) was isolated from his bile sample. He was discharged after the administration of an effective antibiotic treatment. The subsequent patients 3–12 were admitted to the ICU ward, and the first OXA-232-producing CRKP was detected between the end of December 2019 and March 2020 in these 10 patients. Some patients received invasive procedures because of their condition (for example, endotracheal intubation, indwelling urinary catheterization, gastric intubation, thoracentesis, abdominal puncture, surgery, or some other procedure). Six of the patients lost their lives because of septic shock and multiple organ failure. Figure 1 presents the infection schedule of the patients.
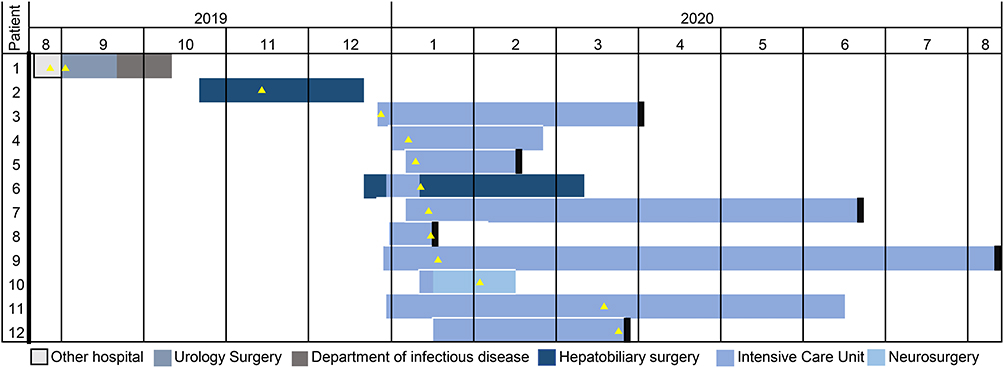 |
Figure 1 The timeline of OXA-232-producing CRKP outbreak in south-eastern China. Different wards are indicated in different colors. The black rectangle indicates that the outcome of this patient is death. The yellow triangle indicates the isolation of the OXA-232-producing CRKP strain. |
An urgent infection control plan was adopted after the identification of the MDR strain, which was reported to the doctors and immediate actions were taken. As per the doctor’s orders, the bedside warning signs and bedsheets of these patients were marked in blue. Waste generated by the infected patients was collected in a separate trash can and sealed before disposal. The hand hygiene of the medical staff and their families had been strengthened; the number of disinfectants in the nearby environment was increased; the courses for infection prevention and control had been rescheduled whenever necessary. Thus, the transmission was successfully controlled and no new cases were found after May 2020.
Genetic Relatedness of OXA-232-Producing CRKP
The clonal relatedness between CRKPs producing OXA-232 was analyzed by MLST and PFGE. Through MLST, we found that all the strains belong to the same clonal type ST15. In addition, PFGE results indicated that 26 strains were divided into four PFGE clusters (A, B, C, and D) with similar PFGE patterns (≥ 85% identity, Figure 2). The PFGE pattern showed a close genetic correlation between them. Cluster D accounted for 84.6% (22/26) of all isolates, indicating that these strains were highly clonal.
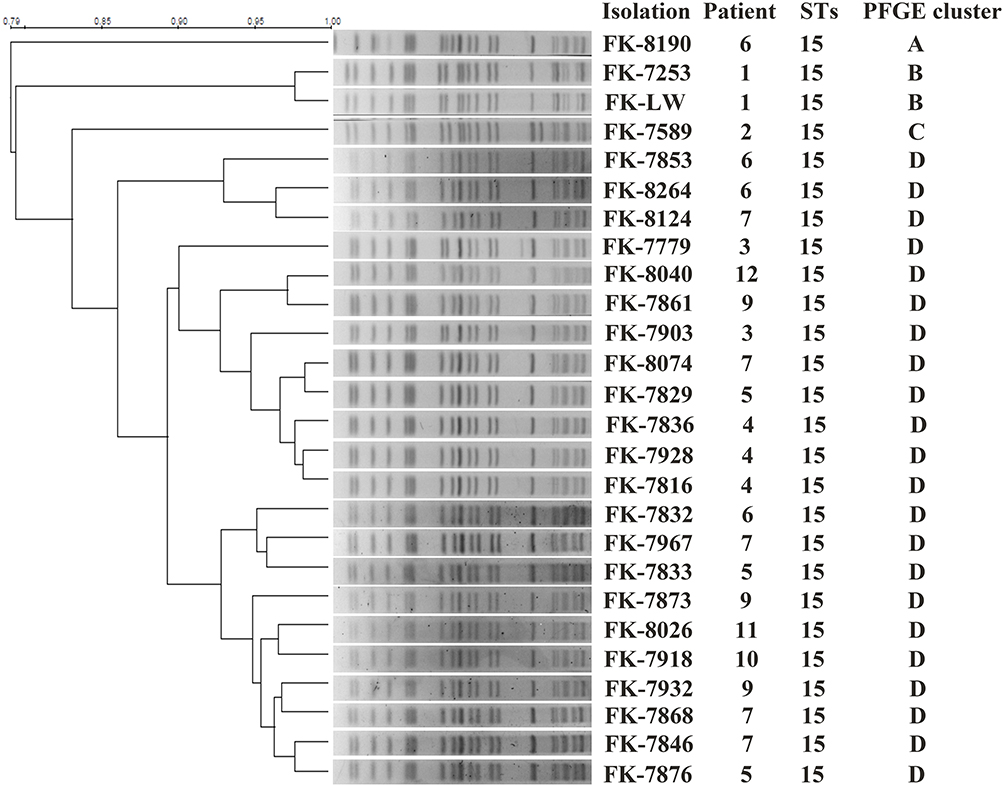 |
Figure 2 PFGE and MLST typing of 26 OXA-232-producing CRKP isolates. PFGE and MLST typing of 26 OXA-232-producing CRKP isolates. Genomic DNA from each research strains was digested using Xba I and the digests were subjected to PFGE to generate diagnostic genomic DNA fragmentation fingerprints. The dendrogram of the PFGE profiles was clustered by the UPGAMA on the basis of the Dice similarity by the Quantity One software package 4.6. |
Antibiotic Resistance in the Isolates
The antibiotic susceptibility test for 26 K. pneumoniae reported high resistance to cephalosporins, aminoglycosides, and fluoroquinolones. The strains were sensitive to ceftazidime/avibactam, colistin, and tigecycline and showed different levels of resistance to different carbapenems (imipenem, meropenem, and ertapenem). All the isolates were resistant to ertapenem (MICs ≥8 μg/mL) but had different levels of resistance to meropenem (MICs ranged from 1 to >64 μg/mL) and imipenem (MICs ranged from 0.5 to >64 μg/mL). The preliminary results of the susceptibility testing to disinfectants (triclosan and chlorhexidine) did not report increased disinfectant resistance (Table 2).
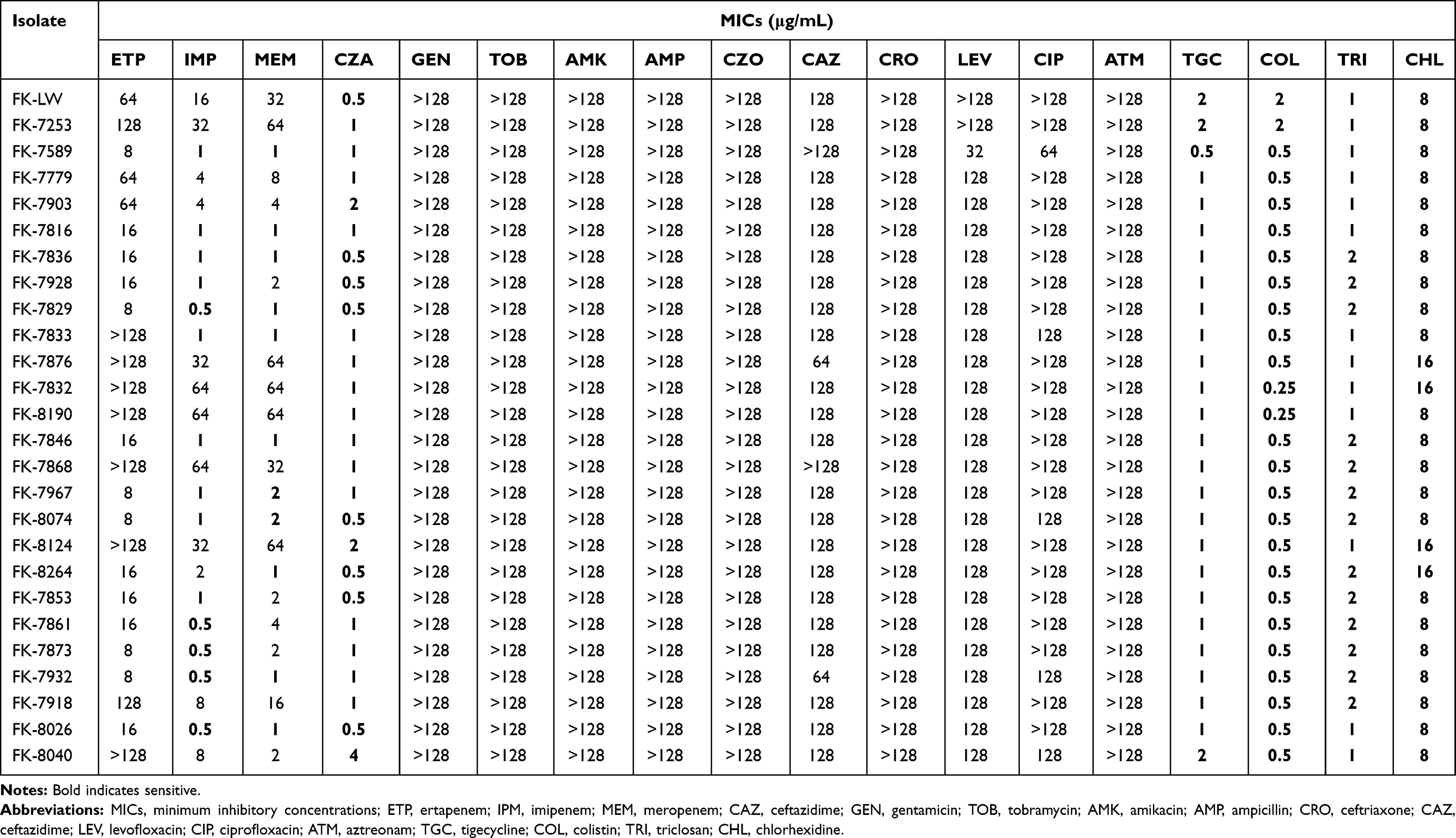 |
Table 2 In vitro Activities of Antimicrobial Agents and Disinfectants Against OXA-232-Producing K. Pneumoniae |
Carbapenem Resistance Genes and Plasmid Transmission
Among all the OXA-232-producing CRKP, eight strains showed ESBL-encoding gene blaCTX-M-15 (Figure 3). The unsuccessful transfer of the plasmid carrying blaOXA-232 to the EC600 and J53 strains through conjugation experiments showed that the plasmid carrying blaOXA-232 was not highly conjugative.
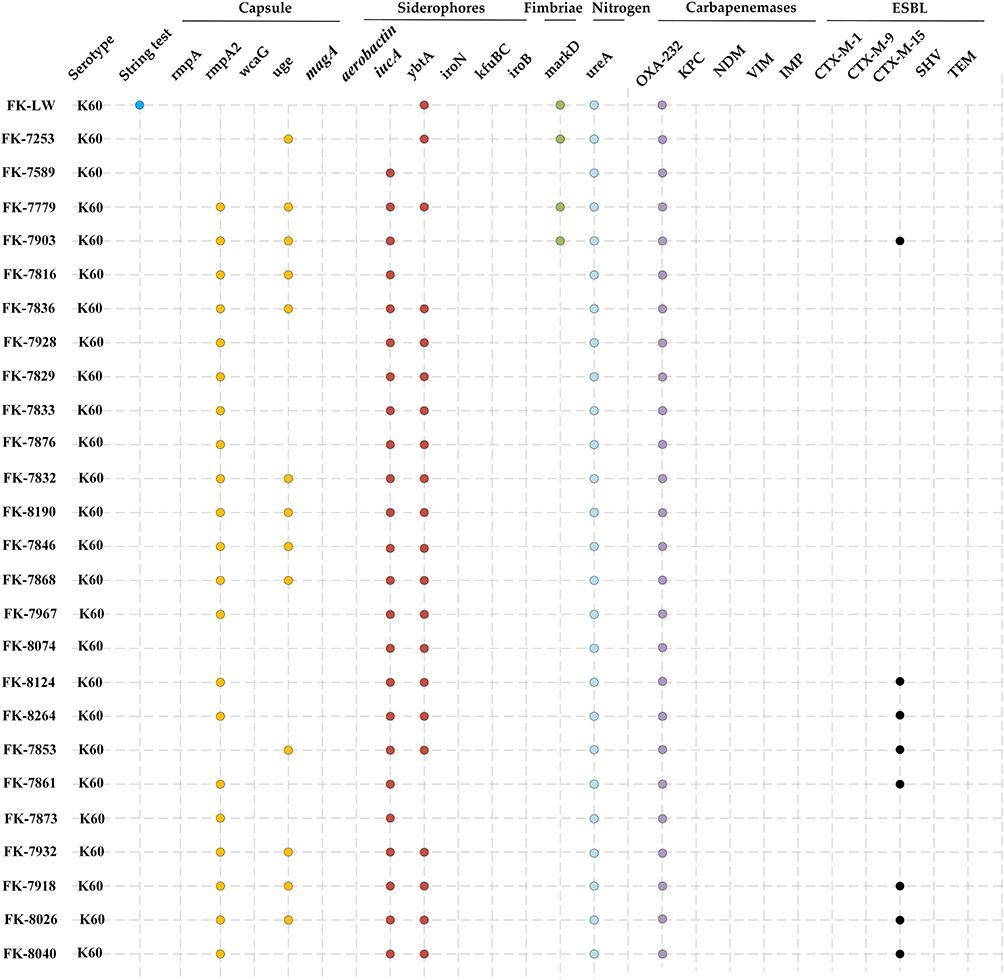 |
Figure 3 Gene profiles of K. pneumoniae isolates. Virulence genes and drug-resistance genes identified by PCR-based profiling are indicated with colored dots. |
Virulence Characteristics of OXA-232-Producing CRKP
Only one strain FK-LW (isolated from the First People’s Hospital of Longwan district) was positive for the string test. The capsular type and virulence genes of OXA-232-producing CRKP were detected by PCR, and the results are presented in Figure 3. The results showed that the rmpA and aerobactin genes, which were closely related to the genes in hypervirulent and capsular type K1 and K2 were not detected in the 26 OXA-232-producing CRKP. The capsular types of all the strains were K60. Among the 26 OXA-232-producing CRKP, the rate of virulence genes rmpA, uge, iucA, ybtA, and ureA in the strains were between 50% and 100%, while the rate of virulence gene markD was relatively low, which was 15.4%. The survival curve of Galleria mellonella larvae infected with the OXA-232-producing CRKP (FK-LW, FK-7859, FK-7779, FK-8190, and FK-7853) is presented in Figure S1. The lethality of the FK-LW strain to Galleria mellonella larvae was time and concentration-dependent. In addition, when the larvae of Galleria mellonella were infected with 106 CFU suspension, the lethality of OXA-232-producing CRKP to Galleria mellonella larvae was close (Figure 4). The virulence level of all OXA-232-producing CRKP was low.
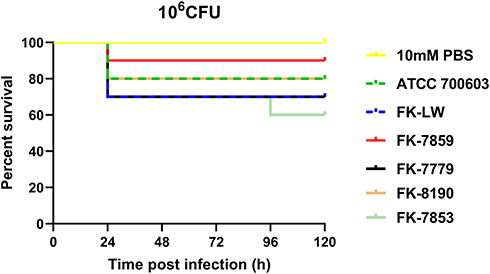 |
Figure 4 The effect of 1×106 colony-forming units (CFU) of each OXA-232-producing CRKP strain on survival was observed in Galleria mellonella. The results do not have statistically significant by the Log rank test. |
Discussion
In this study, we described the outbreak involving a total of 26 K. pneumoniae strains recovered from the patients in a teaching hospital and a secondary hospital in the Zhejiang province in southern China. This outbreak was caused by ST15 K. pneumoniae that produces OXA-232. Although OXA-232 producing K. pneumoniae is not as widespread as KPC-2 producing K. pneumoniae in China, their multi-drug resistance limits the treatment options and poses a potential threat to global public health.
Regarding the source of infection, several epidemiological studies have reported that the hospital outbreak started from the patients themselves, whereas environmental reservoirs, such as hospital sinks/toilets, were the main places responsible for the spread of the infection; and also healthcare workers were potential vectors.16–18 According to our investigation, OXA-232-producing CRKP has appeared in our hospital for the first time. Its source, outbreak trajectory, and the reason for its sudden disappearance are worth exploring for the effective management of the outbreak. According to the clinical data we collected, the prevalence of OXA-232 producing K. pneumoniae in our hospital originated from a secondary hospital because of the patient’s transfer. No large-scale clonal transmission of K. pneumoniae isolated from Patient 1 was observed. More than two months later, PFGE type B K. pneumoniae strain appeared in the bile of Patient 2 and antibiotics could eliminate it. The PFGE profiles of K. pneumoniae isolated from ICU Wards (Patients 3 to 12) were almost identical, indicating that the strains were transmitted via clonal spread in this area. A study has reported that the factors promoting the spread of CRKP strains in the hospital environment include inefficient prevention and control measures, abuse of antibiotics, and improper sewage treatment.19 As we conducted a retrospective study, investigating the specific transmission route was difficult. However, a remarkable fact was observed that inpatients infected with OXA-232-producing CRKP had their beds very close to each other’s beds. We speculated that shared goods or improper disinfection of the patient area might lead to its spread. Among the cases of OXA-232 K. pneumoniae infection, a total of 6 patients died because of severe infection (septic shock) or multiple organ failure and the mortality rate was higher than the previously reported mortality rate on OXA-232 in our country. No new case has been reported since March 2020. We speculated that the use of antimicrobials in the ICU ward led to the disappearance of this strain and our antimicrobial susceptibility results for disinfectants are also consistent with this point (Table 2). Hand hygiene can effectively prevent healthcare-related infections and we suspect that the positive hand hygiene measures of health care workers play a certain role in controlling the dissemination and elimination of OXA-232-producing CRKP.20–22 According to reports, factors such as invasive procedures, ICU admission, and antibiotic exposure increase the risk of infection to patients with CRKP infection.23 This is consistent with our results. Therefore, once there is a risk exposure, surveillance should be conducted as soon as possible.
Currently, in clinical practice, ceftazidime-avibactam and colistin are effective antibiotics against CRKP infection. In our present study, all OXA-232 producing strains were resistant to ertapenem, but some strains were sensitive to imipenem and or meropenem. Even strains resistant to imipenem and/or meropenem showed different levels of resistance. These results were consistent with the results of another study.24 The differences in the MICs may be because of different levels of the beta-lactamase (OXA232).25 In some strains, ESBLs and CTX-M-15 were detected, which might be the reason for the aforementioned drug-resistant phenotype. Although all isolates producing OXA-232 that we detected in our study were sensitive to ceftazidime, tigecycline, and colistin, we still need to be wary of the long-term applications of these drugs that might lead to the emergence of relevant resistant strains. In our study, in cases of scarce treated options, a combination of two or more antibiotics was used to eliminate the drug-resistant strains and reduce the side effects of the drugs.26
The horizontal transmission of mobile elements such as plasmids, phages, integrations, conjugate elements, and insertion elements is a key factor in the outbreak of K. pneumoniae.27 Potron A. and colleagues found that the plasmid-mediated carbapenem-resistance gene blaOXA-232 was located on a small plasmid pOXA-232 of 6,41 bp and carried a ColE-type backbone.4 The plasmid pOXA-232 was a non-conjugative plasmid because it could not be transferred through conjugation experiments.4,9,28 The plasmid in our experimental strains was similar to plasmids in other studies.4–7,9,28,29 The conjugation experiment failed to transfer this blaOXA-232 into E. coli, indicating that it was a non highly conjugative plasmid. However, we found OXA-232-producing E. coli during the outbreak. The OXA-232-producing E. coli appeared in another ward and no correlation case was found. This showed that the prevalence of OXA-232 Enterobacteriaceae in China has been underestimated. We speculate that the spread of blaOXA-232 via Enterobacteriaceae is because of the presence of mobile elements. Further exploration is needed for a better understanding of the spread of blaOXA-232.
For molecular characterization, whole-genome sequencing (WGS) has become the new gold standard. The molecular characterization method used in our study is PFGE, and the PFGE data may not yield the level of discrimination required to differentiate intrafacility transmission from the introduction of a closely related strain from another healthcare facility transmissions.30 However, some studies have confirmed that PFGE is still appropriate for the investigation of local outbreaks and is more economic than WGS.31
pLVPK-like virulent plasmids often have a strong correlation with high hypervirulent phenotypes in ST23 K. pneumoniae, including regulatory factors that encode capsule type (rmpA/rmpA2) and siderophores (iucABCD/iutA/iroBCDN clusters).32 The WGS of ST15 K. pneumoniae carrying blaOXA-232 indicated that although K. pneumoniae positive for blaOXA-232 had pLVPK-like virulence plasmid, its virulence level was low.5 We detected the related gene loci of pLVPK-like virulence plasmid by PCR and found that OXA-232-producing CRKP carried virulence-related genes rmpA2 and iucA but its virulence level was low in Galleria mellonella in vivo-infection model. Although hypervirulent OXA-232-producing CRKP has not been found in China, K. pneumoniae has the potential to evolve to hypervirulent type.10 Hence, there is an urgent need to strengthen surveillance and take strict infection control measures to prevent the widespread of OXA-232-producing CRKP in China.
Conclusion
This study describes a nosocomial outbreak of OXA-232-producing CRKP in our hospital from September 2019 to May 2020. The OXA-232-producing CRKP isolates appeared to be clonally transmitted and ST15 was the clonal cluster leading to the outbreak. Therefore, effective infection control measures are urgently needed to prevent its epidemic in the region in the future.
Ethical Approval
This study was approved by the First Affiliated Hospital of Wenzhou Medical University Ethics Committee. Informed consent was not needed due to the study’s retrospective nature; additionally, the patient data accessed in this research was anonymous. Therefore, the First Affiliated Hospital of Wenzhou Medical University Ethics Committee waived the need for consent.
Acknowledgments
We thank the Health Department of Zhejiang Province of the People’s Republic of China (no. 2011KYA106 and no. 2019KY098) and the National Natural Science Foundation of China (no. 81971986) for providing financial funding.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pitout JDD, Peirano G, Kock MM, Strydom K-A, Matsumura Y. The Global Ascendency of OXA-48-Type Carbapenemases. Clin Microbiol Rev. 2019;33(1):e00102–00119. doi:10.1128/CMR.00102-19
2. de Jonge BLM, Karlowsky JA, Kazmierczak KM, Biedenbach DJ, Sahm DF, Nichols WW. In Vitro Susceptibility to Ceftazidime-Avibactam of Carbapenem-Nonsusceptible Enterobacteriaceae Isolates Collected during the INFORM Global Surveillance Study (2012 to 2014). Antimicrob Agents Chemother. 2016;60:3163–3169. doi:10.1128/AAC.03042-15
3. Karlowsky JA, Lob SH, Kazmierczak KM, et al. In Vitro Activity of Imipenem against Carbapenemase-Positive Enterobacteriaceae Isolates Collected by the SMART Global Surveillance Program from 2008 to 2014. J Clin Microbiol. 2017;55:1638–1649. doi:10.1128/JCM.02316-16
4. Potron A, Rondinaud E, Poirel L, et al. Genetic and biochemical characterisation of OXA-232, a carbapenem-hydrolysing class D beta-lactamase from Enterobacteriaceae. Int J Antimicrob Agents. 2013;41(4):325–329. doi:10.1016/j.ijantimicag.2012.11.007
5. Shu L, Dong N, Lu J, et al. Emergence of OXA-232 Carbapenemase-Producing Klebsiella pneumoniae That Carries a pLVPK-Like Virulence Plasmid among Elderly Patients in China. Antimicrob Agents Chemother. 2019;63(3). doi:10.1128/AAC.02246-18
6. Li X, Ma W, Qin Q, et al. Nosocomial spread of OXA-232-producing Klebsiella pneumoniae ST15 in a teaching hospital, Shanghai, China. BMC Microbiol. 2019;19(1):235. doi:10.1186/s12866-019-1609-1
7. Yin D, Dong D, Li K, et al. Clonal Dissemination of OXA-232 Carbapenemase-Producing Klebsiella pneumoniae in Neonates. Antimicrob Agents Chemother. 2017;61(8). doi:10.1128/AAC.00385-17
8. Tian D, Pan F, Wang C, Sun Y, Zhang H. Resistance phenotype and clinical molecular epidemiology of carbapenem-resistant Klebsiella pneumoniae among pediatric patients in Shanghai. Infect Drug Resist. 2018;11:1935–1943. doi:10.2147/IDR.S175584
9. Weng X, Shi Q, Wang S, Shi Y, Sun D, Yu Y. The Characterization of OXA-232 Carbapenemase-Producing ST437 Klebsiella pneumoniae in China. Can J Infect Dis Med Microbiol. 2020;2020:5626503. doi:10.1155/2020/5626503
10. Yang X, Dong N, Chan EW, Zhang R, Chen S. Carbapenem Resistance-Encoding and Virulence-Encoding Conjugative Plasmids in Klebsiella pneumoniae. Trends Microbiol. 2021;29(1):65–83. doi:10.1016/j.tim.2020.04.012
11. Mukherjee S, Naha S, Bhadury P, et al. Emergence of OXA-232-producing hypervirulent Klebsiella pneumoniae ST23 causing neonatal sepsis. J Antimicrob Chemother. 2020;75(7):2004–2006. doi:10.1093/jac/dkaa080
12. Zhao Y, Zhang X, Torres VVL, et al. An Outbreak of Carbapenem-Resistant and Hypervirulent Klebsiella pneumoniae in an Intensive Care Unit of a Major Teaching Hospital in Wenzhou, China. Front Public Health. 2019;7:229. doi:10.3389/fpubh.2019.00229
13. Morrissey I, Oggioni MR, Knight D, et al. Evaluation of epidemiological cut-off values indicates that biocide resistant subpopulations are uncommon in natural isolates of clinically-relevant microorganisms. PLoS One. 2014;9(1):e86669. doi:10.1371/journal.pone.0086669
14. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
15. Russo TA, Olson R, Fang CT, et al. Identification of Biomarkers for Differentiation of Hypervirulent Klebsiella pneumoniae from Classical K. pneumoniae. J Clin Microbiol. 2018;56(9). doi:10.1128/JCM.00776-18
16. Magiorakos AP, Burns K, Rodriguez Bano J, et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: guidance from the European Centre for Disease Prevention and Control. Antimicrob Resist Infect Control. 2017;6:113. doi:10.1186/s13756-017-0259-z
17. Klein S, Boutin S, Späth I, et al. Acquisition and Transmission of Carbapenemase-Producing (blaKPC-2) Enterobacter cloacae in a Highly Frequented Outpatient Clinic. Clin Infect Dis. 2021;72(5):e158–e161. doi:10.1093/cid/ciaa1734
18. Kizny Gordon AE, Mathers AJ, Cheong EYL, et al. The Hospital Water Environment as a Reservoir for Carbapenem-Resistant Organisms Causing Hospital-Acquired Infections-A Systematic Review of the Literature. Clin Infect Dis. 2017;64(10):1435–1444. doi:10.1093/cid/cix132
19. Pirs M, Cerar Kisek T, Krizan Hergouth V, et al. Successful control of the first OXA-48 and/or NDM carbapenemase-producing Klebsiella pneumoniae outbreak in Slovenia 2014–2016. J Hosp Infect. 2019;101(2):142–149. doi:10.1016/j.jhin.2018.10.022
20. Carter E, Wyer P, Giglio J, et al. Environmental factors and their association with emergency department hand hygiene compliance: an observational study. BMJ Qual Saf. 2016;25(5):372–378. doi:10.1136/bmjqs-2015-004081
21. Ojanperä H, Kanste O, Syrjala H. Hand-hygiene compliance by hospital staff and incidence of health-care-associated infections, Finland. Bull World Health Organ. 2020;98(7):475–483. doi:10.2471/BLT.19.247494
22. Sickbert-Bennett E, DiBiase L, Willis T, Wolak E, Weber D, Rutala W. Reduction of Healthcare-Associated Infections by Exceeding High Compliance with Hand Hygiene Practices. Emerg Infect Dis. 2016;22(9):1628–1630. doi:10.3201/eid2209.151440
23. Snyder BM, Montague BT, Anandan S, et al. Risk factors and epidemiologic predictors of blood stream infections with New Delhi Metallo-b-lactamase (NDM-1) producing Enterobacteriaceae. Epidemiol Infect. 2019;147:e137. doi:10.1017/S0950268819000256
24. Poirel L, Potron A, Nordmann P. OXA-48-like carbapenemases: the phantom menace. J Antimicrob Chemother. 2012;67(7):1597–1606. doi:10.1093/jac/dks121
25. Kocer K, Klein S, Hildebrand D, et al. Pitfalls in genotypic antimicrobial susceptibility testing caused by low expression of blaKPC in Escherichia coli. J Antimicrob Chemother. 2021. doi:10.1093/jac/dkab267
26. Thaden J, Pogue J, Kaye K. Role of newer and re-emerging older agents in the treatment of infections caused by carbapenem-resistant. Enterobacteriaceae Virulence. 2017;8(4):403–416. doi:10.1080/21505594.2016.1207834
27. Zhu J, Li Q, Li X, et al. Successful control of the first carbapenem-resistant Klebsiella pneumoniae outbreak in a Chinese hospital 2017–2019. Antimicrob Resist Infect Control. 2020;9(1):91. doi:10.1186/s13756-020-00757-y
28. Abdul Momin MHF, Liakopoulos A, Phee LM, Wareham DW. Emergence and nosocomial spread of carbapenem-resistant OXA-232-producing Klebsiella pneumoniae in Brunei Darussalam. J Glob Antimicrob Resist. 2017;9:96–99. doi:10.1016/j.jgar.2017.02.008
29. Teo JW, Kurup A, Lin RT, Hsien KT. Emergence of clinical Klebsiella pneumoniae producing OXA-232 carbapenemase in Singapore. New Microbes New Infect. 2013;1(1):13–15. doi:10.1002/2052-2975.4
30. Jiang Y, Wei Z, Wang Y, Hua X, Feng Y, Yu Y. Tracking a hospital outbreak of KPC-producing ST11 Klebsiella pneumoniae with whole genome sequencing. Clin Microbiol Infect. 2015;21(11):1001–1007. doi:10.1016/j.cmi.2015.07.001
31. Martak D, Meunier A, Sauget M, et al. Comparison of pulsed-field gel electrophoresis and whole-genome-sequencing-based typing confirms the accuracy of pulsed-field gel electrophoresis for the investigation of local Pseudomonas aeruginosa outbreaks. J Hosp Infect. 2020;105(4):643–647. doi:10.1016/j.jhin.2020.06.013
32. Struve C, Roe CC, Stegger M, et al. Mapping the Evolution of Hypervirulent. Klebsiella Pneumoniae mBio. 2015;6(4):e00630.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.