")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Orexin/hypocretin levels in the cerebrospinal fluid and characteristics of patients with myotonic dystrophy type 1 with excessive daytime sleepiness
Authors Omori Y, Kanbayashi T , Imanishi A, Tsutsui K, Sagawa Y, Kikuchi YS, Takeshima M , Yoshizawa K , Uemura S , Shimizu T
Received 2 December 2017
Accepted for publication 3 January 2018
Published 8 February 2018 Volume 2018:14 Pages 451—457
DOI https://doi.org/10.2147/NDT.S158651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Yuki Omori,1 Takashi Kanbayashi,1,2 Aya Imanishi,1 Ko Tsutsui,1 Yohei Sagawa,1 Yuka S Kikuchi,1 Masahiro Takeshima,1 Kazuhisa Yoshizawa,1 Sachiko Uemura,3 Tetsuo Shimizu1,2
1Department of Neuropsychiatry, Akita University Graduate School of Medicine, Akita, Japan; 2International Institute for Integrative Sleep Medicine (WPI-IIIS), University of Tsukuba, Tsukuba, Japan; 3Department of Physical Therapy, Akita University Graduate School of Health Sciences, Akita, Japan
Purpose: Myotonic dystrophy type 1 (DM1) is often characterized by excessive daytime sleepiness (EDS) and sleep-onset rapid eye movement periods caused by muscleblind-like protein 2. The EDS tends to persist even after treatment of sleep apnea. We measured the cerebrospinal fluid (CSF) orexin levels in DM1 patients with EDS and compared the clinical characteristics with narcolepsy type 1 and idiopathic hypersomnia (IHS) patients.
Patients and methods: We measured the CSF orexin levels in 17 DM1 patients with EDS and evaluated subjective sleepiness using the Epworth Sleepiness Scale (ESS), objective sleepiness using mean sleep latency (MSL), and sleep apnea using apnea-hypopnea index (AHI). We compared the ESS scores and MSL between decreased (≤200 pg/mL) and normal (>200 pg/mL) CSF orexin group in DM1 patients. Furthermore, we compared the CSF orexin levels, ESS scores, MSL, and AHI among patients with DM1, narcolepsy type 1 (n=46), and IHS (n=30).
Results: Seven DM1 patients showed decreased CSF orexin levels. There were significant differences in the ESS scores and MSL between decreased and normal CSF orexin groups in DM1 patients. The ESS scores showed no significant difference among patients with DM1, narcolepsy type 1, and IHS. The MSL in DM1 and IHS patients were significantly higher than narcolepsy type 1 patients (p=0.01, p<0.001). The AHI in DM1 patients was significantly higher than narcolepsy type 1 patients (p=0.042) and was insignificantly different from IHS patients. The CSF orexin levels in DM1 patients were significantly lower than IHS patients and higher than narcolepsy type 1 patients (p<0.001, p<0.001).
Conclusion: The CSF orexin levels of DM1 patients moderately decreased compared to those of IHS patients as the control group. However, the EDS of DM1 patients may not be explained by only orexin deficiency.
Keywords: myotonic dystrophy type 1, orexin, narcolepsy, sleep-onset rapid eye movement periods, muscleblind-like protein
Corrigendum for this paper has been published
Introduction
Myotonic dystrophy type 1 (DM1) is a type of inherited disorder called muscular dystrophies that shows autosomal dominant inheritance, and is caused by a cytosine-thymine-guanine (CTG) triplet expansion in the 3′ untranslated region of the dystrophia myotonica protein kinase (DMPK) gene on chromosome 19q13. This expansion is present in ubiquitously expressed genes and when transcribed accumulates in the nucleus as expanded CUG repeat RNA. This causes sequestration of muscleblind-like protein (MBNL) and upregulation of CUG-binding protein, resulting in altered splicing and causing various symptoms of DM1. As reported that MBNL2 knockout mice exhibit increased rapid eye movement (REM) sleep propensity and short REM sleep latency,1 the MBNL2 gene is particularly involved in the development of central nervous system (CNS) symptoms.1–5
The major symptoms of DM1 are myotonia, progressive muscle atrophy, and muscle weakness, whereas various other organ disorders are also observed. Excessive daytime sleepiness (EDS) is frequently observed as a CNS symptom. While it was a study limited only to childhood-onset DM1, the EDS was reported in approximately half of patients.6 Although EDS in DM1 patients is often accompanied by sleep-disordered breathing (SDB), it tends to persist even if noninvasive positive pressure ventilation (NIPPV) is properly used.7,8 Furthermore, some of the DM1 patients show REM sleep-related abnormalities, such as sleep-onset REM periods (SOREMPs).9,10 The EDS and SOREMPs resemble those observed in narcolepsy caused by decreased orexin (hypocretin) levels in the cerebrospinal fluid (CSF). Several studies have reported CSF orexin deficiency in DM1 patients, but the results are inconsistent. Martinez-Rodriguez et al found decreased CSF orexin levels in DM1 patients,11 while Ciafaloni et al reported that CSF orexin levels in DM1 patients were not different from the control group.12
Therefore, to further elucidate the role of orexin in EDS of DM1 patients, we verify whether orexin levels of DM1 patients differ from those of patients with narcolepsy type 1 and idiopathic hypersomnia (IHS), which is a disease with normal CSF orexin levels.
Patients and methods
We retrospectively analyzed data from 17 DM1 patients with EDS, 46 with narcolepsy type 1, and 30 with IHS that were previously collected to measure CSF orexin levels. All patients were Japanese. Written informed consent was obtained from all patients and/or their guardian(s). This study was approved by the ethics committee of Akita University Graduate School of Medicine.
We enrolled DM1 patients with EDS in this study and measured their CSF orexin levels (Figure 1). All DM1 patients complained of EDS, but without cataplexy. The diagnosis of DM1 was clinically and genetically confirmed in all patients. The clinical types included in this study were adult-onset form or milder child-onset form, while severe congenital form was not included. Sleepiness was evaluated subjectively using the Epworth Sleepiness Scale (ESS)13 for 11 DM1 patients and objectively using the mean sleep latency (MSL) from the multiple sleep latency test (MSLT) for 6 DM1 patients. The ESS scores and MSL were compared between decreased and normal CSF orexin groups (n=7 and 10, respectively). Sleep apnea was evaluated using the apnea-hypopnea index (AHI) of polysomnography (PSG) for 10 DM1 patients. In addition, other information such as clinical symptoms, duration of disease before CSF orexin measurement, body mass index (BMI), presence of SOREMPs in MSLT or PSG, whether NIPPV was used, number of CTG repeats, and brain imaging findings were collected for some DM1 patients. For comparison, we identified age- and sex-matched patients with narcolepsy type 1 and IHS who had previously undergone measurement of CSF orexin levels. The ESS scores, MSL, and AHI were obtained for these patients. All patients with narcolepsy type 1 and IHS were diagnosed according to the International Classification of Sleep Disorders – Third Edition.14
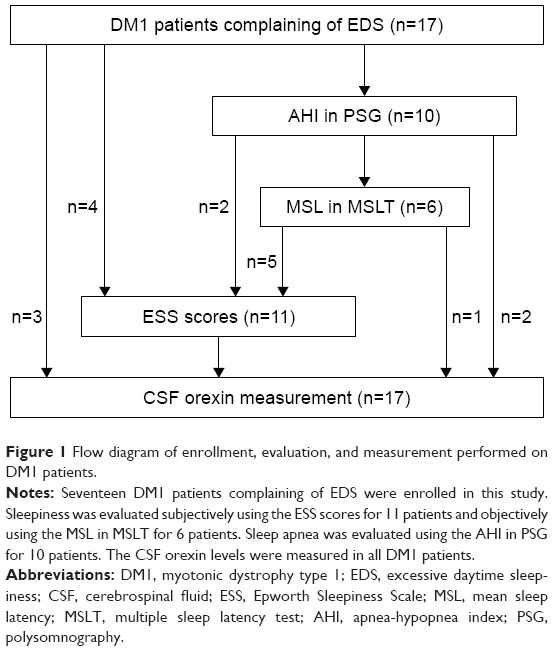 | Figure 1 Flow diagram of enrollment, evaluation, and measurement performed on DM1 patients. |
Sleep measurement
PSG was performed using unipolar induction electrodes including electroencephalogram (C3-A2, C4-A1, O1-A2, and O2-A1), chin electromyogram, and electrooculogram (left eye-A1, right eye-A2). Airflow was measured by airflow sensors attached to the nose and mouth using the thermocouple method. The breathing movements were recorded by band sensors attached to the chest and abdomen using the piezoelectric method. The body position, snoring, and arterial oxygen saturation were recorded by body position sensors, snore sensors, and pulse oximeters, respectively. In each hospital, recorders such as The Neurofax EEG-1524 (Nihon Kohden Corporation, Tokyo, Japan) were used. Subjects were put to bed at 9:00 pm and awakened at 6:00 am. All evaluations were based on the criteria of Rechtschaffen and Kales.15 An apnea was scored when a >90% decrease in baseline airflow that persisted for ≥10 s was observed. A hypopnea was scored when a 50%–90% decrease in baseline airflow associated with arousal, awakening, or <3% decrease in arterial oxygen saturation was observed. AHI was defined as the total number of apneas and hypopneas per hour of sleep and was defined as severe (>30 times/h), moderate (15–30 times/h), and mild (5–15 times/h).
MSLT was performed following PSG. MSLT naps were evaluated 4 times at 9:30 am, 11:30 am, 1:30 pm, and 15:30 pm, respectively. Sleep latency was determined by identifying the latency to either 3 consecutive epochs of stage 1 sleep or the first epoch of any other stage of sleep, and MSL was calculated from the sleep latency of each nap. SOREMPs were defined as the onset of REM sleep ≤15 min of sleep onset.
CSF orexin-A measurement
The lumbar punctures to obtain the CSF were performed around 10:00 am to 4:00 pm. The CSF orexin-A levels were measured using a commercially available 125I radioimmunoassay (RIA) kit (Phoenix Pharmaceuticals, Belmont, CA, USA) as previously described.16,17 The CSF orexin-A levels were determined against a known standard curve (1–128 pg/mL). For measuring, 100 μL of each sample was diluted 10 times with 900 μL of RIA buffer, and 100 μL of samples were incubated with 100 μL of provided rabbit anti-orexin-A antibody at 4°C for 24 h. Then, 100 μL of 125I-orexin-A was introduced and samples were incubated at 4°C for 5 days. On the third day, 100 μL of provided secondary antibody (goat anti-rabbit IgG) and 100 μL of provided normal rabbit serum were added to the mix and incubated at room temperature for 90 min. Finally, samples were centrifuged at 1,700× g for 20 min at 4°C and supernatants were immediately removed. The level of radioactivity left in the pellet was measured with an RIA counter. The detection limit of orexin was arbitrarily set at 40 pg/mL. The CSF orexin levels were defined as low (≤110 pg/mL), intermediate (>110 to ≤200 pg/mL), or normal (>200 pg/mL), since the mean CSF orexin level was ~300 pg/mL and significant differences according to sex or age have not been reported.18,19
Statistical analysis
Data were reported as mean ± standard deviation or median (25%–75%). Student’s t-test was used to analyze the differences in the ESS scores and MSL between decreased and normal CSF orexin groups among DM1 patients. Since CSF orexin levels, MSL, and AHI did not show homogeneity of variances, the differences among patients with DM1, narcolepsy type 1, and IHS were analyzed using Kruskal-Wallis test. When the p-value in Kruskal-Wallis test was statistically significant, Mann–Whitney U test was performed to compare groups. Mann–Whitney U test was followed by Bonferroni post-hoc test. All analyses, along with the calculation of two-sided p-values, were performed using IBM SPSS statistics version 24, and the significance level was set at p<0.05.
Results
Seventeen DM1 patients with complaints of EDS (8 males, 9 females) and aged 14–70 years, with mean of 39±18 years, were included in this study (Table 1). The CSF orexin levels decreased in 7 out of 17 patients (cases 1–7). These patients were included in the “decreased CSF orexin” group while the others were included in the “normal CSF orexin” group. Four patients from the decreased CSF orexin group had low levels of orexin, including 2 undetectable levels (<40 pg/mL), and 3 had intermediate levels. In 8 patients who had used NIPPV, their subjective complaints of EDS were not fully ameliorated following therapy, and the ESS scores and MSL were evaluated after the treatment with NIPPV. The ESS score was >10 (mean: 13.6±4.7) in 9 out of 11 patients whose data were available. The MSL was <8 min (mean: 9.1±6.4) in 3 out of 6 patients whose data were available. The AHI of 10 patients were: severe (>30 times/h) in 5 patients, moderate (15–30 times/h) in 2 patients, and mild (5–15 times/h) in 1 patient, and the mean was 32.8±29.2 times/h. Three patients exhibited SOREMPs in MSLT, and 1 patient exhibited increased amount of REM sleep in all-night PSG (33.2%); however, their CSF orexin levels were all normal.
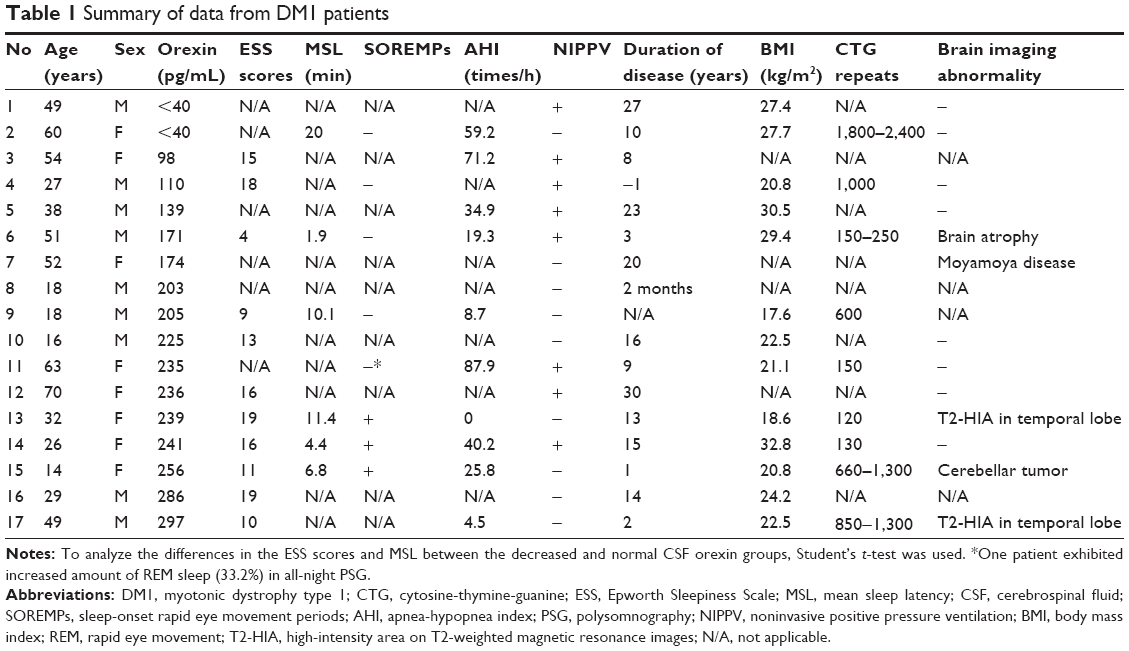 | Table 1 Summary of data from DM1 patients |
In the decreased CSF orexin group of DM1 patients, the mean ESS score and MSL were 12.3±7.3 and 11.0±12.8 min, respectively. In the normal CSF orexin group of DM1 patients, the mean ESS score and MSL were 11.8±4.0 and 8.2±3.2 min, respectively. Differences of the ESS scores and MSL between decreased and normal CSF orexin groups were insignificant among DM1 patients (p>0.05).
When comparing among patients with DM1, narcolepsy type 1, and IHS, the median of the CSF orexin levels were 205 pg/mL (139, 239), 42.5 pg/mL (40, 58.8), and 292 pg/mL (242.3, 361.5), respectively. The ESS scores were insignificantly different. The MSL of patients with DM1 and IHS was significantly higher than that of patients with narcolepsy type 1. The AHI of DM1 patients was significantly higher than that of patients with narcolepsy type 1, and showed no significant difference to that of IHS patients. The CSF orexin levels of patients with DM1 were significantly lower than those of patients with IHS and significantly higher than those of patients with narcolepsy type 1 (Table 2, Figure 2).
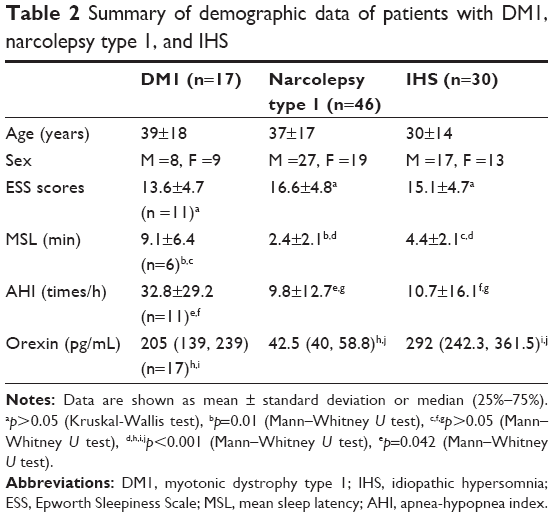 | Table 2 Summary of demographic data of patients with DM1, narcolepsy type 1, and IHS |
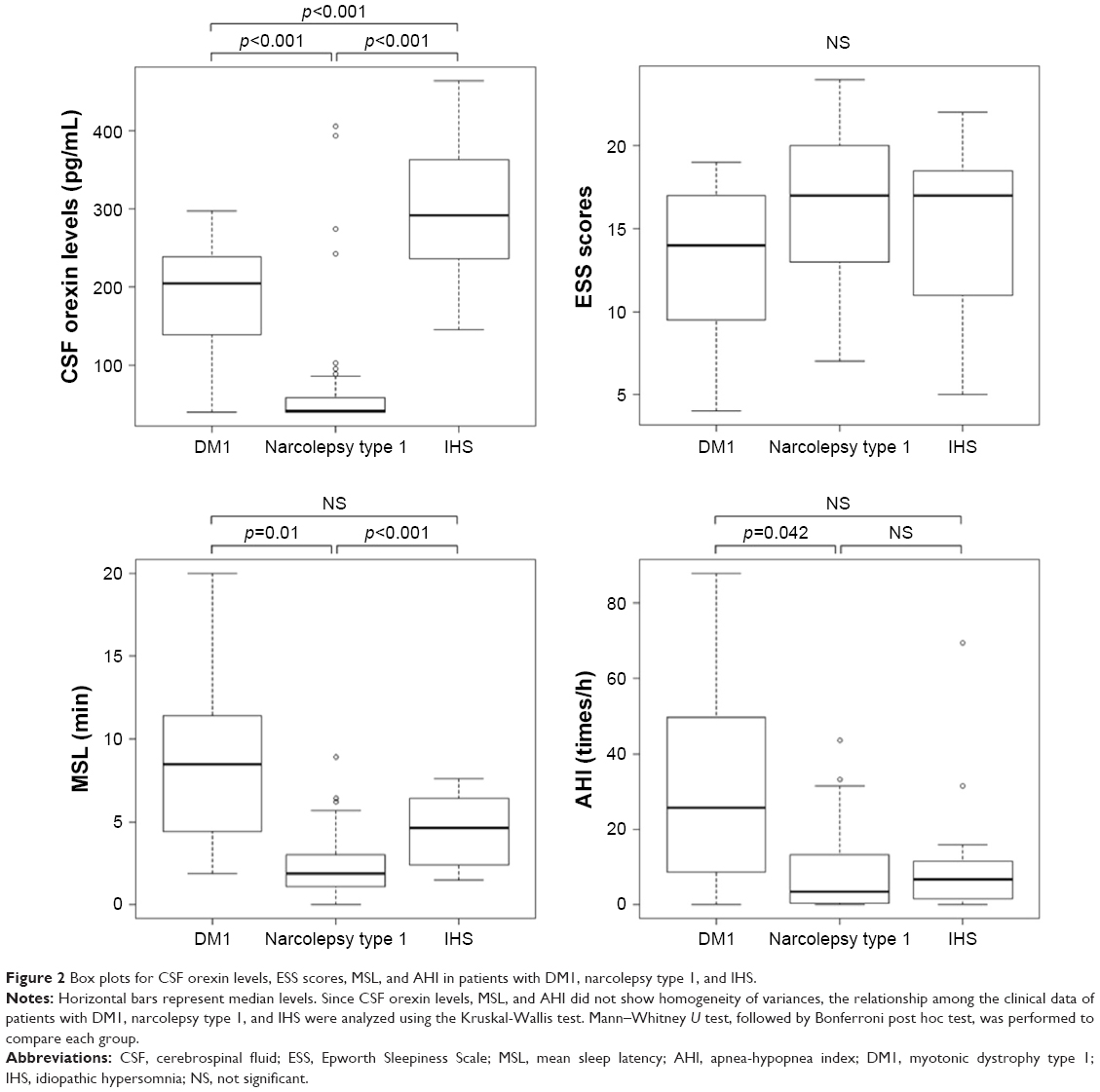 | Figure 2 Box plots for CSF orexin levels, ESS scores, MSL, and AHI in patients with DM1, narcolepsy type 1, and IHS. |
Discussion
CSF orexin levels and sleepiness evaluations
Sleep disturbances in DM1 patients are common and include SDB, periodic limb movement, central hypersomnia, and REM sleep dysregulation.20 Approximately 87.9% of DM1 patients have been reported to experience impaired sleep or daytime sleepiness.21 Since Martinez-Rodriguez et al initially observed orexin deficiency,11 they postulated that EDS in DM1 patients might be caused by decreased orexin release. In contrast to their data, Ciafaloni et al reported that 17 out of 38 DM1 patients complained of EDS and found that none of the 38 DM1 patients showed decreased CSF orexin levels, which is typically associated with narcolepsy (≤110 pg/mL).12
In this study, CSF orexin levels decreased in 7 out of 17 DM1 patients with EDS. In these patients, 2 had undetectable levels (<40 pg/mL);22,23 however, none of them had cataplexy and SOREMPs did not appear in MSLT in 1 patient. In addition, differences of the ESS scores and MSL between the decreased and normal CSF orexin groups were insignificant as reported by Martinez-Rodriguez et al.11
The CSF orexin levels of DM1 patients were significantly higher than those of patients with narcolepsy type 1 and lower than those of patients with IHS (considered as the control group with normal CSF orexin levels). Meanwhile, when comparing the sleepiness evaluations, the ESS score of DM1 patients was equivalent to that of patients with narcolepsy type 1 and IHS; however, the MSL of DM1 patients was significantly higher than that of patients with narcolepsy type 1 and IHS. These results suggest that the EDS reported by DM1 patients may not reflect the true sleepiness, because EDS of DM1 patients could include fatigue. Cytokines such as interleukin-6 (IL-6) are increased in DM1 patients,24 and IL-6 induces the sensation of fatigue.25 DM1 patients possibly experience fatigue, which is misinterpreted as EDS. Therefore, the features of the EDS reported in DM1 patients are not consistent with those of patients with narcolepsy type 1 and IHS, and orexin deficiency may not be the major factor of EDS in DM1 patients.
REM sleep dysregulation
In this study, 3 patients with normal CSF orexin levels exhibited SOREMPs, and 2 of them were accompanied by short MSL. Besides, 1 patient with normal CSF orexin level had increased amount of REM sleep in all-night PSG (case 11). Some DM1 patients have been reported to exhibit SOREMPs and short MSL9,10 and increased REM sleep.9 Although the associations among CSF orexin levels, short MSL, and SOREMPs are unclear, the presence of REM sleep-related abnormalities in 4 out of 7 patients, which was confirmed by detailed PSG or MSLT findings, is interesting. Studies on the mouse model of DM1 have already demonstrated the role of MBNL2 in REM sleep dysregulation,1,26 and the relationship between the underlying mechanism and orexin nervous system should also be investigated.
Influence of SDB
Reports of SDB are common in DM1 patients with EDS. In this study, AHI of DM1 patients was significantly higher than that of patients with narcolepsy type 1, that is, the influence of SDB on EDS in DM1 patients could not be completely excluded. However, the EDS of DM1 patients with SDB has been reported to lack improvement even after adequate therapy,8 and a considerable number of DM1 patients with EDS do not have SDB. Thus, SDB alone would not be the cause of EDS in these patients. However, methods to reduce the influence of SDB should be explored.
Limitation
This study has several limitations. Firstly, the number of DM1 patients with EDS included in this study may be too small. However, since the ESS scores and MSL of decreased and normal CSF orexin groups were similar, we could not conclude that orexin deficiency was a major factor in the EDS of DM1 patients. Consequently, more number of cases and prospective studies are needed. Secondly, clinical data concerning EDS, such as the ESS scores and MSL, were not available for some of the patients. Thirdly, since the ESS scores, MSL, and AHI of DM1 patients were not evaluated both before and after the treatment of SDB, the precise degree of influence of SDB could not be assessed.
Conclusion
CSF orexin levels were reduced in DM1 patients with EDS. In patients with DM1, their CSF orexin levels were not associated with the results from subjective or objective sleepiness evaluations, and features of their sleepiness seemed to differ from those of patients with narcolepsy type 1 or IHS. Although DM1 patients exhibited decreased CSF orexin levels, orexin deficiency may not be the major factor of EDS. Fatigue caused by cytokines, such as IL-6, may be perceived as sleepiness in these patients. The relationship between MBNL2-mediated REM sleep dysregulation and orexin nervous system should be investigated.
Acknowledgments
We would like to thank Dr Hiroaki Nozaki, Takayoshi Shimohata, Yumi Sekine, Kumiko Yasui, Naoki Suzuki, Daisuke Sato, Nobuyoshi Fukuhara, Yoshikazu Takayanagi, Ayumi Nishiyama, Genki Mizukoshi, Konomi Shimoda, Aiko Yasuniwa, Keisuke Suzuki, Kazusa Katanoda, Tsubasa Tei, and Ako Fujii for providing the patient samples and clinical data used in this study. This study was funded by a Special Coordination Fund from the Ministry of Education, Culture, Sports and Technology (MEXT). Additional support was provided by the International Institute for Integrative Sleep Medicine, sponsored by the World Premier International Research Center Initiative, from MEXT, Japan. We would like to thank Editage (www.editage.jp) for English language editing.
Author contributions
All authors contributed toward data analysis, drafting and revising of the paper, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Charizanis K, Lee KY, Batra R, et al. Muscleblind-like 2 mediated alternative splicing in the developing brain and dysregulation in myotonic dystrophy. Neuron. 2012;75(3):437–450. | ||
Kanadia RN, Shin J, Yuan Y, et al. Reversal of RNA missplicing and myotonia after muscleblind overexpression in a mouse poly (CUG) model for myotonic dystrophy. Proc Natl Acad Sci U S A. 2006;103(31):11748–11753. | ||
Hao M, Akrami K, Wei K, et al. Muscleblind-like 2 (Mbnl2)-deficient mice as a model for myotonic dystrophy. Dev Dyn. 2008;237(2):403–410. | ||
Wang ET, Cody NAL, Jog S, et al. Transcriptome-wide regulation of pre-RNA splicing and mRNA localization by muscleblind proteins. Cell. 2012;150(4):710–724. | ||
Suenaga K, Lee KY, Nakamori M, et al. Muscleblind-like 1 knockout mice reveal novel splicing defects in the myotonic dystrophy brain. PLoS One. 2012;7(3):e33118. | ||
Quera Salva MA, Blumen M, Jacquette A, et al. Sleep disorders in childhood-onset myotonic dystrophy type 1. Neuromuscul Disord. 2006;16(9–10):564–570. | ||
Guilleminaut C, Philip P, Robinson A. Sleep and neuromuscular disease: bilevel positive airway pressure by nasal mask as a treatment for sleep disordered breathing in patients with neuromuscular disease. J Neurol Neurosurg Psychiatry. 1998;65(2):225–232. | ||
Dauvilliers YA, Laberge L. Myotonic dystrophy type 1, daytime sleepiness and REM sleep dysregulation. Sleep Med Rev. 2012;16(6):539–545. | ||
Yu H, Laberge L, Jaussent I, et al. Daytime sleepiness and REM sleep characteristics in myotonic dystrophy: a case-control study. Sleep. 2011;34(2):165–170. | ||
Laberge L, Begin P, Dauvilliers Y, et al. A polysomnographic study of daytime sleepiness in myotonic dystrophy type 1. J Neurol Neurosurg Psychiatry. 2009;80:642–646. | ||
Martinez-Rodriguez JE, Lin L, Iranzo A, et al. Decreased hypocretin-1 (orexin-A) levels in the cerebrospinal fluid of patients with myotonic dystrophy and excessive daytime sleepiness. Sleep. 2003;26(3):287–290. | ||
Ciafaloni E, Mignot E, Sansone V, et al. The hypocretin neurotransmission system in myotonic dystrophy type 1. Neurology. 2008;70(3):226–230. | ||
Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. | ||
American Academy of Sleep Medicine. The International Classification of Sleep Disorders. 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014. | ||
Rechtschaffen A, Kales A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Washington, DC: Government Printing Office; 1968. | ||
Nishino S, Ripley B, Overeem S, et al. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355:39–40. | ||
Nishino S, Ripley B, Overeem S, et al. Low cerebrospinal fluid hypocretin (orexin) and altered energy homeostasis in human narcolepsy. Ann Neurol. 2001;50(3):381–388. | ||
Kanbayashi T, Yano T, Ishiguro H, et al. Hypocretin-1 (orexin-A) levels in human lumbar CSF in different age groups: infants to elderly persons. Sleep. 2002;25(3):337–339. | ||
Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol. 2002;59(10):1553–1562. | ||
Romigi A, Albanese M, Liguori C, et al. Sleep-wake cycle and daytime sleepiness in the myotonic dystrophies. J Neurodegener Dis. 2013;2013:692026. | ||
Heatwole C, Bode R, Johnson N, et al. Patient-reported impact of symptoms in myotonic dystrophy type 1 (PRISM-1). Neurology. 2012;79(4):348–357. | ||
Iwata T, Suzuki N, Mizuno H, et al. [A marked decrease of orexin in the cerebrospinal fluid in a patient with myotonic dystrophy type 1 showing an excessive daytime sleepiness]. Rinsho Shinkeigaku. 2009;49:437–439. Japanese. | ||
Yasui K, Saito T, Tatsumi M, et al. [A case of myotonic dystrophy type 1 with recurrent sleep attack and low CSF orexin level]. Rinsho Shinkeigaku. 2010;50(7):501. Japanese. | ||
Johansson A, Carlström K, Ahrén B, et al. Abnormal cytokine and adrenocortical hormone regulation in myotonic dystrophy. J Clin Endocrinol Metab. 2000;85:3169–3176. | ||
Robson-Ansley PJ, de Milander L, Collins M, et al. Acute interleukin-6 administration impairs athletic performance in healthy, trained male runners. Can J Appl Physiol. 2004;29(4):411–418. | ||
Sakai N, Charizanis K, Lee K, et al. Sleep phenotype characterization of muscleblind-like 2 knockout mouse, a central model of myotonic dystrophy. Sleep Abstract Supplement. 2016;39:A14–A15. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.