")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 11
Oral health in patients with Prader-Willi syndrome: current perspectives
Authors Bantim YCV, Kussaba ST, Carvalho GP, Garcia-Junior IR, Roman-Torres CVG
Received 5 February 2019
Accepted for publication 10 June 2019
Published 4 July 2019 Volume 2019:11 Pages 163—170
DOI https://doi.org/10.2147/CCIDE.S183981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Christopher E. Okunseri
Yasmin Comoti Vita Bantim,1 Sérgio Takashi Kussaba,2,3 Gilberto Paiva de Carvalho,4 Idelmo Rangel Garcia-Junior,1 Caio Vinícius Gonçalves Roman-Torres3
1Department of Surgery an Integrated Clinic, Araçatuba School of Dentistry, São Paulo State - University Unesp, Araçatuba, SP, Brazil; 2Department of Dentistry, Cathedral College, Boa Vista, RR, Brazil; 3Department of Dentistry, University Santo Amaro, São Paulo, SP, Brazil; 4Nursing College, Center of Health Science – Federal University of Roraima, Boa Vista, RR, Brazil
Abstract: Prader-Willi syndrome (PWS) is a rare complex multisystem disorder and presents several aspects related to dentistry. The purpose of this review is to present current perspectives about oral health in patients with PWS. Delay development, hyperphagia, foamy and highly viscous saliva raise the risk of caries and contribute to tooth wear. Cariogenic foods uncontrolled consumption allows to obesity and dental problems progress worsening systemic disorders. These factors can be controlled. The success in follow-ups with caries free and oral health controlled demonstrate the importance of multidisciplinary team intervention corroborated by support at home from birth to adulthood. Thereby, current perspective on the disease is that there is possibility of proper maintenance of oral health in PWS patients. Guided care interferes positively with the overall well-being and quality of life of the individual with PWS and their family. A multidisciplinary team with a focus on teaching patients and family members will help minimize eventual problems.
Keywords: Prader-Willi syndrome, oral health, patient care management
Introduction
Prader-Willi syndrome (PWS) presents odontological aspects of interest. Many deleterious effects on the oral cavity were associated with this behavioral and endocrine disorder that may cause surgery and/or worsening of the clinical condition.1
History
First described by Dr. Langdom Down in 1887, it was named “polysardia” and documented by Andrea Prader, Heinrich Willi, and Alexis Labhart in 1956.2 Besides Prader-Willi syndrome, others scientific names are Willi-Prader syndrome, Prader-Labhart-Willi syndrome,3,4 and Prader-Labhart-Willi-Fanconi’s syndrome.4
Definition, prevalence and, genetics
PWS is a complex and rare multisystem disorder,5 it occurs at a similar prevalence between genders with an incidence of 1/15,000 to 1/25,000.6 A lack of expression of Paterno’s gene in chromosome 15q11–q135,7–11 causes PWS, and it is characterized by hypothalamic dysfunction.7
Genetic testing is performed to confirm the diagnosis.11 There is a relationship between the clinical characteristics and the age range of the PWS carrier. This criterion is used to facilitate the analysis for the later request of DNA tests (Table 1). Feeding problems are a feature in infancy whereas hypogonadism is a problem in adolescence.12
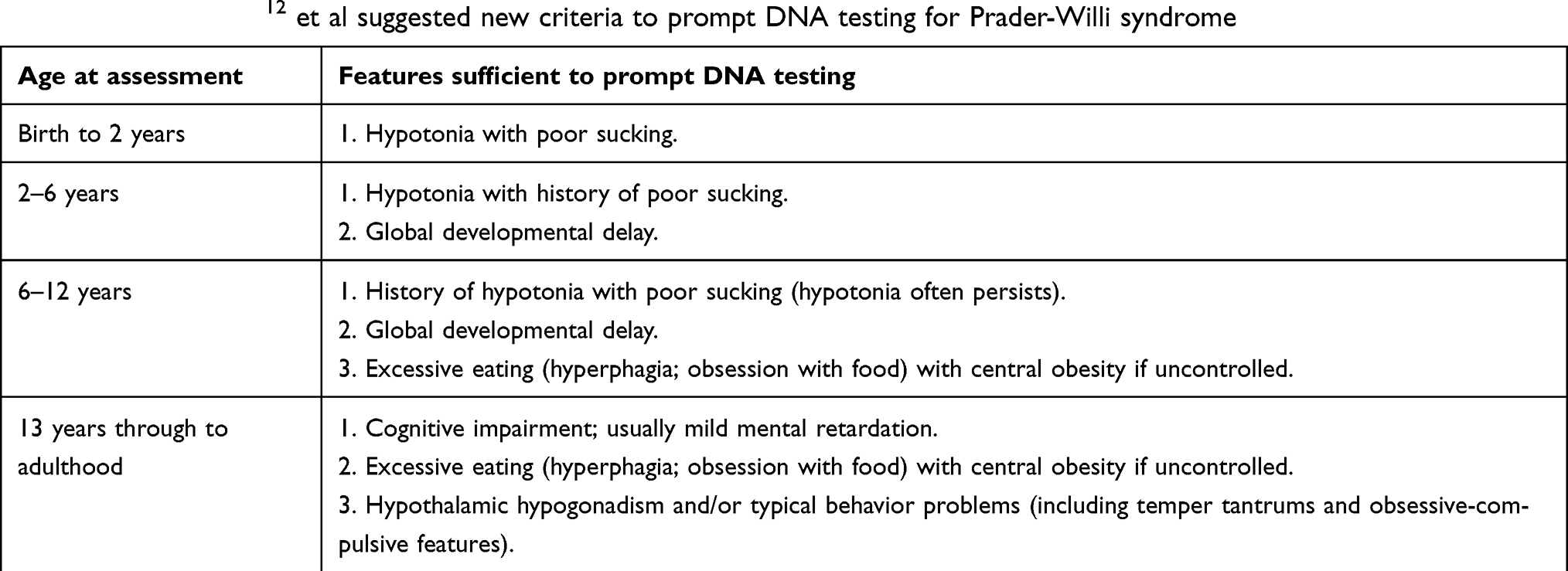 |
Table 1 Gunay-Aygun12 et al suggested new criteria to prompt DNA testing for Prader-Willi syndrome |
General signs and symptoms
In general, hypotonia, dysmorphic appearance obesity,9,13 hypogonadism, osteoporosis and bone density, short stature,9,13–15 hypothyroidism, adrenal insufficiency, and sleep disorders are features observed.14,15 This syndrome is the first human genomic imprinting disorder. It is one of the most common microdeletion syndromes which causes genetic obesity. A multidisciplinary approach should be employed in the management of PWS patients.16
PWS presents with variations between its carriers, changes that are manifested throughout the life of the individuals themselves. Systemic diseases may be discretely influenced by the effects of PWS directly or indirectly, reaching the nervous, cardiovascular, musculoskeletal, respiratory, gastrointestinal, or urinary tract systems.17
Newborn features (age at assessment: from birth to 2 years)
Neonates with PWS present with characteristics such as hypotonia, poor responsiveness, feeding difficulty, and infrequent and weak crying were observed. All the patients exhibited typical facial features like a prominent forehead, almond-shaped eyes, a downturned mouth, a narrow face, a thin upper lip, a micro-mandible, a small mouth,9,17,18 downturned angles of the mouth with abundant and thick saliva, and small hands and feet. Global developmental delays and feeding problems due to hypotonia are present in the newborn.5
Childhood features (age at assessment: 2–6 years and 6–12 years)
Age at assessment in childhood is divided into two periods: 2–6 years old and 6–12 years old. In this phase, short stature, small hands, and feet, developmental delay and hypogonadism occur sequentially.9,17 The presence of high-grade hypotonia and limitations in feeding stimulate the onset of morbid obesity and consequently diabetes,19 if uncontrolled.8,9,17
Teenager to adulthood features (age at assessment: 13 through to adulthood)
Behavioral problems and hyperphagia become more prevalent during adolescence. The adulthood is marked by behavioral problems and obesity systemic complication,5 increasing mortality causing hypoventilation and obesity because of hypothalamic dysfunction.14
Hypogonadism/delayed puberty, central adrenal insufficiency (CAI), hypothyroidism, bone density, growth hormone deficiency (GHD), diabetes, obesity, and sleep apnea are clinical problems during the transition period in PWS when chronic patients pass the pediatric age and become adults.20
Facial repercussions
Repercussions such as a micro-mandible and a small mouth,18 facial features, hypotonia as a cause9,13 of sleep disorders,14,15 mouth breathing,21 feeding difficulties in neonates18 and drooling22 are general characteristics of patients with PWS related to dental care. Thus, the purpose of this review is to present current perspectives about oral health in patients with Prader-Willi syndrome.
Oral manifestations
The oral clinical features present in PWS attract a lot of attention in dentistry. Hypotonia can explain the asymmetry in facial expressions and low function in clenching the teeth,22 it affects the ability to articulate words, the rate of speech, the quality of the voice by reduced oral motor skills and contributes to poor speech-sound development.23,24 This fact changes the normal oral mechanism, limiting sucking, chewing, and swallowing. Hyperphagia is present and stimulates the ingestion of food, allowing a greater consumption of soft carbohydrates.16 Another finding was constant drooling in almost half of the patients.22
A variety of oral diseases are found in patients with PWS (Table 2) such as caries,1,17,21,25–31 hypoplastic enamel,1,17,25,28,31 viscous saliva,1,17,21,25,30–32 periodontal disease,25–28 tooth wear,1,26,27,31,32 dental erosion,33 rampant caries,1,29,31 oral microsomia,25,31 dental malocclusion,1,17,21,26–29 candidiasis,25,27 erythematous lesions of the oral mucosa,27 increased biofilm accumulation,1,21,25,31,32 gingivitis,1,25,27,31,32 angular cheilitis, dry mouth,28 demineralization,21,25,31 dentoalveolar abscess,29,31 hypotonic tongue,21,31 mouth breathing,21,31,32 root stumps30 and a delay in tooth eruption.28
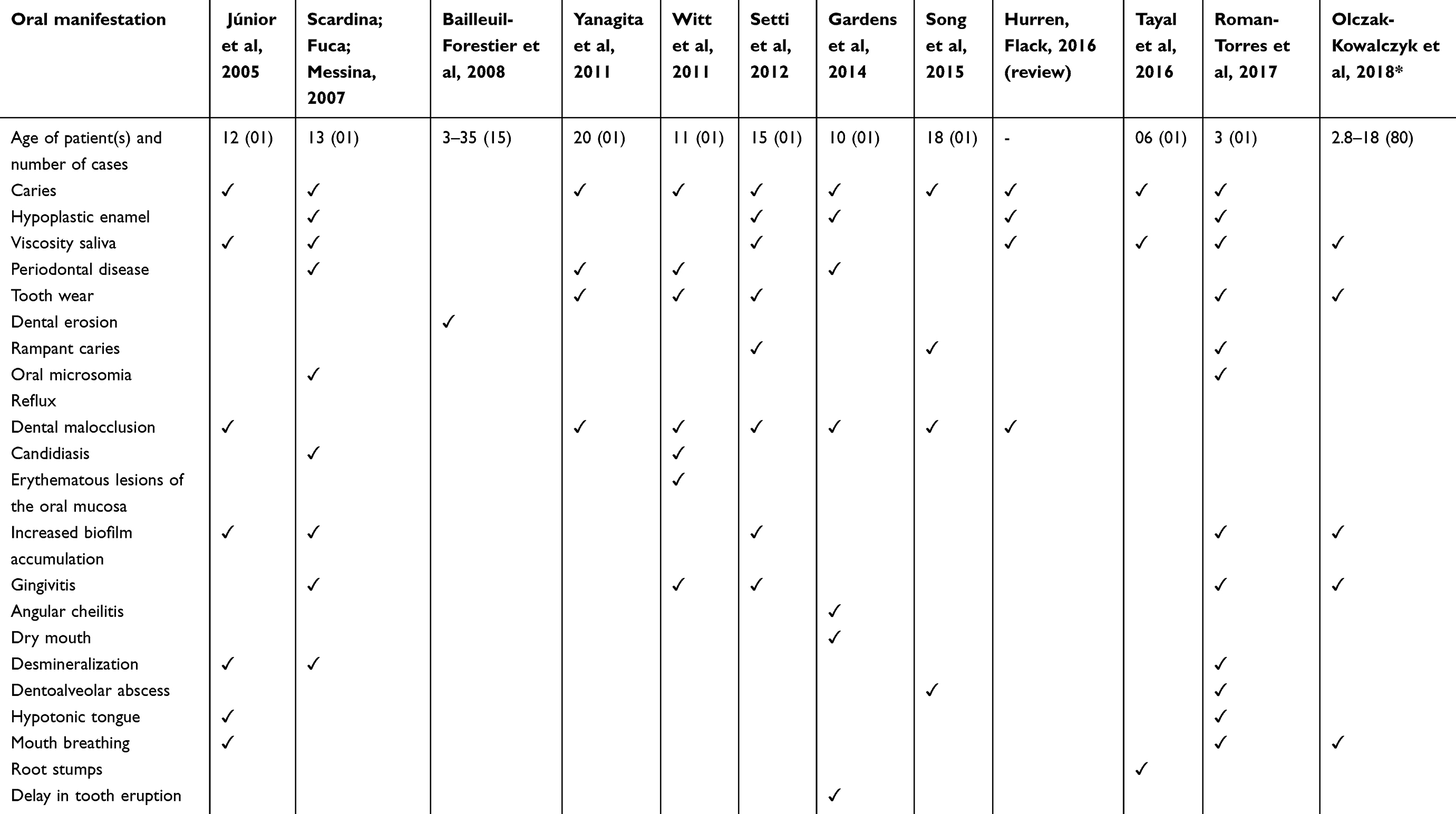 |
Table 2 Oral manifestation, reference |
Salivary abnormalities
PWS patients have low salivary production.34,35 Consequently, the quantity and quality of saliva can increase the risk of caries.16 It is unknown whether saliva consistency on drooling and on the forming of a bolus influence swallowing since it is viscous and foamy in these individuals.22 Investigating salivary flow rates and assessing whole salivary total protein in individuals with PWS showed that the saliva was viscous containing MUC7 (mucin-7 protein) and a high level of total protein when compared with healthy individuals. The groups were divided into unstimulated whole saliva (UWS), stimulated whole saliva (SWS), submandibular/sublingual (SS), and parotid saliva (PS). The production of all proteins was similar between PWS and the control group. However, total protein and MUC7 concentrations in UWS were higher in the PWS group. This result indicated that the syndrome affects the fluid and protein secretion mechanisms differently.36
Viscous and thick saliva in PWS patients contributes to poor speech-sound development.10 Thick and viscous saliva with a reduced volume results in dry mouth facilitating articulation problems and dental caries.9 A recent study observed that gingivitis and dental wear in children and adolescents with PWS presented with an etiology from changes in saliva. More viscosity, minor salivary secretion, and mouth breathing are components that predispose patients to the risks of plaque inducing gingivitis and tooth wear.32 Abnormal salivary fluid influences enamel loss, caries, and dental erosion. Ingesting highly acidic drinks, occlusal parafunction, and poor oral care habits make patients susceptible to intense tooth wear.37
Periodontal and dental implications
A case report described a 20-year-old man with PWS with localized periodontitis. Occlusal trauma, tooth malposition, and crowding blended with poor plaque control led to periodontal pathology. It appeared that plaque was the primary etiology and malocclusion made the case worse.26 Besides this, delayed tooth eruption in a 10-year-old boy was observed to conform with periapical and panoramic radiographic examination.28 Delayed healing of wounds was reported after the extraction of teeth.30
A combination of abrasion, attrition, and erosion or each isolate condition may cause tooth wear. Intraoral photographs in 49 individuals with PWS were evaluated indicated tooth wear associated with tooth grinding. There was a relationship with wear and erosion. While the occlusal surface was affected by wear, erosion caused the loss of substance in the non-occlusal free surfaces. The need for prosthodontic rehabilitation in young adults with PWS is important since there is often dental attrition and wear.35
In a recent study, the microscopic structure of enamel and dentine in primary and permanent teeth from individuals with PWS was described using scanning electron microscopy (SEM), microradiography, and light microscopy. These structures were normal with the exception of a slight increase in interglobular dentin (IGD), which is probably of minor clinical significance. Severe gastroesophageal reflux was confirmed in three individuals that had reflux assessment analyzed by esophageal pH monitoring. This disease needs more investigation in these patients.38
Treatment under general anesthesia
The cases reported cooperation by the patient with PWS.26,27 However, poor cooperation encourages conscious sedation29 or general anesthesia.29,31 Stubbornness, aggression, temper tantrums, and impulsivity were observed in an 18-year-old PWS patient in the first oral intervention. Emergency treatment of the traumatic injury, a crown fracture of the maxillary central incisors caused by a fall with pulp involvement were planned. Other treatments were made under general anesthesia.29
Another case reported a 3-year-old child with PWS exhibiting mood swings, bouts of aggressiveness towards their family, and self-injurious behavior when contradicted. Signs of resistance to some verbal commands were noticed in the initial dental attendance. After frustrating attempts to execute an additional examination of the periapical radiographs, dental treatment under general anesthesia was proposed, allowing an adequate observation of the oral environment in a single session.31
PWS patients have a higher anesthesiologic risk.5,29 Airway management is difficult due to scoliosis, a high palatal vault, and micrognathia. Hypotonia causes the possibility of delayed recovery of spontaneous respiration.29 Dense salivation can compromise the airway patency, especially during extubation,5,39 as well as thermoregulation control and an exaggerated response to hypnotic drugs. Such features are more severe in obese patients who may present with obstructive apnea, right ventricular hypertrophy, and pulmonary hypertension. Cardiac and respiratory evaluation is suggested.5
Clinical follow up of patients with PWS
There is great clinical variability in this multigenic pathology. The features change over the course of life in each patient. Four age classes can be identified considering all the lifelong problems patients might have: from birth to 3 years, from 3 to 10 years, from 10 to 18 years and adulthood.5 The pediatric and adult team must be synchronized to negotiate the transitional period. Previous guidelines should guarantee continuity, flexibility, and care focused on the patient.20
An early diagnosis with preventive interventions is necessary.9,18,25,29,33,40 A combination of medical and daily routine management should be established in PWS patients to improve their quality of life.41 Health education and extensive information about PWS must be given to the parents (Table 3). Nutritional instruction and feeding control, preventing suffocation, physiotherapy for functional motor disorders are factors that contribute to good health.18 When a diagnosis of PWS is confirmed, an orofacial evaluation should be performed to facilitate the treatment.22
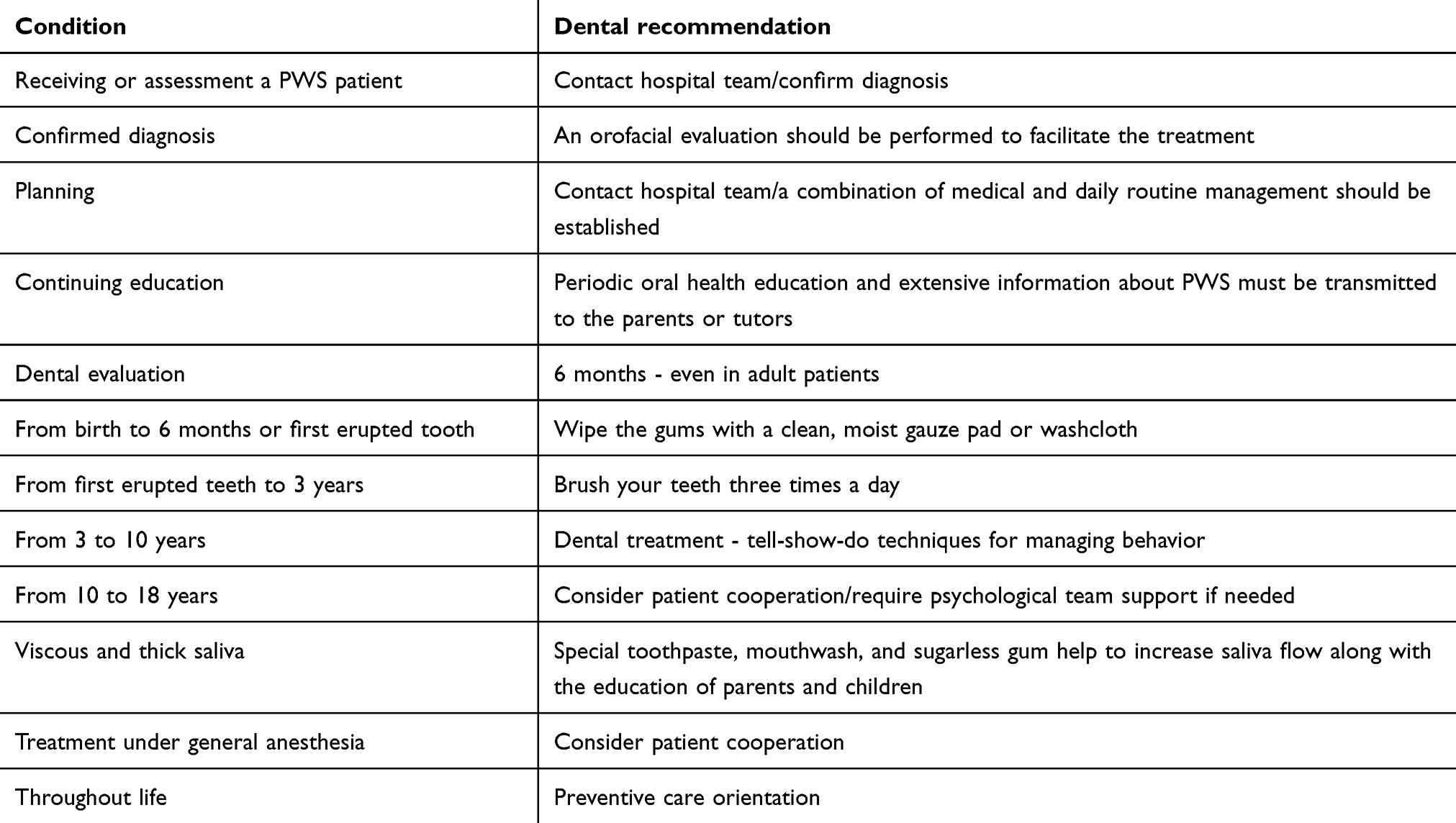 |
Table 3 Condition and dental recommendation for the Prader-Willi syndrome (PWS) patient |
Recent surveys have described PWS in individuals with satisfactory oral health when compared with previous studies that related caries indices and enamel defects.33 Education of parents and children must be applied because of low salivary production. Increased salivary flux could be done by stimulatory products. Drinking and feeding controls prevent dental complications, and orthodontic intervention is needed.5 An uncontrolled diet and infant hyperphagia caused obesity in the PWS patients.5 The disordered consumption of cariogenic foods and motor limitations leads to an increase in oral problems. Oral problems induce general harm in PWS patients.
Even though some centers are successful in maintaining satisfactory dental conditions,33,36 other studies reported episodes of caries,1,21,25–31 rampant caries, and gingivitis.1,29,31 There was also a report of a patient with PWS who needed hospitalization due to pneumonia and subsequent referral to ICU for mechanical ventilation with a diagnosis of septic shock secondary to hospital pneumonia.1 An integrated multidisciplinary approach starting from the neonatal period is mandatory20 to greatly improve the health and quality of life in children with PWS.40 Dental care assessment needs to be done from 3 months to adolescence and adulthood.9
Dental orientation care, use of topical fluoride, periodic checkups, preventive measures when primary dentition erupt, dental treatment when necessary, and oral hygiene supervised by parents or tutors, according to the patient’s cognitive ability and collaboration.34
These interventions were noted in nine subjects investigated with an oral cavity free of caries among fifteen individuals due to the early multidisciplinary health support network interventions.33 Success in maintaining overall health and good oral status is based on a multidisciplinary work with adequate information on eating, behavioral disorders, and a successful transition from childhood to adulthood.20 A tremendous effort is required by caregivers to control the PWS patients’ weight. A supporting team must be prepared to encourage performance.14
The presence of dental plaque is an indication of gingivitis. The features of saliva features also influence and makes it difficult to clean the teeth. Viscosity and poor salivary flow are factors for dental plaque accumulation and gingivitis.32 Normal salivation has been shown to be crucial in protecting teeth against the acidic factors that initiate dental erosion through its buffering capacity, clearance by swallowing, pellicle formation, and remineralization of demineralized enamel.37
Consistent patient care improves the daily and medical situation of PWS patients. Controlling weight led to improvements in blood pressure and metabolic condition. Thus, assisted supervision and conservative treatments are favorable in PWS patients.41 In this way, adequate home care orientation can be powerful in preventing oral problems. Providing oral health care for children with Prader-Willi Syndrome – particularly teenagers – is a difficult task.27 Temper tantrums, obsessive-compulsive disorder, and stubbornness21,27,29–31 affect oral care. Behavioral and emotional disorders, especially attachment to fixed routines and stubbornness, require attention and patience from the dental surgeon and the assisting personnel.27
Behavior and learning problems appear when PWS individuals reach adolescence needing more influence from their parents. Egocentric, angry, mood-labile, stubborn, persistent, and rage episodes arise in PWS adolescents. Feeding disorders are intensify regarded by psychiatric problems.11,42
The pediatric dentist must be knowledgeable about this condition to confirm a diagnosis, prevent any adverse drug effects, medical problems, and to do a suitable preventive plan. The team needs to develop dietary guidelines.33 Health care of PWS patients needs to involve all contributors to promote appropriate transition and continued care. The medical team and parents must share information and be present in meetings, interacting for the well-being of the patient.20
Many oral pathologies are associated with PWS such as caries, hypoplastic enamel, viscous saliva, periodontal disease, and tooth wear. It is necessary to incorporate systematic prevention and monitoring of these patients to minimize any possible illness.43 The family needs instructions regarding proper oral hygiene, to make them also responsible for the treatment, even if the patient is followed-up in a dental care program.28 Special toothpaste, mouthwash, and sugarless gum help to increase saliva flow along with the education of the parents and children. The sensibility to thirst of PWS individuals is lower and increases the risk of dehydration. Regular daily drinking prevents this fact and assists in oral care.44
Regular dental checkups, adequate oral hygiene, and parent-orientated care reduce the risk of oral diseases. Information is the key to success in patients with PWS. The multidisciplinary team must be alert and prepared for intervention with the family giving extensive information to them.
The impact of the parent training program for the management of children and adolescents with PWS on the mental health of caregivers was analyzed in four phases: pre-intervention, intervention, post-intervention, and follow-up. There was an improvement in the indicators of emotional difficulties of mothers, seized identify, and to manage factors that harmed the physical health, behavior, and school learning of the children and the need to involve other family members in child care.45
Conclusion
The success in follow-ups with caries free and oral health control demonstrate the importance of multidisciplinary team intervention corroborated by support at home from birth to adulthood. Thereby, a current perspective on the disease is that there is the possibility of proper maintenance of oral health in PWS patients. Guided care positively interferes with the overall well-being and quality of life of the individual with PWS and their family. A multidisciplinary team with a focus on teaching patients and family members will help minimize eventual problems.
Disclosure
The authors report no conflicts on interest in this work.
References
1. Setti JS, Pinto SF, Gaetti-Jardim EC, Manrique GR, de Mendonça JCG. Assistência multiprofissional em unidade de terapia intensiva ao paciente portador de síndrome de Prader-Willi: um enfoque odontológico. Rev Bras Ter Intensiva. 2012;24(1):106–110. doi:10.1590/S0103-507X2012000100016
2. Gilbert P. Prader-Willi syndrome. In: Gilbert P, ed. The A-Z Reference Book of Syndromes and Inherited Disorders. Boston, MA: Springer;1996:236–237. doi:10.1007/978-1-4899-6918-7_62
3. Pagliano Sassi L, Quarti M. The Prader-Labhart-Willi syndrome. (Description of a case). Minerva Pediatr. 1971;23(25):1109–1112.
4. Russell B. Prader-Willi’s syndrome. Prader-Labhart-Willi-Fanconi’s syndrome. Ugeskr Laeger. 1971;133(6):247.
5. Elena G, Bruna C, Benedetta M, Stefania DC, Giuseppe C. Prader-Willi syndrome: clinical aspects. J Obes. 2012;Article ID:13. doi:10.1155/2012/473941
6. McCandless S. Clinical report—health supervision for children with Prader-Willi syndrome. Pediatrics. 2011;127(1):195–204. doi:10.1542/peds.2010-2820
7. Prader A, Labhart A, Willi H. Ein syndrom von adipositas, kleinwuchs, kryptorchismus und oligophrenie nach myotonieartigem zustand im neugeborenenalter. Schweiz Med Wochenschr. 1956;86:1260.
8. Butler MG. Prader-Willi Syndrome: obesity due to genomic imprinting. Curr Genomics. 2011;12(3):204–215. doi:10.2174/138920211795677877
9. Cassidy SB, Driscoll DJ. Prader–willi syndrome. Eur J Hum Genet. 2009;17(1):3–13. doi:10.1038/ejhg.2008.165
10. Holm VA, Cassidy SB, Butler MG, et al. Prader-Willi syndrome: consensus diagnostic criteria. Pediatrics. 1993;91(2):398–402.
11. Cassidy SB, Schwartz S, Miller JL, Driscoll DJ. Prader-Willi syndrome. Genet Med. 2012;14(1):10–26. doi:10.1038/gim.0b013e31822bead0
12. Gunay-Aygun M, Schwartz S, Heeger S, Riordan MAO, Cassidy SB. The changing purpose of Prader-Willi syndrome clinical diagnostic criteria and proposed revised criteria. Pediatrics. 2001;108(5):E92. doi:10.1542/peds.108.6.1367
13. Cassidy SB. Prader-Willi syndrome. J Med Genet. 1997;34(11):917–923. doi:10.1136/jmg.34.11.917
14. Medeiros CB, Bordallo AP, Souza FM, Collett-Solberg PF. Endocrine management of children with Prader–willi syndrome. Pediatr Heal Med Ther. 2013;4:117–125.
15. Angulo MA, Butler MG, Cataletto ME. Prader‑Willi syndrome: a review of clinical, genetic, and endocrine findings. J Endocrinol Invest. 2015;38(12):1249–1263. doi:10.1007/s40618-015-0312-9
16. Umapathy T, Premkishore K, Mithesh D. Oral and general findings: management of Prader-Willi syndrome. J Indian Acad Oral Med Radiol. 2013;1(25):30–34. Available from: http://www.jaypeejournals.com/eJournals/ShowText.aspx?ID=5083&Type=FREE&TYP=TOP&IN=~/eJournals/images/JPLOGO.gif&IID=392&isPDF=YES
{kind=link}
17. Hurren BJ, Flack NAMS. Prader–Willi syndrome: a spectrum of anatomical and clinical features. Clin Anat. 2016;29:590–605. doi:10.1002/ca.22686
18. Wang P, Zhou W, Yuan W, Huang L, Zhao N, Chen X. Prader–Willi syndrome in neonates: twenty cases and review of the literature in Southern China. BMC Pediatr. 2016;16(1):124. doi:10.1186/s12887-016-0662-2
19. Koch A, Eisig S. Syndromes with unusual facies. Atlas Oral Maxillofac Surg Clin NA. 2014;22(2):205–210. doi:10.1016/j.cxom.2014.05.004
20. Crinò A, Fintini D, Bocchini S, Carducci C, Grugni G. Prader–Willi syndrome: clinical problems in transition from pediatric to adult care. Res Reports Endocr Disord. 2016;6:49–57.
21. Júnior ADFC, Rodrigues VMDS, Caldas KU, Barros JADP, Cabral AMC, Souza MDFD. Síndrome de Prader-Willi: relato de caso. Rev Cir Traumatol Buco-Maxilo-Fac. 2005;6(1):37–42.
22. Saeves R, Åsten P, Storhaug K, Bågesund M. Orofacial dysfunction in individuals with Prader-Willi syndrome assessed with NOT-S. Acta Odontol Scand. 2011;69:310–315. doi:10.3109/00016357.2011.568961
23. Akefeldt A, Akefeldt B, Gillberg C. Voice, speech and language characteristics of children with Prader-Willi syndrome. J Intellect Disabil Res. 1997;41(4):302–311.
24. Ho AY, Dimitropoulos A. Clinical management of behavioral characteristics of Prader–Willi syndrome. Neuropsychiatr Dis Treat. 2010;6:107–118. doi:10.2147/ndt.s5560
25. Scardina GA, Fucà G, Messina P. Oral diseases in a patient affected with Prader-Willi syndrome. Eur J Paediatr Dent. 2007;8(2):96–99.
26. Yanagita M, Hirano H, Kobashi M, et al. Periodontal disease in a patient with Prader-Willi syndrome: a case report. J Med Case Rep. 2011;5(1):329. doi:10.1186/1752-1947-5-329
27. Witt A, Olczak-Kowalczyk D, Ginalska-Malinowska M, Zadurska M. Oral findings in Prader-Willi syndrome – case report. Dent Med Probl. 2011;48(1):103–107.
28. Gadens ME, Kowalski OA, Torres MF, Brancher JA, Fregoneze AP. Prader-Willi Syndrome: clinical case report. Rsbo. 2014;11(3):309–312.
29. Song KU, Nam OH, Kim MS, Choi SC, Lee H. An 18-year-old patient with Prader-Willi syndrome: a case report on dental management under sedation and general anesthesia. J Dent Anesth Pain Med. 2015;15(4):251–255. doi:10.17245/jdapm.2015.15.4.251
30. Tayal E, Indushekar K, Saraf BG, Sheoran N, Doda A. Prader-Willi syndrome: a case report. Public Heal - Open J. 2016;1(1):12–15. doi:10.17140/PHOJ-1-104
31. Roman-Torres CVG, Kussaba ST, Bantim YCV, Oliveira RDBAAD. Special care dentistry in a patient with Prader–Willi syndrome through the use of atraumatic restorative treatment under general anesthesia. Case Rep Dent. 2017;(Article ID 7075328):4.
32. Olczak-Kowalczyk D, Korporowicz E, Gozdowski D, Lecka-Ambroziak A, Szalecki M. Oral findings in children and adolescents with Prader-Willi syndrome. Clin Oral Investig. 2018. doi:10.1007/s00784-018-2559-y
33. Bailleul-forestier I, Verhaeghe V, Fryns J, Vinckier F, Declerck D, Vogels A. The oro-dental phenotype in Prader–willi syndrome: a survey of 15 patients. Int J Paediatr Dent. 2008;18(1):40–47. doi:10.1111/j.1365-263X.2007.00857.x
34. González LC, Villa CG, Cárdenas AC. Prader willi syndrome: saliva quantification and culture in 10 patients. Med Oral Patol Oral Cir Bucal. 2008;13(12):2006–2009.
35. Saeves R, Espelid I, Storhaug K, Sandvik L, Nordgarden H. Severe tooth wear in Prader-Willi syndrome. A case – control study. BMC Oral Health. 2012;12:12. doi:10.1186/1472-6831-12-12
36. Saeves R, Reseland JE, Kvam BM, Sandvik L, Nordgarden H. Saliva in Prader-Willi syndrome: quantitative and qualitative characteristics. Arch Oral Biol. 2012;57(10):1335–1341. doi:10.1016/j.archoralbio.2012.05.003
37. Atar M, Körperich EJ. Systemic disorders and their influence on the development of dental hard tissues: a literature review. J Dent. 2010;38(4):296–306. doi:10.1016/j.jdent.2009.12.001
38. Saeves R, Klinge RF, Risnes S. Microscopic structure of dental hard tissues in primary and permanent teeth from individuals with Prader-Willi syndrome. Arch Oral Biol. 2016;66:55–60. doi:10.1016/j.archoralbio.2016.02.008
39. Dougall A, Fiske J. Access to special care dentistry, part 6. Special care dentistry services for young people. Br Dent J. 2008;205(5):235–249. doi:10.1038/sj.bdj.2008.734
40. Anglin K. Prader–Willi syndrome 101: an overview for pediatric nurses. J Pediatr Nurs. 2017;36:263–264. doi:10.1016/j.pedn.2017.04.007
41. Hauber M, Stratmann B, Hoedebeck-Stuntebeck N, Tschoepe D. Medical management for adults with Prader–willi syndrome. Metab Syndr Relat Disord. 2013;11(6):392–396. doi:10.1089/met.2012.0178
42. Bonnot O, Cohen D, Thuilleaux D, Consoli A, Cabal S, Tauber M. Psychotropic treatments in Prader-Willi syndrome: a critical review of published literature. Eur J Pediatr. 2016;175(1):9–18. doi:10.1007/s00431-015-2670-x
43. Molina-García A, Castellanos-Cosano L, Machuca-Portillo G, Paz MPL. Impact of rare diseases in oral health. Med Oral Patol Oral Cir Bucal. 2016;21(5):e587–e594. doi:10.4317/medoral.20972
44. Goldstone AP, Holland AJ, Hauffa BP, Tauber M. Recommendations for the diagnosis and management of Prader-Willi syndrome. J Clin Endocrinol Metab. 2008;93:4183–4197. doi:10.1210/jc.2008-0649
45. Mesquita MLGD, Suriano R, Carreiro LRR, Teixeira MCTV. Parental training for the behavioral management of children with Prader-Willi syndrome : impact on the mental health and parenting practices of the caregiver Treino parental para manejo comportamental de crianças com síndrome de Prader-Willi : impacto sob. Rev CEFAC. 2016;18(5):1077–1086. doi:10.1590/1982-021620161850516
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.