")
Back to Journals » Journal of Healthcare Leadership » Volume 6
Optimizing enactment of nursing roles: redesigning care processes and structures
Authors Jackson K, White D, Besner J, Norris J
Received 27 August 2013
Accepted for publication 29 October 2013
Published 26 February 2014 Volume 2014:6 Pages 1—14
DOI https://doi.org/10.2147/JHL.S53603
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 8
Karen Jackson,1 Deborah E White,2 Jeanne Besner,1 Jill M Norris2
1Health Systems and Workforce Research Unit, Alberta Health Services, Calgary, Alberta, Canada; 2Faculty of Nursing, University of Calgary, Calgary, Alberta, Canada
Background: Effective and efficient use of nursing human resources is critical. The Nursing Role Effectiveness Model conceptualizes nursing practice in terms of key clinical role accountabilities and has the potential to inform redesign efforts. The aims of this study were to develop, implement, and evaluate a job redesign intended to optimize the enactment of registered nurse (RN) clinical role accountabilities.
Methods: A job redesign was developed and implemented in a single medical patient care unit, the redesign unit. A mixed-methods design was used to evaluate the job redesign; a second medical patient care unit served as a control unit. Data from administrative databases, observations, interviews, and demographic surveys were collected pre-redesign (November 2005) and post-redesign (October 2007).
Results: Several existing unit structures and processes (eg, model of care delivery) influenced RNs' ability to optimally enact their role accountabilities. Redesign efforts were hampered by contextual issues, including organizational alignment, leadership, and timing. Overall, optimized enactment of RN role accountabilities and improvements to patient outcomes did not occur, yet this was predictable, given that the redesign was not successful. Although the results were disappointing, much was learned about job redesign.
Conclusion: Potential exists to improve the utilization of nursing providers by situating nurses' work in a clinical role accountability framework and attending to a clear organizational vision and well-articulated strategic plan that is championed by leaders at all levels of the organization. Health care leaders require a clear understanding of nurses' role accountabilities, support in managing change, and leadership development opportunities.
Keywords: nursing scope of practice, nursing role enactment, nursing role accountabilities, job redesign, leadership
Introduction
The growing shortage of health professionals, increasing pressure to contain costs and reduce wait times, and overall demand to improve quality of care have placed increasing pressure on health care organizations internationally. In particular, countries including Canada, the United Kingdom, Australia, and the United States of America are seeking solutions to nursing shortages and sustaining care quality.1 Potentially aggravating nursing shortages and contributing to poor patient outcomes is the widely acknowledged situation that registered nurses (RNs) are not effectively utilized in many practice settings.2 As RNs represent the largest group of health professionals involved in delivery of health care, attention to the effective and efficient utilization of nursing human resources is critical.
Well-established findings from organizational literature inform us that the design of work can be a factor in job dissatisfaction, underutilization of professional knowledge and skills, and workload.3 In the 1990s, health care reform efforts proposed redesign, restructuring, and reengineering. Unfortunately, these efforts achieved limited success, in part due to a focus on cost containment.4,5 Sibbald et al6 reported that nursing redesigns focused on increasing the depth of a job, substituting nurses by another type of worker, and introducing new types of workers. Their analysis of the impact of these redesigns revealed a lack of good evidence on the scope, efficiency, and effectiveness of the changes.
Recently, numerous health care organizations have adopted lean thinking (examination of structures and processes to maximize value and eliminate waste) to primarily address operational inefficiencies, neglecting aspects such as organizational climate, team learning and problem solving skills, and workforce development.7 Many lean projects related to bedside nursing have also focused on eliminating work inefficiencies6 (eg, accessibility of supplies, duplication of documentation), reducing time spent in nonclinical activity (eg, delivering food trays, stocking supplies), and/or minimizing workflow interruptions (eg, during medication administration). The intent in most cases was to achieve more nursing time at the bedside; however, this has not necessarily been the outcome for all organizations.8
Campbell and Briley4 suggest that redesign in health care requires a systematic and integrated approach to transformation that includes improvement in systems and processes (eg, allocation of appropriate services and resources at the point of care), physical geography (eg, location of medication stations), models of care delivery (eg, modified primary nursing), and innovation in cultures of care delivery (eg, style of management). If RNs are to optimally contribute to patient outcomes, they need to be supported by appropriate structures and processes.
RNs are knowledge workers who apply nursing science principles to guide their clinical judgment and decision-making.9 Their work cannot simply be defined on the basis of time spent in direct care at the bedside. Spending more time in direct care activities does not necessarily equate to more appropriate utilization of nursing knowledge and skill. For example, spending more time in direct personal care activities such as feeding does not always require the knowledge and skill of an RN, whereas collaborating with another health care provider to prepare for discharge or transition of care, while not an actual direct care activity, does benefit the patient and draws on nursing knowledge. As Upenieks et al suggest, utilization of nurses “must be evaluated in terms of value-added care, a vision that goes beyond direct care activities.”10
Irvine et al11 have developed the Nursing Role Effectiveness Model (NREM) to conceptualize and guide assessment of the roles nurses undertake. Based on Donabedian’s12 structure–process–outcome model of quality care, the NREM contends that specific outcomes are linked to key clinical nursing role accountabilities (see Figure 1). Rather than addressing tasks and skills, this model conceptualizes nursing practice in terms of role accountabilities, considers contextual variables, and incorporates the needs of the patient population in determining appropriate enactment of nurses’ roles. The model incorporates key elements of nurses’ clinical roles, including comprehensive assessment, nursing interventions (eg, medications and treatments), coordination of care, and patient/family teaching. These role accountabilities contribute to effective management of patients’ health and comorbidities, recognition of potential social and physical risks, enhancement of patients’ and families’ knowledge, and optimization of self-care capacity. Testing of the NREM by Doran et al13 supported the premise that RN role performance explained the relationship between structure variables (eg, patient characteristics) and achievement of patient outcomes (eg, hospital readmission). Using the NREM to conceptualize nursing role enactment has the potential to inform redesign efforts.
 | Figure 1 Adapted from the Nursing Effectiveness Model.11 |
Aims
The aims of this study were to develop, implement, and evaluate a job redesign intended to optimize the enactment of RN clinical role accountabilities. We hypothesized that, by targeting NREM structures and processes through the job redesign, patient outcomes would improve. The intent of this article is to highlight structures and processes necessary to support enactment of RN clinical role accountabilities, as well as the successes and challenges of the redesign process.
Methods
Design
A mixed-methods design was used in this study. Redesign experts agree that change is most easily implemented when it is the result of a participatory process involving those directly affected by the change.14 The research was predicated on a participatory approach. Participatory approaches focus on conducting research with people,15 emphasizing collaboration between participants and researchers through the refinement of research questions, collection of data, analysis and interpretation of findings, and dissemination of results.16,17 A participatory approach was used to plan and implement a redesign on one patient care unit. The approach was guided by principles of voluntary participation, collaborative decision-making, and an iterative cycle of planning, acting, observing, and reflecting.18,19 Researchers, along with unit managers and staff from one unit (herein called the redesign unit), sought to fully enact the roles of RNs through the redesign of work. Unit managers and staff were involved in deliberative discussions related to data acquisition, analysis, and interpretation, as well as actively planning and implementing desired changes. The impact of the redesign on nursing role enactment was evaluated by comparing the redesign unit to a second patient care unit that served as a control unit. Data were collected during two time frames (pre-redesign and post-redesign). The data collection time frames were separated by 2 years, allowing the job redesign to be planned and implemented during year 1, with time to integrate and sustain the changes during year 2.
Setting and participants
A convenience sample of RNs on two general medical units in a large tertiary hospital in Alberta, Canada participated in the study. Administration indicated the units were agreeable and available to participate. The two units were selected because of comparable numbers of beds, patient population, and number and mix of staff. As the nursing staff mix on both units were comprised of RNs and health care aides (HCAs), HCAs were also included in the sampling frame. Staff were recruited through presentation and poster advertisements; all participants volunteered and consented to the study.
Data collection
Data were collected through administrative databases, observations, interviews, and demographic surveys during two time frames (pre-redesign in November 2005 and post-redesign in October 2007). The data were used to provide participating staff with rationale for the redesign, inform the redesign, and evaluate outcomes as a result of implementing a redesign. While data collection and analysis are described below, further detail related to methods is available elsewhere.20,21
Administrative databases
Baseline descriptive information about structural elements such as patient population characteristics (eg, primary diagnosis, age), as well as patient outcomes (eg, inpatient readmission and emergency department visits within 90 days of discharge, length of stay), were abstracted from corporate administrative databases. Toad for Oracle software (v 9.1; Dell Software, Aliso Viejo, CA, USA) facilitated data abstraction by a data repository expert.
Observations
The work activities of RNs and HCAs were observed across five day and five evening shifts and occurred over a 7.75-hour shift. Night shifts were not included for feasibility. It was also acknowledged that some nursing role accountabilities, such as patient and family assessment and support (eg, psychosocial assessment, patient/family teaching), would be limited during night shifts. Time spent on personal breaks was excluded. The resulting mean observation time was 6.52 hours for RNs and 5.81 hours for HCAs. In total, 71 RN and 33 HCA shifts (79 unique individuals) were observed. Overall, 27,780 minutes (463 hours) and 11,520 minutes (192 hours) were documented for RNs and HCAs, respectively.
Observation of nursing work was captured using Function Analysis™ (FA) (version 4; Workflow Integrity Network, Duncan, BC, Canada), a palm pilot electronic tool to capture work activities and workflow. Twelve trained observers used palm pilots to document participants’ use of time on a second-by-second basis across a variety of predefined activities. The FA technology was developed by a member of the research team, and has been used in other care delivery redesign projects.22 Observer training occurred in both pre- and post-redesign, since the majority of observers were not consistent across the two time frames. Observers were trained by an FA expert during 2 half-days in a classroom followed by hands-on practical training over 1 half-day. To ensure internal consistency among the observers, the FA expert monitored the observers as they recorded activities at random times during training and data collection time frames.
RN activities were mapped to categories guided by a modified NREM,11 including biomedical assessment, patient and family assessment and support, medications and treatments, coordination of care, and activities of daily living and personal care. HCA activities were mapped to the following categories: activities of daily living and personal care, patient support, coordination of basic care, and room cleaning/organizing. Additional categories, such as documentation, administrative tasks, and travel, were also included, as these are part of nursing work. Descriptions of unit processes and nursing work were augmented with observer field notes and weekly tracking of contextual information (eg, bed occupancy rate, staff shortages, and other environmental pressures).
Interviews
Participants who agreed to be observed were also interviewed. Using a semi-structured interview guide, the trained observers elicited information from nursing staff about judgments and decisions that influenced delivery of care. To avoid interrupting care delivery, interviews were conducted at the end of the shift. Interviews were audio-recorded and transcribed verbatim. All observers were asked to complete daily field notes and participate in a group interview subsequent to data collection to supplement the observation data. The intent was to capture perspectives that the observer experienced or reflected upon in the course of collecting data.
Demographic survey
Participants were asked to complete a demographic questionnaire (including age, education, years of nursing experience, and professional designation) to describe provider structural elements.
Data analysis
Quantitative data were cleaned and descriptive statistics were calculated using Stata S/E software (v 10.0; StataCorp LP, College Station, TX, USA). Seconds spent in specific job activities were summed per shift, and mean time (minutes) for each activity per shift was calculated. As the process and patient outcomes were continuous variables, linear regression analyses were carried out in order to address statistical differences as well as magnitude and direction of change. Linear regression analyses of the observation data were performed to look at differences in outcome variables between units and over time and the interaction between units and time (α=0.05). Both unit and time differences were modeled as bivariable values, with the control unit and pre-redesign time period as the reference groups, respectively. The interaction term was modeled as the effect of the redesign unit post-redesign. If there was evidence of non-normality in the model residuals, we used appropriate transformations. All else constant, the regression coefficients for each effect (unit, time, redesign) represent the difference between the mean changes in the outcome variable.
To facilitate data management, interview transcripts were imported and coded using the QSR N6 program (QSR International Pty Ltd, Doncaster, Australia). The approach to analysis was a collaborative effort amongst the multidisciplinary members of the research team. Three experienced qualitative researchers and two research assistants completed data-coding and analysis through a series of iterative phases.23
Ethical review
Ethical approval was obtained through the University of Calgary Conjoint Health Research Ethics Board. All participants signed informed consents. All administrative data and transcripts were stripped of identifiers prior to analyses, and participants were assigned a code number. To ensure the confidential management of all data, data were securely kept in locked file cabinets or password-protected computer drives.
Results
The redesign unit had 28 beds, while the control unit had 32 beds. The bed occupancy on the unit was 100%. The majority of patients discharged from each unit were over the age of 70 years. The mean age for patients on each unit was 75 years. Each patient had one or more frequently recurring diagnoses (eg, chronic pulmonary obstructive disease, pneumonia, hypertension, dementia, heart failure, urinary system disorder). On the control unit, patients’ average length of stay was 10 days, whereas this was 11 days on the intervention unit 11. The majority of patients were discharged home.
Nursing staff members from each unit (n=120) consented to participate in the study; 111 of them completed the demographic survey (92.5% response rate). Over 80% of the staff were female (see Table 1 for other staff characteristics). From the 79 participants who were observed, 77 also completed interviews.
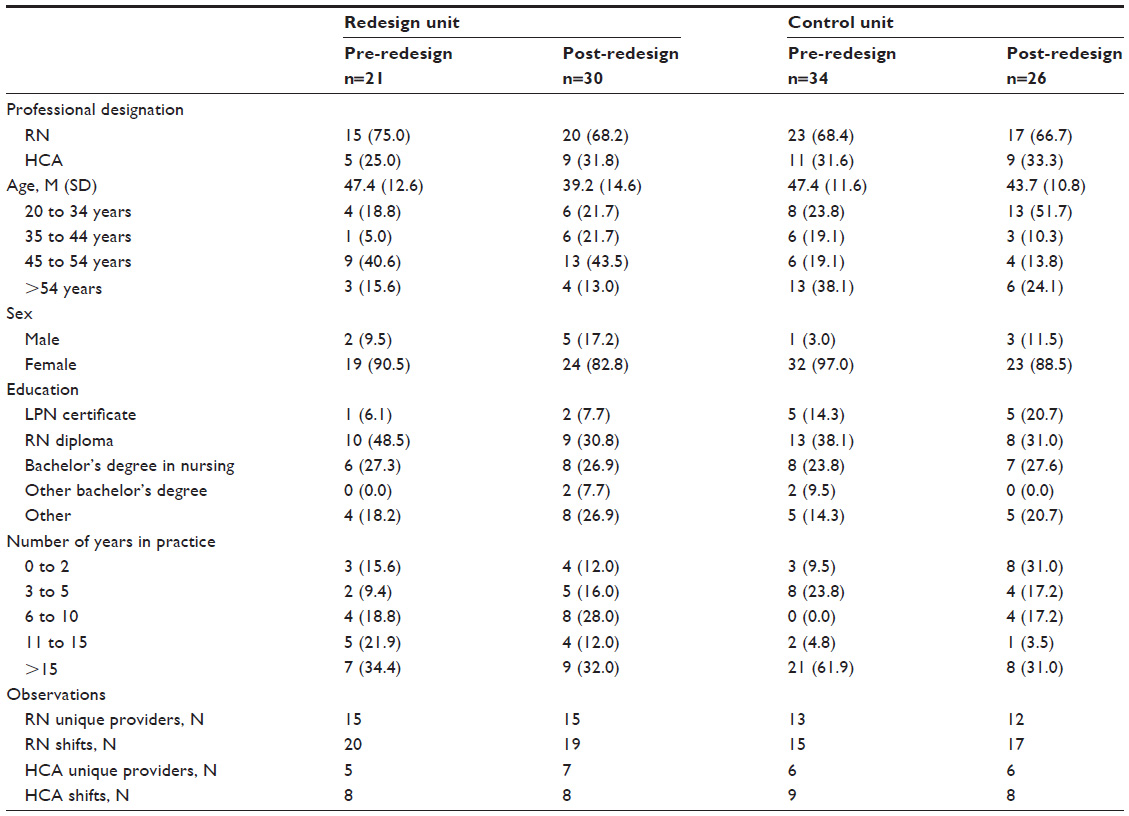 | Table 1 Demographics of study sample of nursing providers |
Development phase: redesign unit
The redesign was guided by baseline data (administrative, observation, and interview), the NREM,11 and evidence from organizational change principles, including: 1) staff engagement throughout the entire redesign process;24–27 2) articulating a clear vision of nursing role accountabilities;28,29 and 3) understanding structures and processes that contribute to optimal enactment of one’s role accountabilities.26,28 Context, including organizational alignment and readiness for change. were also considered.30
A clinical leader (RN) and a change team consisting of managers, RNs, HCAs, and researchers led the change process. The Power to Change Team, as they were named, was intimately engaged in the development of a unit-based strategic plan. This group met biweekly over a 4-month period, and meetings were recorded to describe planning and implementation of change on the unit. At times, representatives of regulatory bodies and allied health professionals were invited to these meetings to inform redesign efforts.
Building peoples’ understanding and commitment to change is critical to inspiring a shared vision.31 Research has revealed that nurses’ work is poorly understood by colleagues in other disciplines, health care administrators, and, unfortunately, by some nurses themselves.32 To provide rationale for the redesign, nursing staff required an understanding of the current enactment of nursing (RN, HCA) role accountabilities. As well, they needed to understand the characteristics and needs of the patient population on the unit in order to critically reflect on time spent in each activity. The following data specific to the redesign unit were shared with The Power to Change Team.
Structure
Patient characteristics
From the administrative data, staff were not surprised to learn that 70% of patients were elderly and had one or more chronic diseases, but they were unaware that their patients experienced a high rate of hospital readmission (26%) and emergency department visits (34%) within 90 days of discharge. Moreover, some of their patients experienced potentially preventable health concerns, such as fluid and electrolyte imbalance, pneumonia, and fluid overload, subsequent to admission to the unit.
RN provider characteristics
Data from the demographic survey indicated that 27.3% (n=6) of RNs had a bachelor’s degree in nursing, while 48.5% (n=10) had a diploma. Approximately 55% (n=12) had greater than 10 years of clinical experience.
Unit characteristics
The model of care on the unit was a modified primary nursing model, in which one RN was responsible for the majority of care for their assigned patients during their shift. Interview data revealed that HCAs supported the work of two or more RNs; however, he/she was left to determine priorities. Nursing providers reported rarely working together as a team to plan, coordinate, and implement care:
The barriers I suppose are communication or lack thereof. If you’re not communicating the needs to the nursing attendant [HCA], they don’t always know what the expectations are. So communication is important for teamwork.
In addition, RNs and HCAs began their shift at different times, which contributed to reactive and ad hoc communication; this contributed to frequent interruptions throughout the shift (three to four interruptions/hour), as demonstrated in the observation data. These interview and observation findings revealed less-than-optimal interactions and workflow between RNs and HCAs, highlighting that current structures and processes were ineffective. In particular, staff raised questions as to whether optimized role enactment and improved patient outcomes could be achieved without reconsidering the model of nursing care delivery on the unit.
Process
Role accountabilities
Staff were very interested in the data describing current nursing role enactment measured through the FA methodology. The observation data not only provided a compelling quantitative description of time allocated to various activities, but also validated previous qualitative research that highlighted that a large proportion of nurses were not working to their full scope of practice.33 Baseline observation data (see Table 2) revealed that patient assessment by RNs was primarily focused on biomedical aspects (8.0%), with limited time spent on patient and family assessment and support (4.6%). Substantial time was allocated to activities related to personal care (13.0%), medications/treatments (13.2%), and coordination of care (12.6%). While one might expect that RNs would spend time managing the sequence, timing, and/or effectiveness of care from admission to discharge with other providers, such as allied health providers, physicians, or community programs, much of the time was spent coordinating the daily provision of care with HCAs or other RNs. A large proportion of time was also allocated to documentation and/or review of patient information (20.9%), travel (12.8%), and other work activities (eg, cleaning, administrative tasks [9.3%]). RNs acknowledged that they were overwhelmed with performing regulated activities (eg, medication administration) and felt unable to attend to the comprehensive needs of patients given existing workloads. HCA observation data confirmed that a substantial amount of time was spent in activities of daily living and personal care (33.5%), coordination of care with the RN and/or other HCAs (20.2%), travel (16.4%), and cleaning/organizing patients’ rooms (12.3%). HCAs and others identified that HCAs required continuing education to address standardization in competencies such as skin care and documentation of fluid intake and urinary output.
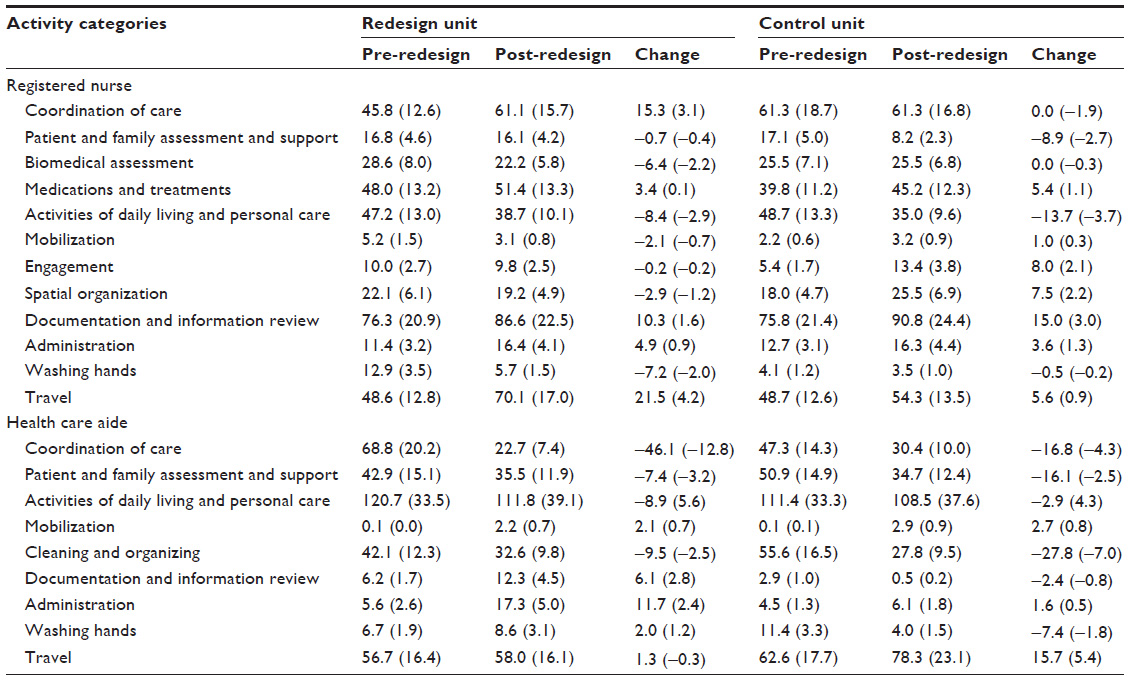 | Table 2 Minutes per shift on activities related to clinical role accountabilities and other work pre- and post-redesign |
The above mentioned data, supplemented with a literature review related to the needs of the patient population (eg, discharge planning, chronic disease management, geriatric care, and predictors of hospital readmission), provided clear evidence of the gap between ideal and actual role enactment and legitimized the need for change. The use of data in telling a compelling story helped overcome potential resistance to change and facilitated staff discussion about needed change:
After I looked at the data, I thought, boy, there is a lot of room to do a lot of things … to change a lot of things for the better or to start getting things where you could focus more on what we’re supposed to be doing a lot of the time.
Implementation phase: redesign unit
The change team worked with unit staff to identify priorities for change and associated strategies (see Table 3). Priorities and strategies were informed by baseline data, presentations by clinicians with expertise in gerontology, and research literature.
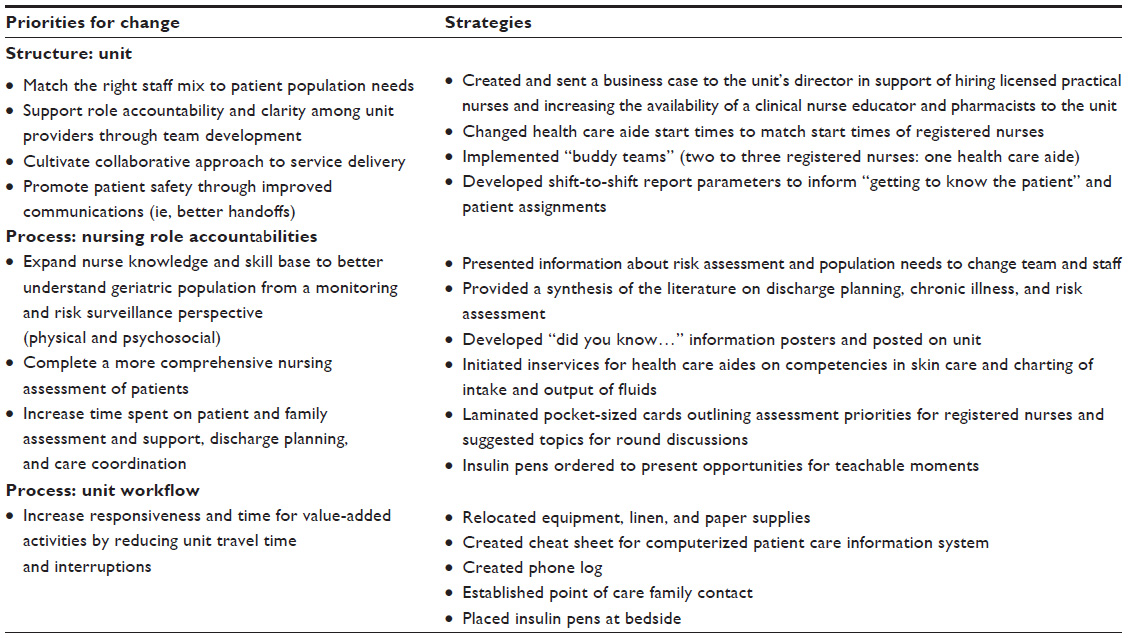 | Table 3 Unit-based strategic plan |
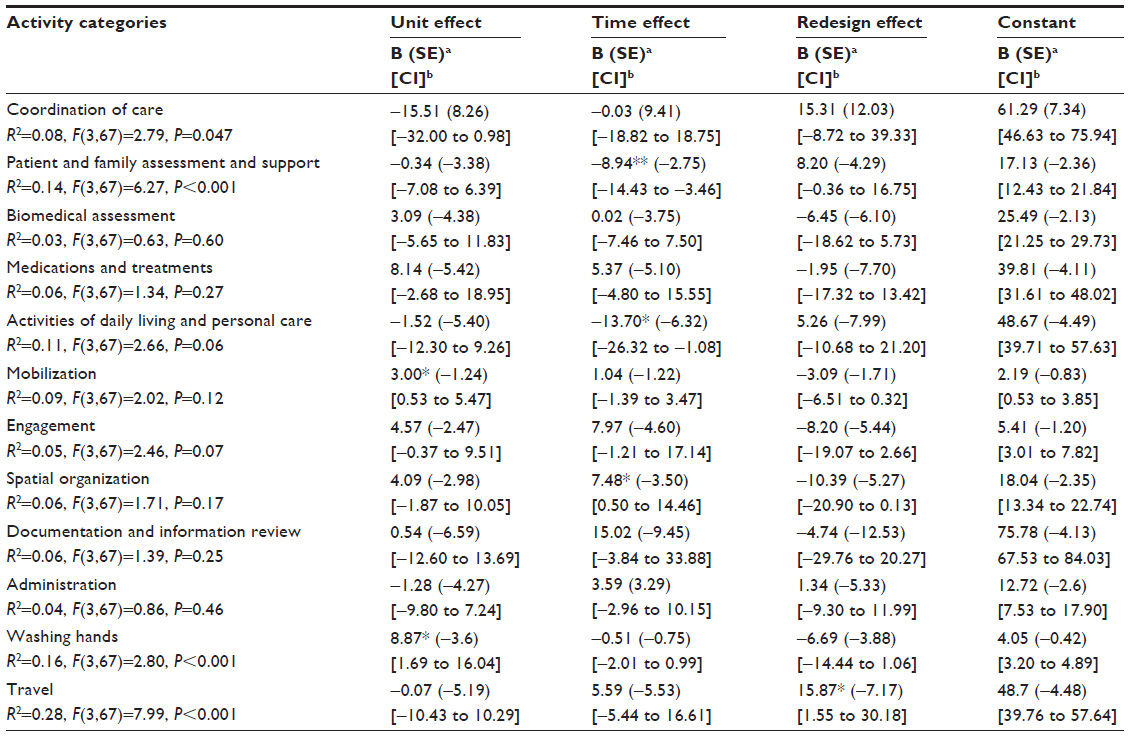 | Table 4 Bivariate regression results: registered nurse observation data |
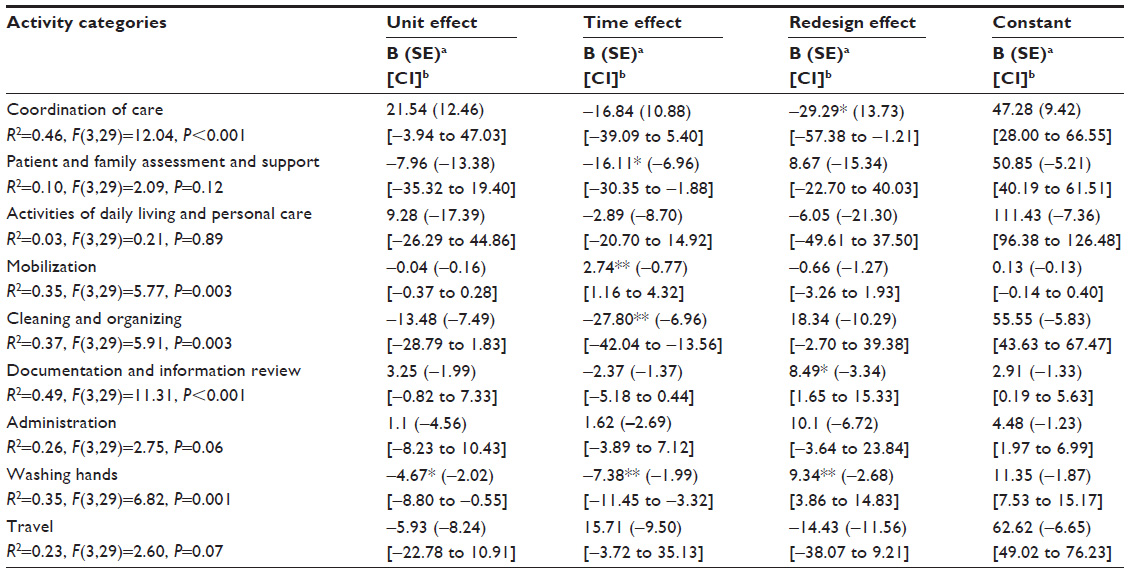 | Table 5 Bivariate regression results: health care aide observation data |
Structure
Unit
Two primary strategies were identified to strengthen unit structures: 1) recruit more RNs; or 2) hire licenced practical nurses (LPNs), who have legislated authority to carry out many of the regulated activities, as a new provider to the unit and to complement the mix of nursing staff. A critical shortage of RNs made the first option unrealistic. Published evidence33,34 demonstrating better patient outcomes associated with higher proportions of RN care when compared with models containing higher levels of LPN care and unregulated care providers raised concerns among some staff about opting for a mix of RNs, LPNs, and HCAs on the nursing team. It was nonetheless recognized that hiring more RNs would do nothing to overcome the inefficiency inherent in having RNs perform work that, in many instances, could be assigned to other health care providers, which ultimately contributes to job dissatisfaction. With these concerns in mind, there was growing recognition of the need to implement a new care delivery model. Staff identified that one of the redesign strategies should focus on increased HCA involvement in documenting fluid intake and urinary output.
Implementing a collaborative nursing model of care wherein RNs, LPNs, and HCAs together plan, implement, and evaluate the care of a group of patients for whom they are collectively accountable was seen as an approach to potentially align provider knowledge and competencies with the needs of the patient population, as well as promote team respect and communication. An important first step was to change HCA shift times to coincide with those of RNs. As there were no LPNs on the unit, two to three RNs and one HCA formed buddy teams to provide care. Development of the buddy teams was guided by literature that suggested that rounding contributes to improved communication, collaboration, and coordination, as well as nursing satisfaction.35 Buddy teams proactively planned care by conducting a nursing team round at the beginning of the shift with their assigned patients.
Process
Role accountabilities
Researchers and staff brainstormed strategies to assist RNs with achieving optimal role enactment (ie, spending more time providing care related to monitoring and surveillance of risk factors in the geriatric population, comprehensive patient assessment, support for patients and their families across care transitions). Patient population profiles heightened staff awareness of the predominance of patients who were elderly with multiple chronic diseases. This realization highlighted the lack of gerontology expertise amongst the providers on the unit. Nursing staff wanted to improve patient outcomes (eg, readmission rates). They suggested improving their knowledge of common risk factors for elderly patients and focusing on surveillance and monitoring of those risks. In addition, RNs identified the need to provide more attention to completing comprehensive patient assessments (including psychosocial aspects), patient and family teaching and support, and discharge planning.
A variety of strategies were employed to assist staff in providing more optimal care. One strategy was the creation of a laminated, pocket-sized card to aid buddy teams with focusing their assessment and care planning on patients’ comprehensive needs. Another strategy involved team members posting “did you know” facts about the needs of the elderly in areas on the unit frequented by staff. In a third strategy, staff attended an education session by a geriatric nurse practitioner aimed at increasing staff knowledge about risk factors associated with the elderly. RNs requested further inservices on geriatric assessment, identifying that this should be a required competency for all RNs on the unit. Unfortunately, the RN inservices were not held due to staff shortages on the unit and a lack of available education resources. Additional inservices with HCAs, as requested by staff, were able to occur, and these focused on improved skin care competency and standardization in charting urinary intake and output.
Workflow
One predominant priority identified by staff involved space and technology issues (eg, time spent in travel, availability and functionality of equipment). Observation data showed that both RNs and HCAs spent a large amount of time in travel, and that travel resulted in an average of three to four interruptions per hour. Staff identified and implemented strategies to reduce travel time and improve the flow of work. Strategies included the relocation of supplies closer to the point of care and use of a phone log, whereby phone calls from families were recorded and then returned when the RN was available. This latter strategy was aimed at reducing interruptions and travel.
Evaluation phase
Structure
Unit
Staff on the redesign unit reflected positively on the new team approach to care. They noted a reduction in the heavy use of call bells. HCAs felt more valued as colleagues:
I think that was one of the best things […] I feel like we are more a part of the team.
RNs felt they had permission to consult with each other about patient care, whereas, prior to implementation of buddy teams, they were concerned about interrupting their colleagues. They also suggested that “knowing the patient” was enhanced:
I’m certainly more comfortable with my buddy’s patients as well, because you do get to know them, and certainly if you know the patients, I guess, if you have to make any decisions while your buddy is on break, it’s easier to make that decision.
Overall, the implementation of buddy teams increased RNs’ and HCAs’ sensitivity to patients’ health needs, facilitated decision-making, and enhanced awareness of their colleagues’ workloads. It was perceived by most nursing providers that buddy teams had a positive impact on teamwork, job satisfaction, coordination of care, communication, and understanding of others’ roles:
Yeah I think it [buddy teams] has really strengthened the teamwork, and I think there’s more job satisfaction, just being in the know a little bit more about what’s going on with another group of patients. And it’s definitely been good. And there’s been a little bit more of getting to know each other too with it.
Post-redesign observers commented that the redesign unit was more proactive in terms of team communication, noting, in particular, that care planning occurred between nursing team members at the beginning of a shift: “it was a lot more organized” on the redesign unit, while “there wasn’t that pre-planning” on the control unit. One observer commented on a HCA’s contribution to nursing team communication, saying, “she wasn’t on the periphery […] it was a team,” while, on the control unit, “communication was very limited.” Although not unexpected, improvement in teamwork, team communication, role clarity, and respect was not expressed by participants on the control unit.
Process
Role accountabilities
Over time, RNs on both units spent significantly less time on activities of daily living/personal care (redesign =–2.9%, control =–3.7%, t[67]=–2.17, P=0.03) and patient and family assessment and support (redesign =–0.4%, control =–2.7%, t[67]=–3.25, P=0.002). In terms of HCAs, both units increased time spent purposefully mobilizing patients (redesign =0.7%, control =0.8%, t[29]=3.55, P=0.001). There were redesign effects for coordination of care activities (redesign =–12.8%, control =–4.3%, t[29]=–2.13, P=0.04), documentation and information review (redesign =2.8%, control =–0.8%, t[29]=2.54, P=0.02), and time spent hand-washing (redesign =1.2%, control =–1.8%, t[29]=3.49, P=0.002). It was apparent that these collective small changes were not enough of a “dose” to change the overall distribution of time spent in other value-added activities. Indeed, it was disappointing for the RNs that they were unable to effect changes in the amount of time spent on comprehensive patient assessment or support for patients and their families across care transitions despite the redesign efforts.
Workflow
Visitors to the redesign unit (other hospital staff and research team members) noted that the unit appeared “less chaotic” and “better organized.” For RNs, there was a redesign effect for time spent in travel, in which RNs on the redesign unit spent more time travelling following the redesign (redesign =4.2%, control =0.9%, t[67]=2.21, P=0.03). Over time, HCAs on both units spent less time in cleaning/organizing (redesign =–2.5%, control =–7.0%, t[29]=–3.99, P<0.001). Providers were interrupted between three and four times per hour, the mean of which did not change in either unit over time.
Patient outcomes
It was anticipated that, if RNs were to spend more time on clinical role accountabilities, patient outcomes would be positively impacted. There were no significant improvements in either unit over time.
Discussion
Using a participatory approach to redesign engages the hearts and minds of those who will be implementing practice change. In this study, quick wins, such as minimizing perceived inefficiencies related to location of supplies and equipment, promoted staff engagement and the change team’s feelings of success. With a sense of empowerment, the change team implemented buddy teams, which were viewed as a more proactive approach to organizing and coordinating care amongst the nursing team. Buddy team success was reflected in the significant decrease of time spent in coordination of care and travel by HCAs on the redesign unit as well as in staff feelings of improved teamwork and collaboration. As well, the significant increase spent documenting by HCAs on the redesign unit was also deemed a success, as, previously, HCAs did not have access to clinical documentation to review patient needs, such as diet, nor were HCAs routinely documenting information such as fluid intake and urinary output.
Some changes proved to be unattainable, however. The premise of this study was that patient outcomes would improve by redesigning the work of RNs and HCAs. In reality, no significant changes occurred, yet this was predictable, given that the redesign was not successful. Although the results were disappointing, much was learned about job redesign.
Contextual influences on the job redesign
Regrettably for staff, time spent in patient and family assessment and support decreased over time on both units for both RNs and HCAs. Staff partially attributed this finding to increased workload as a result of the introduction of overcapacity beds. Contextual factors contributed to other findings. For example, HCAs’ time spent in mobilization increased significantly on both units. This change was seen as potentially related to the organization’s implementation of a patient fall-prevention program during the study. Other findings believed to be influenced by context included: decreased time spent on activities of daily living by RNs on both units (attributed to overcapacity beds); increased time spent by RNs on both units in spatial organization (attributed to the introduction of computers on wheels); decreased time spent by HCAs on both units on cleaning and organizing (attributed to overcapacity beds); and increased time spent by RNs on the redesign unit in travel (attributed to physical relocation of unit).
It became obvious as the study progressed that influencing time spent on critical role accountabilities could not be realized simply by streamlining activities or improving team communication. Organizational literature addresses the importance of system-level structures and processes in supporting and sustaining change and quality improvement activities.36–38 Unfortunately, the redesign effort suffered from a lack of organizational alignment around the vision for collaborative nursing care, inadequate support for frontline leadership, and timing challenges.
Organizational alignment
It is clear that optimal role enactment is difficult, if not impossible, when the redesign is focused on a single unit. Alignment to a common organizational vision and the development of organization-level strategies are required to support structure (eg, new models of care delivery) and process (eg, role clarity) changes. Several authors have suggested that patient safety and quality initiatives can succeed only to the extent that organizational leaders attend to a well-designed strategic plan.39–41 Leaders need to create an organization-wide strategy that addresses investment and integration as well as accountability of human resources, information management, and technology.42,43 Also, synergistic “bottom-up” and “top-down” strategies are needed to support change.41,43 In our study, there was no clear organizational message that workforce optimization was a priority and, as general work pressures mounted, staff became frustrated with the lack of progress and support.
Dedicated structures and focused strategies are necessary to sustain change and support shared organizational learning.44,45 Implementation and sustainability of innovative patient care delivery requires the organization to pledge necessary resources.46 The vision for collaborative nursing care in the organization was only in its infancy during this study and, in fact, not all leaders were supportive of the suggested staff mix or the collaborative nursing care delivery model. Had there been organizational alignment and support, one might have expected a redeployment of LPNs to the unit in order to implement a new and more appropriate staff mix and fully test the collaborative model of care. Access to a clinical nurse educator to provide continuing education and coaching related to role accountabilities and collaborative practice would also have made the transition to the new model of care easier for staff.
Frontline leadership
A number of authors have acknowledged the role of leadership to successful care transformation.39,47,48 In particular, unit-level leadership is key to operationalize the vision and create a climate for effective implementation of innovation.49,50 Managers on the redesign unit were accountable for implementing change; however, they were not always available or able to support staff with the new ways of working. Some staff members were critical of the support provided, while others acknowledged that the managers had many demands placed on them. It was obvious that frontline leaders had insufficient experience in leading change and mentoring staff through work redesign. As well, they lacked needed support from the organization in changing ineffective structures and processes that prevented effective utilization of staff.
Timing
A number of unanticipated factors made the timing for redesign particularly poor. A new patient information system was introduced in the hospital, resulting in additional staff stress. Hospital construction created a noisy and often chaotic environment within the unit. Rapid increases in the local population contributed to increased hospital utilization, resulting in the addition of three beds (known as overcapacity beds) on the unit. In addition, frontline management changed on the unit and the unit was physically relocated within the hospital. Staff shortages plagued the unit and led to the dissolution of the change team and the discontinuation of the designated clinical leader.
Limitations
Beyond those detailed already, other limitations should be considered when interpreting the results of this study. As our analysis is based on two acute care units in a large urban tertiary treatment facility, a limited number of staff were observed; however, data from over 650 hours were collected over the study. Future work with a larger sample would facilitate examination of potential covariates in the modeling of data. While our data are subject to several biases, a rigorous process to ensure credibility of the qualitative and quantitative data was undertaken by the research team.
Conclusion
Competing priorities and lack of systemic support made it tremendously difficult for frontline managers and staff to make the changes needed to attain full enactment of the roles of nursing providers. Nonetheless, the research was successful in: 1) quantifying time spent by RNs and HCAs in activities associated with clinical role accountabilities; 2) identifying structures and processes that acted as facilitators and barriers to work redesign and informing new models of care delivery; and 3) extending existing knowledge about the nature of nursing work through discussion of key role accountabilities. The research also highlighted the need for these types of initiatives to be linked to the organization’s strategic plan and for leadership at all organizational levels to play a central role in removing barriers and acting as a catalyst for moving redesign forward. In particular, a clear organizational vision and well-articulated strategic plan related to role optimization is required.
Included within a strategic and tactical plan should be identification of appropriate resources, tools, and training materials, as well as accountability for development and implementation of each action item. Furthermore, access to necessary coaching and mentoring for staff and frontline leaders must be provided. Unfortunately, lack of awareness of the amount of organizational support needed to impact change at the unit level, limited what could be redesigned. This study also points to the importance of taking a patient population needs-based approach to guide reflection on workforce needs, such as staff mix, role clarity, provider utilization, provider continuing education, and provision of patient- and family-centered care. Consideration of patient population needs includes examining factors such as determinants of health, patient risk factors, and current patient outcomes (eg, adverse events, post-admission comorbidities). Furthermore, clear expectations and defined mechanisms (eg, bedside shift-to-shift report) are required to support patient/family engagement at the point of care. Finally, ensuring efficient and effective teams requires attention to communication mechanisms (eg, interprofessional rounds, nursing team huddles/rounds) and role clarity. Of note, the sharing of this research with other jurisdictions across Canada and key government, regulatory, and education stakeholders has catalyzed more research, implementation projects, and curriculum refinement.
Implications for health care leaders
Although we were unable to implement and evaluate a collaborative model of care that fostered optimal enactment of RN and HCA roles, study findings have informed an initiative aimed at transforming workforce models within Alberta Health Services. Ideally, all health care providers should be supported in fully enacting the roles in which they are educated and which they are legislated to perform. A clear understanding of nursing role accountabilities is required by frontline managers so that they may support, coach, and mentor their nursing staff. These frontline managers also require access to knowledge and resources related to change management and support in changing ineffective structures and processes preventing effective staff utilization. Senior leaders need to clearly articulate the vision and align strategic plans in order to minimize organizational barriers and enhance facilitators. Finally, leadership development opportunities must be provided for managers by organizations and manager efforts to improve workforce utilization need to be acknowledged by senior leaders.
Acknowledgments
We are indebted to the health care providers and managers who made the time to participate and remained committed to the study despite managing heavy workloads and dealing with substantial challenges. We truly appreciate the willingness of patients to contribute to the research with full knowledge that there would be no immediate benefit to them or their families. As well, we would like to acknowledge the contribution to this study by all members of the research team. Finally, the authors would like to acknowledge funding by Alberta Innovates – Health Solutions (the former Alberta Heritage Foundation for Medical Research). The funder had no involvement in study design; data collection, analysis, or interpretation; or report writing. We also acknowledge in-kind and cash contributions from Alberta Health Services (including the former Calgary Health Region) and the University of Calgary Faculty of Nursing. Karen Jackson is presently with Workforce Research and Evaluation, Alberta Health Services, Calgary, Alberta, Canada. Dr Jeanne Besner is presently with JFB Workforce Consulting.
Disclosure
The authors report no conflicts of interest in this work.
References
Fowler J, Hardy J, Howarth T. Trialing collaborative nursing Models of Care: the impact of change. Aust J Adv Nurs. 2006;23(4):40–46. | |
D’Amour D, Dubois CA, Déry J, et al. Measuring actual scope of nursing practice: a new tool for nurse leaders. J Nurs Adm. 2012;42(5):248–255. | |
Morrison D, Cordery J, Girardi A, Payne R. Job design, opportunities for skill utilization and intrinsic job satisfaction. European Journal of Work and Organizational Psychology. 2005;14:59–79. | |
Campbell GM, Briley T. Bundled redesign: transformational reorganization of acute care delivery. Crit Care Nurs Clin North Am. 2008;20:489–498. | |
Hyde P, McBride A, Young R, Walshe K. Role redesign: new ways of working in the NHS. Personnel Review. 2005;34(6):697–712. | |
Sibbald B, Shen J, McBride A. Changing the skill-mix of the health care workforce. J Health Serv Res Policy. 2004;9 Suppl l:28–38. | |
Joosten T, Bongers I, Janssen R. Application of lean thinking to health care: issues and observations. Int J Qual Health Care. 2009;21(5):341–347. | |
Brackett T, Comer L, Whichello R. Do lean practices lead to more time at the bedside? J Healthc Qual. 2013;35(2):7–14. | |
Ebright P. The complex work of RNs: implications for healthy work environments. Online J Issues Nurs. 2010;15(1). | |
Upenieks VV, Akhavan J, Kotlerman J. Value-added care: a paradigm shift in patient care delivery. Nurs Econ. 2008;26(5):294–300. | |
Irvine D, Sidani S, Hall LM. Finding value in nursing care: a framework for quality improvement and clinical evaluation. Nurs Econ. 1998;16(3):110–116, 131. | |
Donabedian A. The quality of care. J Am Med Assoc. 1988;260(12):1743–1748. | |
Doran D, Sidani S, Keatings M, Doidge D. An empirical test of the Nursing Role Effectiveness Model. J Adv Nurs. 2002;38(1):29–39. | |
Roberto MA, Levesque LC. The art of making change initiatives stick. MIT Sloan Manag Rev. 2005;46(4):53–60. | |
Thesen J, Kuzel AJ. Participatory inquiry. In: Crabtree BF, Miller WL, editors. Doing Qualitative Research. Thousand Oaks, CA: Sage Publications; 1999:269–290. | |
Marshall C, Rossman G. Designing Qualitative Research. Thousand Oaks, CA: Sage Publications; 1999. | |
Morse JM, Richards L. Readme First for a User’s Guide to Qualitative Methods. Thousand Oaks, CA: Sage Publications; 2002. | |
Baum F, MacDougall C, Smith D. Participatory action research. J Epidemiol Community Health. 2006;60(10):854–857. | |
Koch T, Mann S, Kralik D, van Loon AM. Reflection: look, think and act cycles in participatory action research. J Res Nurs. 2005;10(3):261–278. | |
White D, Jackson K, Besner J, et al. Enhancing Nursing Role Effectiveness Through Job Redesign: Final Report. Calgary, AB: Alberta Health Services; 2009. Available from: http://www.albertahealthservices.ca/Researchers/if-res-hswru-job-redesign-report-2009.pdf. Accessed October 8, 2013. | |
White DE, Jackson K, Besner J, Norris JM. The examination of nursing work through a role accountability framework. J Nurs Manag. Epub November 27, 2013. | |
Stevenson L, Parent K, Purkis ME. Redesigning care delivery in British Columbia. Healthc Manage Forum. 2012;25(1):16–19. | |
Crabtree BF, Miller WL, editors. Using codes and code manuals: a template organizing style of interpretation. Doing Qualitative Research. Thousand Oaks, CA: Sage Publications; 1999:163–178. | |
Improvement Leaders’ Guide to Redesigning Roles. NHS Modernisation Agency; 2004. Available from: http://web.archive.org/web/20040205224111/www.modern.nhs.uk/improvementguides/reading/redesigningroles_final.pdf. Accessed July 18, 2012. | |
Gunderson M. Rethinking Productivity From a Workplace Perspective. Ottawa, ON: Canadian Policy Research Networks; 2002. Available from: http://www.cprn.org/documents/12329_en.PDF. Accessed January 15, 2009. | |
Stebbins MW, Shani AB. Organization design and the knowledge worker. Leadership and Organization Development Journal. 1995;16:23–30. | |
Koehoorn M, Lowe GS, Rondeau KV, Schellenberg G, Wagar TH. Creating High-Quality Health Care Workplaces. Ottawa, ON: Canadian Policy Research Networks; 2002. Available from: http://www.cprn.org/documents/8984_en.PDF. Accessed January 15, 2009. | |
Carney M. The development of a model to manage change: reflection on a critical incident in a focus group setting. An innovative approach. J Nurs Manag. 2000;8:265–272. | |
Kotter JP. Leading Change. Boston, MA: Harvard Business Press; 1996. | |
Hayman B, Wilkes L, Cioffi J. Change process during redesign of a model of nursing practice in a surgical ward. J Nurs Manag. 2008;16(3):257–265. | |
Kouzes JM, Posner BZ. The Leadership Challenge. 4th ed. San Francisco, CA: Jossey-Bass; 2007. | |
Besner J, Doran D, McGillis Hall L, et al. A Systematic Approach to Maximizing Nursing Scopes of Practice. Ottawa, ON: Canadian Health Services Research Foundation; 2005. Available from: http://www.chsrf.ca/Migrated/PDF/ResearchReports/OGC/besner_e.pdf. Accessed July 18 2012. | |
Needleman J, Buerhaus PI, Stewart M, Zelevinsky K, Mattke S. Nurse staffing in hospitals: is there a business case for quality? Health Aff (Millwood). 2006;25(1):204–211. | |
Tourangeau AE, Doran DM, McGillis Hall L, et al. Impact of hospital nursing care on 30-day mortality for acute medical patients. J Adv Nurs. 2007;57(1):32–44. | |
Geary S, Cale DD, Quinn B, Winchell J. Daily rapid rounds: decreasing length of stay and improving professional practice. J Nurs Adm. 2009;39(6):293–298. | |
Odwazny R, Hasler S, Abrams R, McNutt R. Organizational and cultural changes for providing safe patient care. Qual Manag Health Care. 2005;14(3):132–143. | |
Pronovost P, Weast B, Rosenstein B, et al. Implementing and validating a comprehensive unit-based safety program. J Patient Saf. 2005;1(1):33–40. | |
Ramanujam R, Rousseau DM. The challenges are organizational not just clinical. J Organ Behav. 2006;27(7):811–827. | |
Caldwell DF, Chatman J, O’Reilly CA 3rd, Ormiston M, Lapiz M. Implementing strategic change in a health care system: the importance of leadership and change readiness. Health Care Manage Rev. 2008;33(2):124–133. | |
Kosnik LK, Espinosa JA. Microsystems in health care: Part 7. The microsystem as a platform for merging strategic planning and operations. Jt Comm J Qual Saf. 2003;29(9):452–459. | |
Ramanujam R, Keyser D, Sirio C. Making a case for organizational change in patient safety initiatives. In: Henriksen K, Battles JB, Marks ES, Lewin DI, editors. Advances in Patient Safety: From Research to Implementation. Vol 2. Rockville, MD: Agency for Healthcare Research and Quality; 2005:455–465. | |
Golden BR, Martin RL. Aligning the stars: using systems thinking to (re)design Canadian healthcare. Healthc Q. 2004;7(4):34–42. | |
Glickman SW, Baggett KA, Krubert CG, Peterson ED, Schulman KA. Promoting quality: the health-care organization from a management perspective. Int J Qual Health Care. 2007;19(6):341–348. | |
Dixon NM, Shofer M. Struggling to invent high-reliability organizations in health care settings: insights from the field. Health Serv Res. 2006;41(4 Pt 2):1618–1632. | |
Woodward S. Learning and sharing safety lessons to improve patient care. Nurs Stand. 2006;20(18):49–53. | |
Brach C, Lenfestey N, Roussel A, Ammozegar J, Sorensen A. Will it Work Here? A Decisionmaker’s Guide to Adopting Innovations. Prepared by RTI International under Contract No. 233-02-0090. Agency for Healthcare Research and Quality (AHRQ) Publication No. 08-0051. Rockville, MD: AHRQ;2008. Available from: http://www.innovations.ahrq.gov/guide/guideTOC.aspx. Accessed July 18, 2012. | |
Appelbaum SH, Berke J, Taylor J, Vazquez JA. The role of leadership during large scale organizational transitions: lessons from six empirical studies. Journal of American Academy of Business, Cambridge. 2008;13(1):16–24. | |
Massoud MR, Nielsen GA, Nolan K, Schall MW, Sevin C. A Framework for Spread: From Local Improvements to System-Wide Change. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare Improvement; 2006. Available from: www.IHI.org. Accessed July 18, 2012. | |
MacPhee M. Strategies and tools for managing change. J Nurs Adm. 2007;37(9):405–413. | |
Birken SA, Lee SY, Weiner BJ. Uncovering middle managers’ role in healthcare innovation implementation. Implement Sci. 2012; 7(1):28. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.