")
Back to Journals » Clinical Interventions in Aging » Volume 12
Oral health-related quality of life and prosthetic status of nursing home residents with or without dementia
Authors Klotz AL, Hassel AJ, Schröder J, Rammelsberg P, Zenthöfer A
Received 19 October 2016
Accepted for publication 28 January 2017
Published 11 April 2017 Volume 2017:12 Pages 659—665
DOI https://doi.org/10.2147/CIA.S125128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Walker
Anna-Luisa Klotz,1 Alexander Jochen Hassel,1 Johannes Schröder,2,3 Peter Rammelsberg,1 Andreas Zenthöfer1
1Department of Prosthodontics, Dental School, 2Institute of Gerontology, 3Section of Geriatric Psychiatry, University of Heidelberg, Heidelberg, Germany
Purpose: The objective of this cross-sectional study was to evaluate the effect of prosthetic status on the oral health-related quality of life (OHRQoL) of nursing home residents with or without dementia.
Methods: The study was performed in 14 nursing homes across the federal state of Baden-Württemberg, Germany. All eligible participants were included, and general and medical information and information about their dental and prosthetic statuses were collected. The Geriatric Oral Health Assessment Index (GOHAI) was administered to evaluate OHRQoL. The Mini-Mental State Examination (MMSE) served to classify participants into living or not living with dementia according to the established cutoff value for dementia (MMSE <24). Parametric bivariate statistics and logistic regression models were used to analyze data at P<0.05.
Results: A total of 169 participants were included in this study. The mean age of the participants was 82.9 years. A total of some 70% of the sample was living with dementia. The mean GOHAI score along the sample was 49.1 (8.3), and 41% of the sample reported substantially compromised OHRQoL (GOHAI <50). OHRQoL was statistically similar for people with or without dementia (P=0.234); objective oral health was also similar in both groups (P>0.05). The number of teeth (odds ratio [OR]: 2.0), the type of prosthetic status (OR: 6.5), and denture-related treatment needs (OR: 2.4) were the major factors significantly affecting OHRQoL (P<0.05).
Conclusion: The OHRQoL of elderly nursing home residents is substantially compromised. Several prosthetic treatment needs for residents living with or without dementia were identified. Edentulism without tooth replacement and having <5 teeth resulted in an increased risk of substantially compromised OHRQoL. Further studies should be conducted to determine whether improvements in prosthetic status can increase OHRQoL.
Keywords: nursing home, dementia, oral health-related quality of life, prosthetic condition
Introduction
Aging of the population is a long-term trend in all middle- and high-income countries. As a result, the total amount of care needed increases and many of those care dependent elderly are living in nursing homes.1,2 Studies have consistently revealed poor oral hygiene and health among people living in nursing homes compared with younger and community-dwelling older adults. Nursing home residents face more severe oral problems, for example, tooth loss, periodontal disease, caries, and xerostomia.1–4 Worsening of oral health not only affects chewing function, and therefore nutrition, but also general health by aggravating cardiovascular diseases and infectious respiratory diseases.5–8 Most elderly people wear some sort of denture, increasingly frequently combined with natural teeth or implants needing adequate daily hygiene and dental aftercare.9 For nursing home residents, the following three major threats cause deteriorating oral conditions: first, carers frequently have limited knowledge of the specific oral care needed by the elderly and insufficient time to perform this properly; second, access to dental care providers is limited because of immobility; and, third, oral health issues are of low importance to the elderly themselves in the context of multimorbidity, including dementia.3,10
The World Health Organization suggests, however, that health is defined not only by the absence of disease but also by subjective well-being (health-related quality of life). Oral health-related quality of life (OHRQoL) is one aspect of this.11 Instruments have been developed for the assessment of OHRQoL. Besides the Oral Health Impact Profile (OHIP), a popular means of evaluation of OHRQoL in many communities, the Geriatric Oral Health Assessment Index (GOHAI) has been described as a quick and valid tool enabling the detection of small changes in oral health among elderly populations.12,13
Although OHRQoL is an important dental endpoint, the literature contains few reports of evaluation of dental and prosthetic factors affecting OHRQoL among the elderly. With regard to prosthetic factors, the number of teeth and the type of denture worn seem to be relevant to the OHRQoL of different community-dwelling populations.14–18
Limited information is available about the OHRQoL of elderly people living in nursing homes, who often live with dementia. Although studies have suggested that self-perception of oral health can differ from objective oral conditions among the elderly, whether with or without dementia,1,19 use of the GOHAI and OHIP among people with dementia is not yet well established in research. Ribeiro et al19 used the GOHAI to evaluate the OHRQoL of patients with dementia; to reduce the possibility of bias, participants in this study were assisted by their caregivers.
In a preliminary study of 94 nursing home residents living in four residential homes of the same care society, dementia was assessed using the Mini-Mental State Examination (MMSE),20 and possible factors affecting OHRQoL were assessed using the GOHAI.18 Initial results indicated that OHRQoL was associated with the type of denture worn but not with dementia.18 Larger sample sizes and a higher explanatory power would, however, be desirable to confirm these findings and to enable robust multivariate analysis to be conducted.
The objective of this study was, therefore, to evaluate the effect of prosthetic and dental statuses on OHRQoL among nursing home residents with or without dementia.
Methods
Study setting
This study was approved by the local review board of the University of Heidelberg (approval number S-002/2012). Fourteen nursing homes in Baden-Württemberg, one of the 16 federal states of Germany, were selected by the Ministry of Social Affairs as representative of the state’s facilities to enable generalization of the results of the study. The nursing homes differed in size, location (urban and rural), and residents’ distribution. All residents, or, if they were not sui legis, their legal representatives, were asked to participate in the study. Written and oral information were provided by a dentist, and participants were asked to give consent. There were no other inclusion criteria, and 277 residents were included in the study. This study includes preliminary results for 94 participants living in the four homes of one care society; the results have been published elsewhere after the use of a different statistical approach.20
Sociodemographic variables and dementia
Age, gender, number of diseases, and permanent medication were extracted from the care documentation. These variables were assessed to estimate the general condition of the participants. Cognitive impairment of the participants was evaluated using the MMSE.20 Examinations were performed by four psychologists trained in the memory clinic of the University of Heidelberg. Using the MMSE requires participants to solve 30 tasks devised to enable the assessment of cognitive and motor skills. Correctly performed exercises were awarded one point, whereas failed exercises were awarded zero. Scores could therefore range from 0 to 30; scores <24 were regarded as indicative of dementia, as recommended in several studies.20–23
Type of denture
Each participant underwent a comprehensive dental examination by two experienced dentists trained by investigation of elderly patients attending the Department of Prosthodontics, University of Heidelberg, before the start of the study. For the Revised Oral Assessment Guide (ROAG) used for estimation of dental treatment needs (see section ‘Dental treatment needs’) interexaminer reliability was studied (Cronbach’s alpha >0.9). Dental status, including number of natural teeth, type of denture, and denture-related treatment needs, was recorded for each participant. For analytical purposes, the type of denture was assigned to one of the following four categories: 1) edentulous without teeth replacement, 2) complete denture (CD), 3) removable dental prosthesis (RDP), and 4) natural teeth or fixed dental prosthesis (FDP). The type of denture worn was classified according to the weaker restored jaw.16 Denture-related problems were also assessed dichotomously (yes =1 and no =0).
Dental treatment needs
Dental treatment needs were evaluated using the ROAG. Saliva, swallow, speech, caries, mucosa, gums, denture retention, denture fitting, and denture condition were assessed dichotomously (0= healthy/1= treatment needed; maximum 12 points).24,25
OHRQoL assessment
The German version of the GOHAI was used to assess OHRQoL. Using the GOHAI requires participants to answer 12 questions related to pain and/or discomfort and physical and/or psychosocial function with regard to oral condition on a 5-point scoring scale (5= always, 4= often, 3= sometimes, 2= seldom, and 1= never). Questions 3, 5, and 7 are inversely scaled (1= always and 5= never). The final GOHAI score can therefore range from 12 to 60 points. Patients with a low GOHAI have a worse OHRQoL.12,26 In this study, the interviewers read the questions slowly. A copy of the questionnaire was also handed to the participants to enable them to read the questions themselves.
If the study dentist believed that the participant was unable to differentiate among the answer categories or gave invalid answers, the question was repeated. Such events were documented, and the results from these participants were excluded from statistical analysis (discussed in the “Results” section).
Statistical evaluation
Although the GOHAI scores were not normally distributed (Kolmogorov–Smirnov; P<0.15), the residuals did not violate the assumption of normality (P>0.15). Parametric statistics were therefore used to describe and analyze the data. For descriptive purposes, mean, standard deviation, and frequencies were used. In bivariate analysis of association of the target variables with GOHAI score, categorized variables were compared using unpaired t-tests or generalized linear mixed equations whereas continuous variables were analyzed using Pearson correlations. The effect on OHRQoL of prosthetic restoration adjusted for the dichotomized variables age, number of teeth, ROAG (median), gender, and dementia. GOHAI <50 was taken as indicative of very compromised OHRQoL,12 which was analyzed using two multivariate models, one for all participants and one for residents wearing removable dentures only, with the additional factor conditions. Statistical analysis was performed using SPSS Version 23.0 (IBM Corporation, New York, NY, USA). The level of probability for local statistical significance was set to P<0.05.
Results
Of the 277 participants initially included, 74 participants had to be excluded because they did not complete the GOHAI questionnaire (two participants were mute and 72 participants were unable to give valid answers to the questions). Thirty-four other participants had to be excluded from statistical analysis because of missing MMSE values. Thus, complete data for 169 participants were available for final analysis. The mean (SD) age of the study population was 82.9 (8.9) years. The majority of the participants were female (67%), and ~70% of the sample was living with dementia. The mean number of diseases was 3.5 (2.2), and the mean number of permanently taken medication was 6.7 (3.4). These variables reveal to a compromised general condition of the participants. The mean GOHAI score for the sample was 49.1 (8.3), and 70 participants (41%) had a GOHAI score of <50, which is indicative of compromised OHRQoL. The mean number of natural teeth was 8.3 (8.9); 32 participants wore an FDP, 37 participants wore removable partial dentures, and 90 participants wore CDs in at least one jaw. Ten participants were edentulous without teeth replacement in at least one jaw. The need for denture-related treatment among the sample was high (64%). Detailed data and results from bivariate comparisons of the participants’ characteristics are listed in Table 1.
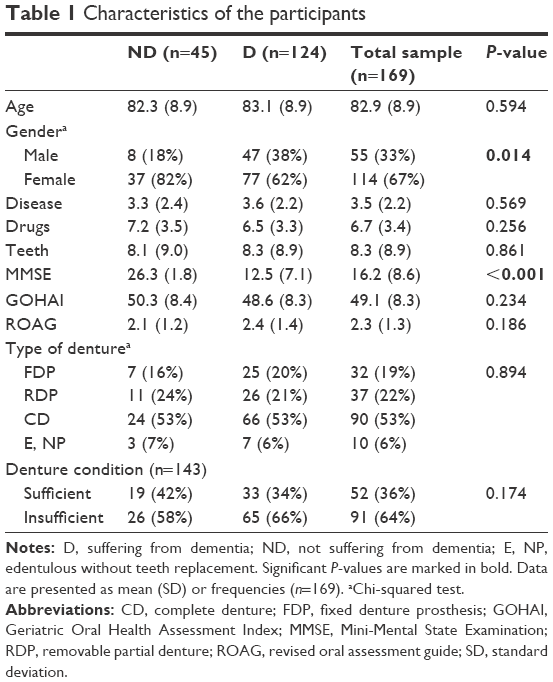 | Table 1 Characteristics of the participants |
Bivariate associations with OHRQoL
OHRQoL was significantly associated with the type of prosthetic restoration, with a linear decrease in OHRQoL from FDP, RPD, and CD to NP (P<0.001). The number of natural teeth (P<0.001) and the amount of dental treatment needed, as measured by mean values of the ROAG (P=0.049), also significantly affected OHRQoL. For denture wearers (n=137; 81%), a significant association of denture conditions (denture-associated treatment needs) with GOHAI was detected (P=0.013). None of the other comparisons of GOHAI scores between the target variables reached statistical significance (P>0.05). Detailed results from these analyses are listed in Table 2.
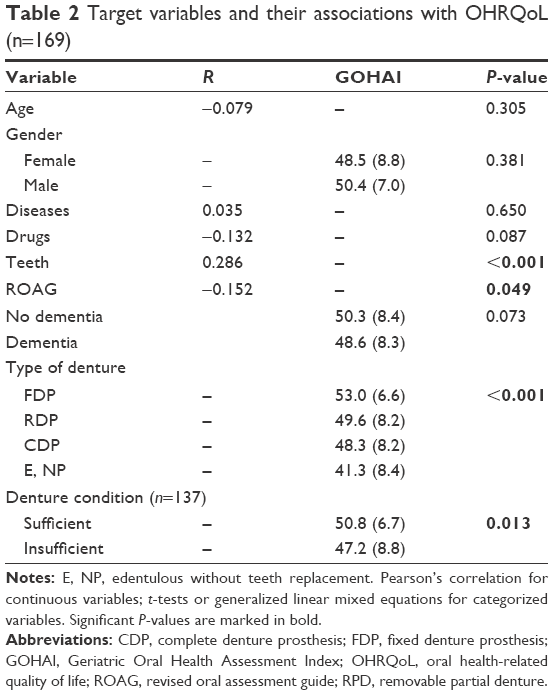 | Table 2 Target variables and their associations with OHRQoL (n=169) |
Multivariate associations with OHRQoL
The logistic regression model for all participants (n=169) revealed a 6.5-fold risk (95% CI 1.3–32.4) of extremely compromised OHRQoL (GOHAI <50) among edentulous subjects without prosthetic restorations (P<0.023). Furthermore, having fewer than five natural teeth independently doubled the risk of low OHRQoL (P<0.036). None of the other confounders reached statistical significance (P>0.05, Table 3). The regression model for denture wearers only (n=137) revealed a lower risk of reduced OHRQoL for participants older than the median (P=0.028). A ~2.5-fold risk of compromised OHRQoL was detected for participants with denture-related treatment needs (P=0.024). None of the other confounders, including the number of natural teeth, was found to affect OHRQoL (Table 4).
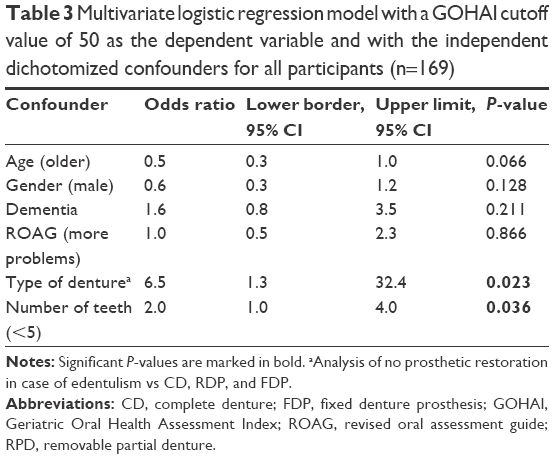 | Table 3 Multivariate logistic regression model with a GOHAI cutoff value of 50 as the dependent variable and with the independent dichotomized confounders for all participants (n=169) |
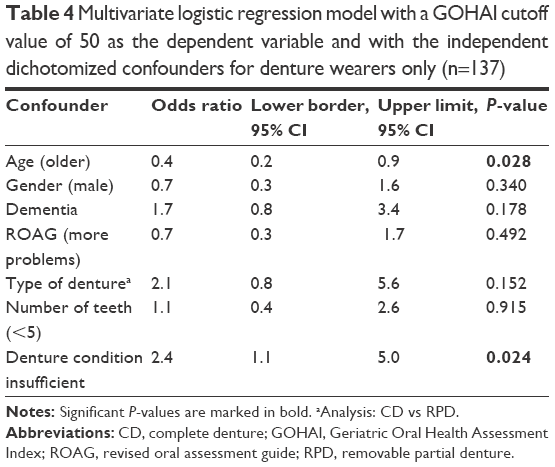 | Table 4 Multivariate logistic regression model with a GOHAI cutoff value of 50 as the dependent variable and with the independent dichotomized confounders for denture wearers only (n=137) |
Discussion
The results of this study suggest that better oral health (more natural teeth and adequate prosthetic restorations), especially, is positively associated with acceptable OHRQoL.
OHRQoL found in this study was usually substantially lower than that documented in previous studies investigating community-dwelling elderly;25,26 this may be explained by the study of a specifically compromised nursing home sample facing a variety of dental treatment needs. Reduced OHRQoL might also be because the nursing home residents are provided with extensive prosthetic restorations, which can result in functional and esthetic compromises compared with natural dentition or fixed dental prostheses. In our recent study, 59% of the participants were edentulous in at least one jaw and 6% of the participants were edentulous without teeth replacement. In contrast, community-dwelling elderly have more teeth and a better prosthetic status than old people in nursing homes.27,28
The relevance of prosthetic status to OHRQoL has, however, been proved for different communities, including young adults and community-dwelling elderly.15,29 Accordingly, the most important reasons for better OHRQoL in this recent sample were dental in nature. With increasing number of natural teeth and the presence of FDP, higher OHRQoL was observed. These findings are also in accordance with those of Tramini et al,14 who also investigated a nursing home population (although the OHRQoL of participants in that study was not as compromised as in this recent study). In our study, participants with FDP had the highest OHRQoL, with a linear decrease from those with RDP and CDs to those who were edentulous and without dentures. This finding is not surprising and confirms our preliminary results for a smaller cohort of 94 participants published elsewhere.20 With loss of teeth, chewing ability also can be limited. Studies investigating masticatory performance revealed that chewing efficiency decreases from patients wearing FDP to those wearing RPD and CDP.30–32 Reduced masticatory performance also affects food selection and can even result in a requirement for food with a mushy consistency. In this context, one should also consider that eating is an important social event and extremely meaningful as a constant daily routine for seniors in a nursing home.16 These results were confirmed by multivariate analysis; a 6.5-fold risk of extremely compromised OHRQoL (GOHAI <50) was, moreover, proved for edentulous people with no tooth replacement. However, the significant differences between wearing CD and RDP could not be reproduced in multivariate analysis, albeit there is a trend to a higher risk for those with CD (P=0.152). One might speculate that a possible difference between these groups can only be proved using a higher sample size.
Denture-related treatment needs also significantly affected OHRQoL. First, poorly fitting and less retentive dentures are associated with reduced chewing efficacy; second, bad denture condition results in psychological and social problems, which also affect OHRQoL. In this study, the need for denture-related treatment was higher (64%) but comparable to those detected in previous studies.2,19 Although the number of general dental treatment needs, as measured using the ROAG, was associated with OHRQoL in bivariate analysis, this effect could not be confirmed by multivariate analysis. This finding is, nevertheless, in accordance with previous reports indicating discrepancies between objectively measured oral health (eg, gingivitis) and OHRQoL, especially among the elderly. OHRQoL is based on effects on daily performance, and some oral problems (eg, oral neglect) are asymptomatic or of minor significance in comparison with general health problems.
The finding that greater age is positively associated with better OHRQoL is in a similar direction. Interestingly, people with or without dementia had a comparable OHRQoL, even though objectively measured health indicators are frequently indicative of worse oral health (eg, periodontitis and caries) among subjects living with dementia, as reported in the literature.19,33,34 In our recent study, however, comparable dental and prosthetic statuses and prevalence of dental treatment needs were observed among those with or without dementia, leading to similar OHRQoL. Similar levels of OHRQoL among demented and “healthy” elderly people have also been detected in previous studies.19,35
Strength and weaknesses of the study
Dropout of ~40% in this study suggests caution in interpretation and generalization of the results. Participants were, perhaps, more interested in their health than nonresponders. It is also conceivable that some of the subjects participated in the study because they had acute dental problems. The sample is, however, a sub-population from a large, representative interdisciplinary study initiated by the Ministry of Social Affairs of the state of Baden-Württemberg, Germany. All potential residents of the participating nursing homes who gave written informed consent were included in the study (irrespective of cognitive status and care needs). It should be recognized that the comprehensive medical, psychological, and dental examinations were time-consuming (~2 h), which definitely led to concerns about participation in many cases. It should also be remembered that self-assessments of oral health by elderly subjects with dementia were performed in this study; this may not be consistently accurate and may lead to underestimation of oral problems. OHRQoL was, however, assessed using the GOHAI, which has been reported to enable more successful and sensitive detection of oral problems among compromised elderly populations than using the OHIP.13 In addition, the ability of the participants to give valid answers was confirmed by the interviewers in all cases. Each participant was asked the GOHAI questions and received the questionnaire to read, to reduce the possibility of bias. (As a consequence, results from 74 participants were excluded from statistical analysis.) We also stress that all dental examinations were performed by two dentists experienced in epidemiological surveys who received comprehensive training before the start of the study and tested their reliability in ROAG assessments.
Conclusion
Among nursing home residents, OHRQoL and oral health conditions are severely compromised, and the need for denture-related treatment is high.
Dental and prosthetic conditions have a substantial effect on OHRQoL. Prevention of tooth loss at an early stage and denture-related treatments (adjustment of dentures) seem to be important to maintain high OHRQoL among the aged nursing home populations. Because measurement of OHRQoL might not fully capture objective oral health conditions for people with cognitive impairment or dementia, oral health should be periodically monitored. Frequent dentists’ visits to nursing homes would be desirable to prevent deterioration of oral conditions. Longitudinal studies are encouraged to confirm these results with a higher level of evidence.
Acknowledgments
We are grateful to all the participants in this study for their patience and to Altenpflegeheime Mannheim GmbH for their considerable support. We thank the Ministry of Social Affairs of Baden-Württemberg (Sozialministerium Baden-Württemberg) for financial support of the study. We also thank Ian Davis, copy editor, for English language revision.
Author contributions
Anna-Luisa Klotz was responsible for data input and drafted the article. Alexander Jochen Hassel and Andreas Zenthöfer contributed to the study design and management. Johannes Schröder and Peter Rammelsberg critically revised the article. All authors contributed toward data analysis. All authors have read and approved the final article to be published. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Adam H, Preston AJ. The oral health of individuals with dementia in nursing homes. Gerodontology. 2006;23(2):99–105. | ||
Montal S, Tramini P, Triay JA, Valcarcel J. Oral hygiene and the need for treatment of the dependent institutionalised elderly. Gerodontology. 2006;23(2):67–72. | ||
Zenthofer A, Dieke R, Dieke A, Wege KC, Rammelsberg P, Hassel AJ. Improving oral hygiene in the long-term care of the elderly – a RCT. Community Dent Oral Epidemiol. 2013;41(3):261–268. | ||
Wang TF, Huang CM, Chou C, Yu S. Effect of oral health education programs for caregivers on oral hygiene of the elderly: a systemic review and meta-analysis. Int J Nurs Stud. 2015;52(6):1090–1096. | ||
Adachi M, Ishihara K, Abe S, Okuda K. Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. Int J Dent Hyg. 2007;5(2):69–74. | ||
Awano S, Ansai T, Takata Y, et al. Oral health and mortality risk from pneumonia in the elderly. J Dent Res. 2008;87(4):334–339. | ||
Juthani-Mehta M, De Rekeneire N, Allore H, et al. Modifiable risk factors for pneumonia requiring hospitalization of community-dwelling older adults: the Health, Aging, and Body Composition Study. J Am Geriatr Soc. 2013;61(7):1111–1118. | ||
Scannapieco FA, Rethman MP. The relationship between periodontal diseases and respiratory diseases. Dent Today. 2003;22(8):79–83. | ||
Micheelis W, Hoffmann T. Vierte Deutsche Mundgesundheitsstudie – (DMS IV): Neue Ergebnisse zu oralen Erkrankungensprävalenzen, Risikogruppen und zum zahnärztlichen Vorsorgungsgrad in Deutschland 2005. Köln: Dt. Ärzte-Verl; 2006. | ||
Adams R. Qualified nurses lack adequate knowledge related to oral health, resulting in inadequate oral care of patients on medical wards. J Adv Nurs. 1996;24(3):552–560. | ||
Callahan D. The WHO definition of ‘health’. Stud Hastings Cent. 1973;1(3):77–88. | ||
Atchison KA, Dolan TA. Development of the geriatric oral health assessment index. J Dent Educ. 1990;54(11):680–687. | ||
El Osta N, Tubert-Jeannin S, Hennequin M, Bou Abboud Naaman N, El Osta L, Geahchan N. Comparison of the OHIP-14 and GOHAI as measures of oral health among elderly in Lebanon. Health Qual Life Outcomes. 2012;10:131. | ||
Tramini P, Montal S, Valcarcel J. Tooth loss and associated factors in long-term institutionalised elderly patients. Gerodontology. 2007;24(4):196–203. | ||
John MT, Koepsell TD, Hujoel P, Miglioretti DL, LeResche L, Micheelis W. Demographic factors, denture status and oral health-related quality of life. Community Dent Oral Epidemiol. 2004;32(2):125–132. | ||
Hassel AJ, Koke U, Schmitter M, Rammelsberg P. Factors associated with oral health-related quality of life in institutionalized elderly. Acta Odontol Scand. 2006;64(1):9–15. | ||
Inukai M, John MT, Igarashi Y, Baba K. Association between perceived chewing ability and oral health-related quality of life in partially dentate patients. Health Qual Life Outcomes. 2010;8:118. | ||
Zenthofer A, Rammelsberg P, Cabrera T, Schroder J, Hassel AJ. Determinants of oral health-related quality of life of the institutionalized elderly. Psychogeriatrics. 2014;14(4):247–254. | ||
Ribeiro GR, Costa JL, Ambrosano GM, Garcia RC. Oral health of the elderly with Alzheimer’s disease. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(3):338–343. | ||
Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. | ||
Velayudhan L, Ryu SH, Raczek M, et al. Review of brief cognitive tests for patients with suspected dementia. Int Psychogeriatr. 2014;26(8):1247–1262. | ||
Almeida OP. [Mini mental state examination and the diagnosis of dementia in Brazil]. Arq Neuropsiquiatr. 1998;56(3b):605–612. Portuguese. | ||
Tombaugh TN, McIntyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–935. | ||
Andersson P, Hallberg IR, Renvert S. Inter-rater reliability of an oral assessment guide for elderly patients residing in a rehabilitation ward. Spec Care Dentist. 2002;22(5):181–186. | ||
Hassel AJ, Leisen J, Rolko C, Rexroth W, Ohlmann B, Rammelsberg P. [Clinical assessment of oral health between physician and dentist – a pilot study on inter-examiner reliability]. Z Gerontol Geriatr. 2008;41(2):132–138. German. | ||
Hassel AJ, Rolko C, Koke U, Leisen J, Rammelsberg P. A German version of the GOHAI. Community Dent Oral Epidemiol. 2008;36(1):34–42. | ||
Moriya S, Tei K, Murata A, Muramatsu M, Inoue N, Miura H. Relationships between Geriatric Oral Health Assessment Index scores and general physical status in community-dwelling older adults. Gerodontology. 2012;29(2):e998–e1004. | ||
Esmeriz CE, Meneghim MC, Ambrosano GM. Self-perception of oral health in non-institutionalised elderly of Piracicaba city, Brazil. Gerodontology. 2012;29(2):e281–e289. | ||
Abud MC, Figueiredo MD, dos Santos MB, Consani RL, Marchini L. Correlation of prosthetic status with the GOHAI and TMD indices. Eur J Prosthodont Restor Dent. 2011;19(1):38–42. | ||
Rissin L, House JE, Manly RS, Kapur KK. Clinical comparison of masticatory performance and electromyographic activity of patients with complete dentures, overdentures, and natural teeth. J Prosthet Dent. 1978;39(5):508–511. | ||
Schimmel M, Katsoulis J, Genton L, Muller F. Masticatory function and nutrition in old age. Swiss Dent J. 2015;125(4):449–454. | ||
Wayler AH, Muench ME, Kapur KK, Chauncey HH. Masticatory performance and food acceptability in persons with removable partial dentures, full dentures and intact natural dentition. J Gerontol. 1984;39(3):284–289. | ||
Zenthofer A, Schroder J, Cabrera T, Rammelsberg P, Hassel AJ. Comparison of oral health among older people with and without dementia. Community Dent Health. 2014;31(1):27–31. | ||
Avlund K, Holm-Pedersen P, Morse DE, Viitanen M, Winblad B. Tooth loss and caries prevalence in very old Swedish people: the relationship to cognitive function and functional ability. Gerodontology. 2004;21(1):17–26. | ||
Walker RJ, Kiyak HA. The impact of providing dental services to frail older adults: perceptions of elders in adult day health centers. Spec Care Dentist. 2007;27(4):139–143. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.