")
Back to Journals » Pathology and Laboratory Medicine International » Volume 7
Optimizing polymerase chain reaction testing for the diagnosis of pertussis: current perspectives
Authors Arbefeville S, Ferrieri P
Received 19 May 2015
Accepted for publication 21 July 2015
Published 7 September 2015 Volume 2015:7 Pages 67—73
DOI https://doi.org/10.2147/PLMI.S56415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Paul Zhang
Sophie Arbefeville, Patricia Ferrieri
Department of Laboratory Medicine and Pathology, University of Minnesota Medical School, Minneapolis, MN, USA
Abstract: Nucleic acid testing has revolutionized the diagnosis of pertussis in the clinical microbiology laboratory and has become the main avenue of testing for pertussis infection. Real-time polymerase chain reaction (RT-PCR) is an important tool for timely diagnosis of pertussis and is more sensitive than culture. The most commonly amplified targets are the insertion-sequence (IS) genes, which are found in multiple copies in the genome of Bordetella species. Some strains of Bordetella pertussis have more than 200 copies of IS481 in their genome. This high number of repeats allows RT-PCR assays to be very sensitive and makes nucleic acid testing two to three times more sensitive than culture. Despite these advantages, RT-PCR can give inaccurate results due to contamination or lack of specificity. Contamination can easily happen during specimen collection, DNA extraction, or nucleic acid amplification steps. To avoid contamination, laboratories need to have quality controls and good workflows in place. The poor specificity of the nucleic acid assays amplifying the IS genes is because they are found in various Bordetella species and, thus, not unique to a specific species. Bordetella holmesii, a more recently described Bordetella species found to be responsible for respiratory symptoms similar to pertussis in adolescents and adults, can be misidentified as B. pertussis in RT-PCR assays that amplify only the IS481 target. Use of multiple targets may improve specificity of RT-PCR assays for pertussis. In the past few years, the US Food and Drug Administration has cleared three commercial assays for the detection of B. pertussis in respiratory specimens. Several commercial assays and analyte-specific reagents, which are not US Food and Drug Administration cleared, are available for the detection of one or more Bordetella species by nucleic acid testing. Because of the diversity of nucleic acid amplification assays used, pertussis testing is not standardized across clinical laboratories.
Keywords: nucleic acid testing, real-time PCR, Bordetella pertussis, Bordetella species
Introduction
Pertussis is a disease of the respiratory tract caused by the fastidious Gram-negative rod bacteria Bordetella pertussis, and a pertussis-like illness can be caused by Bordetella parapertussis. Pertussis can cause serious illness in infants, children, and adults. Pertussis is still prevalent worldwide and is an important cause of death among neonates and infants too young to have completed their primary vaccination series. WHO estimates that, in 2008, 16 million pertussis cases occurred worldwide and that approximately 195,000 children died from the disease, representing 2% of the global causes of death in children aged 1–59 months.1,2 Approximately half of infants younger than 1 year of age who develop the disease are hospitalized.3 Before vaccination, pertussis was one of the most common childhood diseases worldwide. Pertussis continues to be a public concern even in countries with high vaccination coverage. In the USA, from 1940 through 1945, before the introduction of the pertussis vaccine, the incidence of pertussis was approximately 150 cases per 100,000 population. Following the implementation of the whole-cell pertussis vaccine in the late 1940s, pertussis gradually declined to approximately eight cases per 100,000 population in 1960 and reached a low of approximately one case per 100,000 population during 1980–1990. Since then, the number of reported cases of pertussis has begun to increase gradually, and in 2014, more than 28,000 cases were reported nationwide with an incidence of 9.1 cases per 100,000 population (CDC Surveillance report).4,5 While the incidence of pertussis in the USA is still highest among infants younger than 1 year of age, the incidence among older children and adults has increased substantially during the past decade. The reasons for the increase, despite high vaccination coverage, are not fully understood, but several factors have been suggested, including genetic changes in B. pertussis, decreased effectiveness of vaccine, waning of immunity from vaccination over time, increasing awareness by clinicians, and better laboratory detection.6,7
Bordetella species
The genus Bordetella contains eight species, four of which are known to cause respiratory disease in humans: B. bronchiseptica, B. holmesii, B. parapertussis, and B. pertussis. B. holmesii is a novel organism that was first described in 1995 as a cause of bacteremia in patients with comorbidities such as asplenia, but since has been shown to cause respiratory symptoms in otherwise healthy individuals.8 B. pertussis, B. parapertussis, and B. bronchiseptica are closely related species, but B. parapertussis and B. bronchiseptica do not produce the pertussis toxin due to a mutation in the promoter region of the genes encoding this toxin.9 B. holmesii does not produce the virulence factors produced by the other three species. B. parapertussis is found in sheep and humans, and B. pertussis is thought to be a strictly human pathogen.10 B. bronchiseptica can cause respiratory infections in many animal species and, infrequently, also in humans. An increasing number of pertussis-like cases are attributed to the emergent pathogen B. holmesii.8 It is still unknown whether this species is truly pathogenic for humans or only an opportunistic organism, but microbiologic diagnosis has confirmed the presence of B. holmesii in human respiratory samples.8
Laboratory diagnosis of pertussis
There are two different approaches to the diagnosis of pertussis in the laboratory: the direct approach, which consists of identifying the microorganism responsible for the disease, either by culture, direct fluorescent antibody (DFA) testing, or real-time polymerase chain reaction (RT-PCR), and the indirect approach which consists of detecting specific antibodies in the serum of infected individuals.
Culture
Isolation and identification of B. pertussis is highly specific, but the recovery is low and declines with age, if the patient has received prior antibiotic therapy effective against B. pertussis, if the collection of the specimen has been delayed beyond the first 2 weeks of illness, and if the patient has been vaccinated.11 However, culture is particularly useful for confirming pertussis diagnosis when an outbreak is suspected and allows for strain identification and antimicrobial resistance testing.
DFA testing
DFA staining of nasopharyngeal swabs or nasopharyngeal aspirates is rapid and simple, but because of its low sensitivity and variable specificity, it is not accepted as proof of infection.10
Real-time polymerase chain reaction
RT-PCR is more sensitive than culture and has been accepted as evidence of laboratory confirmation of pertussis in different countries (examples: USA and Canada). It is still recommended to send specimens for culture, particularly during outbreaks, as bacterial isolates may be required for evaluation of antibacterial resistance or epidemiologic studies. RT-PCR is able to detect the organism at a later stage of the infection, when the ability to culture the organism declines.
Serology
Serology consists of detecting specific anti-pertussis toxin (PT) antibodies in the serum of infected individuals after 2–3 weeks of the cough. Serology testing should not be used in infants, as their immune systems are immature and susceptible to interference by maternal antibodies, or in patients who have been vaccinated within 1 year since it does not differentiate between antibodies due to the vaccine and natural infection. Generally, serologic tests are more useful for diagnosis in later phases of the disease when it is too late to perform culture or nucleic acid amplification testing (NAAT). Other antibodies to pertussis antigens are not routinely available but are usually included in pertussis vaccine trials (eg, anti-filamentous hemagglutinin, anti-fimbriae, anti-pertactin). A battery of antibody tests may be advantageous rather than just anti-PT.
RT-PCR testing for the diagnosis of pertussis
RT-PCR has revolutionized the way clinical laboratories diagnose B. pertussis. NAAT is a rapid and sensitive way to detect B. pertussis from upper respiratory samples. It does not require viable bacteria for detection. This permits the use of more diverse collection devices and simplifies the transport and storage of specimens for pertussis testing.
RT-PCR has an optimal sensitivity during the first 3 weeks of illness when bacterial DNA is still present in the nasopharynx.12 One study showed that the bacterial DNA could be detected by RT-PCR up to 58 days into illness even after antimicrobial therapy.13 Nevertheless, after the fourth week of cough, the amount of bacterial DNA rapidly diminishes and might be too low to be detected by NAAT, and thus, serology (IgA or IgG anti-PT or other antibody testing) is recommended.
Amplification targets
Several Bordetella gene targets have been selected for the amplification and detection of Bordetella species by NAAT. The most commonly used targets are the insertion-sequence (IS) genes because they are usually found in multiple copies in the bacterial genome and, thus, increase the sensitivity of the nucleic acid assay. However, they are usually found in more than one species of Bordetella and, thus, not limited to a single Bordetella species. IS481 is found in 50 to more than 200 copies in the genome of B. pertussis, 8–65 copies in the genome of B. holmesii, and less than five copies in the genome of some strains of B. bronchiseptica.14–16 IS1001 is present in approximately 20 copies in the genome of B. parapertussis and 1–7 copies in the genome of B. bronchiseptica. IS1002 is found as 1–9 copies in the genome of B. pertussis, B. parapertussis, and B. bronchiseptica.15–17 hIS1001 is only found in the genome of B. holmesii and in only 3–21 copies (Table 1).18
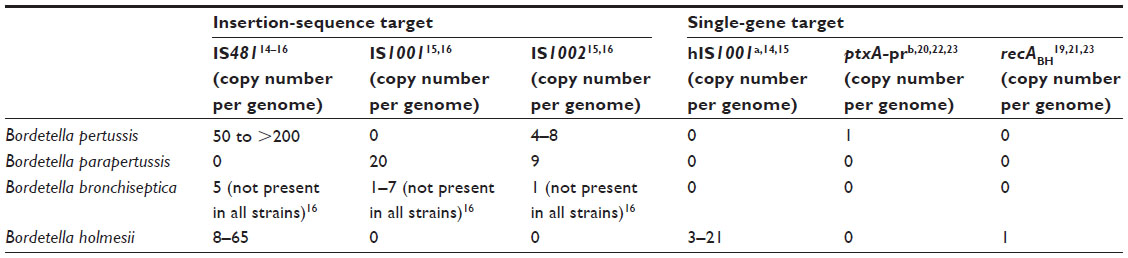 | Table 1 Targets that are most commonly used for the detection of Bordetella pertussis by nucleic acid amplification |
The insertion sequences, IS481 and IS1001, are the most commonly used RT-PCR targets for the diagnosis of B. pertussis and B. parapertussis, respectively. Since both targets are also present in more than one species of Bordetella, these RT-PCR assays potentially can misidentify B. holmesii and B. bronchiseptica as B. pertussis or B. parapertussis, respectively.19
NAAT assays that use a single gene-copy target like the pertussis toxin S1 promoter ptxA-pr gene also known as ptxP, which is only found in B. pertussis, and the housekeeping gene recABH that is only found in B. holmesii are very specific but, in general, have poor sensitivity.20–23 Their sensitivity is comparable to culture, in contrast to RT-PCR assays that use multicopy targets like IS481, which are approximately 2–3 times more sensitive than culture.24–26
Some laboratories have developed multiplex RT-PCR assays that incorporate the B. holmesii-specific recABH primers with the IS481 primers to differentiate between B. pertussis and B. holmesii.19,21,23
Because pertussis NAATs are not standardized across clinical laboratories, the results may not be comparable from one laboratory to another. Different testing methods, amplification targets, and result interpretation are used to determine positive, indeterminate, or negative results.
Collecting devices
Dacron and rayon swabs are the recommended swabs for the collection of nasopharyngeal specimens to be tested by RT-PCR and also culture. The calcium-alginate swabs are not recommended as they inhibit the polymerase chain reaction.27 Recently flocked swabs (eg, ESwab; Copan Diagnostics, Inc., Corona, CA, USA) have been shown to be acceptable collecting devices for the collection of nasopharyngeal specimens for detection of pertussis by RT-PCR testing.28
US Food and Drug Administration cleared commercial assays
Until a few years ago, there were no US Food and Drug Administration (FDA) cleared NAATs for B. pertussis or other Bordetella species. In the last 4 years, the FDA approved three commercial NAATs for rapid B. pertussis testing, but there is still no FDA-cleared assay for the detection of any other Bordetella species (Table 2).
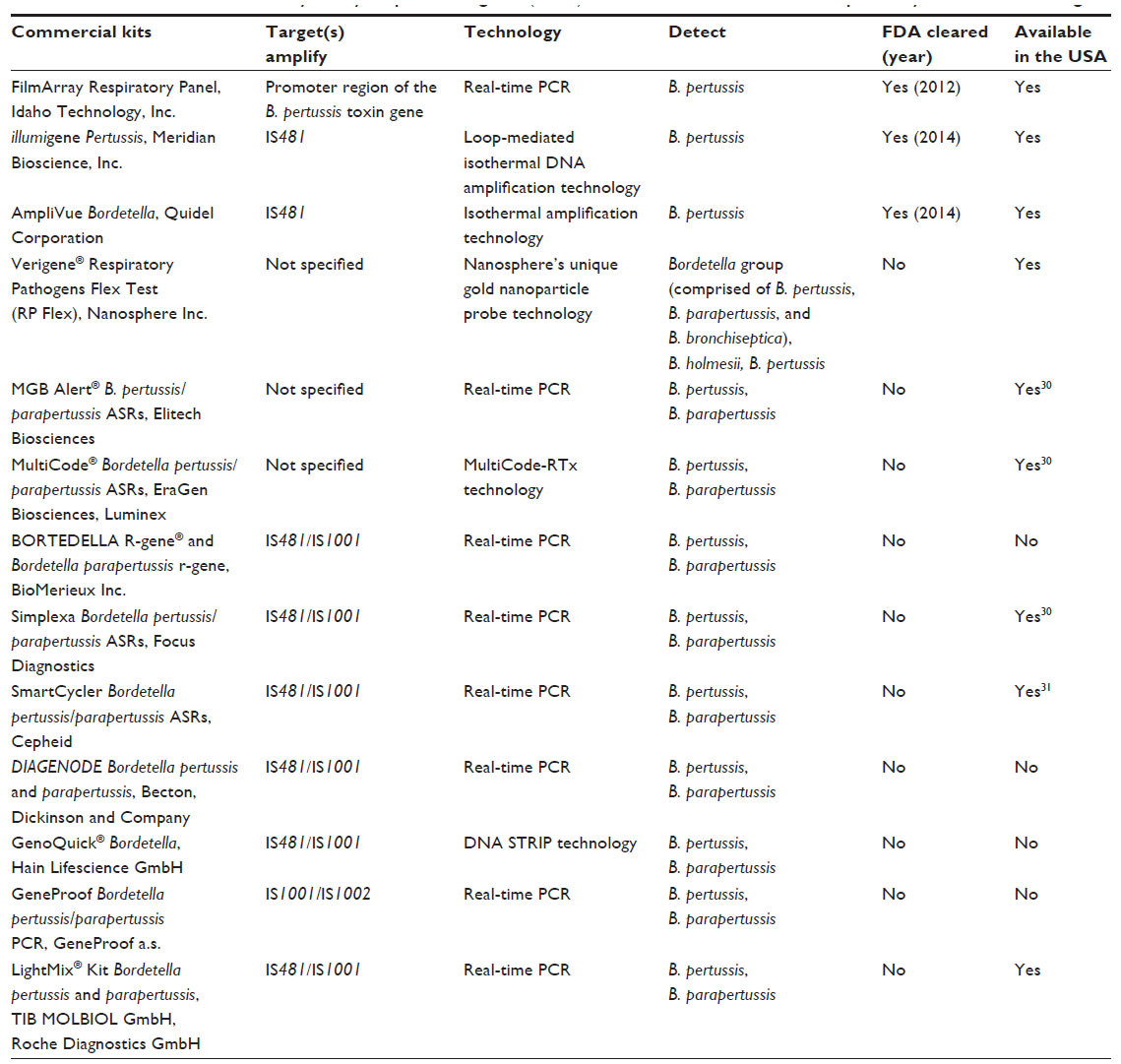 | Table 2 Available commercial assays/analyte-specific reagents (ASRs) for the detection of Bordetella species by nucleic acid testing |
In May 2012, Idaho Technology, Inc., was the first to receive FDA clearance for RT-PCR testing of B. pertussis for its FilmArray Respiratory Panel. It targets the single-copy promoter region of the pertussis toxin gene that is specific for B. pertussis. The product insert reports a sensitivity of 4,000 CFU/mL (~450 CFU/reaction).
In March 2014, Meridian Bioscience, Inc., Cincinnati, OH, USA, received FDA clearance for its new molecular diagnostic test for B. pertussis, on the illumigene® molecular platform. The illumigene Pertussis assay utilizes loop-mediated isothermal DNA amplification technology to detect B. pertussis by targeting the IS481 insertional element of the B. pertussis genome. It claims a sensitivity of 3,265 CFU/mL (1.48 CFU/test). The product insert includes this disclaimer “Respiratory infection with B. pertussis, B. holmesii, or B. bronchiseptica may yield positive test results in IS481 assays”.
In December 2014, Quidel Corporation received clearance from the FDA for its AmpliVue Bordetella assay for the detection of B. pertussis nucleic acids isolated from nasopharyngeal swab specimens. The assay utilizes an isothermal amplification technology of helicase-dependent amplification of the insertion sequence IS481. The assay limit of detection for B. pertussis is 2,358 CFU/mL (3.93 CFU/assay). The product insert mentions cross-reactivity with B. bronchiseptica and B. holmesii.
Laboratory developed assays
Many commercial assays and analyte-specific reagents are available in the market for B. pertussis and/or B. parapertussis detection in clinical specimens, but they are not FDA cleared. Review of the literature comparing the performances of some of the commercial assays to laboratory developed assays shows that the performance of commercial assays varies, some performing better than others.29,30 Any commercial assays or laboratory-developed assays need to be fully validated to demonstrate that the performance of the assay is acceptable for patient testing.31
Automation has become part of molecular testing, and many laboratories are using automated platforms to extract bacterial DNA from respiratory samples, but manual extraction using extraction kits or simple hit lysis are still performed. Not all extraction methods have the same efficiency to extract bacterial DNA, and a comparison between the different methods has yet to be performed to assess the efficiency of each method.32 Manual extraction increases the possibility of DNA cross-contamination. Hit lysis is a very efficient technique to release DNA but does not remove potential PCR inhibitors, and an internal control needs to be added to the RT-PCR reaction to monitor the presence of any PCR inhibitor.
Advantages of NAAT
The use of RT-PCR to diagnose pertussis has improved the sensitivity of diagnosis and decreased the turnaround time to diagnosis, permitting faster treatment and prophylaxis of contacts. It has extended the window period in which testing for pertussis is still reliable up to 58 days into illness.13 Antibiotics do not affect the result of the RT-PCR assays. RT-PCR testing has given us a new understanding of the epidemiology of pertussis in the adolescent and adult population and, thus, has provided better control and prevention of outbreaks.
Drawbacks of NAAT
Contamination is a major problem in testing for pertussis by NAAT. Pseudo outbreaks have been reported with false-positive RT-PCR results due to contamination.33 The contaminant can be introduced during specimen collection or during processing and set up of the RT-PCR assay. RT-PCR assays that use repetitive IS target genes, like the IS481, are more susceptible to contamination than single-gene target assays because of the very high quantity of repeats present in the bacterial genome. To avoid such events, it is important that strategies like unidirectional workflow and quality control (negative and positive controls) be put in place. The other issue in using IS targets is the interpretative dilemma of results where high cycle threshold (Ct) values of more than 35 cycles may represent concentrations of DNA target of less than one bacterial genome per assay reaction.34 The clinical significance of such a low level of bacteria is not clear and clinical correlation is mandatory. A high Ct value could represent a true infection in somebody who had been previously vaccinated, or someone who had received antimicrobial therapy, or it could be due to an inadequate specimen collection in a truly infected person or contamination in performing the assay.35 Laboratories need to define which Ct values they will call a positive, indeterminate, or negative result. High Ct values in NAATs that used IS targets need to be interpreted with caution as they might represent false-positive results and should be analyzed in conjunction with patients’ signs and symptoms and epidemiological information. A false-positive result can mislead patient management and treatment and possibly miss a major diagnosis. It will also have an impact on contact prophylaxis.15
The consequence of miscalling a Bordetella species has not been fully investigated. The significance and the health impact of the detection of B. holmesii in healthy individuals with pertussis-like symptoms are not certain. Controversy as to whether the bacterium is a mere colonizer with minimal pathogenic implication or a true respiratory pathogen is still debated.8,19 The true prevalence of B. holmesii in the population is not known. Its prevalence is difficult to evaluate because the majority of clinical laboratories are using RT-PCR assays that target only the IS481 region that does not discriminate between B. pertussis and B. holmesii. The laboratories that use RT-PCR assays which are species-specific are not attracted to identify B. holmesii because of its unknown significance.
Summary and conclusion
The resurgence of pertussis has been attributed to several factors, one of them being that the numbers of reported cases may have been inflated because of greater awareness of pertussis and the use of NAAT for the detection of pertussis. However, it is clear that this cannot be the only reason for the increase of reported pertussis cases, and other factors like the diphtheria–tetanus–acellular pertussis (DTaP) vaccines not being as effective as the whole-cell vaccines and waning of immunity from vaccination over time may be contributory.36,37 The higher sensitivity of NAAT to detect pertussis has demonstrated that adults who had been vaccinated in childhood were susceptible to pertussis infection. They usually have a milder course of illness and may have an atypical clinical presentation. This suggests waning of immunity to pertussis from vaccination over time. The other age group affected includes children born in the USA after 1997 who received only the acellular vaccine for their primary series and had a faster waning of their pertussis immunity compared to those born in the 1940s to early 1990s who received the whole-cell vaccine.3,7 These observations demonstrated the need for boosters to maintain immunity and the need of a better vaccine that will confer longer immunity against pertussis. Still, the highest burden of disease is seen in infants less than 12 months, and severe and fatal disease continues to occur almost exclusively in infants who are too young, less than 2 months, to be vaccinated against pertussis. During the 2010 pertussis epidemic, the main strategy to protect neonates was “cocooning”, which involved vaccinating all people who are in contact with the child.3 However, this method was not enough to prevent pertussis infection. This is because cocooning does not provide any direct protection (antibodies) to the infant, and it is difficult to ensure that everyone who is around the neonate has received the pertussis vaccine. In 2011, it was shown that antipertussis antibodies from the mother were efficiently transferred to the fetus through the placenta, conferring protection to the vulnerable infants until they are old enough to receive the primary series of DTaP starting at the age of 2 months.38 It is now recommended that every pregnant woman receive Tdap during the third trimester of every pregnancy because antibody levels decline between pregnancies.3,39
The need for a new vaccine that confers better and longer immunity than the acellular pertussis vaccine and that does not have the adverse reactions associated with the whole-cell vaccine is evident. Understanding the epidemiology of pertussis in vaccinated groups of individuals with waning immunity is important for the design of a better vaccine. The diagnosis of pertussis in this group of individuals is challenging because of the nonspecific clinical symptoms they present with. The increased sensitivity of NAAT has permitted us to detect the bacteria in this group of people for whom culture was not sensitive enough. The problem is lack of standardization of testing and that the accuracy of diagnosis varies among laboratories. Different protocols, DNA extraction methods, nucleic acid amplification techniques, and amplification targets are used by laboratories to detect Bordetella species. These factors influence the sensitivity and the accuracy of results.32 Conformity in the diagnostic approaches to detect pertussis is desirable to have a true knowledge of the prevalence of pertussis in the population. It is imperative that laboratories assess the performance of their nucleic acid amplification assay by participating in external assessments to ensure that their results are comparable to their peers.
To achieve better standardization of pertussis testing by RT-PCR, by adaptation of multiplex RT-PCR assays, one can target the IS genes (eg, IS481, IS1000) to confer high sensitivity, and single-target genes specific to Bordetella species (eg, pertussis toxin S1 promoter ptxA-pr or recABH) to achieve high specificity. Multiplex RT-PCR with primers and probes that give high sensitivity and specificity for all four major clinical Bordetella species would be ideal.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization (WHO). Pertussis vaccines: WHO position paper. Wkly Epidemiol Rec. 2010;85(40):385–400. | |
Black RE, Cousens S, Johnson HL, et al; Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet. 2010;375(9730):1969–1987. | |
Winter K, Glaser C, Watt J, Harriman K; Centers for Disease Control and Prevention (CDC). Pertussis epidemic – California, 2014. MMWR Morb Mortal Wkly Rep. 2014;63(48):1129–1132. | |
Centers for Disease Control and Prevention. Epidemiology and Prevention of Vaccine-Preventable Diseases. 13th ed. Washington, DC: Public Health Foundation; 2015. Available from: http://www.cdc.gov/vaccines/pubs/pinkbook/index.html. Accessed July 2, 2015. | |
Centers for Disease Control and Prevention (CDC). Notifiable diseases and mortality tables. MMWR Morb Mortal Wkly Rep. 2015;63:733–746. | |
Cherry JD. Historical perspective on pertussis and use of vaccines to prevent it. Microbe. 2007;2(3):139–144. | |
Cherry JD. Epidemic pertussis in 2012 – the resurgence of a vaccine-preventable disease. N Engl J Med. 2012;367(9):785–787. | |
Pittet LF, Emonet S, Schrenzel J, Siegrist CA, Posfay-Barbe KM. Bordetella holmesii: an under-recognised Bordetella species. Lancet Infect Dis. 2014;14(6):510–519. | |
Aricò B, Rappuoli R. Bordetella parapertussis and Bordetella bronchiseptica contain transcriptionally silent pertussis toxin genes. J Bacteriol. 1987;169(6):2847–2853. | |
Wirsing von König C-H, Riffelmann M, Coenye T. Bordetella and related genera. In: Versalovic J, Carroll KC, Jorgensen JH, Funke G, Landry ML, Warnock DW, editors. Manual of Clinical Microbiology. Vol 1. 10th ed. Washington, DC: ASM Press, Inc.; 2011:739–750. | |
Faulkner A, Skoff T, Martin S, et al; Centers for Disease Control and Prevention. Pertussis. In: Manual for the Surveillance of Vaccine-Preventable Diseases. Atlanta, GA: Centers for Disease Control and Prevention; 2012. Available from: http://www.cdc.gov/vaccines/pubs/surv-manual/chpt10-pertussis.html. Accessed July 2, 2015. | |
Palmer CM, McCall B, Jarvinen K, Nissen MD. Bordetella pertussis PCR positivity, following onset of illness in children under 5 years of age. Commun Dis Intell Q Rep. 2007;31(2):202–205. | |
Stone BL, Daly J, Srivastava R. Duration of Bordetella pertussis polymerase chain reaction positivity in confirmed pertussis illness. J Pediatric Infect Dis Soc. 2014;3(4):347–349. | |
Harvill ET, Goodfield LL, Ivanov Y, et al. Genome sequences of nine Bordetella holmesii strains isolated in the United States. Genome Announc. 2014;2(3):e00438-14. | |
Loeffelholz M. Towards improved accuracy of Bordetella pertussis nucleic acid amplification tests. J Clin Microbiol. 2012;50(7):2186–2190. | |
Tizolova A, Guiso N, Guillot S. Insertion sequences shared by Bordetella species and implications for the biological diagnosis of pertussis syndrome. Eur J Clin Microbiol Infect Dis. 2013;32(1):89–96. | |
Van der Zee A, Vernooij S, Peeters M, van Embden J, Mooi FR. Dynamics of the population structure of Bordetella pertussis as measured by IS1002-associated RFLP: comparison of pre- and post-vaccination strains and global distribution. Microbiology. 1996;142(pt 12):3479–3485. | |
Antila M, He Q, de Jong C, et al. Bordetella holmesii DNA is not detected in nasopharyngeal swabs from Finnish and Dutch patients with suspected pertussis. J Med Microbiol. 2006;55(pt 8):1043–1051. | |
Guthrie JL, Robertson AV, Tang P, Jamieson F, Drews SJ. Novel duplex real-time PCR assay detects Bordetella holmesii in specimens from patients with pertussis-like symptoms in Ontario, Canada. J Clin Microbiol. 2010;48(4):1435–1437. | |
Riffelmann M, Wirsing von König CH, Caro V, Guiso N; Pertussis PCR Consesus Group. Nucleic acid amplification tests for diagnosis of Bordetella infections. J Clin Microbiol. 2005;43(10):4925–4929. | |
Njamkepo E, Bonacorsi S, Debruyne M, Gibaud SA, Guillot S, Guiso N. Significant finding of Bordetella holmesii DNA in nasopharyngeal samples from French patients with suspected pertussis. J Clin Microbiol. 2011;49(12):4347–4348. | |
Litt DJ, Jauneikaite E, Tchipeva D, Harrison TG, Fry NK. Direct molecular typing of Bordetella pertussis from clinical specimens submitted for diagnostic quantitative (real-time) PCR. J Med Microbiol. 2012;61(pt 12):1662–1668. | |
Qin X. Resurgence of pertussis and its laboratory diagnosis. Clin Microbiol Newsl. 2015;37(9):69–76. | |
Centers for Disease Control and Prevention (CDC). Pertussis – United States, 2001–2003. MMWR Morb Mortal Wkly Rep. 2005;54(50):1283–1286. | |
Kretsinger K, Broder KR, Cortese MM, et al; Centers for Disease Control and Prevention; Advisory Committee on Immunization Practices; Healthcare Infection Control Practices Advisory Committee. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP) and recommendation of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC), for use of Tdap among health-care personnel. MMWR Recomm Rep. 2006;55(RR–17):1–37. | |
Jerris RC, Williams SR, MacDonald HJ, Ingebrigtsen DR, Westblade LF, Rogers BB. Testing implications of varying targets for Bordetella pertussis: comparison of the FilmArray Respiratory Panel and the Focus B. pertussis PCR assay. J Clin Pathol. 2015;68(5):394–396. | |
Cloud JL, Hymas W, Carroll KC. Impact of nasopharyngeal swab types on detection of Bordetella pertussis by PCR and culture. J Clin Microbiol. 2002;40(10):3838–3840. | |
Arbefeville S, Ferrieri P. Comparison of rates of positivity for Bordetella pertussis by real-time PCR between specimens collected with rayon swabs on aluminum wire shaft in Amies gel with charcoal and specimens collected with flocked swabs in universal viral transport medium during an epidemic. J Clin Microbiol. 2014;52(7):2656–2658. | |
Lanotte P, Plouzeau C, Burucoa C, et al. Evaluation of four commercial real-time PCR assays for detection of Bordetella spp. in nasopharyngeal aspirates. J Clin Microbiol. 2011;49(11):3943–3946. | |
Hassan F, Hays L, Bell J, Selvarangan R. Evaluation of 3 analyte-specific reagents for detection of Bordetella pertussis and Bordetella parapertussis in clinical specimens. Diagn Microbiol Infect Dis. 2014; 80(3):181–184. | |
Arbefeville S, Levi MH, Ferrieri P. Development of a multiplex real-time PCR assay for the detection of Bordetella pertussis and Bordetella parapertussis in a single tube reaction. J Microbiol Methods. 2014;97:15–19. | |
Williams MM, Taylor TH, Warshauer DM, Martin MD, Valley AM, Tondella ML. Harmonization of Bordetella pertussis real-time PCR diagnostics in the United States in 2012. J Clin Microbiol. 2015;53(1):118–123. | |
Mandal S, Tatti KM, Woods-Stout D, et al. Pertussis pseudo-outbreak linked to specimens contaminated by Bordetella pertussis DNA from clinic surfaces. Pediatrics. 2012;129(2):e424–e430. | |
Guthrie JL, Seah C, Brown S, Tang P, Jamieson F, Drews SJ. Use of Bordetella pertussis BP3385 to establish a cutoff value for an IS481-targeted real-time PCR assay. J Clin Microbiol. 2008;46(11):3798–3799. | |
Papenburg J, Fontela P. What is the significance of a high cycle threshold positive IS481 PCR for Bordetella pertussis? Pediatr Infect Dis J. 2009;28(12):1143; author reply Waters V, et al. 1143–1144. | |
Cherry JD. Tetanus-diphtheria-pertussis immunization in pregnant women and the prevention of pertussis in young infants. Clin Infect Dis. 2015;60(3):338–340. | |
Cherry JD. Pertussis: challenges today and for the future. PLoS Pathog. 2013;9(7):e1003418. | |
Warfel JM, Papin JF, Wolf RF, Zimmerman LI, Merkel TJ. Maternal and neonatal vaccination protects newborn baboons from pertussis infection. J Infect Dis. 2014;210(4):604–610. | |
Centers for Disease Control and Prevention (CDC). Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (Tdap) in pregnant women – Advisory Committee on Immunization Practices (ACIP), 2012. MMWR Morb Mortal Wkly Rep. 2013;62(7):131–135. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.