")
Back to Journals » Local and Regional Anesthesia » Volume 11
Optimizing the securement of epidural catheters: an in vitro trial
Authors Hakim M , Froyshteter AB , Walia H, Tumin D, Veneziano G , Bhalla T, Tobias JD
Received 1 May 2018
Accepted for publication 6 June 2018
Published 17 July 2018 Volume 2018:11 Pages 31—34
DOI https://doi.org/10.2147/LRA.S172799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Stefan Wirz
Mohammed Hakim,1 Alexander B Froyshteter,2 Hina Walia,1 Dmitry Tumin,1,3 Giorgio Veneziano,1 Tarun Bhalla,1,4 Joseph D Tobias1,3,4
1Department of Anesthesiology and Pain Medicine, Nationwide Children’s Hospital, Columbus, OH, USA; 2Department of Anesthesiology, Rush University Medical Center, Chicago, IL, USA; 3Department of Pediatrics, The Ohio State University College of Medicine, Columbus, OH, USA; 4Department of Anesthesiology and Pain Medicine, The Ohio State University College of Medicine, Columbus, OH, USA
Introduction: Epidural anesthesia is frequently used to provide postoperative analgesia following major surgical procedures. Secure fixation of the epidural catheter is necessary to prevent premature dislodgment and loss of epidural analgesia. Using an in vitro model, the current prospective study evaluates different types of dressings for securement of an epidural catheter by quantifying the force in Newtons (N) required for dislodgment using a digital force gage.
Methods: Four methods of epidural catheter securement were used on a simulator mannequin: 1) Suresite® Window Clear Dressing, 2) Op-Site Post-Op® Visible Dressing, 3) Steri-Strips® and Suresite Window Clear Dressing, and 4) Steri-Strips and Op-Site Post-Op Visible Dressing. Each method of securement was assessed 10 times to calculate the mean force required to dislodge the catheter. Mean force of dislodgment for each method was compared using parametric tests.
Results: The force (mean ± SD) required for catheter dislodgment for the four methods was 14.0±2.9, 2, 10.7±1.5, 8.6±2.3, and 9.6±2.2 N, respectively. The pairwise difference showed that the Suresite Window Clear Dressing was the best securement method when compared with other methods.
Conclusion: Our study demonstrates the advantage of the Suresite Window Clear Dressing in securing the epidural catheter. Future clinical trials are needed to validate these findings.
Keywords: epidural catheter, securement, dressings
Introduction
Epidural catheters are used during various surgical procedures in children to supplement general anesthesia and provide postoperative analgesia. A secured catheter is necessary to decrease complication rates, obtain maximum analgesic effect, and provide optimal patient comfort. Catheter dislodgment has been shown to be as high as 30% in data from the Pediatric Regional Anesthesia Network.1 Several techniques have been advocated to secure the epidural catheter including sterile tape, topical skin adhesive, anchoring devices, and subcutaneous tunneling.2,3 In a 2-year quality improvement review of our institution’s experience, we noted that the dislodgment rate was highest for lumbar catheters (11%), while dislodgment rates with thoracic, caudal epidural catheters, and peripheral nerve catheters were 9%, 0%, and 4%, respectively. We aimed to decrease the rate of unintentional removal or catheter dislodgment by identifying the optimal method of catheter securement using an in vitro investigation. Our primary aim was to measure the force required to dislodge the epidural catheter with various methods of catheter securement to a mannequin.
Methods
This was a prospective, non-blinded, in vitro trial that did not involve patient care. As such, there was no need for Institutional Review Board approval. The epidural catheter was secured to a mannequin model (Nursing Kid®, Wappingers Falls, NY, USA) using four methods: 1) Suresite® Window Clear Dressing (Medline Inc, Mundelein, IL, USA); 2) Op-Site Post-Op® Visible Dressing (Smith & Nephew Medical limited, Hull, UK); 3) Steri-Strips® (3M Health Care, St. Paul, MN, USA) and Suresite Window Clear Dressing (Figure 1); and 4) Steri-Strips and Op-Site Post-Op Visible Dressing (Figure 2). At the time the study was conducted, epidural catheters were typically secured by Suresite window clear dressing in clinical use. The Suresite Window Clear Dressing does not have foam padding, while the Op-Site Post-Op Visible Dressing does have foam padding. Each of these two devices was compared separately and with the addition of Steri-Strips to secure the catheter under the devices, thereby resulting in the four study groups. The catheter was placed at the L4–5 level, identified by the superior margin of the iliac crests, and was secured by one of the study investigators.
 | Figure 1 Securement of epidural catheter to mannequin using Steri-Strips® and Suresite® window clear dressing. |
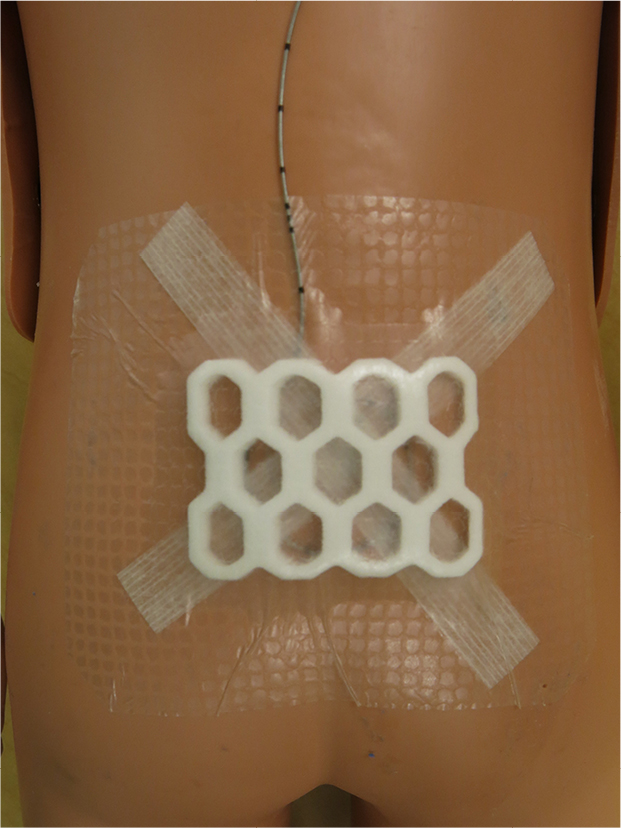 | Figure 2 Securement of epidural catheter to mannequin using Steri-Strips and Op-Site Post-op® visible dressing. |
The direction of the force applied to dislodge the catheter was at a 45° angle to the surface of the mannequin, as it was postulated to be the most consistent way to maintain a consistent vector for the force and to test the efficacy of securement with the different dressings. The traction was initiated 1 minute after the catheter had been secured in place. Catheter dislodgment was defined as full dislodgement or separation of the catheter from the surface of the mannequin. A second experimenter used a Nidex® (Zoro, Buffalo Grove, IL, USA) digital force gage to measure the force in newtons (N) needed to dislodge or pull the catheter from the mannequin. For each method of securement, the trial was repeated 10 times.
Force data collected in the study were found to be normally distributed (Shapiro–Wilk test P=0.175). Unpaired t-tests were used to compare the force required for catheter dislodgment between each pair of methods. Due to the exploratory nature of the study, no a priori power analysis was performed. No adjustment was made for multiple comparisons. P<0.05 was considered statistically significant. Stata/IC 14.2 (StataCorp, LP, College Station, TX, USA) was used for statistical analysis.
Results
The force required to dislodge the catheter using the four securement techniques is summarized in Table 1. The greatest force was required to dislodge catheters secured by the Suresite Window Clear Dressing without Steri-Strips, followed by catheters secured by the Op-Site Post-Op Visible Dressing without Steri-Strips. Increased resistance to dislodgment with the Suresite Window Clear Dressing compared with Op-Site Post-Op Visible Dressing was statistically significant when analyzing securement without Steri-Strips (P=0.005), but not when analyzing securement with Steri-Strips (P=0.312). Table 2 shows the pairwise differences, 95% CI of difference, and P-value, which also supported that the Suresite Window Clear Dressing was the best method for securement.
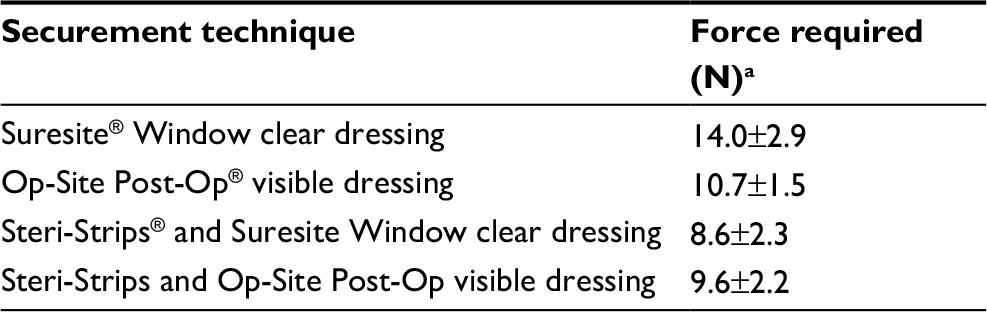 | Table 1 Force (in newtons) required to dislodge the epidural catheter Notes: aForce in newtons (N) as the mean ± SD. Each trial was repeated 10 times. |
 | Table 2 Pairwise differences: 95% CI of difference and P-value of the techniques |
Discussion
The current study evaluated the efficacy of four commonly used methods to secure an epidural catheter. We noted that catheter securement by the Suresite Window clear dressing required the highest force for dislodgment. Of note, the addition of Steri-Strips to either dressing did not improve the efficacy of securement and in fact, decreased the forced required for catheter dislodgment, suggesting that their addition to commonly used dressings is not indicated.
In the pediatric population, epidural anesthesia is a well-established technique during the intraoperative and postoperative periods and remains one of the preferred methods of analgesia due to its efficacy and safety.4 However, technical factors may interfere with the efficacy of analgesia. Postoperatively, patient movement is inevitable and may lead to catheter dislodgment. Maintenance of catheter integrity to ensure its efficacy and secure placement despite patient movement as well as exposure to blood, perspiration, and moisture remains a challenge.5,6 The leading technical problems associated with epidural catheter placement are leakage around the insertion site and dislodgment of the catheter.6 Complications associated with catheter movement may include catheter failure with inadequate pain control, catheter dislodgment, or even dural puncture with inadvertent complete spinal anesthesia.6–8
Previous studies have demonstrated that the site of placement may influence the rate of catheter dislodgment. Ahsan et al reported a failure rate of 26% for supraclavicular when compared with 19% for infraclavicular perineural catheters.9 The authors attributed this difference to lack of musculature around the supraclavicular site to prevent the movement and dislodgment as well as different methods of securement. In our clinical experience, we have noted a higher rate of dislodgment with lumbar epidural vs caudal or thoracic epidural catheters.
There are limitations in our present study that warrant consideration. We employed a mannequin model as in vitro model to test the strength of catheter securement, which is not an exact representation of in vivo catheter securement in human patients due to other factors which may play a role including the presence of fluid, blood, or perspiration under the dressing as well as differences in adherence of the dressing or Steri-Strips to skin vs the artificial surface of the mannequin. The epidural catheter was merely taped on top of the mannequin without direct insertion into the tissue or device. Our assessment was based on the force required to dislodge the epidural catheter measured by a Nidex force gage. The experimenter dislodging the catheter was instructed to apply force at a 45° angle to the surface of the mannequin from the securement site. This may not always represent the vector of force that occurs clinically as twisting or pulling from the side or other directions may occur.
Our study demonstrates a potentially better technique for securement of the epidural catheter insertion site. Furthermore, it demonstrates that the use of Steri-Strips under these dressings offers no advantage. Epidural catheter dislodgment leading to premature removal or disruption of postoperative epidural analgesia is a recognized concern. Various studies have shown that dislodgment of perineural and epidural catheters remains a significant problem in clinical practice. Securement techniques have included addition of an adhesive anchoring device or dressing as in the current study, application of topical agents such as Dermabond® or cyanoacrylate glue, and subcutaneous tunneling.3,10,11 Although dressing techniques may play a vital role in the prevention of epidural catheter dislodgment, there are limited data to determine the optimal technique. Further validation with in vivo trials is needed to provide additional information regarding the optimal dressing techniques for securement of an epidural catheter.
Disclosure
The authors report no conflicts of interest in this work.
References
Walker BJ, Long JB, de Oliveira GS, et al. Peripheral nerve catheters in children: an analysis of safety and practice patterns from the pediatric regional anesthesia network (PRAN). Br J Anaesth. 2015;115(3):457–462. | ||
Ilfeld BM. Continuous peripheral nerve blocks in the hospital and at home. Anesthesiol Clin. 2011;29(2):193–211. | ||
Marhofer D, Marhofer P, Triffterer L, et al. Dislocation rates of perineural catheters: a volunteer study. Br J Anaesth. 2013;111(5):800–806. | ||
Vane D, Pietropaoli J, Smail FD, Hong A, Abajian JC, et al. Continous retropleural infusion for analgesia after thoracotomy in newborn infants. Pediatr Surg Int. 1995;10(5-6):311–314. | ||
Burns SM, Cowa CM, Barclay PM, Wilkes RG. Intrapartum epidural catheter migration: a comparative study of three dressing applications. Br J Anaesth. 2001;86(4):565–567. | ||
Gurnaney H, Kraemer FW, Maxwell L, Muhly WT, Schleelein L, Ganesh A. Ambulatory continuous peripheral nerve blocks in children and adolescents: a longitudinal 8-year single center study. Anesth Analg. 2014;118(3):621–627. | ||
Bishton IM, Martin PH, Vernon JM, Liu WH. Factors influencing epidural catheter migration. Anaesthesia. 1992;47(7):610–612. | ||
Philip JH, Brown WU. Total spinal anesthesia late in the course of obstetric bupivacaine epidural block. Anesthesiology. 1976;44(4):340–341. | ||
Ahsan ZS, Carvalho B, Yao J. Incidence of failure of continuous peripheral nerve catheters for postoperative analgesia in upper extremity surgery. J Hand Surg Am. 2014;39(2):324–329. | ||
Klein SM, Nielsen KC, Buckenmaier CC, et al. 2-Octyl cyanoacrylate glue for the fixation of continuous peripheral nerve catheters. Anesthesiology. 2003;98(2):590–591. | ||
Auyong DB, Cantor DA, Green C, Hanson NA. The effect of fixation technique on continuous interscalene nerve block catheter success: a randomized, double-blind trial. Anesth Analg. 2017;124(3):959–965. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.