")
Back to Journals » Clinical Ophthalmology » Volume 16
Oral Sedation is Non-Inferior to Intravenous Sedation for Cornea and Glaucoma Surgery: A Randomized Controlled Trial
Authors Lee HJ , Desai MA , Sadlak N , Fiorello MG , Githere WG, Subramanian ML
Received 17 February 2022
Accepted for publication 28 April 2022
Published 1 July 2022 Volume 2022:16 Pages 2105—2117
DOI https://doi.org/10.2147/OPTH.S354570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hyunjoo J Lee, Manishi A Desai, Natalie Sadlak, Marissa G Fiorello, Wanjiku G Githere, Manju L Subramanian
On behalf of The Oral versus Intravenous Sedation Study Group
Department of Ophthalmology, Boston Medical Center, Boston, MA, USA
Correspondence: Hyunjoo J Lee, Department of Ophthalmology, Boston Medical Center, 85 East Concord Street, 8th Floor, Boston, MA, 02118, USA, Tel +1 617 414 2020, Fax +1 617 414 2929, Email [email protected]
Purpose: To determine whether oral sedation is as safe and effective as IV sedation for ophthalmic surgeries other than cataract surgery, we tested whether patient satisfaction with oral triazolam was non-inferior to IV midazolam for cornea and glaucoma surgeries.
Patients and Methods: Seventy-five cornea and 49 glaucoma surgery patients 18 years and older at Boston Medical Center (Boston, MA) were randomized within each study group (cornea or glaucoma) to receive oral triazolam + IV placebo, or oral placebo + IV midazolam before surgery in a double-masked fashion. Supplemental IV anesthesia was administered as needed during surgery. The primary outcome measure was patient satisfaction with anesthesia, compared between oral and IV sedation groups via t-test for non-inferiority, based on 70 cornea and 43 glaucoma subjects completing the study. Secondary outcome measures included surgeon and anesthesia provider satisfaction with anesthesia, rate of supplemental IV anesthesia, and incidence of adverse events and surgical complications.
Results: Using an a priori non-inferiority margin of 0.5, initial oral sedation was non-inferior to initial IV sedation in cornea (n=70, p< 0.001) and glaucoma (n=43, p=0.017) groups, even after excluding subjects administered supplemental IV anesthesia. There were no significant differences in anesthesia provider or surgeon satisfaction, intra-operative complications, adverse events, or supplemental anesthesia between groups, except for higher anesthesia provider satisfaction with oral sedation in an Ahmed or Baerveldt implant ± cataract surgery sub-group (p=0.04). Subjects receiving supplemental anesthesia included 6 oral (18.2%) and 5 IV (13.5%) in the cornea group (p=0.59), and 7 oral (29.2%) and 6 IV (31.6%) in the glaucoma group (p=0.50).
Conclusion: Our results suggest that an initial dose of oral triazolam is equivalent to IV midazolam for non-cataract anterior segment surgeries. However, there was a relatively high need for supplemental IV anesthesia during some surgery types, particularly with glaucoma tube shunt implantation.
Keywords: triazolam, midazolam, oral sedation, anesthesia, cornea, glaucoma, ophthalmic surgery
Introduction
In most settings in the United States, ophthalmic surgeries are performed using a local anesthetic, such as a nerve block and/or topical anesthesia, along with a sedative to reduce anxiety while still maintaining consciousness, with supervision by an anesthesia provider.1,2 Benzodiazepines are most often used as a sedative agent during ophthalmic surgeries in the absence of contraindications, and of this class of drugs, intravenous (IV) midazolam is currently the most popular choice due to its rapid onset and elimination.3 However, IV sedation requires fasting for at least 6 hours prior to surgery, as well as placement of an IV line.4 Additionally, IV sedation is associated with a greater financial burden due to the higher cost of IV sedatives and increased staffing requirements, among other factors.5
Recently, a number of studies have examined the safety and efficacy of oral sedation in cataract surgery, the most commonly performed ophthalmic surgery. In two independent studies, Rocha et al and Chen et al found that use of an oral sedative in addition to a local anesthetic was a safe and effective means of managing pain and anxiety for low-risk cataracts patients.6,7 Cataract surgery performed in an outpatient office-based setting with a back-up medical emergency team, in lieu of active monitoring by an anesthesia provider, has also been found to be safe.8 Our group has previously reported that oral triazolam was non-inferior to intravenous midazolam for patient satisfaction in cataract surgery amongst a diverse patient population in an urban, safety-net hospital setting.9
The use of oral sedatives or office-based procedure rooms for non-cataract ophthalmic surgeries has not been widely studied. Minimizing the need for continuous monitored anesthesia care for a wider variety and larger number of ophthalmic surgeries could lead to further gains in healthcare value. Reported outcomes with oral sedation for cataract surgery are not directly applicable to other anterior segment surgeries, because operative times are generally longer, and tissue handling may be more extensive than in a typical cataract surgery. No other studies have compared patient experience with oral compared to intravenous sedation for non-cataract anterior segment surgery from our review. We thus sought to examine whether various anterior segment surgeries, including endothelial keratoplasty, pterygium excision, minimally invasive glaucoma surgery, and glaucoma filtering surgeries, could be successfully performed with oral sedation in an urban academic teaching hospital setting with a diverse patient population. We herein describe the results of our prospective, double-masked, randomized trial to determine if oral sedation is non-inferior to IV sedation for patient satisfaction in non-cataract anterior segment surgeries. In addition to patient satisfaction, secondary outcomes measured included surgeon satisfaction, anesthesia provider satisfaction, surgical and non-surgical complications, and whether additional anesthesia or other interventions by an anesthesia provider were necessary during surgery.
Patients and Methods
We performed a prospective, single-center, randomized, double-masked, parallel-group study conducted at Boston Medical Center (BMC), an urban, academic medical center that treats a diverse patient population in Boston, Massachusetts. This study was internally funded by Boston Medical Center’s Ambulatory Services Department, approved by the BMC Institutional Review Board (IRB), followed the tenets of the Declaration of Helsinki, and was compliant with all HIPAA regulations. The BMC IRB approved the screening of patients, randomization of subjects, administration of study medications, and the collection of all data presented in this study in a prospective manner. All study subjects provided written informed consent using forms approved by the BMC IRB. The clinical trial is registered at http://clinicaltrials.gov (NCT03246724, PI: Manju Subramanian).
Patients who were scheduled to receive one of the following cornea or glaucoma surgeries between October 2017 and November 2019 were screened for eligibility. The cornea group included: Descemet Membrane Endothelial Keratoplasty (DMEK) with or without concurrent phacoemulsification cataract extraction with intraocular lens implant (phaco/IOL), Descemet Stripping Endothelial Keratoplasty (DSEK) with or without phaco/IOL, conjunctival and/or corneal lesion excision with cryotherapy and amniotic membrane transplantation, and pterygium excision with conjunctival autograft. The glaucoma group included the following procedures with or without phaco/IOL: trabeculectomy, Ahmed® (New World Medical, Ranch Cucamonga CA) or Baerveldt® implant (Johnson & Johnson Vision, Jacksonville, FL) with corneal patch graft, endoscopic cyclophotocoagulation (ECP) (Beaver Visitec, Inc., Waltham, MA), iStent® (Glaukos, San Clemente, CA), Kahook dual blade® (New World Medical, Ranch Cucamonga CA) or Cypass® micro-stent (Alcon, Fort Worth, TX) implantation. CyPass® micro-stent was recalled in August of 2018, and no Cypass® cases actually met criteria during the study period.
Eligibility criteria included age 18 years or older, and ability to read, speak and give independent informed consent in English, Spanish, or Haitian Creole. Exclusion criteria included a surgical plan that called for general anesthesia, allergy or sensitivity to benzodiazepines, pregnancy or active nursing, active use of an oral or IV medication known to be a cytochrome P450 3A inhibitor, previous enrollment in this study for the fellow eye, and enrollment in a clinical trial involving an investigational drug in the last 3 months. If the subject was 70 years of age or older, a 6-question delirium screening questionnaire was administered prior to surgery. If a passing score was not achieved, patients were deemed ineligible for study participation. On the day of surgery, eligibility to receive a benzodiazepine was re-reviewed by the anesthesia service according to standard of care procedures. Intoxication with drugs or alcohol on the day of surgery led to subject exclusion. The involvement of trainees (residents or fellows) in the surgical cases was not a factor in patient selection for study participation.
Subjects within each group, cornea or glaucoma, were randomized 1:1 to the oral triazolam (treatment) group and the IV midazolam (control) group, and each subject was assigned both a study ID and randomization ID number. To ensure masking of treatment assignments, our statistician was responsible for randomization. All other persons involved in the study, including subjects, surgeons, anesthesiologists, certified registered nurse anesthetists (CRNAs), research assistants, and investigators were masked to the treatment and control assignments for the entirety of the study. At the completion of the study, the statistician unmasked the treatment assignments to analyze the data, and forwarded the results to the rest of the study team.
The study drugs were prepared by Investigational Pharmacy Services (IPS) at BMC, and were dosed according to subjects’ body mass index (BMI). Subjects with a BMI < 35 received 0.125 mg (1 capsule) of oral triazolam or microcrystalline cellulose placebo and 1.0 mg IV midazolam or saline placebo. Subjects with a BMI ≥ 35 received 0.25 mg (2 capsules) of oral triazolam or microcrystalline cellulose placebo and 2.0 mg IV midazolam or saline placebo. On the day of surgery, subjects in the oral sedation (treatment) group were given their dose of oral triazolam 30 minutes before the start of their surgery and the IV saline placebo 5 minutes before the start of their surgery. Subjects in the IV sedation (control) group were given the oral microcrystalline cellulose placebo 30 minutes before the start of their surgery and their dose of IV midazolam 5 minutes before the start of their surgery. A nasal cannula was placed on each patient, and supplemental oxygen given as needed to maintain normal oxygen saturation, while avoiding the use of supplemental oxygen during any use of surgical cautery. A bar attached to the patients’ bed with air flowing through small vents helped to keep the surgical drape away from the patients’ nose and mouth.
A total of 10 surgeons contributed patients for this study. Ophthalmology residents or glaucoma fellows were involved to various degrees in performing the procedures at the discretion of the attending surgeon. Each procedure was performed using standard techniques, and the local anesthetic agent (s) of the surgeon’s choice. Additional IV anesthesia or other medications were administered at the discretion of the surgeon and the anesthesia provider if it was deemed that the study medication was not sufficient for patient comfort or safety. Subject demographic information, operative times, adverse events, and intraoperative complications were recorded.
Surgeons and anesthesia providers completed satisfaction surveys immediately after each operation. Subjects completed a satisfaction survey during their postoperative visit the following day to avoid the effects any residual sedation would have on their ability to answer questions. The survey designs were previously described, and were based on the Iowa Satisfaction with Anesthesia Scale, a previously validated tool for assessing patient satisfaction with cataract surgery.9,10
Sample Size Justification
Patient satisfaction was the primary outcome measure. In order to determine non-inferiority of oral triazolam vs IV midazolam for patient satisfaction, the non-inferiority margin was determined a priori to be 0.5 with a mean satisfaction score of 5.5 on a scale of 1–6, and a standard deviation of 0.75. This was based on pilot survey results of 20 patients undergoing cataract surgery with IV sedation. Details of this justification were previously published.9 The total sample size estimated to obtain statistical significance with a power of 90% and 1:1 randomization of oral triazolam to IV midazolam was 80 subjects for each surgical population (cornea or glaucoma), with approximately 40 subjects in each treatment group (IV or oral).
Primary Outcome Measure
The primary outcome measure was patient satisfaction measured by a 13-question (12 scored, 1 unscored) satisfaction survey. (Table S1). The satisfaction survey was written in each subject’s preferred language (English, Spanish, or Haitian Creole), and was completed at the first post-operative visit. In the event the patient could not see well enough to read the survey, the survey was administered verbally by a research assistant, with an interpreter if required. Each question was scored on a Likert scale of 1–6. Each subject’s total score was calculated by taking the mean of the 12 scored questions, with 6 being the highest possible total score.
Mean patient satisfaction scores for patients given oral triazolam were compared to those of patients given IV midazolam via t-test for non-inferiority.
Secondary Outcome Measures
Anesthesia provider satisfaction (Table S2) and surgeon satisfaction (Table S3) were measured by a 6-question satisfaction survey immediately following completion of the surgical case. Each question was scored on a Likert scale of 1–6. The total score was calculated by taking the mean of the 6 questions, with 6 being the highest possible total score. Administration of additional IV anesthetic during surgery was allowed at the discretion of the operating surgeon and anesthesia provider to assuage concerns from the institutional review board and participating surgeons about patient comfort during surgery. Details of anesthesia administration were recorded including: medication name, dose, time of administration, and reason behind the administration. Intraoperative complications and peri-operative adverse events were also recorded.
The secondary outcomes were compared between the treatment groups using t-tests for continuous variables and chi-squared or Fisher’s exact tests for categorical variables. Analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC).
Results
A total of 84 subjects were consented into the cornea group, and 52 consented into the glaucoma group during the 25-month enrollment period (October 2017 to November 2019). The study was ended when enrollment was deemed to be sufficient based on our sample size justification. Seventy-five cornea and 49 glaucoma subjects were randomized, and 70 and 43 subjects completed each study, respectively. The reasons for subjects being dropped from the study after enrollment were: patient withdrawal of consent (n = 6 cornea, n = 2 glaucoma), barriers to surgical booking (n = 6 cornea), surgeon withdrawing their participation due to delays in medication delivery to pre-operative area (n = 2 cornea, n = 1 glaucoma), ineligibility on the day of surgery either due to a change in surgical plan (n =1 glaucoma), contraindications to receiving a benzodiazepine (n = 2 glaucoma), altered mental status of patient (n = 1 glaucoma), and ineligibility determined after study completion due to already having participated in this study with the fellow eye (n = 1 glaucoma). Of the 22 subjects administered the delirium questionnaire prior to randomization, none failed the screening. The patient demographics and medical conditions of the study populations are included in Table 1. In the cornea group, a higher proportion of subjects in the oral group were Spanish-speakers (p = 0.05). There were no other significant differences in demographics or medical conditions between subjects receiving oral or IV sedation in the cornea study. There were no statistically significant differences in demographics and medical conditions in the glaucoma group. The breakdown of the surgical case types included in both studies and the average lengths of each surgery are shown in Table 2. Case times (minutes between incision and wound closure) were not found to be significantly different between groups. In the cornea group, the mean case time was 37.18 ± 14.52 with oral sedation, and 36.08 ± 13.08 with IV sedation (p = 0.74). In the glaucoma group, the mean case time was 66.75 ± 29.03 with oral sedation and 72.74 ± 32.09 with IV sedation (p = 0.53).
 |
Table 1 Patient Characteristics |
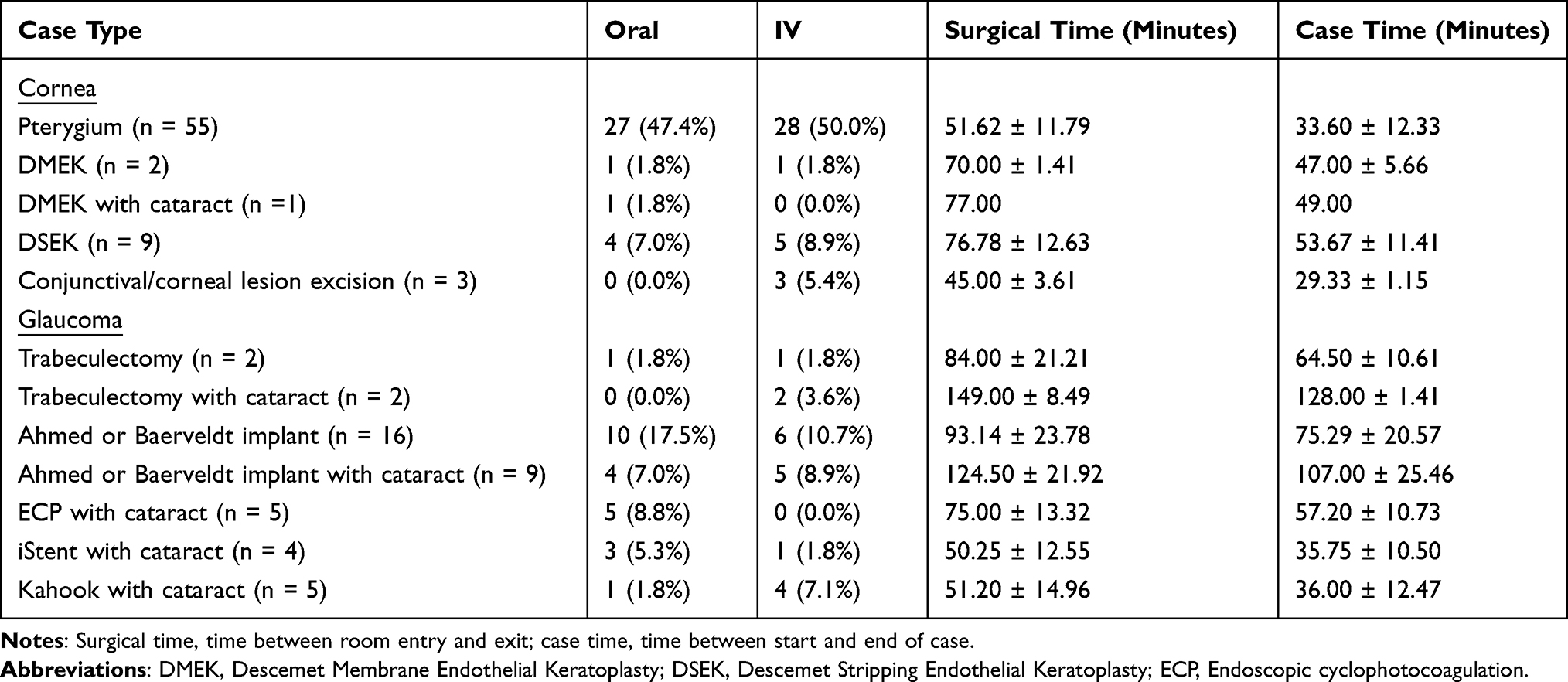 |
Table 2 Surgical Case Types and Operative Times |
Primary Outcome
Patient Satisfaction
The primary outcome measure was non-inferiority of patient satisfaction scores with oral sedation compared to IV sedation. In the cornea group (n = 70), the mean patient satisfaction score for the oral sedation group was 5.44 ± 0.75 (range 2.58–6.00) compared to 5.31 ± 0.62 (range 3.42–6.00) for the IV group. In the glaucoma group (n = 43), the mean patient satisfaction score for the oral sedation group was 5.10 ± 0.92 (range 3.00–6.00) compared to 5.00 ± 0.86 (range 3.50–6.00) for the IV group. Using an a priori non-inferiority margin of 0.5, oral sedation was non-inferior to IV sedation in both the cornea (p < 0.001) and glaucoma groups (p = 0.017). Realizing that many of the procedures in the cornea group had more similarities with procedures in the glaucoma group than to other procedures within the same group, and vice versa, we also performed a post hoc analysis of both study groups together (n =113). For instance, pterygium surgery and glaucoma filtering surgeries both involve conjunctival and scleral manipulation and cautery, whereas minimally-invasive glaucoma surgery and endothelial keratoplasty are intraocular procedures performed through clear corneal incisions. In the combined group, 57 received oral sedation (50.4%) and 56 received IV sedation (49.6%). The mean patient satisfaction score for oral sedation was 5.30 ± 0.83 (range 2.58–6.00) compared to 5.20 ± 0.71 (range 3.42–6.00) for IV sedation. Again, oral sedation was found to be non-inferior to IV sedation (p < 0.001) for the combined groups.
Secondary Outcomes
Surgeon and Anesthesia Provider Satisfaction
In the cornea group, the mean surgeon satisfaction score was 5.23 ± 1.03 (range 1.83–6.00) for oral sedation and 5.44 ± 0.88 (range 3.00–6.00) for IV sedation (p = 0.37). The anesthesia provider satisfaction in the cornea group was 5.34 ± 0.87 (range 2.17–6.00) for oral sedation and 5.31 ± 0.76 (range 3.17–6.00) for IV sedation (p = 0.87). In the glaucoma group, the surgeon satisfaction score was 4.80 ± 1.20 (range 2.50–6.00) for oral sedation, and 4.46 ± 1.51 (range 1.33–6.00) for IV sedation (p = 0.42). The anesthesia provider satisfaction in the glaucoma group was 4.95 ± 0.97 (range 2.67–6.00) for oral sedation, and 4.33 ± 1.30 (range 2.17–6.00) for IV sedation (p = 0.08). Combining the data from the cornea and glaucoma groups, the surgeon satisfaction score was 5.05 ± 1.11 (range 1.83–6.00) for oral sedation, and 5.11 ± 1.21 (range 1.33–6.00) for IV sedation (p = 0.79). The combined group anesthesia provider satisfaction with oral sedation was 5.18 ± 0.93 (range 2.17–6.00), and 4.98 ± 1.07 (range 2.17–6.00) with IV sedation (p = 0.29). There were no statistically significant differences between surgeon or anesthesia provider satisfaction between oral and IV sedation in the cornea, glaucoma or combined group data.
Sub-Group Analyses
Non-inferiority analyses of patient, surgeon, and anesthesia provider satisfaction scores were also compared between oral and IV sedation groups for the two largest surgery sub-groups in our study: pterygium surgery (n = 55), and Ahmed or Baerveldt implants with or without cataract surgery (n = 25). Patient satisfaction with oral sedation was non-inferior to IV sedation for pterygium (5.55 ± 0.59 oral vs 5.37 ± 0.63 IV, p < 0.001), and for Ahmed or Baerveldt implants ± cataract (5.07 ± 1.02 oral vs 4.76 ± 0.79 IV, p = 0.02). Surgeon satisfaction with oral sedation was non-inferior to IV sedation for pterygium (5.41 ± 0.76 oral vs 5.47 ± 0.85 IV, p = 0.02), but not for Ahmed or Baerveldt implants ± cataract (4.68 ± 1.26 oral vs 4.33 IV ± 1.52, p = 0.07). Anesthesia provider satisfaction with oral sedation was non-inferior to IV sedation for pterygium (5.43 ± 0.63 oral vs 5.29 ± 0.78 IV, p < 0.001), and for Ahmed or Baerveldt implants ± cataract (4.81 ± 1.02 oral vs 3.82 ± 1.27 IV, p = 0.002). A comparison of means showed that the higher anesthesia provider satisfaction with oral sedation in the Ahmed or Baerveldt implant ± cataract group was significant (p = 0.04). Sub-group analyses were not performed for other surgery types because the small sample sizes precluded meaningful statistical analysis.
Supplemental IV Anesthesia
Our studies were designed to allow the administration of additional IV anesthesia in the operating room if the study medication was deemed insufficient for patient comfort in order to maximize patient safety. We recorded the frequency with which IV sedatives or analgesic medications (midazolam, remifentanil, or fentanyl) were administered in addition to the study medication. In the cornea group, the number of subjects receiving supplemental IV anesthesia did not differ significantly between the oral (18.2%, n = 6) and IV sedation group (13.5%, n = 5) (p = 0.59). In the glaucoma group, there was also no significant difference between the number of subjects requiring supplemental IV anesthesia between the oral (29.2%, n = 7) and IV group (31.6%, n = 6) (p = 0.50). Similarly, in the combined analysis, there was no significant difference between the number of subjects requiring supplemental IV anesthesia [oral 23% (n = 13) vs IV 20% (n = 11), p = 0.56].
Because patient satisfaction could potentially be affected by whether or not subjects received supplemental IV anesthesia, we re-examined patient satisfaction excluding subjects that received supplemental anesthesia. In the cornea group, the adjusted patient satisfaction scores were 5.65 ± 0.43 (range 4.50–6.00) for oral sedation, and 5.35 ± 0.61 (range 3.42–6.00) for IV sedation. After excluding subjects receiving supplemental anesthesia, patient satisfaction with oral sedation was again non-inferior to IV sedation with a non-inferiority margin of 0.5 (p < 0.001), and was in fact significantly higher with oral sedation in the cornea group (p = 0.04). In the glaucoma group, the adjusted patient satisfaction scores were 5.34 ± 0.85 (range 3.00–6.00) with oral sedation, and 5.12 ± 0.89 (range, 3.50–6.00) with IV sedation, with oral sedation non-inferior to IV sedation (p = 0.017). In the combined group analysis, the adjusted patient satisfaction scores were 5.59 ± 0.51 (range, 3.92–6.00) for oral sedation, and 5.33 ± 0.66 (range, 3.42–6.00) for IV sedation, again with oral sedation non-inferior to IV sedation (p < 0.001).
Despite the fact that there were no significant differences in the rate of supplemental IV anesthesia administered between oral and IV sedation groups, we observed that 30% of glaucoma subjects as a whole, and 16% of cornea subjects as a whole, were administered supplemental IV anesthesia. The procedure types associated with the highest proportion of the subjects requiring supplemental anesthesia (44%) were Ahmed or Baerveldt implant, with or without cataract surgery. Additionally, in a combined analysis of both groups, 50% (7 of 14) of all surgeries with case times longer than 90 minutes required supplemental IV anesthesia; whereas, 10% (3 of 29) surgeries with case times 30 minutes or less required supplemental IV anesthesia.
We also examined whether the type of local anesthesia used could have influenced the rate of supplemental IV anesthesia (Table 3). In the combined group of all surgeries, there was no significant association between the type of local anesthesia used and the rate of supplemental IV anesthesia (p = 0.26 oral, p = 0.47 IV, p = 0.20 total combined). After analyzing possible associations within the surgical groups listed in Table 3, the only significant association between local anesthetic type and rate of supplemental IV anesthesia was found in the combined oral and IV pterygium group (p = 0.027), with higher rates of supplemental IV anesthesia associated with topical anesthetic use (66%, n = 3) than with subconjunctival anesthetic (10%, n = 10) or with a regional block (sub-Tenon’s, peribulbar or retrobulbar) (12%, n = 42).
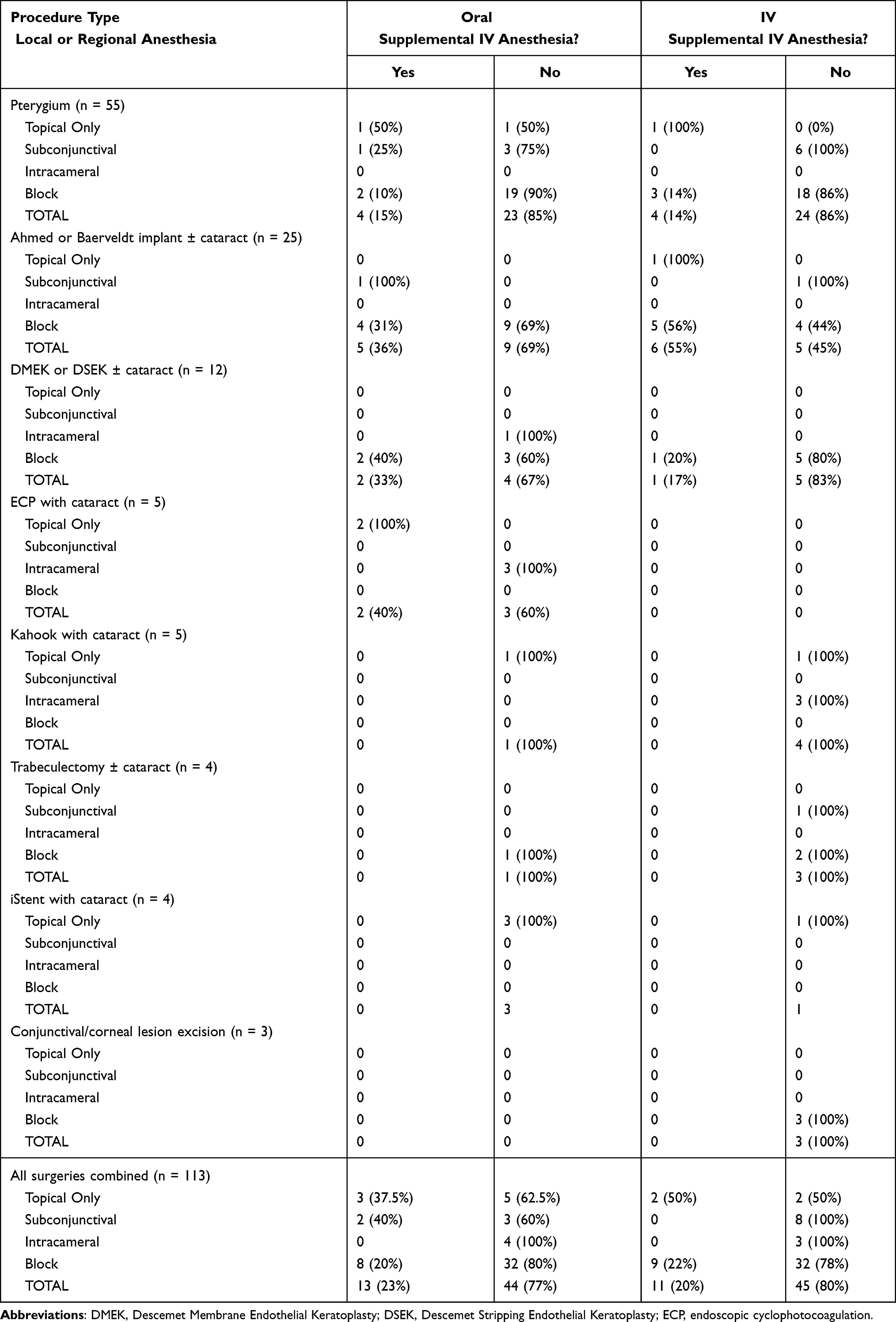 |
Table 3 Rates of Supplemental IV Anesthesia by Local or Regional Anesthesia Type |
Safety Outcomes
In both the cornea and glaucoma groups, there were no statistically significant differences in intra-operative complications or adverse events between the oral and IV groups (Table 4). However, there appeared to be a trend toward more adverse events occurring in the IV sedation groups. Intra-operative surgical complications included hyphema, floppy iris syndrome, and an extended closure of conjunctiva requiring amniotic membrane during a glaucoma shunt surgery.
 |
Table 4 Intra-Operative Complications and Adverse Events |
Discussion
The objective of this prospective, single-center, randomized, double-masked, parallel-group study was to determine whether oral sedation could feasibly be introduced in non-cataract anterior segment surgeries. Prior to this study, it was uncertain whether trends observed in cataract surgery with regard to oral sedation would hold true across other types of anterior segment procedures, as certain cornea and glaucoma surgeries can be more invasive, involving conjunctival manipulation or contact with extra-ocular muscles, or longer in duration than uncomplicated cataract surgery. Our results indicated that initial sedation with oral triazolam could be a viable alternative to initial sedation with IV midazolam, as oral triazolam was found to be non-inferior to IV sedation in terms of patient satisfaction for both cornea and glaucoma surgeries. In the cornea group, patient satisfaction was actually higher with oral sedation when excluding subjects in either sedative group that received supplemental IV anesthesia. Additionally, there was no significant difference in mean surgeon satisfaction, mean anesthesia provider satisfaction, rate of intraoperative complications, incidence of adverse events, or need for supplemental anesthesia in the cornea or glaucoma groups. In a sub-group analysis, anesthesia providers were more satisfied with initial oral sedation in the sub-group of patients undergoing Ahmed or Baerveldt implantation with or without cataract surgery.
Our finding that oral triazolam may be an appropriate initial sedative in anterior segment surgeries beyond cataract surgery has a number of implications. Primarily, switching to initial oral sedation for a wide variety of surgeries could be a cost-saving measure. Oral sedation has been associated with reduced costs compared to IV sedation in previously published studies. An extensive cost analysis on the use of oral vs IV sedation for cataract surgery suggested an 8-fold reduction in cost per patient.5 In another study, the cost of a single dose of IV midazolam was found to be approximately 100 times greater than that of its oral counterpart.7 Next, avoidance of IV sedation when possible may help improve surgical outcomes. For most ophthalmic surgeries, an IV injection is used to achieve conscious sedation to help relax the patient and alleviate anxiety and pain.2 However, a prior study found that IV sedation for the purpose of pain or anxiety relief in cataract surgery was associated with an increased incidence of intraoperative complications and adverse events as compared to the same procedure without IV placement.11 Likewise, in our study, we saw a trend toward higher rates of adverse events with IV sedation, although there was no statistically significant difference. The reason for potentially higher rates of adverse events and complications with IV midazolam compared to oral triazolam is not entirely clear, but could be related to the greater bioavailability of IV midazolam, or the greater overall safety profile of oral triazolam.12,13 Interestingly, we also saw higher satisfaction with oral sedation for cornea surgeries when excluding subjects that received supplemental IV anesthesia. Notably, the study design required that subjects in the oral sedation group still had to fast prior to surgery and have IV lines placed, suggesting that this greater satisfaction is related to differences in pharmacologic effects of the oral triazolam versus IV midazolam in this group. Overall, this suggests that utilizing an initial oral sedative may contribute to a decrease in cost, and possible increase in patient satisfaction in some cases, regardless of whether cornea and glaucoma surgeries are performed in an operating room with an anesthesia provider, or in an office-based setting.
Our studies were designed to allow participating surgeons and anesthesia providers to administer supplemental IV anesthesia as needed in order to maximize patient safety. Given that the rate of supplemental IV anesthesia was not different between the oral and IV sedation groups, and that patient satisfaction with oral sedation was still non-inferior to IV sedation after excluding the subjects that had received supplemental IV anesthesia, we believe that allowing subjects to receive supplemental anesthesia did not significantly bias our primary outcome. We did, however, note significant variability in the rate of supplemental anesthesia for different surgery types and durations, with higher rates for procedures lasting longer than 90 minutes. Ahmed or Baerveldt implants with or without cataract surgery required more supplemental IV anesthesia, and were among the longest duration cases included in our studies, but we could not determine from our data whether certain cases may have required more frequent supplemental anesthesia because they were longer, or because of other factors. Surgeries such as these that frequently require supplemental IV anesthesia may not be well suited for an office-based setting without an anesthesia provider present, regardless of whether initial oral sedation is non-inferior to initial IV sedation.
Potential factors affecting the rates of supplemental IV anesthesia could have been the type of local anesthesia the surgeons chose to use, and the involvement of residents and fellows. We did not find an influence of local anesthetic type on the rates of supplemental IV anesthesia in the overall group, but there was a significant association within the pterygium surgery group. Our results suggest that pterygium surgery is best performed with a block (sub-Tenon’s, peribulbar, or retrobulbar) or subconjunctival injection of anesthetic if there is a desire to limit the need for supplemental IV anesthesia. In addition, it seems likely that intracameral anesthesia is preferable to topical anesthesia to limit rates of supplemental IV anesthesia for endoscopic cyclophotocoagulation with cataract surgery given that all topical cases needed supplemental IV anesthesia (n = 2), and all intracameral cases did not (n = 3) (Table 4). The sample size was too small to perform meaningful statistical analysis, but it stands to reason that adequate local anesthesia would not be achieved for a procedure involving destruction of uveal tissue with a topical agent alone. Further study is needed to determine whether certain types of local anesthesia can minimize the need for supplemental IV anesthesia with other surgery types. We did not record whether the primary surgeons were trainees or attendings, but the usual practices of participating surgeons suggest that well over 80% of the glaucoma and pterygium surgeries would have been primarily performed by a resident or fellow, whereas all of the endothelial keratoplasty and conjunctival/corneal lesion excision cases were performed by an attending cornea specialist. Cases that were primarily performed by a trainee may have been longer, and may have involved more tissue handling than cases primarily performed by an attending surgeon. Given the randomization process, we would expect an even distribution of trainee cases in the oral and IV groups, and although we are not able to confirm this, we do not believe that this should have influenced our outcomes of patient, surgeon and anesthesia provider satisfaction non-inferiority. However, the rates of supplemental IV anesthesia for pterygium and glaucoma surgeries could have very well been influenced by trainee involvement, and warrants further study to determine how surgeon experience affects the ability to comfortably and safely perform certain surgeries in an office-based setting.
Our subjects were racially and ethnically diverse, and had a wide variety of concurrent medical conditions. However, we only enrolled patients who were low risk candidates for oral sedation with a benzodiazepine. Also, certain case types were excluded, such as micropulse transcleral cyclophotocoagulation (TSCPC) (IRIDEX Corp., Mountain View, CA), deep anterior lamellar keratoplasty (DALK) or penetrating keratoplasty (PKP). The reason for exclusion of patients undergoing micropulse TSCPC was that it is usually performed with brief, very deep sedation due to the amount of pain generally associated with this short treatment, and the study medication dosages were thought to be inadequate. DALK and PKP are often performed under general anesthesia. In order to avoid selecting some DALK/PKP patients to be eligible for the study over others planned for general anesthesia, all DALK and PKP patients were excluded. Thus, our results do not suggest that oral sedation is appropriate for all patients undergoing anterior segment surgeries; rather, they indicate that oral sedation may be a suitable alternative to IV sedation for patients who meet a certain set of criteria that have yet to be fully determined.
We relied on the use of the Iowa Satisfaction with Anesthesia Survey (ISAS) to assess our primary outcome, patient satisfaction. This tool was previously validated for use with cataract surgery, but has not specifically been validated for use in cornea, conjunctiva, or glaucoma surgeries.10 We still believe that it was appropriate to use the ISAS, as this tool has been successfully used in research across a wide variety of surgery types, including other ophthalmic surgeries.14 Furthermore, using a survey as the primary endpoint measurement always runs the risk of introducing bias, as responses may be influenced by the subject’s expectations and beliefs, even if masking is maintained. This is especially relevant in the context of a non-inferiority study, as there is the potential for this type of analysis to determine non-inferiority when there is none. However, to protect against this, we selected a non-inferiority margin such that any subtle differences between the two groups would not be clinically relevant and would not affect our analysis. Additionally, the range of responses seen in patients (range 2.58–6.00), surgeons (range 1.33–6.00), and anesthesia provider (range 2.17–6.00) did not suggest the presence of any noticeable bias.
One of the major limitations of our study is the wide variety of different case types. Our study was designed to be as inclusive as possible of all non-cataract anterior segment surgeries in order to maximize our statistical power. We also recognize that some case types were not represented in both oral and IV sedation groups, and that the number of cases in each group, with the exception of pterygium, was also small (Table 2). This does not discount the finding of non-inferiority in the overall cornea and glaucoma study groups, or in the combined group of non-cataract anterior segment surgery. However, whether or not oral sedation is equivalent to IV sedation for specific anterior surgery case types, other than pterygium, or Ahmed or Baerveldt implants as a general group, has yet to be determined.
Conclusion
Much of the existing literature comparing oral to intravenous sedation in ophthalmic procedures focuses on studying oral sedation primarily in the context of cataract surgery. Studies that examine the safety, efficacy, and overall satisfaction with oral sedation in other ocular procedures are limited. We determined that initial oral sedation was non-inferior to initial intravenous sedation in terms of patient satisfaction, with no significant difference in anesthesia provider satisfaction, surgeon satisfaction, intraoperative complications, adverse events, or need for supplemental anesthesia between our main groups. Although for longer surgeries, and certain surgery types such as Ahmed and Baerveldt implantations, a single dose of either oral triazolam or IV midazolam was frequently insufficient for complete patient sedation, oral triazolam could still be used as an initial sedative with the option to supplement with IV medications as needed during surgery without compromising patient safety and satisfaction. These findings have clinical, financial, and safety implications that could improve patient experience while reducing overhead costs, but further study is needed to better understand the circumstances under which oral sedation alone without supplementary IV medications could be appropriate for specific non-cataract anterior segment surgeries, including the influence of type and length of surgery and any patient characteristics such as anxiety disorders or language barriers that may influence response to sedation.
Data Sharing Statement
The study flow, characteristics of study subjects, outcomes and adverse events of this study are available at ClinicalTrials.gov (NCT03246724) for as long as. We do not intend to share individual deidentified participant data.
Acknowledgments
The authors thank Gheorghe Doros, PhD of Boston University for statistical analysis, Stephen P. Christiansen, MD of Boston Medical Center for data safety monitoring, and Boston Medical Center administration and staff members: Joe Camillus; Yi-An Huang; Lance Maggiacomo BSN, RN, CNOR; Bryan Guzman, Merit R. Gorgy, BS, Nina Tamashunas, BS, Priyanka Patel, Carrie Chen, Boston Medical Center’s Moakley Anesthesiology Staff, Moakley Nursing Staff, and Investigational Pharmacy Services. Franklin Dexter, MD, PhD and the University of Iowa Research Center, permitted use of elements of the Iowa Satisfaction with Anesthesia Scale.
Collaborators
Department of Ophthalmology, Boston Medical Center, Boston, Massachusetts, USA: Noelle Crough1, Babak Eliassi-Rad1, Elizabeth S. Esparaz1, Jiwoo Kim1, Maria Velazquez-Lamela1, MD Matthew Leidl1, Catherine V. Levitt1, Daniel J. Luther1, Heenal Marfatia1, Kambiz Negahban1, Steven Ness1, Crandall E. Peeler1,3, Tony Pira1, Rohini Rao1, Susannah Rowe1, Nicole H. Siegel1, Viha Vig1; Department of Anesthesiology, Boston Medical Center, Boston, Massachusetts, USA: Wissam H. Mustafa2, Mark C. Norris2, Pavan Sekhar2; Department of Investigational Pharmacy Services, Boston Medical Center, Boston, Massachusetts, USA: Stephen Zalewski4
1Department of Ophthalmology, Boston Medical Center, Boston, Massachusetts, USA
2Department of Anesthesiology, Boston Medical Center, Boston, Massachusetts, USA
3Department of Neurology, Boston Medical Center, Boston, Massachusetts, USA
4Department of Investigational Pharmacy Services, Boston Medical Center, Boston, Massachusetts, USA
Funding
This work was supported by Boston Medical Center, Boston, MA. Boston Medical Center had no role in the design or conduct of this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nouvellon E, Cuvillon P, Ripart J. Regional anesthesia and eye surgery. Anesthesiology. 2010;113(5):1236–1242. doi:10.1097/ALN.0b013e3181f7a78e
2. Greenhalgh DL, Kumar CM. Sedation during ophthalmic surgery. Eur J Anaesthesiol. 2008;25(9):701–707. doi:10.1017/S0265021508004389
3. Loots H, Wiseman R. Agents for sedation in ophthalmic surgery: a review of the pharmacodynamics and clinical applications. Curr Anaesth Crit Care. 2006;17(3–4):179–190. doi:10.1016/j.cacc.2006.09.001
4. Practice Guidelines for Preoperative Fasting and the Use of Pharmacologic Agents to Reduce the Risk of Pulmonary Aspiration. Application to healthy patients undergoing elective procedures: an updated report by the American Society of Anesthesiologists task force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology. 2017;126(3):376–393. doi:10.1097/ALN.0000000000001452
5. Reeves SW, Friedman DS, Fleisher LA, Lubomski LH, Schein OD, Bass EB. A decision analysis of anesthesia management for cataract surgery. Am J Ophthalmol. 2001;132(4):528–536. doi:10.1016/S0002-9394(01)01159-X
6. Rocha G, Turner C. Safety of cataract surgery under topical anesthesia with oral sedation without anesthetic monitoring. Can J Ophthalmol J Can Ophtalmol. 2007;42(2):288–294. doi:10.3129/can.j.ophthalmol.i07-034
7. Chen M, Hill GM, Patrianakos TD, Ku ES, Chen ML. Oral diazepam versus intravenous midazolam for conscious sedation during cataract surgery performed using topical anesthesia. J Cataract Refract Surg. 2015;41(2):415–421. doi:10.1016/j.jcrs.2014.06.027
8. Koolwijk J, Fick M, Selles C, et al. Outpatient cataract surgery: incident and procedural risk analysis do not support current clinical ophthalmology guidelines. Ophthalmology. 2015;122(2):281–287. doi:10.1016/j.ophtha.2014.08.030
9. Peeler CE, Villani CM, Fiorello MG, Lee HJ, Subramanian ML. Oral versus intravenous sedation study group. patient satisfaction with oral versus intravenous sedation for cataract surgery: a randomized clinical trial. Ophthalmology. 2019;126(9):1212–1218. doi:10.1016/j.ophtha.2019.04.022
10. Fung D, Cohen M, Stewart S, Davies A. Can the Iowa Satisfaction with Anesthesia Scale be used to measure patient satisfaction with cataract care under topical local anesthesia and monitored sedation at a community hospital? Anesth Analg. 2005;100(6):1637–1643. doi:10.1213/01.ANE.0000154203.00434.23
11. Katz J, Feldman MA, Bass EB, et al. Adverse intraoperative medical events and their association with anesthesia management strategies in cataract surgery. Ophthalmology. 2001;108(10):1721–1726. doi:10.1016/S0161-6420(01)00704-7
12. Midazolam injection, USP. FDA label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/208878Orig1s000lbl.pdf.
13. Halcion® triazolam tablets, USP CIV. FDA label. Avaialable from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/017892s049lbl.pdf.
14. Barnett SF, Alagar RK, Grocott MPW, Giannaris S, Dick JR, Moonesinghe SR. Patient-satisfaction measures in anesthesia: qualitative systematic review. Anesthesiology. 2013;119(2):452–478. doi:10.1097/ALN.0b013e3182976014
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.