")
Back to Journals » Clinical Optometry » Volume 14
Outbreak of COVID-19-Related Myopia Progression in Adults: A Preliminary Study
Authors Kohmarn T , Srisurattanamethakul N, Watcharapalakorn A , Poyomtip T , Poolsanam C
Received 10 May 2022
Accepted for publication 28 July 2022
Published 4 August 2022 Volume 2022:14 Pages 125—131
DOI https://doi.org/10.2147/OPTO.S374155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Mr Simon Berry
Thitika Kohmarn, Noppadol Srisurattanamethakul, Akarapon Watcharapalakorn, Teera Poyomtip, Chotika Poolsanam
Faculty of Optometry, Ramkhamhaeng University, Bangkok, Thailand
Correspondence: Chotika Poolsanam, Email [email protected]
Purpose: The COVID-19 pandemic has necessitated specific public health measures, resulting in the alteration of lifestyles, such as increased digital screen time and fewer outdoor activities. Such conditions have increased the progression of myopia in children. However, no investigation of myopia progression in early adulthood has been conducted during this period. Consequently, this study aimed to evaluate the outbreak of COVID-19-related myopia progression among adults at an optometry clinic during the COVID-19 pandemic.
Materials and Methods: This was a retrospective cohort study in which participants aged 18– 25 years who first visited (baseline) the optometry clinic between June 2019 and March 2020 were recruited for follow-up from November 2021 to March 2022. Spherical equivalent refraction (SER), uncorrected distance visual acuity (UCDVA), and binocular cross cylinder (BCC) were recorded at baseline and a follow-up visit. Using questionnaires, a survey was conducted to assess the lifestyle changes that transpired during the COVID-19 pandemic.
Results: In total, 37 participants with a mean age of 22.5± 1.4 years were enrolled, of which 89.2% were female. Following the outbreak of the COVID-19 pandemic, most participants self-reported increased daily use of digital devices (89.2%), online education (86.5%), and spending more time at home (94.6%), which increased by approximately 7.6± 3.2 hours, 5.9± 1.7 hours, and 13.2± 7.5 hours, respectively. There were statistically significant differences between SER and BCC at baseline and after approximately 2 years of the COVID-19 pandemic (p < 0.05). The mean two-year myopia progression was − 0.59± 0.67 D (Maximum = 0.00 D, Minimum = − 3.38 D).
Conclusion: This study revealed that myopia could progress during adulthood among those who have lived under public health measures intended to address the COVID-19 pandemic.
Keywords: adult myopia progression, COVID-19, lifestyle change, optometry clinic
Introduction
In recent years, the pandemic caused by the coronavirus that arose in 2019 (COVID-19) has had a global impact on almost every aspect of people’s lives as various national governments globally implemented public health measures to prevent physical contact and limit viral transmission. People of all ages were obliged to home quarantine, and outdoor activities were forbidden.1 Such conditions reduced outdoor activities and increased the use of visual display terminals (VTD) to communicate with others as well as maintain productivity, i.e. online learning and working,2,3 resulting in prolonged digital screen time and blue light exposure. Excessive exposure to blue light can have a harmful effect on the retina and may also contribute to a higher incidence of retina disorder.4 In addition, previous publications have indicated lifestyle changes, such as wearing face masks and increasing digital screen time during containment measures, can promote dry eye.5–7 Moreover, prolonged exposure to digital screens during intensive near-work activities and increased time spent on indoor activities are considered well-known risk factors for myopia progression.8,9
Myopia development is determined by age, the age at which myopia first appears, the duration and intensity of myopia, and ethnic origin.10,11 Myopia can progress quickly in children and become stable as they grow older. Nevertheless, some studies have suggested that myopia may get worse after puberty.12–14 During a 2-year study of first-year medical students, Jacobsen et al identified a mean spherical equivalent shift of −0.40 diopter,13 while Lin et al discovered a considerable mean spherical equivalent shift over a 5-year period starting around the age of 18–21 years.14 As a result, myopia progression among young adults is conceivable during the COVID-19 pandemic, which means that focused near-work activities and less time spent outdoors due to public health actions may impact the progression of myopia in early adulthood.
Several previous studies have reported on myopic progression in children and adolescents during the COVID-19 pandemic.15–17 However, no evidence regarding adult myopia progression has been collected during the same period. Therefore, this study aimed to evaluate the outbreak of COVID-19-related myopia progression in early adulthood.
Materials and Methods
Study Design
This study utilized an observational design comprised of a retrospective cohort setting conducted at the Optometry Clinic of Ramkhamhaeng University, located in Bangkok, Thailand. The protocol, following the Declaration of Helsinki and the Belmont Report, was approved by the Ramkhamhaeng Research Ethics Committee (RU-HRE64/0022). All participants were informed regarding the purpose of the study as well as the risks and benefits, and assured that their information would remain confidential. All of the participants signed written informed consent forms. No participants or public figures were involved in the design, conduction, reporting, or dissemination of the plans for this study.
Study Population, Inclusion and Exclusion Criteria
This study considered the case records of patients who visited the optometry clinic between June 2019 and March 2020. The criteria included in this study were as follows: 1) patients were aged from 18–25 years old, 2) patients were clinically examined by optometry students, who were supervised by the authors (TK, NS, and CP), and 3) patients had spherical equivalent refraction (SER) ≤ −0.50 diopter (D) in both eyes. Among these, the patients’ records were excluded from the study if they 1) had SER ≤ −5.0 D at baseline, 2) constantly used contact lenses, 3) had a history of ocular surgery, 4) used addictive drugs, 5) had an ocular disease, ie glaucoma, cataract, and retinal detachment at baseline and follow-up periods, or 6) had a systemic disease, ie diabetes mellitus and hypercholesterolemia. Ultimately, 444 patients were considered as the population for this study.
Sample Size
The sample size was calculated by G-power18 based on a-priori power analysis assuming an effect size of 0.5, alpha of 0.05, and power of 0.95. Therefore, the appropriate sample size to compare the SER was 57 participants. We randomly selected and invited 100 participants by telephone. Among these, 37 participants agreed to enroll in the study, which was lower than the expected sample size. However, it was a suitable sample size for a preliminary study.19,20
Clinical Examinations
At the clinic, the participants were given comprehensive ophthalmic examinations by optometrist students under CP supervision. Visual acuity was measured both monocularly and binocularly in photopic vision by Snellen’s chart at distance and near. For the participants with uncorrected vision of 0.5 decimal (6/12 in meters) or worse, visual acuity testing was repeated with a pinhole occluder, which is an excellent way to screen for disorders of the eyes and uncorrected refractive errors. Refractive error was measured using both objective and subjective refractive techniques. Objective refraction was performed by static (distance) retinoscopy (Neitz, Japan) to determine a starting point, while subjective refraction was performed with a phoropter (Takagi, Japan) to record uncorrected distance visual acuity (UCDVA) and determine the combination of lenses providing the best-corrected distance visual acuity (BCDVA). The binocular cross-cylinder test (BCC) was performed with the cross grid at 40 cm in dim light. This test found the accommodative response while viewing a near target. The LogMAR score was converted from Log10 ((Snellen denominator/Snellen numerator) – (0.02 × number of optotypes read). Since the eyes are a possible mode of transmission21,22 and universal recommendations on safety systems for clinical optometrists and clinical ophthalmologists are lacking,23 all participants had to report negative rapid antigen tests 12 hours before visiting the clinic, and wear facemasks for the entire time. The examiners wore face masks and face shields for all cases. All equipment in this study was disinfected using 70% alcohol for each participant.
Questionnaire
All of the participants were assigned to complete the questionnaire to self-evaluate their lifestyle alterations due to the COVID-19 pandemic, which comprised four questions: 1) “Do you use electronic devices (smartphones, computers, and tablets) in your daily life more since the outbreak of COVID-19?”; 2) “Have you had online classes since the outbreak of COVID-19?”; 3) “Are you spending more time at home since the outbreak of the COVID-19?”; and 4) “Are you spending more time on social media platforms since the outbreak of COVID-19?”
Statistical Analysis
Data were summarized and presented by mean, standard deviation (SD), and percentage of participants. All statistical testing was conducted using SPSS version 18.0 (SPSS, Chicago, IL, USA). The significance level was p-value < 0.05. The Kolmogorov–Smirnov test and Shapiro–Wilk test were used to evaluate the normality of the data. To compare the mean SE and BCC between baseline and follow-up, the Wilcoxon Signed-Rank test was used.
Results
A total of 37 participants completed the examinations, with 33 (89.2%) participants being female. The mean age of all participants was 22.5 ±1.4 years. Most of the participants (89.2%) self-reported that their daily use of digital devices increased by approximately 7.6 ±3.2 hours, and 32 participants (86.5%) indicated that online classrooms were introduced after the start of the COVID-19 pandemic, using 5.9 ±1.8 hours/day. Among the participants, a 94.6% increase in spending more time at home, up to about 13.2 ±7.5 hours per day, was also reported. Moreover, increased spending of time on social media was reported by 78.4% of the participants (Table 1).
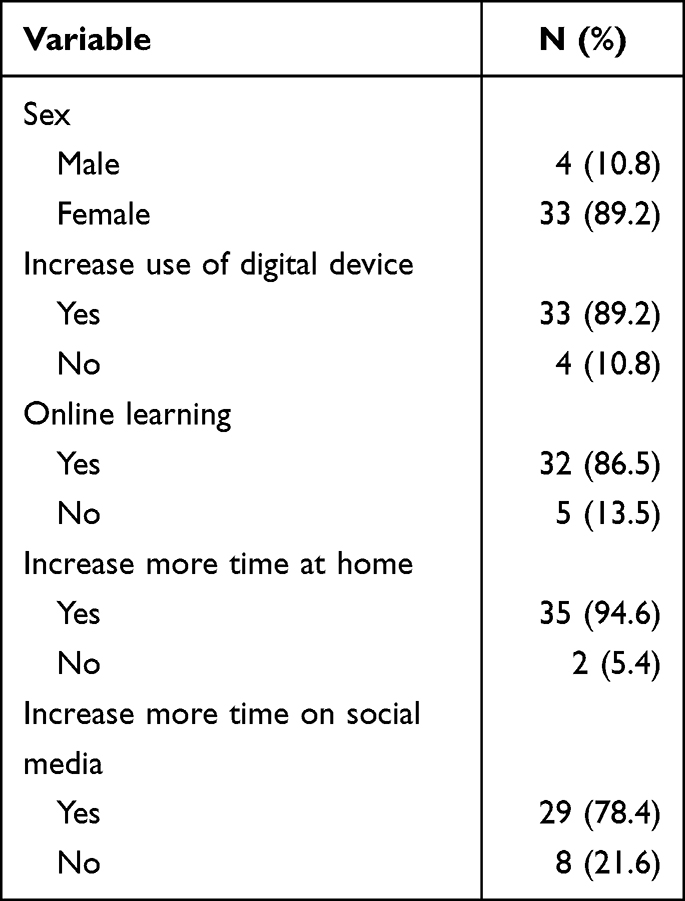 |
Table 1 General Characteristic of Participants (N=37) |
The ocular characteristics (n = 74 eyes) at baseline and follow-up are shown in Table 2. Briefly, the mean UCDVA was 0.62 ± 0.39, and the mean SE was −1.90 ±1.03 D, while the follow-up means of UCDVA and SE were 1.60 ± 0.50 and −2.49 ± 1.30 D, respectively. There was a statistically significant difference between SE before COVID-19 and after approximately 2 years of the pandemic (p-value < 0.05). Additionally, there was a statistically significant difference in the mean binocular cross cylinder (BCC) before COVID-19 and after approximately 2 years of the pandemic (p-value < 0.05). The mean duration between baseline and follow-up was 773 ± 103. The mean two-year myopic progress was −0.59 ±0.67 D (ranged: 0.00 to −3.38 D). Among the 74 eyes, only 21 eyes (28.4%) progressed annually by more than −0.75 D, and 15 eyes (20.3%) showed no myopia progression.
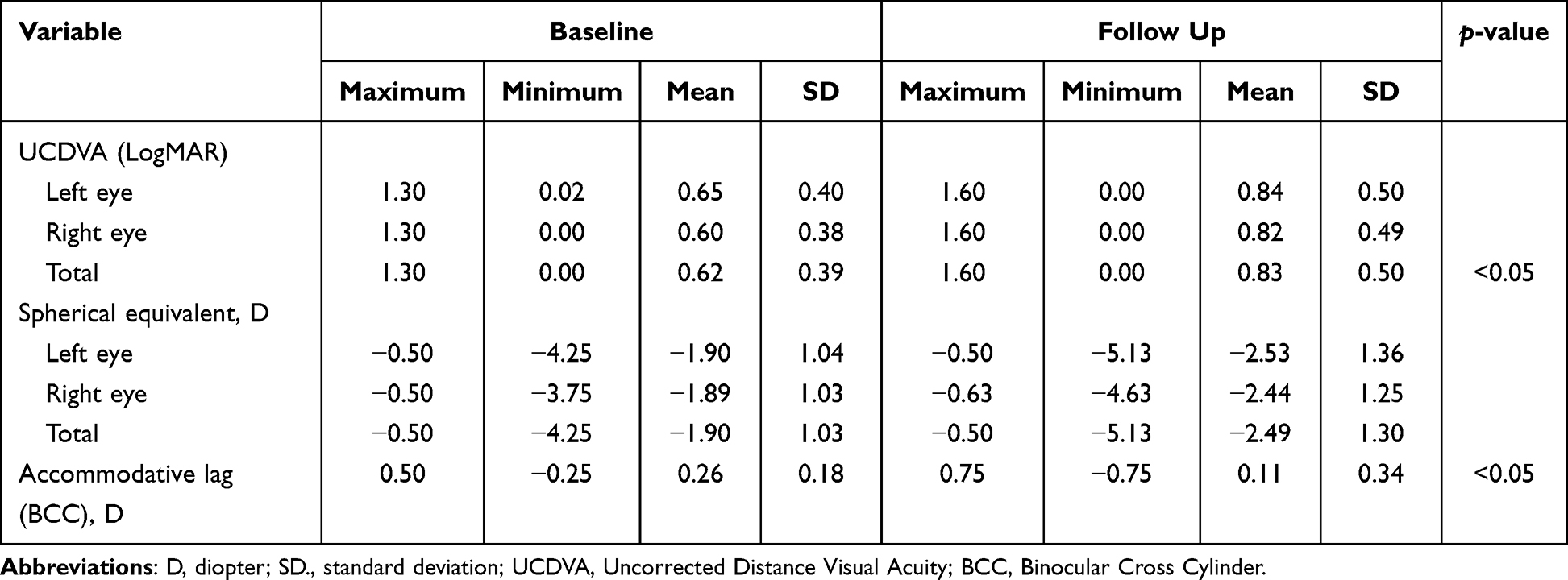 |
Table 2 General Ocular Characteristics of the Participants at Baseline and Follow Up |
Discussion
To the best of our knowledge, this is the first report regarding adult myopic progression during the COVID-19 pandemic. This study reported on lifestyle changes, especially the increase in digital screen time and more time spent on indoor activities and social networking. The mean two-year myopic progression was approximately −0.6 D.
Historically, research on COVID-19-related myopia has been concentrated on myopic shift or myopia control in youths.16,17,24–28 A meta-analysis revealed that the COVID-19 situation, as well as associated public health policies like lockdowns and online education, may have appreciably accelerated myopic progression in children and adolescents when balanced against normal circumstances.29 Resulting from exposure to the risk factors for myopic advancement, particularly extended near-work activity, a high AC/A ratio, and a significant accommodative lag, this trend may also appear in adult myopia with a faster pace.30,31 Unfortunately, only four subjects exhibited no myopic shift in both eyes, so the relationship between these characteristics and myopia development was not investigated in this research.
Although it is difficult to compare adult myopia progression among other studies due to the different durations between baseline and follow-up, methodology, and population,12,14,32–34 and the lack of information concerning adult myopia progression before the outbreak of COVID-19 in our population, the two-year myopia shift −0.6 D indicates a rapid progression from the past. Among Chinese medical students, the significant myopic progress during a 5-year period of follow-up was −0.7±0.65 D and −0.54 ±0.65 D,14 while for a 2-year follow-up, it was −0.29 ±0.37 D and −0.35 ±0.31 D in males and females aged 18–21 years, respectively.12 Takeuchi et al indicated that a 5-year SE change in participants aged 20–29 years who had SE at a baseline of −0.75 to −6.50 D was −0.23 to −0.49 D and −0.19 to −0.39 D in Japanese males and females, respectively.33 McBrien et al reported microscopists aged 21 to 63 years (mean age of 29.7 years) progressed by at least −0.37 D over a 2-year period.32 The prospective single cohort study (Raine Study) examined participants’ eyes at age 20 years and follow-up at 28 years, which indicated a myopic shift of −0.04 D per year.35 In this regard, the main difference from previous studies was the public health measures for COVID-19 that have promoted intensive work on VTD and indoor activity. Therefore, this study suggests that COVID-19-related myopia progression in adults is an ocular health problem that should be considered when public health measures are introduced to prevent physical contact in the digital technology era.
Preventive strategies for myopia control are important, and many studies suggest orthokeratology (Ortho-K) contact lenses are an effective method to mitigate myopia progression in adults.36,37 However, orthokeratology contact lenses may be a more difficult option during the COVID-19 situation. Thus, another way to manage COVID-19-related myopia progression in adults is to wear bifocal or multifocal eyeglasses. These lenses can reduce eye strain while doing work and provide the proper distance prescription when looking at distance targets.38
Other limitations also exist in this study. First, the participants were recruited to visit the optometry clinic from November 2021 to February 2022, during which time the Omicron strain of the pandemic was still ongoing, meaning people in Thailand avoided face-to-face contact. Importantly, both experimental studies and clinical reports suggest that COVID-19 can infect the eyes and cause ocular symptoms.39,40 Thus, it is possible to transmit via the ocular route.21 Both participants and examiners were afraid to get an infection, leading to prospective problems in participant recruitment and causing a small sample size, as well as a low response rate in this study. Moreover, the participants who accepted our invitation and visited the optometry clinic likely had vision problems. Thus, the myopic progress reported in this study may be higher than that of the general population. Subsequently, it was not possible to stratify the participants by sex and SER at baseline for the well-known risk factors of myopic progression.33 Second, the questionnaire used for this study was not validated, which might have affected the results. Lastly, recall bias may have occurred due to the data on the daily use of digital devices, social media use, and spending more time at home being collected by self-reported questionnaires. However, the self-reporting of online classroom time has a minimized recall effect because onsite education is a major system in Thailand. Nevertheless, these limitations should be taken into account when interpreting our results.
Future studies should overcome our limitations by utilizing a larger sample size with a wide range of ages in a community-based setting. Moreover, follow-up at multiple time points should be considered to study the direct effect of public health measures on adult myopic shift during the COVID-19 pandemic, ie comparison of SER change before COVID-19 pandemic, during the pandemic, and after the pandemic becomes endemic. In addition, subgroups by using sex and SER at baseline should be analyzed.
Conclusion
In summary, this preliminary study revealed adult myopic progression and the lifestyle changes that occurred during the COVID-19 pandemic. Therefore, myopic control in adults may be an important point of concern.
Acknowledgments
The authors would like to gratefully thank all of the participants who enrolled in this study. The authors received support from the Faculty of Optometry, Ramkhamhaeng University. This work was supported financially by the 2021 Fund for the Faculty of Optometry, Ramkhamhaeng University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Klaver CCW, Polling JR, Enthoven CA. 2020 as the year of quarantine myopia. JAMA Ophthalmol. 2021;139(3):300–301. doi:10.1001/jamaophthalmol.2020.6231
2. Majumdar P, Biswas A, Sahu S. COVID-19 pandemic and lockdown: cause of sleep disruption, depression, somatic pain, and increased screen exposure of office workers and students of India. Chronobiol Int. 2020;37(8):1191–1200. doi:10.1080/07420528.2020.1786107
3. Nagata JM, Abdel Magid HS, Pettee Gabriel K. Screen time for children and adolescents during the Coronavirus Disease 2019 pandemic. Obesity. 2020;28(9):1582–1583.
4. Kozlowski MR. Blue light-induced retinal damage: a brief review and a proposal for examining the hypothetical causal link between person digital device use and retinal injury. Med Hypothesis Discov Innov Optom. 2020;1(3):6.
5. Saldanha IJ, Petris R, Makara M, Channa P, Akpek EK. Impact of the COVID-19 pandemic on eye strain and dry eye symptoms. Ocul Surf. 2021;22:38–46.
6. Napoli PE, Nioi M, Fossarello M. The “Quarantine Dry Eye”: the lockdown for Coronavirus Disease 2019 and its implications for ocular surface health. Risk Manag Healthc Policy. 2021;14:1629–1636.
7. Giannaccare G, Vaccaro S, Mancini A, Scorcia V. Dry eye in the COVID-19 era: how the measures for controlling pandemic might harm the ocular surface. Graefes Arch Clin Exp Ophthalmol. 2020;258(11):2567–2568.
8. Karthikeyan SK, Ashwini DL, Priyanka M, Nayak A, Biswas S. Physical activity, time spent outdoors, and near work in relation to myopia prevalence, incidence, and progression: an overview of systematic reviews and meta-analyses. Indian J Ophthalmol. 2022;70(3):728–739.
9. Gajjar S, Ostrin LA. A systematic review of near work and myopia: measurement, relationships, mechanisms and clinical corollaries. Acta Ophthalmol. 2021;100(4):376–387.
10. Chua SY, Sabanayagam C, Cheung YB, et al. Age of onset of myopia predicts risk of high myopia in later childhood in myopic Singapore children. Ophthalmic Physiol Opt. 2016;36(4):388–394. doi:10.1111/opo.12305
11. Dolgin E. The myopia boom. Nature. 2015;519(7543):276–278. doi:10.1038/519276a
12. Lv L, Zhang Z. Pattern of myopia progression in Chinese medical students: a two-year follow-up study. Graefes Arch Clin Exp Ophthalmol. 2013;251(1):163–168. doi:10.1007/s00417-012-2074-9
13. Jacobsen N, Jensen H, Goldschmidt E. Does the level of physical activity in university students influence the development and progression of myopia?–a 2-year prospective cohort study. Invest Ophthalmol Vis Sci. 2008;49(4):1322–1327. doi:10.1167/iovs.07-1144
14. Lin LL, Shih YF, Lee YC, Hung PT, Hou PK. Changes in ocular refraction and its components among medical students–a 5-year longitudinal study. Optom Vis Sci. 1996;73(7):495–498. doi:10.1097/00006324-199607000-00007
15. Mohan A, Sen P, Peeush P, Shah C, Jain E. Impact of online classes and home confinement on myopia progression in children during COVID-19 pandemic: digital eye strain among kids (DESK) study 4. Indian J Ophthalmol. 2022;70(1):241–245. doi:10.4103/ijo.IJO_1721_21
16. Wang W, Zhu L, Zheng S, et al. Survey on the progression of myopia in children and adolescents in Chongqing during COVID-19 pandemic. Front Public Health. 2021;9:646770. doi:10.3389/fpubh.2021.646770
17. Wang J, Li Y, Musch DC, et al. Progression of myopia in school-aged children after COVID-19 home confinement. JAMA Ophthalmol. 2021;139(3):293–300. doi:10.1001/jamaophthalmol.2020.6239
18. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
19. Viechtbauer W, Smits L, Kotz D, et al. A simple formula for the calculation of sample size in pilot studies. J Clin Epidemiol. 2015;68(11):1375–1379. doi:10.1016/j.jclinepi.2015.04.014
20. Whitehead AL, Julious SA, Cooper CL, Campbell MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. 2016;25(3):1057–1073. doi:10.1177/0962280215588241
21. Napoli PE, Nioi M, d’Aloja E, Fossarello M. The ocular surface and the Coronavirus Disease 2019: does a dual ‘ocular route’ exist? J Clin Med. 2020;9(5):1269. doi:10.3390/jcm9051269
22. Davis G, Li K, Thankam FG, Wilson DR, Agrawal DK. Ocular transmissibility of COVID-19: possibilities and perspectives. Mol Cell Biochem. 2022;477(3):849–864. doi:10.1007/s11010-021-04336-6
23. Napoli PE, Nioi M, d’Aloja E, Fossarello M. Safety recommendations and medical liability in ocular surgery during the COVID-19 pandemic: an unsolved dilemma. J Clin Med. 2020;9(5):1403. doi:10.3390/jcm9051403
24. Hu Y, Zhao F, Ding X, et al. Rates of myopia development in young Chinese schoolchildren during the outbreak of COVID-19. JAMA Ophthalmol. 2021;139(10):1115–1121. doi:10.1001/jamaophthalmol.2021.3563
25. Zhang X, Cheung SSL, Chan HN, et al. Myopia incidence and lifestyle changes among school children during the COVID-19 pandemic: a population-based prospective study. Br J Ophthalmol. 2021;
26. Erdinest N, London N, Levinger N, Lavy I, Pras E, Morad Y. Decreased effectiveness of 0.01% atropine treatment for myopia control during prolonged COVID-19 lockdowns. Cont Lens Anterior Eye. 2021;45:101475. doi:10.1016/j.clae.2021.101475
27. Ma M, Xiong S, Zhao S, Zheng Z, Sun T, Li C. COVID-19 home quarantine accelerated the progression of myopia in children aged 7 to 12 years in China. Invest Ophthalmol Vis Sci. 2021;62(10):37. doi:10.1167/iovs.62.10.37
28. Xu L, Ma Y, Yuan J, et al. COVID-19 quarantine reveals that behavioral changes have an effect on myopia progression. Ophthalmology. 2021;128(11):1652–1654.
29. Watcharapalakorn A, Poyomtip T, Tawonkasiwattanakun P. Coronavirus disease 2019 outbreak and associated public health measures increase the progression of myopia among children and adolescents: evidence synthesis. Ophthalmic Physiol Opt. 2022;42(4):744–752.
30. Bullimore MA, Reuter KS, Jones LA, Mitchell GL, Zoz J, Rah MJ. The study of progression of adult nearsightedness (SPAN): design and baseline characteristics. Optom Vis Sci. 2006;83(8):594–604.
31. Kaphle D, Varnas SR, Schmid KL, Suheimat M, Leube A, Atchison DA. Accommodation lags are higher in myopia than in emmetropia: measurement methods and metrics matter. Ophthalmic Physiol Opt. 2022. doi:10.1111/opo.13021
32. McBrien NA, Adams DW. A longitudinal investigation of adult-onset and adult-progression of myopia in an occupational group. Refractive and biometric findings. Invest Ophthalmol Vis Sci. 1997;38(2):321–333.
33. Takeuchi M, Meguro A, Yoshida M, et al. Longitudinal analysis of 5-year refractive changes in a large Japanese population. Sci Rep. 2022;12(1):2879.
34. Zadnik K, Mutti DO. Refractive error changes in law students. Am J Optom Physiol Opt. 1987;64(7):558–561.
35. Lee SS, Lingham G, Sanfilippo PG, et al. Incidence and progression of myopia in early adulthood. JAMA Ophthalmol. 2022;140(2):162–169.
36. Gifford KL, Gifford P, Hendicott PL, Schmid KL. Zone of clear single binocular vision in myopic orthokeratology. Eye Contact Lens. 2020;46(2):82–90.
37. Gonzalez-Meijome JM, Carracedo G, Lopes-Ferreira D, Faria-Ribeiro MA, Peixoto-de-Matos SC, Queiros A. Stabilization in early adult-onset myopia with corneal refractive therapy. Cont Lens Anterior Eye. 2016;39(1):72–77.
38. Lam CSY, Tang WC, Tse DY, et al. Defocus Incorporated Multiple Segments (DIMS) spectacle lenses slow myopia progression: a 2-year randomised clinical trial. Br J Ophthalmol. 2020;104(3):363–368.
39. Ma N, Li P, Wang X, et al. Ocular manifestations and clinical characteristics of children with laboratory-confirmed COVID-19 in Wuhan, China. JAMA Ophthalmol. 2020;138(10):1079–1086.
40. Wu P, Duan F, Luo C, et al. Characteristics of ocular findings of patients with Coronavirus Disease 2019 (COVID-19) in Hubei province, China. JAMA Ophthalmol. 2020;138(5):575–578.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.