")
Back to Journals » Patient Preference and Adherence » Volume 14
Ospemifene in the Management of Vulvar and Vaginal Atrophy: Focus on the Assessment of Patient Acceptability and Ease of Use
Authors Cagnacci A , Xholli A, Venier M
Received 1 October 2019
Accepted for publication 28 December 2019
Published 10 January 2020 Volume 2020:14 Pages 55—62
DOI https://doi.org/10.2147/PPA.S203614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Angelo Cagnacci, 1 Anjeza Xholli, 2 Martina Venier 2
1Obstetrics and Gynaecology Unit, Obstetrics and Gynaecology University of Genova, Genova, Italy; 2Obstetrics and Gynaecology Unit, Azienda Sanitaria Universitaria Integrata di Udine, Udine, Italy
Correspondence: Angelo Cagnacci
Ginecologia e Ostetricia, Policlinico San Martino, Via Largo Benzi 10, Genova 16132, Italy
Email [email protected]
Abstract: Endocrinological changes that occur with menopause lead to a chronic and progressive condition named vulvar and vaginal atrophy (VVA). This disease is characterized by symptoms such as dryness, dyspareunia, itching, burning, and dysuria. According to recent epidemiological studies, VVA has a high prevalence and can also occur in younger women prior to the menopause, negatively affecting quality of life, sexual function, intimacy and relationship with the partner. Accordingly, therapy should be effective, initiated early and continued for as long as possible. Up to recent years, available therapeutic options have included over-the-counter lubricants and moisturizers, vaginal oestrogens and systemic hormones. These products are not indicated for all women. Hormones are mostly contraindicated in women with a history of hormone-sensitive cancer and are frequently not accepted even by women without contraindications. Local therapies are frequently considered uncomfortable, difficult to apply, and messy. Indeed, these treatments have a high spontaneous discontinuation rate, mostly due to dissatisfaction, safety concern, side effects and difficulty in vaginal placement. Recently, ospemifene, a new non-hormonal systemic remedy, was approved by FDA (Food and Drug Administration) and EMA (European Medicines Agency) for the treatment of the two most bothersome symptoms of VVA: dryness and dyspareunia. Because ospemifene is a selective estrogen receptor modulator (SERM), it can be administered also in women with a history of breast cancer, and this makes it more acceptable by any woman. In addition, its route of administration minimizes those bothersome side effects intrinsic to the vaginal route of administration. Available data indicate that women using ospemifene have higher adherence to treatment, higher persistence and lower discontinuation rate. Satisfaction is higher than with other local therapies and overall health care cost is lower.
Keywords: ospemifene, vaginal estrogens, vulvar atrophy, vaginal atrophy, acceptability
Introduction
Vulvar and vaginal atrophy (VVA) is a chronic and progressive disease characterized by anatomical-functional alterations caused by aging and hypoestrogenism.1
Since 2014, VVA is considered part of the genitourinary syndrome of menopause (GSM).1 Anatomical changes of VVA (i.e. thinning of vaginal rugae, mucosal dryness, pallor, fragility, and the presence of petechiae)2 develop gradually during years and do not resolve spontaneously. Hypoestrogenism leads to an atrophy of the vaginal, vulvar, urethral and bladder epithelium. Consequently, the vaginal maturation index (VMI), i.e. the ratio among three different vaginal epithelial cell types, parabasal, intermediate, and superficial, changes towards a predominance of parabasal cells. Glycogen production decreases, vaginal microbiota changes, vaginal pH increases above 4.5, and risk of vaginal infection increases.3,4 Related symptoms are dryness, dyspareunia, itching, burning, and dysuria.
In European countries, prevalence of postmenopausal VVA is around 80%.5,6 Noteworthy, 65% of women experience VVA within one year since menopause. Symptoms and signs of VVA occur also in younger women, prior to the menopause. An Italian study,7 performed in a cohort of women aged between 40 and 55 years observed a prevalence of VVA and of vaginal dryness of 36.8% and of 64%, respectively.
Vaginal dryness and dyspareunia are the most bothersome symptoms of VVA.8,9 These symptoms can affect sexuality, intimacy, overall pleasure, sexual satisfaction, relationship with a partner, the seeking of a new relationship and, ultimately, emotional health and woman’s quality of life.10–13
Diagnosis of VVA can be simple: the criteria of a large multicentric Italian study (AGATA study) indicate that the concomitance of a pH>5, sensation of vaginal dryness and an objective index at the examination (thinning of vaginal rugae, mucosal dryness, pallor, fragility, and the petechiae), is enough to make diagnosis. Anyway, diagnosis can be even easier because, as shown in epidemiological studies, all postmenopausal women with VVA suffer from vaginal dryness and dryness alone, without VVA, is present only in a small percentage of cases ranging from 3 to 10%.4,6 Thus, the only presence of vaginal dryness can be sufficient for the diagnosis of postmenopausal VVA. Vaginal dryness is also the most bothersome symptom and its presence is sufficient to start a therapy.
Therapeutic options include local and systemic hormonal and non-hormonal products, ranging from over-the-counter lubricant and moisturizers to medications such as vaginal oestrogens (cream, tablets and ring), systemic hormones and the innovative oral selective estrogen receptor modulator (SERM): ospemifene.14,15
Therapeutic Options
First-line therapies for women with symptomatic VVA include intercourse that can be associated with non-hormonal lubricants and regular use of long-acting vaginal moisturizers or vaginal estrogen.14,16 Therapy should be started early, before irreversible atrophic changes have occurred, and should be continued for as long as possible.17 Systemic hormones are an effective therapy, but they are recommended only to eligible women that beyond VVA suffer from menopausal complaints (e.g. vasomotor symptoms).3,17
Over-the-counter vaginal lubricants and moisturizers are often prescribed as a first-line treatment and are indicated in women with a previous history of hormone-dependent cancers. Unfortunately, they may provide only a transient benefit of vaginal symptoms in comparison to local oestrogens.18 Vaginal lubricants are intended to be used to relieve friction and dyspareunia and are applied to the vaginal introitus before sexual intercourse. Water-based lubricants are the most common, probably because of their wide availability and low price. Unlike oil or silicone lubricants, they do not stain sheets or lingerie. According to a recent review,19 water-based lubricants should have an acidic pH (pH 3.8–4.5) and an osmolarity below 380 mOsm/kg. This is to preserve the vaginal microenvironment and to reduce cytopathic or irritating effects on the vaginal mucosa. Lubricants based on silicone are not absorbed by vaginal mucosa; therefore, they persist longer. A recent study reported that during sexual intercourse, silicone-based lubricants might reduce total sexual discomfort more effectively than water-based products.20
Vaginal moisturizers, rather than lubricants, are locally absorbed by superficial layers, rehydrate dry mucosal tissue and have a long-term action. Specifically, the beneficial effects of vaginal moisturizers are mostly due to adhesive and buffering capacities leading to tissue water retention and vaginal pH reduction.21 Polycarbophil based moisturizers are as effective as vaginal oestrogen therapy in reducing postmenopausal VVA symptoms22,23 but not in improving sexual function and menopause-related quality of life.24
Low dose local oestrogens, in the form of cream, tablet, or ring are all effective for VVA symptoms, with a minimal systemic absorption. Thus, vaginal oestrogen products seem to be safe with only a few adverse effects.25 A review including 44 published studies did not report any case of either thromboembolism or breast cancer. Nevertheless, data on long-term efficacy, risks, and tolerability are limited because most reported studies have a follow-up period of only 12 weeks.26
Adherence to Local Treatments
Epidemiological studies have shown that most women discontinue vaginal therapy. The reason for discontinuation is that they are uncomfortable, difficult to apply, and annoying.9,13 In addition, many women claim a non-sufficient therapeutic efficacy, either for an excessive expectation or an inadequate dose-regimen.9 Indeed, the different types of vaginal treatments are prescribed without a clear rationale, a clear dose and scheme, and a clear indication on duration. This situation is further prompted by the absence of clear guidelines on therapeutic cycles, dosages and duration.9 According to a study published in 2013, many women treated with vaginal oestrogens reported missing doses at least once a month, often because of messiness when filling and inserting the applicator, general unpleasantness of the cream, the need to wash the applicator and leakage of the cream following application.27
Ospemifene an Innovative Option
Recently, ospemifene, a new non-hormonal drug, was approved for the treatment of VVA symptoms. Ospemifene is a third-generation selective estrogen receptor modulator (SERM), that is administered orally at the dose of 60 mg daily. It was initially approved by the FDA28 and endorsed by the North American Menopause Society15 for the treatment of moderate and severe dyspareunia associated with VVA. Following the recent publication of a new clinical trial,29 ospemifene has been approved also for the treatment of moderate to severe vaginal dryness. In Europe, the European Medicines Agency (EMA) has approved ospemifene for the treatment of all VVA symptoms, from moderate to severe. Ospemifene is targeted for acting, as an agonist, in the vulva and vagina, without exerting major side effects in other organs. Through oestrogen receptors stimulation, ospemifene promotes proliferation of the vaginal mucosa epithelial lining.30 Ki-67 immunoreactivity, an index of cell proliferation, increases enormously in the basal layers of the mucosa, sampled both in the upper and the lower third of the vagina.30 The effect is noticeable also on vaginal collagen. Administration of ospemifene increases total collagen both in vaginal mucosa and vestibule. The preferential augmentation of type I rather than type III collagen, increases strength and resistance of vaginal tissue.31 Efficacy and safety of ospemifene was established in randomized, placebo-controlled, Phase II/III studies.32–35 After only four weeks, administration of ospemifene increases superficial cells and decreases parabasal cells and vaginal pH. Concomitantly, VVA symptoms and sexuality improve.29,32–35 Data on tolerability are confirmed by a recent post-hoc analysis documenting a low drop-out rate (7.6% with ospemifene and 3.8% with placebo).36
At the vulva and vaginal vestibule, ospemifene reduces painful transmission of C-type nerve fibres that convey painful stimuli37 and exerts trophic effects. Administration of ospemifene for 20 weeks reduces urethral meatus and anterior vaginal wall prominence, stenosis of the introitus, vestibular pallor and erythema and ameliorates vulvar moisture.38 Modifications are associated with improvement of cotton-tipped swab testing and sexual function.37 Pain at intercourse decreases, while desire and arousal increase.39,40
Ospemifene vs Vaginal Oestrogens: Safety
VVA is a chronic and progressive disease and it would require long-term therapy. Unfortunately, adherence to treatment is weak and many women discontinue vaginal therapy for perceived inefficacy, inconvenient administration or perceived risk.
Several studies focused on safety, specifically on the endometrium, breast and coagulation. There is no direct comparison between ospemifene and vaginal oestrogens, but, from the analysis of the literature, a historical indirect comparison can be tentatively performed (Table 1). Endometrial safety of the two treatments appears to be comparable with no evidence of an increased risk of cancer. Simon et al41 described one event of endometrial carcinoma and one case of complex hyperplasia without atypia in postmenopausal women treated for 52-weeks with an ultra-low-dose (10-microgram) of 17β-oestradiol in vaginal tablets. In a multicentre randomized, double-blind Phase 3 study, one case of simple hyperplasia without atypia and no case of endometrial carcinoma was diagnosed three months after the last administration of a 12-week ospemifene treatment.35 Long-term studies, up to 52 weeks of administration, show no effect of ospemifene on the endometrium.33,42
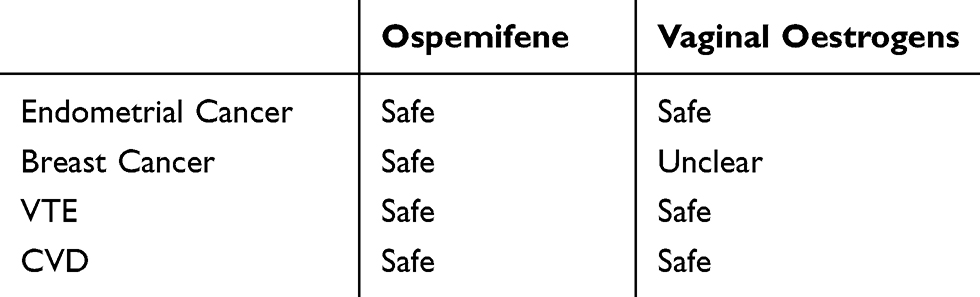 |
Table 1 Safety of Ospemifene and Vaginal Oestrogens on the Risk of Hormone-Dependent Cancer, Venous Thrombosis (VTE) or Cardiovascular Disease (CVD). Summary of the Literature |
Oestrogens administered into the vagina are partially absorbed, slightly increasing systemic exposure. For this reason, they are considered potentially harmful for breast cancer, although there is no evidence of an increased rate of breast cancer during or after their administration.43
In vitro, ospemifene exerts anti-oestrogenic effects in the ER+ MCF-7 breast cancer cells by inhibiting, in a dose-dependent manner, the oestrogen-regulated gene expression of pS2.44 The same findings are observed in ovariectomized mice in vivo, where ospemifene reduces growth of MCF-7 cancer cells. In comparison to control, administration of ospemifene inhibits MCF-7 tumour growth, with a difference in volume that become significant after only 3 weeks of treatment.44 Similar data are shown in another study after only 4 weeks of ospemifene administration.45
In vitro and in animals’ results were replicated on breast tissue, collected from 26 healthy postmenopausal women undergoing reductive mammoplasty. In this model, ospemifene significantly inhibits oestrogen-induced cell proliferation.46 Clinical data are also reassuring.
Safety of ospemifene on breast was evaluated in a post- hoc analysis of six Phase 2 and 3 clinical trials.36 A total of 2200 postmenopausal women were randomized either to ospemifene or placebo for a median duration of treatment of 86 and 84 days, respectively. Breast safety was evaluated by both mammography, performed prior to treatment and after 12 months, and breast palpations performed prior to treatment, at 12 weeks, six months, and 12 months. No case of breast cancer was observed. Prevalence of adverse events such as breast tension (0.9% vs 0.6% for placebo), pain (0.6% vs 0.3%), and breast thickening (0.6% vs 0.4%), were similar in the ospemifene and placebo group (2.5% vs 2.2% for placebo).36 Breast density was not assessed. However, no other abnormal clinically significant mammogram findings were reported, and the prevalence of abnormal not clinically significant findings was similar between ospemifene and placebo.36 Based on these preclinical and clinical data, ospemifene is the only VVA therapy that stimulates oestrogen receptors at the vagina, that can be prescribed to women with a history of breast cancer, after the termination of adjuvant treatment.47
Systemic estrogens48 and SERMS, such as raloxifene or tamoxifen,49–51 increase the risk of venous thromboembolism (VTE). VTE is not increased by vaginal estrogens.43 Also ospemifene does not increase the risk of VTE. In a post-hoc analysis of 6 Phase II and Phase III studies the incidence of cardiovascular events (i.e. specifically deep vein thrombosis, cerebrovascular accidents, and cerebral haemorrhages) was shown to be very low, both in the ospemifene (0.3%) and placebo (0.1%) group.36 In this latter analysis, only two high-risk patients reported VTE during ospemifene, with no case of pulmonary embolism or retinal vein thrombosis. A recent post hoc analysis of five placebo-controlled clinical studies showed that, in comparison to placebo, ospemifene, up to 12 months of use, decreases fibrinogen, a known risk factor for coronary artery disease and VTE and, similarly to oral oestrogens,52 it increases HDL and reduces LDL.53 Differently from oral estrogens,52 ospemifene does not increase triglycerides.53 In a post-marketing observational analysis of the 2-year interim data of the Post Authorisation Safety Study (PASS), the incidence of VTE in the group of women receiving ospemifene (0.12%) is lower than that of women receiving other SERMS for non-neoplastic reasons (0.64%), or of women with AVV not receiving any treatment (1.23%).54 No increased risk of cardiovascular diseases, breast tumours, endometrial hyperplasia, or gynaecological pathologies of any kind is also observed.54
Ospemifene vs Vaginal Oestrogens: Side Effects
Adverse events were reported for both types of treatment, including hot flushes, vaginal discharge, muscle spasms, and headache (Table 2). Among women treated with ospemifene, hot flushes were the most reported adverse event (7.5% vs 2.6% for placebo) and, although low, the most common reason for discontinuation (1.0%).36 Frequency and intensity of hot flushes was higher during the first four weeks of treatment and decreased subsequently with continuous use.55 These symptoms were observed also with vaginal oestradiol, but with an incidence below 1%.56
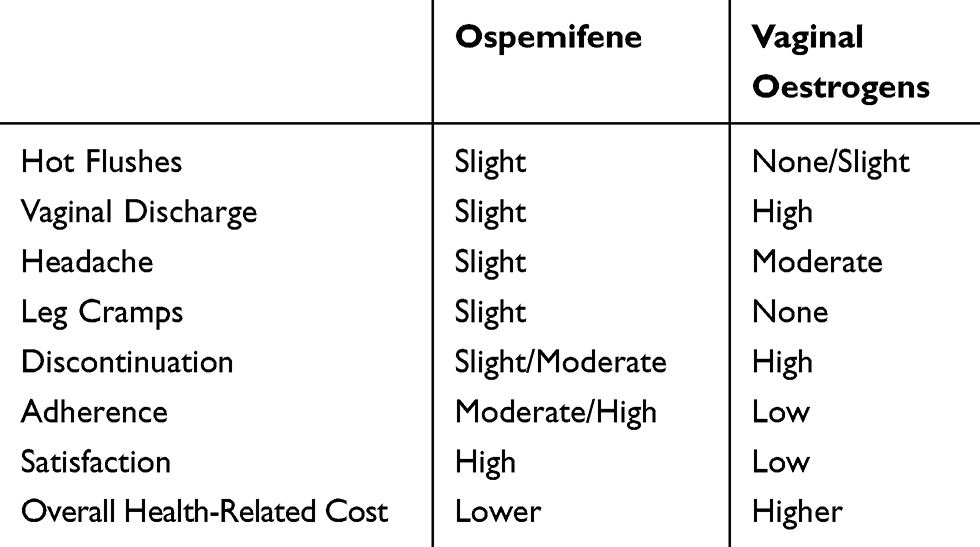 |
Table 2 Risk of Side Effects, Discontinuation Rate, Adherence to, Satisfaction with and Overall Related Cost of Treatment with Ospemifene or Vaginal Oestrogens. Summary of the Literature |
Vaginal discharge or discomfort were reported in up to 10% of patients treated with vaginal estradiol.43,56 Simon et al reported that one of the most common treatment-related adverse events during ospemifene was vaginal discharge (3.8% vs 0.3% for placebo) but this led to treatment discontinuation only in 0.5% of patients.36
As noted with other SERMs, muscle spasms are commonly reported from women using ospemifene (3.2% vs 0.9%)36 and are generally described as mild or moderate leg cramps. This side effect was never reported with local estrogen.43 Headache was reported with the same frequency during placebo or ospemifene (2.4% vs 2.4%)36 whereas its incidence tended to be higher ranging from 1 to 10% during the use of vaginal estrogens.43,56
Therefore, ospemifene and local oestrogens appear to have a similar tolerability, but acceptability, adherence to treatment and discontinuation may differ as the consequence of the different pharmaceutical formulation and route of administration (Table 2).
Ospemifene vs Vaginal Oestrogens: Adherence to Treatment and Satisfaction
One study evaluating adherence to treatment with vaginal oestrogens reported that users of these formulations miss a dose at least once a month, often because of messiness, general unpleasantness of the cream, the need to wash the applicator and leakage of the cream following application.27 Adherence to treatment, i.e. the number of days covered by therapy out of the number of total days considered, was recently evaluated in a 12-months study, comparing ospemifene and vaginal oestrogens. The study was performed in 86,946 patients with more than one pharmacy claim for dyspareunia-related medication.57 Highest adherence was observed for ospemifene in comparison to non-ring local hormonal therapy e.g. conjugated oestrogen cream, oestradiol vaginal insert, and oestradiol cream (40% vs 21%; p<0.0001). Only the ring showed a higher adherence to treatment (52%). Persistence (ie appropriate time of drug refill) was also higher for ospemifene than vaginal creams (23% vs 4–16% of vaginal cream; p<0.0001). The ring had the highest treatment (44%) persistence. Discontinuation rate of ospemifene was 77.1%, and it was significantly lower (P<0.0001) than that of oestradiol vaginal insert (83.6%), conjugated oestrogen cream (95.0%), and oestradiol cream (93.7%). The vaginal ring had the lowest discontinuation rate (56.4%). On these bases ospemifene can be considered superior to vaginal oestrogens but not to the vaginal ring, in terms of adherence, persistence and treatment continuation. However, the ring does not have the indication to the treatment of dyspareunia, that ospemifene has.58 Furthermore, health-care cost, that take into consideration the cost of the product and of medical consultations over a period of 12 months, are higher for the ring, and vaginal oestrogens, than for ospemifene. The cost of ospemifene is higher than that of local hormonal therapies, but medical consultations are less for women on ospemifene than other therapies. This indirectly supports a higher efficacy and tolerability of ospemifene vs any type of vaginal treatment, probably consequent also to a greater adherence and persistence to treatment.
Finally, when using the ring, women are concerned about inserting or removing it, about vaginal infections, hygiene and cleanliness, about the oestrogen dose administered, and about feeling it.27 A recent survey evaluated woman’s perceptions of VVA and its therapeutic options.59 Symptomatic women above 45 years of age were invited to complete a survey containing 63 questions related to VVA symptoms, menopausal status, therapeutic options, way of prescription, efficacy, and acceptability. Among 1858 women that completed the survey, 7% were “current users” of a pharmaceutical therapy for VVA (including vaginal oestrogen or oral SERMS), 18% were “former users” of that therapy, 25% were current or former users of over-the-counter (OTC) products like vaginal lubricants or moisturizers, and 50% had never used any therapy (“never users”). Most recommended treatment in current or former users was vaginal oestrogen and oral hormones, but, among those who had never used any treatment, 35% stated that nothing would convince them to use hormones. Fear of using hormones and discomfort with the application make local hormonal treatments hardly accepted by women.59 Fear of systemic absorption and inconvenient administration of local creams, reduced adherence to treatment. Only few women (33-42%) used more than once per week vaginal oestrogens that were prescribed “continuously”, and 75% of women used moisturizers and lubricants “as needed”, instead of few times per week. The highest adherence to treatment was observed in women receiving the daily dose of ospemifene (59%). Satisfaction was also highest with ospemifene, reaching 67% of users. Satisfaction with lubricants and moisturizers used “as needed” was only 15% and that with vaginal oestrogens for creams, tablets or the ring ranged between 33-35%.59
In conclusion, women’s adherence, persistence and satisfaction with long-term treatment is higher for ospemifene than for other products.59 Likely, this is the consequence of a combination of effectiveness and ease of use. Unlike other local therapies, ospemifene does not need any scheme of treatment, just taking a pill per day. Adherence to treatment is favoured by the oral administration of a non-hormonal drug that avoids the inconvenience of the local application of therapies and the fear of hormones.59,60
Conclusion
Ospemifene is the first oral treatment for VVA that provides an alternative treatment for patients unsuitable for vaginal products or for oestrogen. Its clinical characteristics give the opportunity to propose long-term therapies for VVA that have the possibility to be followed. Ospemifene not only enlarge the number of women that can be treated for VVA, but also increases adherence and persistence to treatment.
Accordingly, in the field of the VVA therapy, ospemifene represents an innovative evolution, that can help to reduce the burden of symptoms and the consequences of postmenopausal VVA.
Disclosure
Angelo Cagnacci report personal fees from Shionogi, personal fees from Italfarmaco/Effik (vaginal estriol), outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Portman DJ, Gass ML. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and The North American Menopause Society. Menopause. 2014;21(10):1063–1068. doi:10.1097/GME.0000000000000329
2. Cagnacci A, Carbone MM, Palma P. Prevalence and association between objective signs and subjective symptoms of vaginal atrophy: the AGATA study. Menopause. 2016;23(10):1139–1145. doi:10.1097/GME.0000000000000675
3. Mac Bride MB, Rhodes DJ, Shuster LT. Vulvovaginal atrophy. Mayo Clin Proc. 2010;85(1):87–94. doi:10.4065/mcp.2009.0413
4. Palma F, Della Vecchia E, Cagnacci A, Writing Group of the AGATA study. Medical and patient attitude towards vaginal atrophy: the AGATA study. Climacteric. 2016;19(6):553–557. doi:10.1080/13697137.2016.1240770
5. Palma F, Volpe A, Villa P, Cagnacci A; writing group of the AGATA study. Vaginal atrophy of women in postmenopause: results from a multicentric observational study: the AGATA study. Maturitas. 2016;83:40–44. doi:10.1016/j.maturitas.2015.09.001
6. Nappi RE, Seracchioli R, Salvatore S, Cagnacci A, Di Paolantonio T, Busacca M; investigators of the EVES Study. Impact of vulvovaginal atrophy of menopause: prevalence and symptoms in Italian women according to the EVES study. Gynecol Endocrinol. 2019;31(1):1–7.
7. Cagnacci A, Xholli A, Sclauzero M, Venier M, Palma F, Gambacciani M, writing group of the ANGEL study. Vaginal atrophy across the menopausal age: results from the ANGEL study. Climacteric. 2019;22(1):85–89. doi:10.1080/13697137.2018.1529748
8. Palma F, Xholli A, Cagnacci A; as the writing group of the AGATA study. The most bothersome symptom of vaginal atrophy: evidence from the observational AGATA study. Maturitas. 2018;108:18–23. doi:10.1016/j.maturitas.2017.11.007
9. Palma F, Xholli A, Cagnacci A, as the writing group of the AGATA study. Management of vaginal atrophy: a real mess. Results from the AGATA study. Gynecol Endocrinol. 2017;33(9):702–707. doi:10.1080/09513590.2017.1309018
10. Nappi RE, Kingsberg S, Maamari R, Simon J. The CLOSER (CLarifying Vaginal Atrophy’s Impact On SEx and Relationships) survey: implications of vaginal discomfort in postmenopausal women and in male partners. J Sex Med. 2013;10(9):2232–2241. doi:10.1111/jsm.12235
11. Nappi RE, Palacios S. Impact of vulvovaginal atrophy on sexual health and quality of life at postmenopause. Climacteric. 2014;17(1):3–9. doi:10.3109/13697137.2013.871696
12. Nappi RE, Biglia N, Cagnacci A, Di Carlo C, Luisi S, Paoletti AM. Management diagnosis and management of symptoms associated with vulvovaginal atrophy: expert opinion on behalf of the Italian VVA study group. Gynecol Endocrinol. 2016;32(8):602–606. doi:10.1080/09513590.2016.1183627
13. Kingsberg SA, Wysocki S, Magnus L, Krychman ML. Vulvar and vaginal atrophy in postmenopausal women: findings from the REVIVE (REal Women’s VIews of Treatment Options for Menopausal Vaginal ChangEs) survey. J Sex Med. 2013;10(7):1790–1799. doi:10.1111/jsm.12190
14. The North American Menopause Society. Management of symptomatic vulvovaginal atrophy: 2013 position statement of The North American Menopause Society. Menopause. 2013;20(9):888–902. doi:10.1097/GME.0b013e3182a122c2
15. Pinkerton JAV, Aguirre FS, Blake J, et al. The 2017 hormone therapy position statement of The North American Menopause Society. Menopause. 2017;24(7):728–753. doi:10.1097/GME.0000000000000921
16. Sarri G, Davies M, Lumsden MA, Guideline Development Group. Diagnosis and management of menopause: summary of NICE guidance. BMJ. 2015;12(351):h5746. doi:10.1136/bmj.h5746
17. Sturdee DW, Panay N, International Menopause Society Writing Group. Recommendations for the management of postmenopausal vaginal atrophy. Climacteric. 2010;13(6):509–522. doi:10.3109/13697137.2010.522875
18. Biglia N, Peano E, Sgandurra P, et al. Low-dose vaginal oestrogens or vaginal moisturizer in breast cancer survivors with urogenital atrophy: a preliminary study. Gynecol Endocrinol. 2010;26(6):404–412. doi:10.3109/09513591003632258
19. Edwards D, Panay N. Treating vulvovaginal atrophy/genitourinary syndrome of menopause: how important is vaginal lubricant and moisturizer composition? Climacteric. 2016;19(2):151–161. doi:10.3109/13697137.2015.1124259
20. Hickey M, Marino JL, Braat S, Wong S. A randomized, double-blind, crossover trial comparing a silicone- versus water-based lubricant for sexual discomfort after breast cancer. Breast Cancer Res Treat. 2016;158(1):79–90. doi:10.1007/s10549-016-3865-1
21. Willhite LA, O’Connell MB. Urogenital atrophy: prevention and treatment. Pharmacotherapy. 2001;21(4):464–480. doi:10.1592/phco.2001.21.issue-4
22. Mitchell CM, Reed SD, Diem S, et al. Efficacy of vaginal estradiol or vaginal moisturizer vs placebo for treating postmenopausal vulvovaginal symptoms a randomized clinical trial. JAMA Intern Med. 2018;178(5):681–690. doi:10.1001/jamainternmed.2018.0116
23. Bygdeman M, Swahn ML. Replens versus dienoestrol cream in the symptomatic treatment of vaginal atrophy in postmenopausal women. Maturitas. 1996;23(3):259–263. doi:10.1016/0378-5122(95)00955-8
24. Diem SJ, Guthrie KA, Mitchell CM, et al. Effects of vaginal oestradiol tablets and moisturizer on menopause-specific quality of life and mood in healthy postmenopausal women with vaginal symptoms: a randomized clinical trial. Menopause. 2018;25(10):1086–1093. doi:10.1097/GME.0000000000001131
25. Biehl C, Plotsker O, Mirkin S. A systematic review of the efficacy and safety of vaginal estrogen products for the treatment of genitourinary syndrome of menopause. Menopause. 2019;26(4):431–453. doi:10.1097/GME.0000000000001221
26. Rahn DD, Carberry C, Sanses TV, et al; Society of Gynecologic Surgeons Systematic Review Group. Vaginal estrogen for genitourinary syndrome of menopause: a systematic review. Obstet Gynecol. 2014;124(6):1147–1156. doi:10.1097/AOG.0000000000000526
27. Minkin MJ, Maamari R, Reiter S. Improved compliance and patient satisfaction with estradiol vaginal tablets in postmenopausal women previously treated with another local estrogen therapy. Int J Womens Health. 2013;5:133–139. doi:10.2147/IJWH.S41897
28. FDA. Osphena. Highlights of Prescribing Information 2013. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/203505s015lbl.pdf.
29. Archer DF, Goldstein SR, Simon JA, et al. Efficacy and safety of ospemifene in postmenopausal women with moderate-to-severe vaginal dryness: a phase 3, randomized, double-blind, placebo-controlled, multicenter trial. Menopause. 2019;26(6):611–621. doi:10.1097/GME.0000000000001292
30. Alvisi S, Baldassarre M, Martellia V, Gava G, Seracchioli R, Meriggiola MC. Effects of ospemifene on vaginal epithelium of post-menopausal women. Gynecol Endocrinol. 2017;33(12):946–950. doi:10.1080/09513590.2017.1332589
31. Alvisi S, Baldassarre M, Gava G, et al. Structure of epithelial and stromal compartments of vulvar and vaginal tissue from women with vulvo-vaginal atrophy taking ospemifene. J Sex Med. 2018;15(12):1776–1784. doi:10.1016/j.jsxm.2018.10.009
32. Bachmann GA, Komi JO. Ospemifene effectively treats vulvovaginal atrophy in postmenopausal women: results from a pivotal phase 3 study. Menopause. 2010;17(3):480–486. doi:10.1097/gme.0b013e3181c1ac01
33. Goldstein SR, Bachmann GA, Koninckx PR, Lin VH, Portman DJ, Ylikorkala O. Ospemifene 12-month safety and efficacy in postmenopausal women with vulvar and vaginal atrophy. Climacteric. 2014;17(2):173–182. doi:10.3109/13697137.2013.834493
34. Simon JA, Lin VH, Radovich C, Bachmann GA, Ospemifene Study Group. One-year long-term safety extension study of ospemifene for the treatment of vulvar and vaginal atrophy in postmenopausal women with a uterus. Menopause. 2013;20(4):418–427. doi:10.1097/gme.0b013e31826d36ba
35. Portman DJ, Bachmann GA, Simon JA, Ospemifene Study Group. Ospemifene, a novel selective estrogen receptor modulator for treating dyspareunia associated with postmenopausal vulvar and vaginal atrophy. Menopause. 2013;20(6):623–630. doi:10.1097/gme.0b013e318279ba64
36. Simon AJ, Altomare C, Cort S, Jiang W, Pinkerton JV. Overall safety of ospemifene in postmenopausal women from placebo-controllated phase 2 and 3 trials. J Womens Health (Larchmt). 2018;27(1):14–23. doi:10.1089/jwh.2017.6385
37. Murina F, Di Francesco S, Oneda S. Vulvar vestibular effects of ospemifene: a pilot study. Gynecol Endocrinol. 2018;34(7):631–635. doi:10.1080/09513590.2018.1427717
38. Goldstein SW, Winter AG, Goldstein I. Improvements to the vulva, vestibule, urethral meatus, and vagina in women treated with ospemifene for moderate to severe dyspareunia: a prospective vulvoscopic pilot study. Sex Med. 2018;6(2):154–161. doi:10.1016/j.esxm.2018.03.002
39. Constantine G, Graham S, Portman DJ, Rosen RC, Kingsberg SA. Female sexual function improved with ospemifene in postmenopausal women with vulvar and vaginal atrophy: results of a randomized, placebo-controlled trial. Climacteric. 2015;18(2):226–232. doi:10.3109/13697137.2014.954996
40. Schiavi MC, Sciuga V, Giannini A, et al. Overactive bladder syndrome treatment with ospemifene in menopausal patients with vulvovaginal atrophy: improvement of sexuality? Gynecol Endocrinol. 2018;34(8):666–669. doi:10.1080/09513590.2018.1441398
41. Simon J, Nachtigall L, Ulrich LG, Eugster-Hausmann M, Gut R. Endometrial safety of ultra-low-dose estradiol vaginal tablets. Obstet Gynecol. 2010;116(4):876–883. doi:10.1097/AOG.0b013e3181f386bb
42. Simon J, Portman D, Mabey RG
43. Bruyniks N, Biglia N, Palacios S, Mueck A. Systematic indirect comparison of ospemifene versus local estrogens for vulvar and vaginal atrophy. Climacteric. 2017;20(3):195–204. doi:10.1080/13697137.2017.1284780
44. Taras TL, Wurz GT, De Gregorio MW. In vitro and in vivo biologic effects of ospemifene (FC-1271a) in breast cancer. J Steroid Biochem Mol Biol. 2001;77(4–5):271–279. doi:10.1016/S0960-0760(01)00066-8
45. Qu Q, Zheng H, Dahllund J, et al. Selective estrogen effects of a novel triphenylethylene compound, FC1271a, on bone, cholesterol level, and reproductive tissues in intact and ovariectomized rats. Endocrinology. 2000;141(2):809–820. doi:10.1210/endo.141.2.7342
46. Eigeliene N, Kangas L, Hellmer C, Kauko T, Erkkola R, Ha¨rko¨nen P. Effects of ospemifene, a novel selective estrogen-receptor modulator, on human breast tissue ex vivo. Menopause. 2016;23:719–730. doi:10.1097/GME.0000000000000624
47. Senshio (ospemifene) tablets. Summary of Product Characteristics. London, UK: Shionogi Ltd; 2015.
48. Rovinski D, Ramos RB, Fighera TM, Casanova GK, Spritzer PM. Risk of venous thromboembolism events in postmenopausal women using oral versus non-oral hormone therapy: a systematic review and meta-analysis. Thromb Res. 2018;168:83–95. doi:10.1016/j.thromres.2018.06.014
49. Barrett-Connor E, Mosca L, Collins P, Raloxifene Use for The Heart (RUTH) Trial Investigators. Effects of raloxifene on cardiovascular events and breast cancer in postmenopausal women. N Engl J Med. 2006;355(2):125–137. doi:10.1056/NEJMoa062462
50. Cummings SR, Eckert S, Krueger KA, et al. The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. Multiple Outcomes of Raloxifene Evaluation. JAMA. 1999;281:2189–2197. doi:10.1001/jama.281.23.2189
51. Saphner T, Tormey DC, Gray R. Venous and arterial thrombosis in patients who received adjuvant therapy for breast cancer. J Clin Oncol. 1991;9:286–294. doi:10.1200/JCO.1991.9.2.286
52. Nanda S, Gupta N, Mehta HC, Sangwan K. Effect of oestrogen replacement therapy on serum lipid profile. Aust N Z J Obstet Gynaecol. 2003;43(3):213–216. doi:10.1046/j.0004-8666.2003.00068.x
53. Archer DF, Altomare C, Jiang W, Cort S. Ospemifene’s effects on lipids and coagulation factors: A post hoc analysis of phase 2 and 3 clinical trial data. Menopause. 2017;24(10):1167–1174. doi:10.1097/GME.0000000000000900
54. Bruyniks N, De Gregorio F, Gibbs T, Carroll R, Fraeman KH, Nordstrom BL. Safety of ospemifene during real-life use. J Gynecol Wom Health. 2018;9(1):1–14.
55. Costantine G, Archer DF, Pollycove R, Jiang W, Altomare C, Pinkerton J. Ospemifene’s effect on vasomotor symptoms: a post hoc analysis of phase 2 and 3 clinical data. Menopause. 2016;23(9):957–964. doi:10.1097/GME.0000000000000656
56. Vagifem summary of product characteristics. Vagifem 10 micro grams vaginal tablets. January 2015. Available from: https://www.medicines.org.uk/emc/print-document?documentId=23819.
57. Faught BM, Soulban G, Yeaw J, et al. Ospemifene versus local estrogen: adherence and costs in postmenopausal dyspareunia. J Comp Eff Res. 2019;21:1111–1123. [Epub ahead of print].
58. Imvexxy Prescribing Information. 2018. Available from: https://www.imvexxy.com/pi.pdf.
59. Kingsberg SA, Krychman M, Graham S, Bernick B, Mirkin S. The women’s EMPOWER survey: identifying women’s perceptions on vulvar and vaginal atrophy and its treatment. J Sex Med. 2017;14(3):413–424. doi:10.1016/j.jsxm.2017.01.010
60. Nappi RE, Palacios S, Panay N, Particco M, Krychman ML. Vulvar and vaginal atrophy in four European countries: evidence from the European REVIVESurvey. Climacteric. 2016;19(2):188–197. doi:10.3109/13697137.2015.1107039
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.