")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Option B+ prevention of mother-to-child transmission of HIV/AIDS service intervention outcomes in selected health facilities, Adama town, Ethiopia
Authors Chaka TE , Abebe TW , Kassa RT
Received 28 October 2018
Accepted for publication 4 March 2019
Published 18 April 2019 Volume 2019:11 Pages 77—82
DOI https://doi.org/10.2147/HIV.S192556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Tolossa Eticha Chaka,1 Tilaye Workneh Abebe,2 Roza Teshome Kassa3
1Department of Pediatrics & Child Health, Adama Hospital Medical College, Adama, Ethiopia; 2Department of Public Health, Adama Hospital Medical College, Adama, Ethiopia; 3Department of Nursing & Midwifery, College of Health Sciences, Addis Ababa University, Ababa, Ethiopia
Background: Vertical HIV transmission from mother-to-child accounts for more than 90% of pediatric HIV/AIDS infection. Virtual elimination of mother-to-child transmission (MTCT) of HIV is possible by giving comprehensive prevention of HIV/AIDS mother-to-child transmission (PMTCT) care. The objective of this study was to assess Option B+ (initiation of antiretroviral therapy for all pregnant mothers) PMTCT service intervention and outcomes in selected health facilities of Adama town, Ethiopia.
Methods: A retrospective study was employed. A total of 248 medical records of mother–infant cohorts were included. Data wer collected from logbooks and/or records and individual medical records using a data abstraction tool.
Results: Mean±SD age of mothers was 26.8±4.3 years. Half (50.8%) of the mothers were enrolled in PMTCT at 13–24 weeks of gestational age. The majority (79.6%) of mothers’ CD4 counts were ≥351/mm3,. Most of the mothers (71%) were on a tenofovir–lamivudine–evafrenz regimen. One-quarter of mothers were prescribed co-trimoxazole prophylactic therapy. Loss to follow-up from the Option B+ continuum was 10 (4.2%). Almost all (98.4%) of the infants were prescribed nevirapine prophylaxis. Nearly 90% (n=223) of the HIV-exposed infants were discharged as HIV negative.
Conclusions: The Option B+ PMTCT service can minimize the chances of MTCT of HIV infection if used optimally. The magnitudes of loss to follow-up and death were lower than in comparable studies. Initiating all pregnant mothers on antiretroviral therapy irrespective of their clinical stage and CD4 count may have contributed to the optimal retention in care and near elimination of MTCT of HIV infection.
Keywords: Option B+, PMTCT, HIV-exposed infant, Adama
Introduction
Each year, over half a million newborns are infected with HIV in sub-Saharan Africa through mother-to-child transmission (MTCT). Of all health crises in the African region, HIV/AIDS has attracted the most political support and resources. Prevention of HIV/AIDS mother-to-child transmission (PMTCT) is one of the efforts to reduce new HIV infections. The PMTCT program has encountered difficulties and confusion since the first isolation of HIV in an 18-month-old child in 1982.1 In the following few years, it became evident that 25% of pregnant HIV-infected mothers will transmit the infection to their children.2 Even though a clear risk of acquisition of HIV from an infected mother was established, few attempts were made to prevent transmission, such as avoiding pregnancy in uninfected mothers or avoiding breast feeding.3 The earliest management proxy of PMTCT was treating the mother herself, to help as a preventive strategy.4
To prevent MTCT, the United Nations recommends a comprehensive four-pronged approach. This comprises the prevention of acquisition of HIV/AIDS infection among women of reproductive age, avoidance of unwanted pregnancy among women living with HIV/AIDS, prevention of HIV transmission from mother to infant, and linkage of mothers living with HIV/AIDS with appropriate treatment, care, and support.5–9
Even though different efforts were being made, about 330,000 children were infected with HIV in 2011 globally, with over 90% of these infections occurring in sub-Saharan Africa, and mainly through MTCT. Twenty-two countries account for more than 90% of the global burden, and Ethiopia is one of these priority countries, where one of every three children born to women living with HIV was infected with HIV.10,11 In 2014, there were 170,000 new HIV infections among children, of which 14% were MTCT, including during breast feeding, worldwide. This shows a 48% decrease in new HIV infections among children.12
Studies show that 3.3% of infants born to infected mothers are identified as being HIV infected. The duration of antenatal highly active antiretroviral therapy (HAART) was the most important predictor of perinatal HIV transmission. Compared with women initiating HAART at least 13 weeks before delivery, women on HAART for only 4 weeks had a 5.5-fold increased odds of HIV transmission.9,12
The Ethiopian government started to implement the Option B+ (initiation of antiretroviral therapy for all pregnant mothers) PMTCT service in 2013. Since then, the Option B+ treatment option has been launched in all PMTCT health facilities. According to the operational plan, under Option B+, all HIV-infected pregnant mothers will receive triple antiretroviral therapy (ART) drugs and will continue the treatment for the rest of their lives.12
The advantages of Option B+ PMTCT intervention include: simplification of ART, protection against MTCT in future pregnancies, a continuing prevention benefit against sexual transmission to sero-discordant partners, and avoiding stopping and starting of antiretroviral drugs.9
A systematic review and meta-analysis study, which included articles conducted in Ethiopia, showed that the estimated pooled prevalence of MTCT was 11.4%. Based on this study, being from a rural residence, home delivery, not taking antiretroviral prophylaxis, the absence of PMTCT intervention, and mixed infant feeding practices were major risk factors for MTCT.13
This study was planned to assess Option B+ PMTCT service intervention and outcome in selected facilities of Adama town.
Methods
This study was conducted in Adama town, which is located in the Rift Valley of central Ethiopia. It is located at 8°32ʹN 39°16ʹE/8°54ʹ°N 39°27ʹE at an elevation of 1712 m above sea level. The town is 99 km south-east of the capital city of Ethiopia, on the main railway to Djibouti, and has an area of 29.86 km2. In Adama, the Option B+ PMTCT service was started in early 2013, after the Ethiopian Government launched the service.
A retrospective design was employed among registers of mother–infant pairs with complete records. The study was conducted in three public health facilities that provide the Option B+ PMTCT service in Adama town. The study assessed a 3-year PMTCT service from the initiation of the Option B+ PMTCT service (end of 2013 to beginning of 2016) in Adama town. The data collection period was from June 1, 2017 to July 30, 2017.
A structured data abstraction form was used to capture data from records. Data were collected by trained midwives. The collected data were cleaned, coded, and entered into Epi-info version 7. Double-entry verification was used to assure quality. Then, the data were exported to SPSS version 20 for analysis. Descriptive statistics were employed to check assumptions for further analysis and to summarize key variables such as socio-demographic variable and magnitude of dropouts.
The study was conducted after obtaining ethical clearance from the institutional ethical review board (IRB) of Adama Hospital Medical College (AHMC). Consent for the record review was obtained from the IRB of AHMC. Health facility records were coded and kept confidential. The data collected were not to be used for any purpose other than the specified objectives. This study was performed in compliance with the Declaration of Helsinki.
Results
In this study, a total of 248 mother–infants’ medical records were included. Concerning maternal characteristics, the mean±SD age of mothers was 26.8±4.3 years. Nearly half (48%) of the mothers were aged 25–29 years.
From the total of 248 women, 173 (87%) were already on ART follow-up at enrollment. Nearly half, 100 (50.8%) of the mothers, were enrolled in PMTCT at 13–24 weeks of gestational age. The majority, 180 (79.6) of mothers, had a CD4 count ≥351/mm3. Most mothers were on a tenofovir–lamivudine–evafrenz (TDF-3TC-EVF) regimen (n=174, 71%), followed by azidothymidine–lamivudine–nevirapine (AZT-3TC-NVP) (n=33, 13.5%) and tenofovir–lamivudine–nevirapine (TDF-3TC-NVP) (n=22, 9%).
Family planning counseling was given to 99% of the mothers (n=243) during HIV chronic care. One hundred and seventy-nine mothers (83.6%) reported condom use prior to the current pregnancy. Dual contraception (condom plus any other contraceptive use) was used by 140 mothers (78.2%) before the current pregnancy. After condoms, injectable hormones were the most commonly used contraceptive method (68.2%), followed by oral contraceptive pills (10.4%).
Seventeen percent of the couples (n=41/112) were sero-discordant. Nearly half of study participants (45.9%) had no history of isoniazid (INH) prophylaxis recorded. One-quarter of mothers were prescribed co-trimoxazole prophylactic therapy (CPT). Nearly all mothers (99%) had used ferrous sulfate/folic acid supplementation during antenatal care follow-up. The proportion of mothers who tested positive for syphilis (by rapid plasma reagin) was 2.2% (n=235) (Table 1).
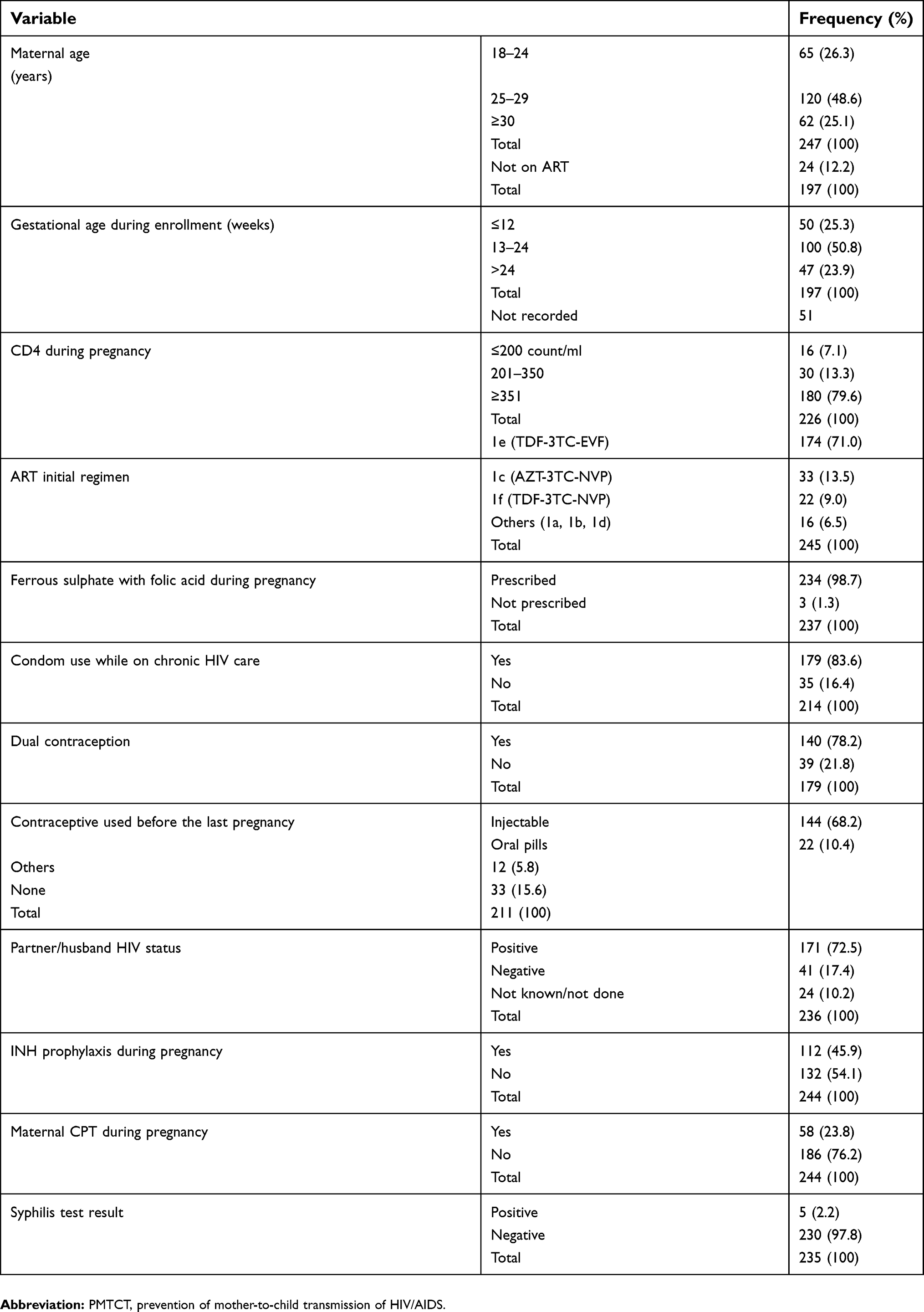 | Table 1 Option B+ PMTCT interventions for mothers in Adama town, 2013–2016 |
The sex ratio of infants included in this study was nearly 1:1. Almost all (98.4%) of the infants were prescribed NVP prophylaxis. Concerning infant feeding practices in the first 6 months, 230 (93.5%) were reported as exclusive breast feeding, while 13 (5.3%) and three (1.2%)received exclusive replacement feeding and mixed feeding, respectively. The majority (93.5%) of HIV-exposed infants (HEIs) received CPT at 6–7 weeks of age (Table 2).
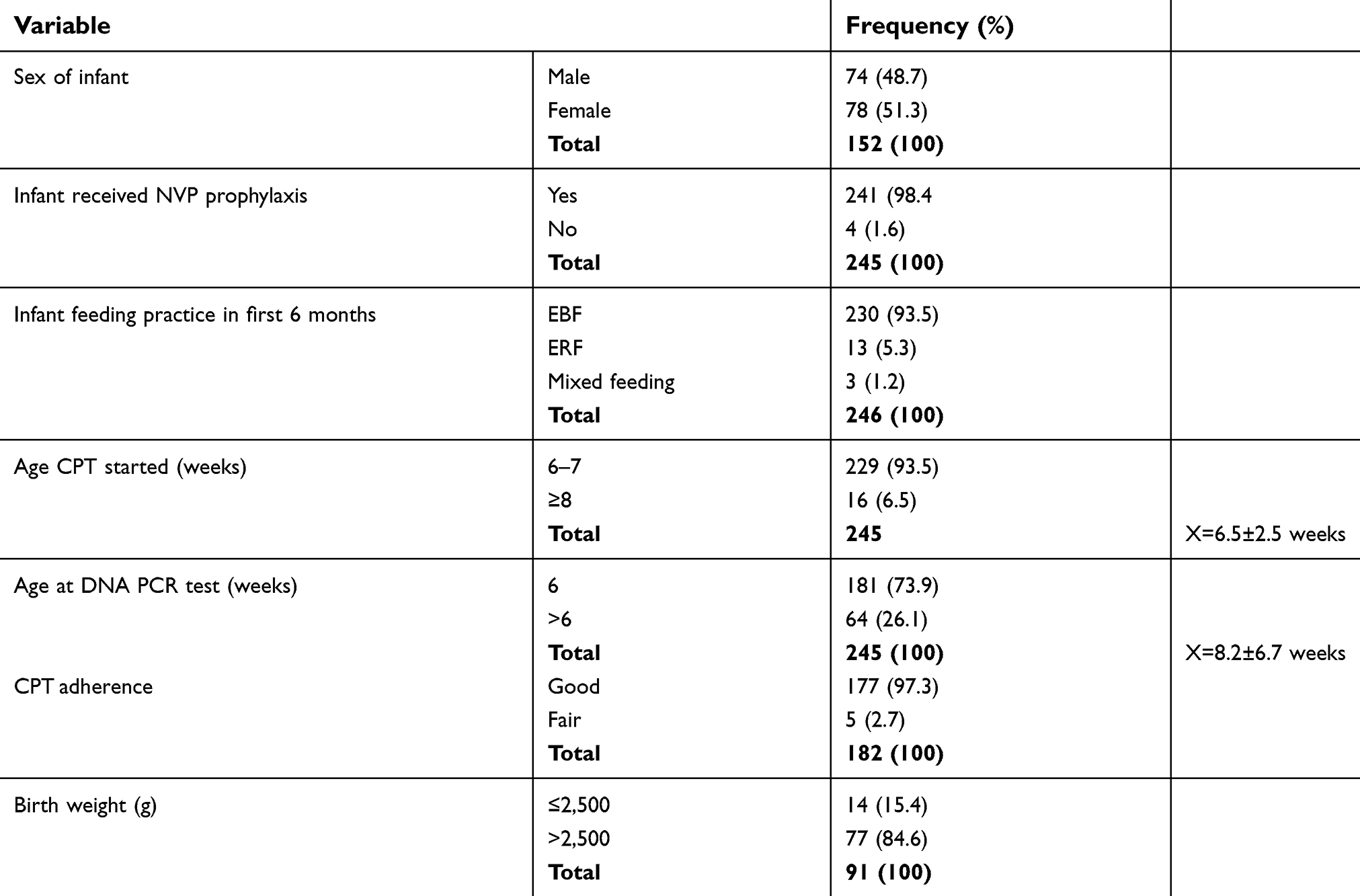 | Table 2 Option B+ PMTCT interventions for infants in Adama town, 2013–2016 |
DNA PCR was done for 73.9% of the HEIs by 6 weeks of age. Over 97% of HEIs were reported to have good adherence to CPT while only 2.7% had fair adherence to this medication. The weight at birth of about 15.4% of infants was <2,500 g (Table 2).
Nearly 90% (n=223) of the HEIs were discharged as negative. The remaining 10% of mother–infant pairs either dropped out or died, or tested positive and were enrolled into chronic HIV care (Figure 1).
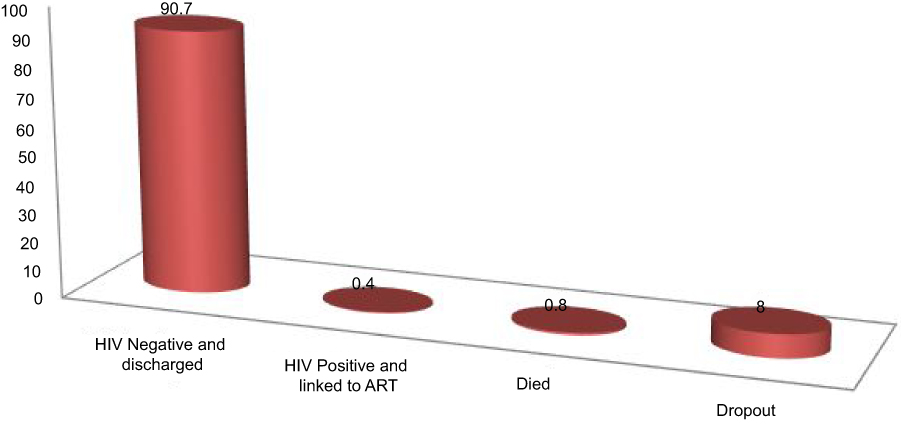 | Figure 1 Final status of HIV-exposed infants in Adama town, 2013–2016.Abbreviation: ART, antiretroviral therapy. |
Discussion
Half (50.8%) of the mothers were enrolled to care at 13–24 weeks of gestational age. Mean±SD gestational age during enrollment was 18±8 weeks. The majority (79.6%) of mothers had a CD4 count during enrollment ≥351/mm3. The median CD4 count was 528/mm3 (IQR=340). This finding showed that most mothers were enrolled to HIV care at an early time, comparable to standards, which may contribute to their good health status, explained by the good CD4 counts at enrollment.
The most commonly used ART regimen during the PMTCT program was TDF-3TC-EFV (71%), followed by AZT-3TC-NVP (13.5%) and TDF-3TC-NVP (9%). This contrasts with a study conducted in Rwanda, which showed figures of 52%, 13%, and 24%, respectively, for these ART regimens.
This record-review study indicated that half (50%) of mothers included in the study had taken INH prophylaxis during pregnancy. Concerning CPT, 25% of mothers took CPT during pregnancy. In this study, the mean age at enrollment of HEIs was 6.4±2.9 weeks. This is the optimal time to follow-up for HEIs, according to the WHO PMTCT guideline.
Nearly 90% of the HEIs were discharged as negative. Dropouts accounted for 8% of infants in the study. This contrasts with other studies in sub-Saharan Africa, where the rates of loss to follow-up from the Option B+ PMTCT program ranged from 19% to 89.4%.14
A systematic review and meta-analysis of loss to follow-up of HEIs within 3 months of delivery ranged from 4.8% to 75%, with a pooled proportion of 33.9%.12 Another study, carried out in three referral hospitals in Cameroon, showed that the attrition rate of HEIs was 9.8%, which is close to the result in this study.15 This may be due to the different approaches utilized to prevent attrition from the PMTCT program over the 4-year gap between the studies.
In this study, only two (0.8%) of the HEIs died and one (0.4%) became HIV positive. This is markedly lower than even the predicted virtual elimination of MTCT, as low as 4%.16
Conclusion
The Option B+ PMTCT service can minimize the chances of HIV transmission from mother to child. Most mothers included in this study were of early reproductive age. Time to PMTCT enrollment, CPT utilization, and INH prophylaxis use were optimal according to the WHO standard. Similarly, HEIs' time to enrollment in care, DNA PCR testing, and CPT were optimal according to the WHO’s recommendations. Magnitudes of dropouts and death were significantly lower. Initiating all pregnant mothers irrespective of their clinical stage and CD4 count may have contributed to the better outcome in this mother–infant cohort.
Acknowledgments
Unreserved thanks go to Adama Hospital Medical College for financial and material support. We want to extend our gratitude to the Antenatal care and ART clinic for their support during data collection.
Disclosure
The authors report that there are no conflicts of interest in this work.
References
1. Bardi J. First Pediatric Cases of HIV: recalling 1981 UCSF AIDS 2012 Blog. Available from:
2. Ammann AJ. Is there an acquired immune deficiency syndrome in infants and children? Pediatrics. 1983;72:430–432.
3.
4. Guay LA, Musoke P, Fleming T, et al. Intrapartum and neonatal single-dose nevirapine compared with zidovudine for prevention of mother-to-child transmission of HIV-1 in Kampala, Uganda: HIVNET 012 randomized trial. The Lancet. 1999;354:795–802. doi:10.1016/S0140-6736(99)80008-7
5.
6.
7. Dorenbaum A, Cunningham CK, Gelber RD, et al. Two-dose intrapartum/newborn nevirapine and standard antiretroviral therapy to reduce perinatal HIV transmission: a randomized trial. J Am Med Assoc. 2002;288(2):189–198. doi:10.1001/jama.288.2.189
8.
9.
10.
11.
12. Sibanda EL, Weller IVD, Hakim JG, Cowan FM. The magnitude of loss to follow-up of HIV-exposed infants along the prevention of mother-to-child HIV transmission continuum of care: a systematic review and meta-analysis. Aids. 2013;27(17):2787–2797. doi:10.1097/QAD.0000000000000027
13. Endalamaw A, Demisie A, Eshetie S, Habtewold T. Systematic review and meta-analysis of vertical transmission route of HIV in Ethiopia. BMC Infect Dis. 2018;18:283. doi:10.1186/s12879-018-3189-3
14. Guliani H, Sepehri A, Serieux J. Determinants of prenatal care use: evidence from 32 low-income countries across Asia, Sub Saharan Africa and Latin America. Health Policy Plan. 2013. doi:10.1093/heapol/czt045
15. Sidze LK, Faye A, Tetang SN. et al. Different factors associated with loss to follow-up of infants born to HIV-infected or uninfected mothers: observations from the ANRS. BMC Public Health. 2015;15(1):228
16.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.