")
Back to Journals » International Journal of General Medicine » Volume 12
Out Of Hospital And In Hospital Management Of Cellulitis Requiring Intravenous Therapy
Authors Ong BS , Ngian VJJ , Yeong C , Keighley C
Received 6 September 2019
Accepted for publication 6 November 2019
Published 29 November 2019 Volume 2019:12 Pages 447—453
DOI https://doi.org/10.2147/IJGM.S230054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bin S Ong,1–3 Vincent Jiu Jong Ngian,1,2 Clarence Yeong,1 Caitlin Keighley1
1Bankstown-Lidcombe Hospital, Bankstown, NSW, Australia; 2University of New South Wales, Sydney, NSW, Australia; 3Department of Ambulatory Care, Bankstown-Lidcombe Hospital, Bankstown, NSW 2200, Australia
Correspondence: Bin S Ong
Department of Ambulatory Care, Bankstown-Lidcombe Hospital, Eldridge Road, Bankstown, NSW 2200, Australia
Tel +61 2 97228637
Email [email protected]
Background: Cellulitis requiring intravenous therapy can be managed via out of hospital programs, but a high number of patients are still admitted to hospital.
Objective: We aimed to review the clinical features, management and outcomes of patients with cellulitis requiring intravenous therapy in a Hospital in the Home (HITH) program compared to patients who are admitted to hospital.
Methods: A prospective cohort study of patients with limb cellulitis requiring intravenous antibiotics was conducted at a metropolitan principal referral hospital.
Results: A total of 100 patients out of 113 eligible patients were recruited. Forty-eight were treated entirely in hospital and 52 were treated entirely or partially via HITH. Patients treated in hospital were older (mean 69.2 vs 56.7 years, p<0.001), less mobile, have more comorbidities (Charlson Comorbidity Index mean 2.2 vs 1.2, P=0.005) and more associated active illness. All patients with Eron Class III were admitted to hospital. Patients treated in hospital had a higher incidence of acute renal failure (27.1% vs 3.8%, p=0.001), nosocomial infection (10.4% vs 0.0%, P=0.023), and a higher 28-day hospital readmission rate (10.4% vs 0.0%, P=0.023).
Conclusion: Approximately half of the patients who require intravenous therapy can be treated via an out of hospital program. Patients admitted to hospital were more unwell and more likely to suffer complications. The presence of comorbid illness does not necessarily exclude participation in HITH and careful selection is essential to ensure safe outcomes.
Keywords: cellulitis, hospital in the home, outpatient parenteral antimicrobial therapy
Introduction
Cellulitis requiring intravenous therapy is a condition that can be managed via out of hospital programs, commonly named Hospital in the Home (HITH), Outpatient Parenteral Antimicrobial Therapy (OPAT) or Community-based Parenteral Antimicrobial Therapy (CoPAT). Treatment in these programs for selected patients have been found to be safe1–3 with similar outcomes to traditional inpatient treatment.4 Home intravenous treatment of cellulitis is also estimated to be cheaper.5,6 Patients treated at home were found to have fewer complications7,8 less functional decline9 and greater satisfaction.10 In Australia, cellulitis accounted for over 250,000 hospital bed days, or 10.5% of potentially preventable hospitalizations, in 2013–14.11 Reducing this number by a fraction would additionally result in significant cost savings to the health care system.
The outcome of cellulitis with appropriate treatment is good in the majority of cases. Initial treatment failure can occur in 16.6% of hospitalized patients.12 However for appropriately selected patients in an out of hospital program, treatment success rate is around 90%.3,13,14 Complications of cellulitis include osteomyelitis and septic arthritis, bacteremia and sepsis.15 Outcome measures that are used by most studies include complications, prolonged hospital stay, recurrence, readmission to hospital and mortality.16–19,
Known risk factors for poorer outcomes in cellulitis can be used to assess suitability for management in HITH programs. These include age >60, weight >100 kg and body mass index (BMI) >40, congestive cardiac failure diabetes, liver disease, chronic pulmonary disease, altered mental status, tachycardia, hypotension, elevated serum creatinine, neutrophilia/neutropenia, hypoalbuminemia, bacteraemia.16–19 Other risk factors for treatment failure in out of hospital programs were noted to be female gender and treatment with Teicoplanin.13 The presence of these risk factors however in themselves do not exclude participation in HITH programs. The degree of risk depends on the severity and acuity of each condition. Furthermore, patients initially admitted to hospital may continue their treatment via HITH when their clinical status improves. There is currently little detailed clinical literature on the target proportion of patients with treatable conditions who can be managed in these programs, or detailed information on factors that limit the treatment of patients in these programs.
We aimed to describe the management of cellulitis and assess the proportion of patients treated via a HITH program. We also aimed to review the factors which lead to hospital admission, where future strategies can be targeted to increase uptake to HITH.
Setting
The Bankstown Ambulatory Care Unit is based in Bankstown-Lidcombe Hospital, a 433 bed metropolitan principal referral hospital which has over 55,000 admissions per year, serving a population of over 193,000 people. The Ambulatory Care Unit manages HITH services, as well as the Day Hospital and acute clinics. It has dedicated medical and nursing staff. Patients are treated in the Ambulatory Care Unit or at home where home visits up to twice a day are provided by community nurses. Other monitoring and contact with the patient may occur by phone.
Methods
We performed a prospective observational study in Bankstown-Lidcombe Hospital, New South Wales, Australia from June 2014 to April 2015. The study was approved by the South-Western Sydney Local Health District (SWSLHD) Ethics Committee. All participants in the study provided informed consent. This study was conducted in accordance with the Declaration of Helsinki.
Patients aged 18 years and above were consecutively recruited if they had a clinical diagnosis of cellulitis and treated with intravenous antibiotics as directed by the admitting clinician. Patients were identified through review of the entire hospital inpatient list three times a week by a study investigator, who obtained signed informed consent for eligible participants. Patients with clinical symptoms and signs consistent with cellulitis, particularly that of erythema, edema and warmth were included in the study. We excluded pregnant patients and those with post-operative wound infections.
Patients were classified as HITH if they were directly admitted to HITH or continued treatment via HITH after hospital admission. Data collected included basic demographics, clinical characteristics, relevant investigations, treatment provided and clinical outcomes. The severity of cellulitis was derived from the Eron classification.20 The Charlson Comorbidity Index21 was calculated from the clinical data. Associated active illness was defined as worsening of comorbidity such as additional diuresis in the setting of known congestive cardiac failure or worsening chronic renal failure requiring fluids. Acute renal failure was defined according to the Kidney Disease Improving Global Guidelines (KDIGO).22 Nosocomial infection was recorded when it was diagnosed and documented by the treating team. Patients were followed up for 28 days following completion of intravenous antibiotics to evaluate for clinical recurrence, hospital readmission and mortality. The 28-day outcome was determined from hospital information systems as well as through telephone contact with participants. We compared the clinical characteristics and outcomes of patients in two cohorts – patients who were entirely treated in hospital, and those who were treated partially or entirely in the Ambulatory Care HITH program.
Data were analyzed using SPSS Version 24 and R version 3.3.1. Two-tailed chi-square tests with Yates continuity correction were used to compare proportions. Student’s t-test was used to compare differences in means for normally distributed variables. For non-normally distributed continuous variables, non-parametric test was used to assess differences in the ranked median scores. Statistically significant results were set at an alpha level of 0.05.
Results
A total of 113 patients were identified during the period of study and 100 patients (88.5%) consented to participate. Of the patients who consented 48 (48.0%) were treated entirely in hospital and 52 (52.0%) were treated entirely or partially via the HITH program. Of the patients treated via HITH program, 25 (48.1%) were treated from admission to discharge entirely via HITH, and 27 (51.9%) were initially admitted into hospital and discharged via HITH.
Patients treated in hospital were older with a mean age of 69.2 ±18.2 years compared to 56.7 ±18.2 years (p<0.001) for patients treated via HITH. A higher proportion treated entirely in hospital were from an Aged Care facility (20.8% vs 0% respectively, p<0.0004) and had impaired mobility (47.9% vs 7.7%, respectively, p<0.0001). The proportion of prior oral antibiotic use in the hospital and HITH treated patients were not significant (37.5% vs 50.0%, p=0.208) (Table 1).
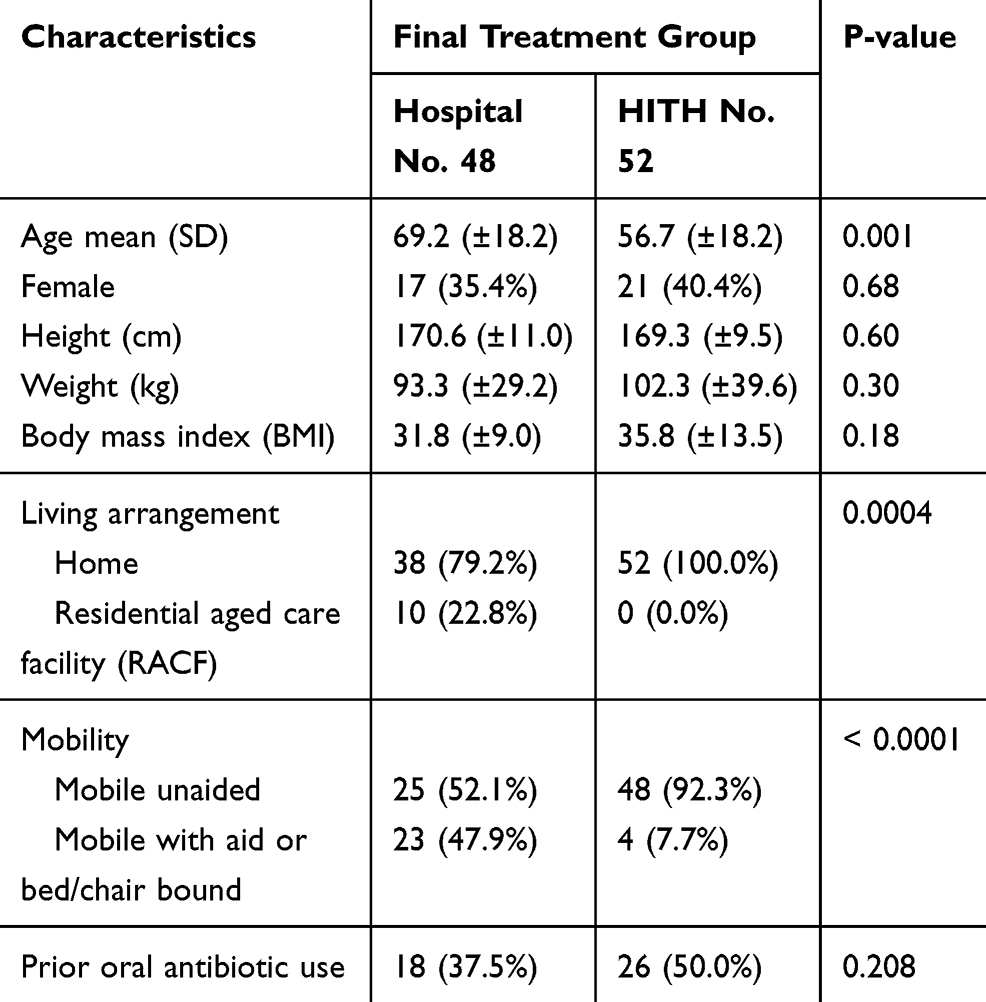 |
Table 1 Patient Demographics |
Patients treated in the hospital also were more unwell. This group had a higher Charlson Comorbidity Index (mean 2.2 [±1.9] vs 1.2[±1.5] p=0.005). A significantly higher proportion of patients treated in hospital was found to have dementia (14.6% vs 0%, respectively, p=0.005), depression (16.7% vs 1.9%, respectively, p=0.013) and cancer (16.7% vs 0%, respectively, p=0.002). Proportions of the other comorbidities assessed were also higher but these were not statistically significant (Table 2).
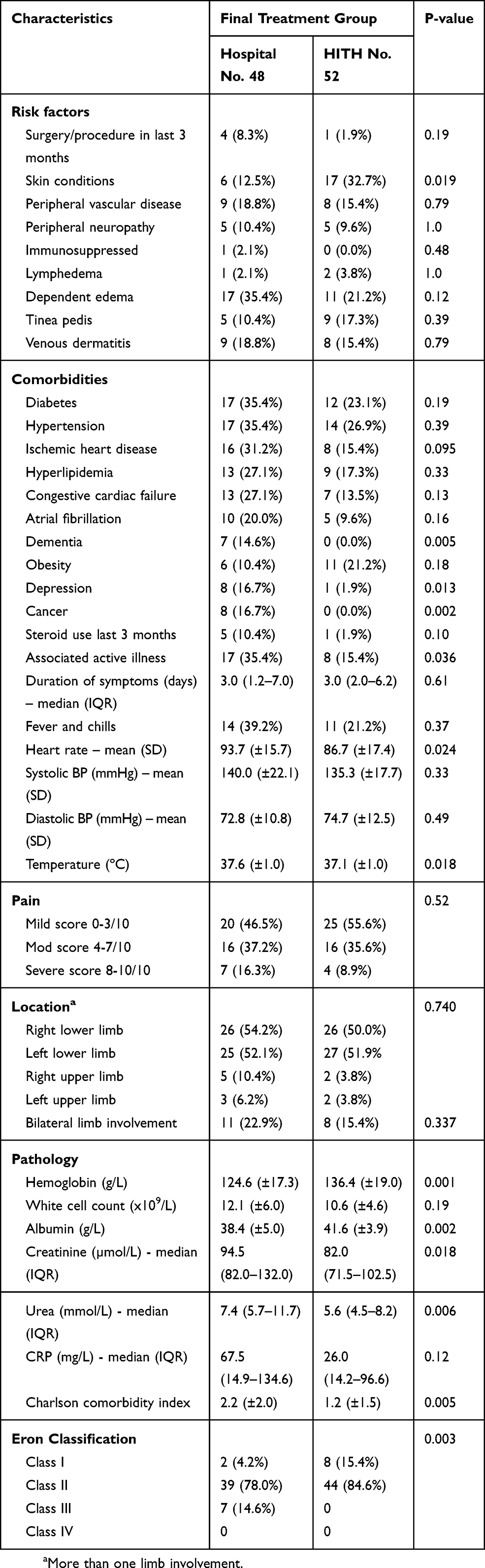 |
Table 2 Clinical Characteristics – Risk Factors |
Patients with more severe cellulitis of Eron Class III were all admitted to hospital. A small number of patients of Eron Class I were admitted to hospital with the majority treated via HITH (4.2% vs 15.4% p=0.003). The majority of patients admitted to hospital and treated via HITH were of Eron Class II. There were minor differences with specific vital signs but the mean heart rate (93.7[±15.7] vs 86.7[±17.4], p=0.024) and the mean temperature (37.6 °C [±1.0] vs 37.1 °C [±1.0], P=0.018) were higher in the patients treated in hospital. There was no statistically significant difference in the pain scores. Investigations revealed a lower mean hemoglobin (124.6 g/L [±17.3] vs 136.4 g/L [±19.0], p=0.001), mean albumin (38.4 g/L [±5.0] vs 41.6 g/L [±3.9], p=0.002), higher mean Urea (7.4 mmol/L vs 5.6 mmol/L, P=0.006). There was no significant difference in the mean white cell count (WCC) or C-reactive protein (CRP) levels.
Patients with Eron class of I or II and who were initially treated as inpatient tend to report more chills and fever (32.4% vs 11.8% p=0.03); had significantly higher mean WCC (12.3x109/L [±5.9] vs 9.2x109/L [±3.0] p=0.006) and higher median CRP (105.3 mg/L [31–213] vs 36 mg/L [15.3–131] p=0.028). More patients in this group had an associated active illness that required treatment (30.9% vs 11.8% p=0.05) and have higher mean Charlson Comorbidity Index (1.9 [±1.9] vs 1.2 [±1.7] p=0.049).
Compared to hospital-treated patients, Cefazolin was the most common antibiotic prescribed in HITH (82.7% vs 31.2%) and Flucloxacillin was more common in the hospital-treated group (33.3% vs 13.5%) p<0.0001.
Patients treated in hospital had a higher complication rate. Statistically significant differences were found in the incidence of acute renal failure (27.1% vs 3.8%, p=0.001), nosocomial infection (10.4% vs 0.0%, P=0.023) and readmission to hospital within 28 days (10.4% vs 0.0%, P=0.023). Of the five patients who were readmitted to hospital, three had recurrent cellulitis and two had osteomyelitis. Two patients treated in hospital died, whereas there were no deaths in patients treated via HITH (Table 3).
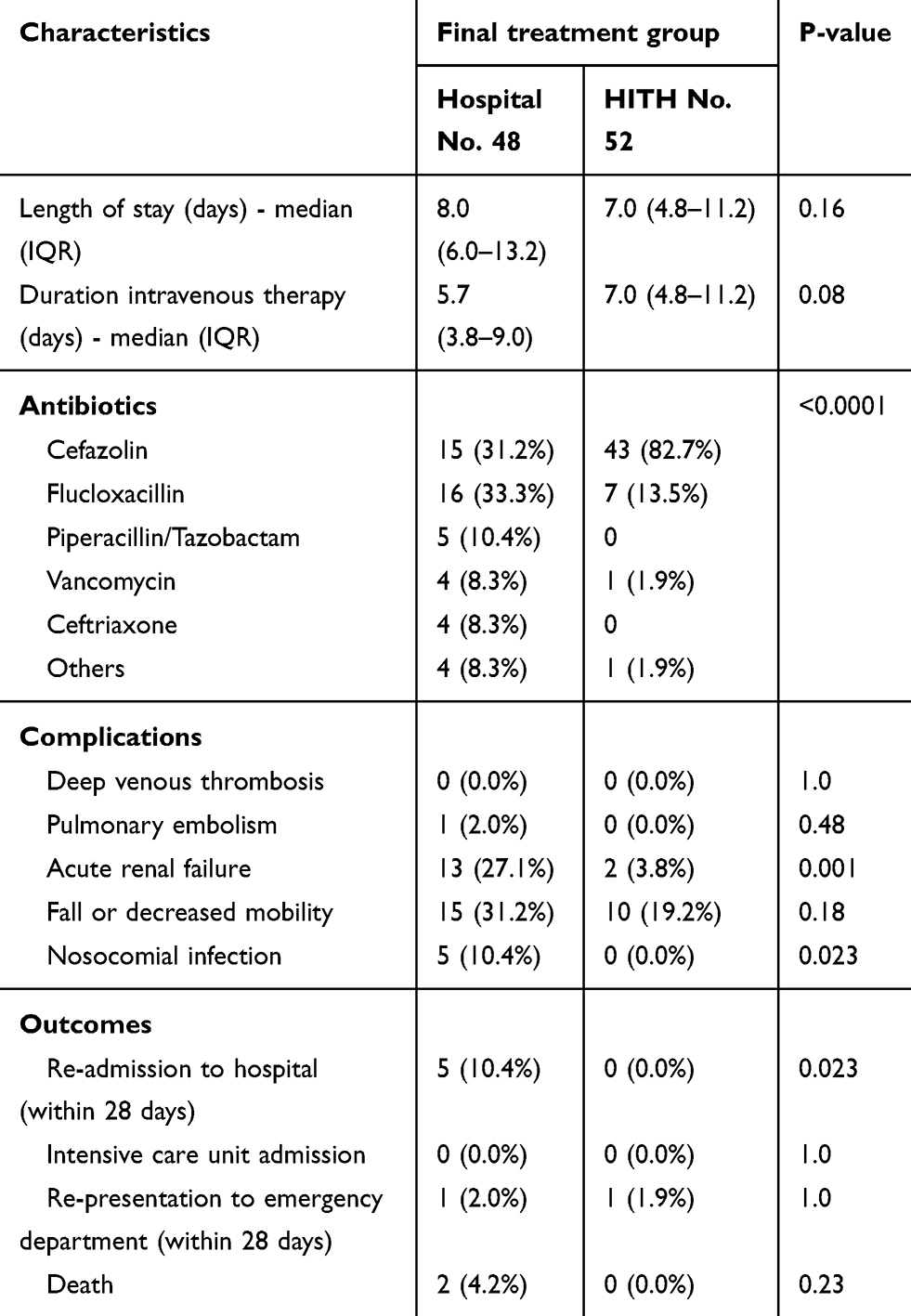 |
Table 3 Treatment, Complications And Outcomes |
Discussion
We found that half of patients who present with cellulitis and require intravenous therapy can be treated via HITH. Information for the patients who did not consent to participate was not collected. Even if all these patients were admitted to hospital, the participation rate of HITH would be 52 out of 113 patients (46%) and so would not significantly have differed.
While patients admitted to hospital were older, 38.5% of patients treated via HITH were over 65, indicating that age should not exclude treatment via HITH. Surprisingly during the study period patients in residential-aged care facilities (RACF) were treated in hospital even though HITH services were available in RACF. Further analysis of this group, however, showed that these patients were more unwell and had more comorbidities.
Patients managed in HITH were more mobile, suggesting that improving mobility can potentially expedite early discharge via an out of hospital program. However, as impaired mobility and functional status correlate with illness severity,23 hospital admission would be required for the majority of these patients. Impaired mobility is usually also associated with a higher need for personal care support.
Patients with severe illness require hospital admission as the intensity of monitoring and treatment required is not available in HITH programs. The presence of unstable vital signs mandates hospital admission, as may poorer biochemical markers such as albumin and urea. Systemic parameters however vary, so where there is clinical concern, a longer period of observation would be required prior to participation in a HITH program. We found no patients higher than Eron Class II cellulitis were treated in HITH.
The majority of cellulitis infections are due to beta-hemolytic streptococci and less commonly methicillin-sensitive S. aureus, making Cefazolin and Flucloxacillin appropriate empiric initial therapy. Cefazolin has a longer duration of action than Flucloxacillin and is logistically easier to use than Flucloxacillin. Flucloxacillin has to be given four times a day, or requires the insertion of a central line and delivered via an infuser pump. In contrast, Cefazolin can be given less frequently in out of hospital programs, commonly at a dose of 2 g twice a day. Infections with resistant organisms and complicated infections, which require alternative antibiotics such as Vancomycin, usually require insertion of a central line, following which patients may be treated in out of hospital programs.
We noted a trend towards a longer duration of intravenous therapy in patients in HITH. A longer length of stay has been previously noted in HITH patients.24 Potential causes include less frequent clinical reviews by medical staff in HITH as compared to in hospital, accessibility of infectious disease consultation service, and a risk-averse approach to early de-escalation to oral therapy. It is worth noting that this longer length of stay is within the home environment rather than imposing on the hospital system, though it is unclear whether longer bed rest in hospital promotes faster recovery. Further study is required to examine this.
Patients treated in hospital also have more medical comorbidities as demonstrated by a higher Charlson Comorbidity Index, and a higher prevalence of associated active illness. We found that patients with dementia and cancer tended to be admitted to hospital. There was no significant association with hospital admission for the other common comorbidities. The presence of these comorbidities do not therefore preclude treatment in HITH programs, requiring the clinician to assess the acuity, severity and accompanying clinical risk of these conditions holistically.
The outcomes of patients treated via HITH were generally good with a low 28-day readmission rate; 10% of patients admitted to hospital were readmitted within 28 days. Complications were more common in the group admitted to hospital. There was a higher incidence of nosocomial infection and acute renal failure. There was also a higher falls rate, though this did not reach statistical significance. There were two deaths in patients admitted to hospital, while low, a little higher than the reported rate of 1.1%.25 Further analysis of patients with Eron Class II cellulitis only, also revealed similar results with a higher incidence of nosocomial infection and acute renal failure in hospitalized patients. A full propensity analysis was not possible due to low numbers in some groups, and we were otherwise unable to ascertain whether it is concomitant comorbidities or hospitalization that contributed more to the higher complication rate. A larger study may be able to examine this further. A meta-analysis of randomized controlled trials had found that for many conditions, out of hospital programs were associated with fewer complications and better outcomes.26
Admission criteria for HITH programs include acuity and complexity of illness, functional status and service-related issues including appropriate venous access. For less acute patients, the degree to which these factors influence the decision to treat in HITH programs depend on the comfort zone of the treating clinician as well as the capacity of the services to address the other care needs of the patient. The clinical trajectory of the majority of patients with cellulitis is good, but clinical variations can occur, particularly when patients have concurrent active comorbidities. Effective management of patients in HITH requires careful risk management with prompt intervention and treatment when clinical condition changes. With the staffing and structure in our service, we are able to treat moderately complex patients in HITH. The low hospital readmission and complication rate indicates that admission criteria are appropriate and treatment is as safe as hospital inpatient-based treatment.
One of the limitations of this study is the small sample size and short recruitment period. However, the patients were identified on a defined schedule, limiting selection bias. A larger study will allow a more detailed review of the clinical characteristics and therapeutic regimens of patients treated in HITH and in the hospital. A randomized control study will be able to provide stronger evidence if out of hospital treatment is preferable to in hospital treatment for cellulitis.
In Australia, hospital admissions have increased at twice the rate of population growth.27 Out of hospital programs that attempt to address this demand are now established in many centers in Australia. Maximizing the use of these programs requires identification of factors associated with hospital admission so that strategies to address them can be developed. The rate of uptake of patients with cellulitis for HITH potentially may be increased further, with increased capacity to address the limiting factors identified affecting uptake to HITH and advances in technology particularly that of improved tele-monitoring.
Conclusion
Approximately half of the patients who required intravenous therapy were treated via an out of hospital program. Patients admitted to hospital had more comorbidities and severe illness, and were more likely to suffer complications. The presence of comorbid illness however does not necessarily exclude participation in HITH and appropriately selected patients had few complications.
Highlights
Around half of the hospitalized patients with cellulitis can be managed via Hospital in the Home (HITH).
Severity of cellulitis and comorbidity define the need for the hospital admission.
Presence of comorbidity and active illness do not exclude participation in HITH.
Appropriately selected patients treated in HITH have fewer complications.
Holistic assessment and careful selection are essential for safe treatment in HITH.
Ethical Considerations
Approval by the South-Western Sydney Local Health District (SWSLHD) Ethics Committee (HREC reference: LNR/14/LPOOL/174). All participants provided informed consent.
Acknowledgment
We would like to thank Tracey McDonald, our Research & Electronic Services Librarian for her assistance in the preparation of this manuscript.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Dr Clarence Yeong reports grants from Boehringer Ingelheim Pty Ltd, outside the submitted work. The authors declare no other conflicts of interest in this work.
References
1. Chapman ALN, Patel S, Horner C, Gilchrist M, Seaton RA. Outpatient parenteral antimicrobial therapy: updated recommendations from the UK. J Antimicrob Chemother. 2019;74(11):3125–3127. Accessed April 6, 2019. doi:10.1093/jac/dkz343
2. Donald M, Marlow N, Swinburn E, Wu M. Emergency department management of home intravenous antibiotic therapy for cellulitis. Am J Emerg Med. 2005;22(10):715–717. Accessed April 6, 2019. doi:10.1136/emj.2004.018143
3. Leder K, Turnidge JD, Grayson ML. Home-based treatment of cellulitis with twice-daily cefazolin. Med J Aust. 1998;169(10):519–522. Accessed April 6, 2019. doi:10.5694/j.1326-5377.1998.tb123398.x
4. Corwin P, Toop L, McGeoch G, et al. Randomised controlled trial of intravenous antibiotic treatment for cellulitis at home compared with hospital. BMJ (Clin Res Ed). 2005;330(7483):129. Accessed April 6, 2019. doi:10.1136/bmj.38309.447975.EB
5. Dalovisio JR, Juneau J, Baumgarten K, Kateiva J. Financial impact of a home intravenous antibiotic program on a medicare managed care program. Clin Infect Dis. 2000;30(4):639–642. Accessed April 6, 2019. doi:10.1086/313755
6. Chapman AL, Dixon S, Andrews D, Lillie PJ, Bazaz R, Patchett JD. Clinical efficacy and cost-effectiveness of outpatient parenteral antibiotic therapy (OPAT): a UK perspective. J Antimicrob Chemother. 2009;64(6):1316–1324. Accessed April 6, 2019. doi:10.1093/jac/dkp343
7. Leff B, Burton L, Mader SL, et al. Hospital at home: feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann Intern Med. 2005;143(11):798–808. Accessed April 6, 2019. doi:10.7326/0003-4819-143-11-200512060-00008
8. Caplan GA, Ward JA, Brennan NJ, Coconis J, Board N, Brown A. Hospital in the home: a randomised controlled trial. Med J Aust. 1999;170(4):156–160. Accessed April 6, 2019. doi:10.5694/j.1326-5377.1999.tb127711.x
9. Leff B, Burton L, Mader SL, et al. Comparison of functional outcomes associated with hospital at home care and traditional acute hospital care. J Am Geriatr Soc. 2009;57(2):273–278. Accessed April 6, 2019. doi:10.1111/j.1532-5415.2008.02103.x
10. Shepperd S, Doll H, Angus RM, et al. Avoiding hospital admission through provision of hospital care at home: a systematic review and meta-analysis of individual patient data. C Cmaj. 2009;180(2):175–182. Accessed April 6, 2019. doi:10.1503/cmaj.081491
11. National Health Performance Authority. Healthy Communities: Potentially Preventable Hospitalisations in 2013–14. Sydney, AU: National Health Performance Authority; 2015.
12. Amin AN, Cerceo EA, Deitelzweig SB, Pile JC, Rosenberg DJ, Sherman BM. Hospitalist perspective on the treatment of skin and soft tissue infections. Mayo Clin Proc. 2014;89(10):1436–1451. Accessed April 6, 2019. doi:10.1016/j.mayocp.2014.04.018
13. Seaton RA, Sharp E, Bezlyak V, Weir CJ. Factors associated with outcome and duration of therapy in outpatient parenteral antibiotic therapy (OPAT) patients with skin and soft-tissue infections. Int J Antimicrob Agents. 2011;38(3):243–248. Accessed April 6, 2019. doi:10.1016/j.ijantimicag.2011.05.008
14. Grayson ML, McDonald M, Gibson K, et al. Once-daily intravenous cefazolin plus oral probenecid is equivalent to once-daily intravenous ceftriaxone plus oral placebo for the treatment of moderate-to-severe cellulitis in adults. Clin Infect Dis. 2002;34(11):1440–1448. Accessed April 6, 2019. doi:10.1086/340056
15. Raff AB, Kroshinsky D. Cellulitis: A Review. JAMA. 2016;316(3):325–337. Accessed April 6, 2019. doi:10.1001/jama.2016.8825
16. Garg A, Lavian J, Lin G, Sison C, Oppenheim M, Koo B. Clinical characteristics associated with days to discharge among patients admitted with a primary diagnosis of lower limb cellulitis. J Am Acad Dermatol. 2017;76(4):626–631. Accessed April 6, 2019. doi:10.1016/j.jaad.2016.11.063
17. Halilovic J, Heintz BH, Brown J. Risk factors for clinical failure in patients hospitalized with cellulitis and cutaneous abscess. J Infect. 2012;65(2):128–134. Accessed April 6, 2019. doi:10.1016/j.jinf.2012.03.013
18. Figtree M, Konecny P, Jennings Z, Goh C, Krilis SA, Miyakis S. Risk stratification and outcome of cellulitis admitted to hospital. J Infect. 2010;60(6):431–439. Accessed April 6, 2019. doi:10.1016/j.jinf.2010.03.014
19. Menzin J, Marton JP, Meyers JL, Carson RT, Rothermel CD, Friedman M. Inpatient treatment patterns, outcomes, and costs of skin and skin structure infections because of Staphylococcus aureus. Am J Infect Control. 2010;38(1):44–49. Accessed April 6, 2019. doi:10.1016/j.ajic.2009.04.287
20. Eron LJ, Lipsky BA, Low DE, Nathwani D, Tice AD, Volturo GA. Managing skin and soft tissue infections: expert panel recommendations on key decision points. J Antimicrob Chemother. 2003;52(Suppl 1):i3–17. Accessed April 6, 2019. doi:10.1093/jac/dkg466
21. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. Accessed April 6, 2019. doi:10.1016/0021-9681(87)90171-8
22. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–c84. Accessed April 6, 2019. doi:10.1159/000339789
23. Fimognari FL, Pierantozzi A, De Alfieri W, et al. The severity of acute illness and functional trajectories in hospitalized older medical patients. J Gerontol A Biol Sci Med Sci. 2017;72(1):102–108. Accessed April 6, 2019. doi:10.1093/gerona/glw096
24. Kameshwar K, Karahalios A, Janus E, Karunajeewa H. False economies in home-based parenteral antibiotic treatment: a health-economic case study of management of lower-limb cellulitis in Australia. J Antimicrob Chemother. 2015;71(3):830–835. Accessed April 6, 2019. doi:10.1093/jac/dkv413
25. Gunderson CG, Cherry BM, Fisher A. Do patients with cellulitis need to be hospitalized? A systematic review and meta-analysis of mortality rates of inpatients with cellulitis. J Gen Intern Med. 2018;33(9):1553–1560. Accessed April 6, 2019. doi:10.1007/s11606-018-4546-z
26. Caplan GA, Sulaiman NS, Mangin DA, Aimonino Ricauda N, Wilson AD, Barclay L. A meta-analysis of “hospital in the home”. Med J Aust. 2012;197(9):512–519. Accessed April 6, 2019. doi:10.5694/mja12.10480
27. Australia Institute of Health and Welfare. Australia’s Health 2018. Canberra, ACT: AIHW; 2018.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.