")
Back to Journals » Clinical Ophthalmology » Volume 13
Optimization of the Oertli CataRhex 3® phacoemulsification machine
Authors Stutz LA , Heczko JB, Bird BA, Thomson RS, Bernhisel AA , Barlow WR , Zaugg B , Olson RJ, Pettey JH
Received 4 December 2018
Accepted for publication 20 February 2019
Published 16 April 2019 Volume 2019:13 Pages 633—639
DOI https://doi.org/10.2147/OPTH.S196281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Lance A Stutz,1 Joshua B Heczko,2 Brian A Bird,3 Rhett S Thomson,2,4 Ashlie A Bernhisel,2 William R Barlow,2 Brian Zaugg,2 Randall J Olson,2 Jeff H Pettey2
1University of Texas Southwestern Medical School, University of Texas Southwestern Medical Center, Dallas, TX 75390, USA; 2Department of Ophthalmology and Visual Sciences, John A Moran Eye Center, University of Utah, Salt Lake City, UT 84132, USA; 3University of Nevada Reno, School of Medicine, Reno, NV 89557, USA; 4University of Utah, School of Medicine, Salt Lake City, UT 84132, USA
Purpose: The aim of this study was to determine optimal bottle height, vacuum, aspiration rate, and power settings of the Oertli CataRhex 3® phacoemulsification machine.
Methods: Porcine lens nuclei were hardened with formalin and cut into 2.0 mm cubes. Lens cubes were emulsified using the easyTip® 2.2 mm at 30°. Fragment removal time (efficiency) and fragment bounces off the tip (chatter) were measured. Settings tested included bottle height of 60, 80, 100 and 120 cm; aspiration rate of 40, 45, and 50 mL/min; vacuum of 400, 500, and 600 mmHg; and power of 50, 60, 70, 80, 90, and 100%.
Results: Efficiency and chatter increased in a linear fashion with increasing vacuum to 600 mmHg (P=0.017, P=0.046, respectively). The most efficient aspiration rate was 50 mL/min, although this finding lacked statistical significance (P=0.66). Increasing power increased efficiency up to 80% without increasing chatter (P=0.042, P=0.71, respectively). Compared to all other power settings, chatter was increased at 100% (P=0.014).
Conclusion: The most efficient machine settings were vacuum at 600 mmHg, aspiration rate at 50 mL/min, and power at 80%.
Keywords: cataract, blindness, underserved countries, vacuum, aspiration rate, power
Plain language summary
Blindness is a condition that affects millions of people worldwide. In countries with little or no access to eye doctors, cataracts or clouding of the natural lens within the eye is a major cause of blindness and limited vision. Some eye doctors travel to these areas to provide eye care, but it can be difficult to bring the necessary equipment to perform modern cataract surgery, also called phacoemulsification (phaco). Many eye doctors are unfamiliar with a portable machine called the Oertli CataRhex 3®, which can be used for phaco. There are several settings that can be adjusted on the machine to change its performance and limit the amount of ultrasound energy needed to break up and extract a cataract. We sought to simulate cataract surgery using pig lenses that were processed to be similar to human cataracts. We sliced these lenses into tiny cubes and ran serial sets of experiments with one cube at a time. Our goal was to determine which settings would be the fastest to chop up and remove the cubes. Only one setting was modified at a time. We identified optimal parameters for each setting, which may be helpful for eye doctors who are either unfamiliar with this machine or looking for objective evidence to guide the settings they use.
Introduction
According to meta-analyses on global blindness, cataracts are the most common cause of blindness worldwide. Recent estimates suggest that there are 36 million people who are blind and 253 million people with moderate to severe vision impairment.1,2 Among these groups, unoperated cataracts account for 35% and 25% of vision impairment, respectively.3 Although phacoemulsification (phaco) is the primary method of cataract removal in high-income countries, manual small-incision cataract surgery occupies a prominent role in ophthalmologically underserved countries.4,5 For ophthalmic surgeons travelling internationally or domestically to remote and/or underserved areas, one barrier to providing cataract surgery via phaco is the lack of portable and reliable equipment. The Oertli CataRhex 3® (Oertli) phaco machine provides an effective solution to this obstacle. Weighing as little as 11 pounds and measuring 8.7×9.5×7.2 inches, this compact machine can be attached to an IV pole and is compatible with voltages ranging from 100 to 240 V.6 In addition to its portability and suitability for the international or remote domestic setting, the Oertli provides cutting-edge technology in the form of easyPhaco® fluidics and axial ultrasound energy delivery. To our knowledge, no study to date has evaluated the performance and optimal settings for the Oertli.
In this investigation, using a porcine lens model developed in our laboratory,7 we sought to determine the optimal bottle height, vacuum, aspiration rate, and power percentage settings in order to achieve the most efficient phaco.
Methods
Porcine lens preparation
Lenses were prepared in a manner previously described.7,8 In short, whole pig eyes were purchased from Visiontech, Inc. (Sunnyvale, TX, USA), and lenses were dissected out within 48 hours of arrival at the John A Moran Eye Center, Salt Lake City, UT, USA. Immediately after dissection, the lens nuclei were placed individually in 10 mL of 10% neutral buffered formalin and incubated at room temperature for 2 hours. The lens nuclei were then rinsed three times in balanced salt solution (BSS) and allowed to equilibrate for 24 hours in BSS. Subsequently, these nuclei were cut into 2.0 mm cubes by a manual lens-cutting apparatus. Cubes were stored in BSS within a moisture chamber until studies were conducted, approximately 24 hours after cubing. The lenses prepared with this protocol are comparable to hard (3 to 4+) human cataract lenses in terms of density and behavior during phaco.8
Phaco
Phaco of lens cubes was performed with the easyTip® 2.2 mm at 30° and the Oertli phaco handpiece. Continuous power delivery of longitudinal ultrasound in the panel mode was utilized to ensure consistent delivery of ultrasonic energy. Vacuum was used in the peristaltic mode. Bottle height was measured from the level of the handpiece to the middle of the drip chamber below the saline infusion bag.
Efficiency was measured and recorded as described previously.8–10 One randomly chosen lens cube was placed inside a chamber filled with BSS. Using aspiration and vacuum alone, the pedal was depressed until the lens fragment occluded the phaco tip. The pedal was then fully depressed to initiate ultrasound. One of the authors (JH) used a handheld stopwatch to record the time from ultrasound initiation until fragment removal and paused the stopwatch if the particle bounced from the tip. When this occurred, the pedal was again depressed to vacuum until the particle once again occluded the tip, and the pedal was fully depressed and the stopwatch restarted. This allowed the chatter delay to be distinct from the total particle removal time. Efficiency was measured in terms of the amount of time in seconds that ultrasound was used to remove the lens particle. A chatter event was recorded each time the lens fragment bounced off the tip during the emulsification process.
Four sets of experiments were conducted to optimize bottle height, vacuum, aspiration rate, and power settings. For the first set, power was set at 70%, aspiration rate at 50 mL/min, and vacuum at 600 mmHg. Twenty lens cubes were tested at each of the following bottle heights: 60, 80, 100, and 120 cm. The data were analyzed as outlined subsequently. Initially, we planned to determine the most efficient bottle height; however, bottle height proved to have minimal influence on efficiency and chatter. Given that no optimal bottle height was definitively identified, 100 cm was chosen as the bottle height for subsequent experiments in accordance with the principles of chamber stability and manufacturer recommendations (easyPhaco® technology; Oertli Instrumente AG, Berneck, Switzerland).
The next data set used a phaco power of 70% and aspiration rate of 50 mL/min for each set of 20 lens cubes with vacuum levels of 400, 500, and 600 mmHg. This allowed us to determine the optimal vacuum level for these parameters. For the third data set, power was set at 70%, and the optimal vacuum level from the second set was used. Twenty lens cubes were tested at each of the following aspiration rates: 40, 45, and 50 mL/min. The final set of experiments used the previously determined optimal settings for vacuum, and aspiration rate; 20 lens cubes were tested at each power level of 50, 60, 70, 80, 90, and 100%.
Statistical analysis
Efficiency times and chatter events were averaged, and SDs were calculated. Data points that were more than two SDs from the mean were considered outliers and removed in the final analysis. This decision was based on previous work,8 which showed that some lens cubes may experience microchatter or bounce around the tip for several seconds before a proper vacuum seal is established to allow prompt emulsification. New mean values and SDs were thus recalculated to reduce noise in the data. For vacuum and power, the data sets for 400 and 500 mmHg, 50 and 60%, and 70 and 80% were also combined into groups, and new mean values and SDs were calculated. Finally, efficiency times and chatter events for each discrete variable tested were compared using one-way ANOVA. When a significant P-value was found, Student’s t-tests were performed to identify distinct relationships between the variables tested. A P-value of <0.05 was considered significant. Statistical analyses were performed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA).
Results
There was no consistent trend for increasing or decreasing efficiency with differing bottle heights of 60, 80, 100, and 120 cm (mean 2.28±1.06 seconds, 2.68±1.04 seconds, 2.32±0.75 seconds, and 2.47±0.79 seconds, respectively; P=0.65) (Figure 1). Results for chatter were similar, with mean events ranging from 0.44 to 1.05 (P=0.06) (Figure 2).
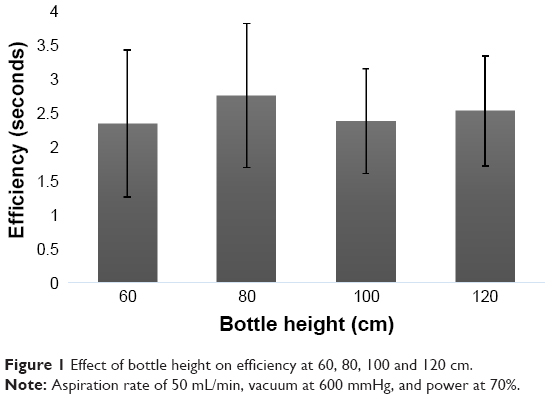 | Figure 1 Effect of bottle height on efficiency at 60, 80, 100 and 120 cm. |
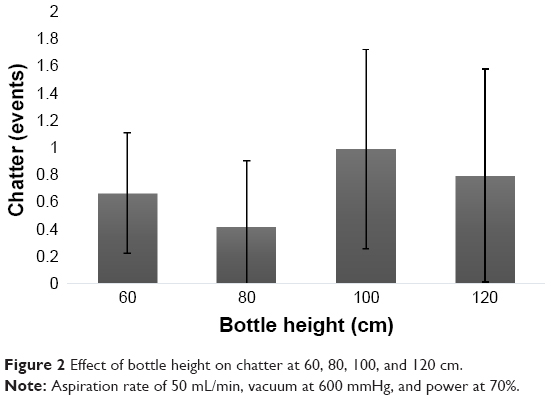 | Figure 2 Effect of bottle height on chatter at 60, 80, 100, and 120 cm. |
Efficiency increased with increasing vacuum, with significant gains when the vacuum was increased from 400 or 500 mmHg to 600 mmHg (mean 3.04±0.58 seconds, 2.82±0.75 seconds, and 2.32±1.05 seconds; P=0.023 and 0.05, respectively) (Figure 3). When the data points from 400 and 500 mmHg were combined and compared to 600 mmHg, the gain in efficiency was even stronger (P=0.017). Chatter also increased in a linear fashion with increasing vacuum (Figure 4). This finding was supported when data sets for 400 and 500 mmHg were combined and compared with 600 mmHg (mean 0.67±0.61 events, 1.05±0.61 events, respectively; P=0.046). Thus, 600 mmHg of vacuum was chosen as the optimal setting for subsequent experiments, despite increased chatter, which was still minimal at 600 mmHg.
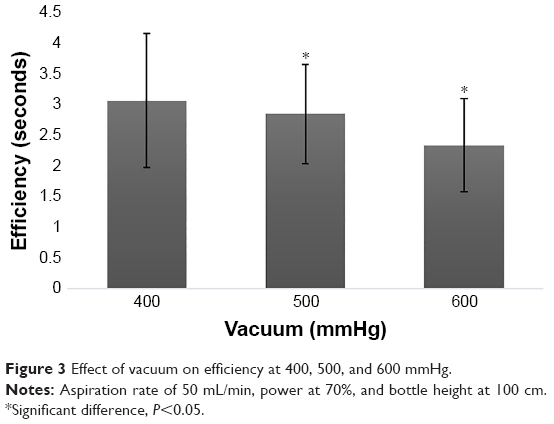 | Figure 3 Effect of vacuum on efficiency at 400, 500, and 600 mmHg. |
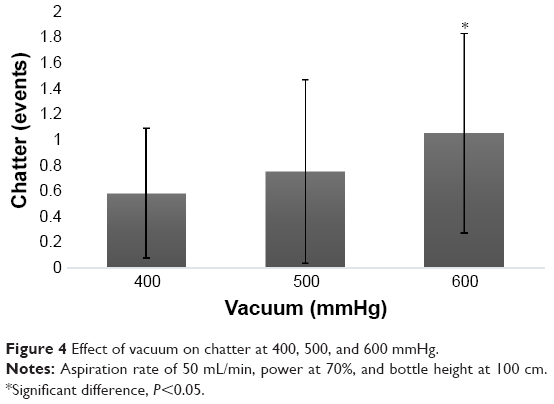 | Figure 4 Effect of vacuum on chatter at 400, 500, and 600 mmHg. |
Aspiration rate had a minimal influence on efficiency. A rate of 50 mL/min (2.32±0.75 seconds) was slightly more efficient than 40 or 45 mL/min (mean 2.51±0.94 seconds, 2.52±0.61 seconds, respectively), but this finding did not achieve statistical significance (P=0.66) (Figure 5). Chatter increased linearly from 40 to 50 mL/min (mean 0.58±0.51 events, 1.05±0.78 events, respectively) (Figure 6). However, no significant difference in chatter was found between the various aspiration rates (P=0.10). Due to the small, though not significant, gain in efficiency at 50 mL/min, this was chosen as the optimal aspiration rate.
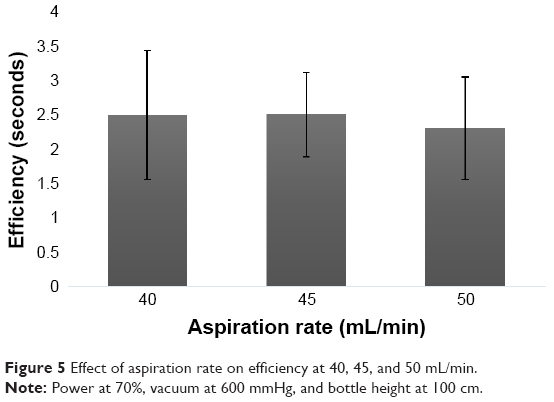 | Figure 5 Effect of aspiration rate on efficiency at 40, 45, and 50 mL/min. |
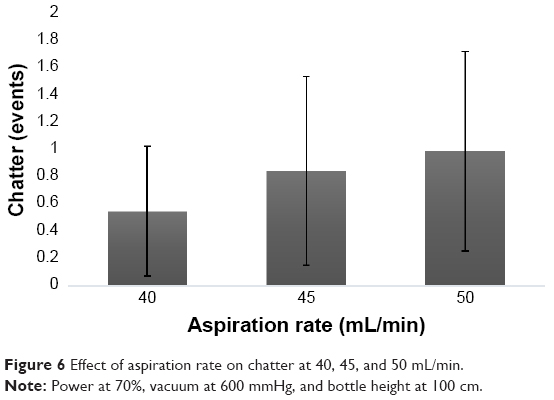 | Figure 6 Effect of aspiration rate on chatter at 40, 45, and 50 mL/min. |
Finally, increasing power led to increased efficiency, with a maximum efficiency at 80% power (mean 2.41±1.09 seconds). However, statistical significance was not achieved when directly comparing individual power settings (P=0.34) (Figure 7). When data points from 80 and 90% power were compared against combined data from 50 and 60% power, a significant difference in efficiency was found (mean 2.43±0.87 seconds, 2.89±0.96, respectively; P=0.042). There was no difference in chatter when comparing these two groups (P=0.63). Compared to all other power settings, chatter was increased at 100% (P=0.014). Chatter was lowest at 90% power (0.50±0.52 events), with a significant increase noted at 100% power (1.26±0.93 events; P=0.006) (Figure 8). There was no difference in chatter when comparing 80%–90% power (P=0.71).
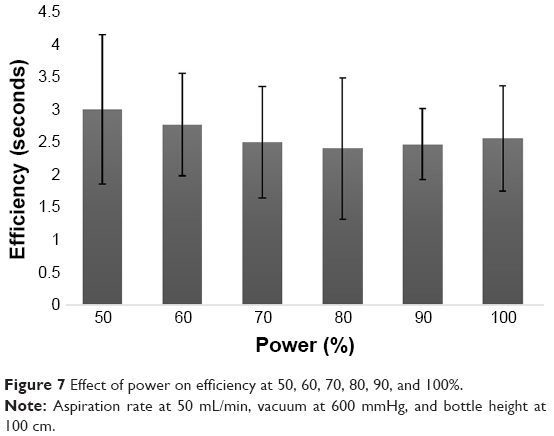 | Figure 7 Effect of power on efficiency at 50, 60, 70, 80, 90, and 100%. |
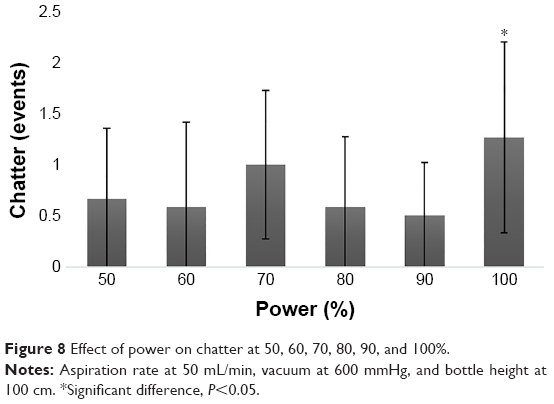 | Figure 8 Effect of power on chatter at 50, 60, 70, 80, 90, and 100%. |
Discussion
Modern phaco is a safe and efficient procedure, providing patients with excellent results. Phaco efficiency correlates with safety due to decreased exposure of ocular structures to ultrasound energy and decreased phaco times. The modern phaco system’s size and reliance on large volumes of consumables make it impractical to transport and use in outreach and/or remote settings. The Oertli provides an effective solution to this limitation because of its portability and reliability. Many surgeons traveling internationally, some of whom may not be familiar with this machine and its settings, could benefit from objective data and supporting recommendations regarding its use.
The model we used to simulate cataract phaco in this study most closely resembles the second stage of cataract removal, when individual lens pieces are emulsified. In previous work, we showed that the hardness of the prepared porcine lenses is similar to an advanced brunescent cataract graded at 3–4+, making it a suitable model for the types of cataracts a surgeon is likely to encounter in many countries in the developing world. One variable we did not assess in this study is the tip diameter. The company-supplied tip used in this study, measuring 1.15 mm, is slightly larger in diameter than those used in other optimization studies9–11 and is suitable for incisions between the sizes of 2.2–2.4 mm. In one study, Farukhi et al12 found a 0.9 mm tip to be more efficient and produce less chatter than either a 0.7 mm or a 1.1 mm tip when used on the same phaco system. However, direct comparisons from previous work are unlikely to yield relevant results, due to the introduction of several confounding variables. Future studies providing direct comparisons of the Oertli to other phaco platforms would further elucidate efficiency.
We found that infusion pressure, which varied with different bottle heights, did not show a significant difference in efficiency or chatter despite infusion pressure that affects these parameters on other phaco systems. It is possible that there could be something unique to either the design of the easyTip 2.2 mm or the machine itself which allowed for consistent performance at various bottle heights. Given that there was no difference in efficiency and chatter, it appears prudent to use the manufacturer’s recommended bottle height of 100 cm (Oertli easyPhaco®technology: Fluidics is your best friend in cataract removal. Berneck, Switzerland: Oertli Instrumente AG; 2009).
Peristaltic pump systems, such as the one used in the Oertli, create aspiration flow by compressing the outflow tubing using a series of rollers. This force draws fluid out to generate vacuum9 and has two modifiable parameters: aspiration rate and vacuum. We observed that increasing the vacuum to the maximum allowable setting of 600 mmHg significantly increased efficiency through the entire vacuum range; however, the improved efficiency at higher vacuum levels was minimal when compared to lower levels. Given the relatively small improvement in our measured parameters at high vacuum, we recommend considering lower levels of vacuum in clinical settings where aggressive vacuum settings may increase the likelihood of complications such as posterior capsule tear.
Somewhat surprisingly, increasing the aspiration rate did not statistically improve efficiency in this series. This is in contrast to our previous work9,10,13–15 and clearly is a feature of the fluidics system which is likely an inherent safety feature.16 Complications with phaco on the mature and dense lenses frequently encountered in outreach settings are common.17,18 By allowing for nearly equivalent efficiency at lower flow levels, this system likely decreases the amplitude of post-occlusion surge events and decreases the likelihood that the posterior capsule is contacted by the vibrating tip and broken. Precisely how the system achieves this is something we will explore in future testing.
Surprisingly, increasing vacuum and aspiration significantly increased the number of chatter events. These findings also contradict previous studies that used other phaco systems, where chatter consistently decreased with increasing aspiration rates and vacuum levels.9,10 Greater vacuum and flow should hold lens fragments more tightly to the phaco tip, allowing for more efficient emulsification. However, given the differences in mean chatter events were minimal, this observation is unlikely to be clinically important and probably is also related to the unique fluidics system used.
Consistent with previous studies,14,15,19 we observed an increase in efficiency with increasing power, with a maximum efficiency noted at 80% power. This finding of maximal efficiency at non-maximum power is not uncommon as chatter events increase with a resultant drop in efficiency.7 It is desirable to utilize the minimum amount of ultrasound energy needed to remove lens material, as excessive power results in increased intraoperative ultrasound delivery to the eye and potentially poorer post-operative outcomes secondary to posterior capsule rupture and/or corneal endothelial damage.20 In this study, the power range with increasing efficiency is quite broad, potentially allowing dense mature cataracts encountered in outreach settings to be removed at lower ultrasound settings.4,17,18 In regard to chatter there was variation in the number of chatter events across the levels tested, but only at 100% power was chatter consistently and significantly elevated. This finding could be expected with a phaco system that utilizes longitudinal movement alone; once stroke length reaches a certain threshold, the tip may be more likely to push the lens fragment away rather than emulsify the fragment as the tip contacts it.
Limitations of this study include the use of a single size of lens cube with a consistently high relative density when compared to cataracts common to wealthy countries. Given this particular machine’s portability and ease of use in outreach settings, assessing its performance on dense lenses is useful to inform machine settings. Another limitation is the in vitro nature of this study. However, it would not be feasible in a clinical setting to perform the number of surgeries or control for all the variables to determine the optimum settings for efficiency and chatter. Additionally, we recognize our use of some statistically non-significant values taken as optimal settings for subsequent experiment sets in this study. Increasing the sample size might decrease the SDs and illuminate other differences between the settings tested; however, additional testing is unlikely to make a substantial difference in our final results or recommendations.
Conclusion
We found that the optimal settings for the Oertli machine with easyTip 2.2 mm at 30°, with a bottle height of 100 cm, are as follows: vacuum 600 mmHg, aspiration rate 50 mL/min, and power 80%. We found that the machine is very consistent in efficiency through a wide range of aspiration and vacuum rates, which may be an important safety advantage. To our knowledge, this is the first study to determine the optimal settings for phaco using this platform. As we continue to increase our knowledge about lens removal by phaco, we will improve our ability to assess optimal settings based on machine type, lens hardness, and particle size.
Ethics approval and informed consent
Since no human subjects were involved, approval from the University of Utah Institutional Review Board was not obtained.
Abbreviations
BSS, balanced salt solution; IOL, intraocular lens; Oertli, Oertli CataRhex 3®; phaco, phacoemulsification.
Acknowledgments
Susan Schulman assisted with manuscript editing and preparation. This study was supported in part by an unrestricted grant from Research to Prevent Blindness, Inc., New York, NY, USA, to the Department of Ophthalmology and Visual Sciences, University of Utah, Salt Lake City, Utah, USA. Materials including an Oertli CataRhex 3® phaco machine, handpiece, tips, and tubing were provided by Oertli Instrumente AG (Berneck, Switzerland). The abstract of this paper was presented at the 2018 American Society of Cataract and Refractive Surgery/American Society of Ophthalmic Administrators Annual Meeting as a conference talk with interim findings. The abstract was published in the conference program for the compiled abstracts. Thomson R, Stutz LA, Heczko J, et al. Optimization of a Phacoemulsification Machine with a Direct Processor Control. Washington, DC: Conference Program, American Society of Cataract and Refractive Surgery/American Society of Ophthalmic Administrators Annual Meeting, April 13–17, 2018.
Disclosure
Dr Olson is on the scientific advisory board of EyeGate Pharmaceuticals and of Perfect Lens. The authors report no other conflicts of interest in this work.
References
Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5:e888–e897. doi:10.1016/S2214-109X(17)30293-0 | ||
World Health Organization. Eye care: the facts. Avilable from: http://www.who.int/pbd/blindness/WorldSightDay17Infographic.pdf?ua=1. 2017. Accessed April 3, 2019. | ||
Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5:e1221–e1234. doi:10.1016/S2214-109X(17)30393-5 | ||
Tabin G, Chen M, Espandar L. Cataract surgery for the developing world. Curr Opin Ophthalmol. 2008;19:55–59. doi:10.1097/ICU.0b013e3282f154bd | ||
Menapace R. Developments in modern cataract surgery – a critical overview. Ther Umsch. 2016;73:53–59. doi:10.1024/0040-5930/a000756 | ||
Oertli Instrumente AG. CataRhex 3®. Available from: https://www.oertli-instruments.com/downloads/downloads/brochures-flyer/prosp_catarhex3_2017.01_us_web.pdf. Accessed April 3, 2019. | ||
DeMill DL, Zaugg BE, Pettey JH, et al. Objective comparison of 4 nonlongitudinal ultrasound modalities regarding efficiency and chatter. J Cataract Refract Surg. 2012;38:1065–1071. doi:10.1016/j.jcrs.2011.12.040 | ||
Oakey ZB, Jensen JD, Zaugg BE, et al. Porcine lens nuclei as a model for comparison of 3 ultrasound modalities regarding efficiency and chatter. J Cataract Refract Surg. 2013;39:1248–1253. doi:10.1016/j.jcrs.2013.01.049 | ||
Cahoon JM, Gupta I, Gardiner G, et al. Comparison of venturi and peristaltic vacuum in phacoemulsification. J Cataract Refract Surg. 2015;41:428–432. doi:10.1016/j.jcrs.2014.12.043 | ||
Gupta I, Cahoon JM, Gardiner G, et al. Effect of increased vacuum and aspiration rates on phacoemulsification efficiency. J Cataract Refract Surg. 2015;41:836–841. doi:10.1016/j.jcrs.2014.09.035 | ||
Shi DS, Jensen JD, Kramer GD, et al. Comparison of vacuum and aspiration on phacoemulsification efficiency and chatter using a monitored forced infusion system. Am J Ophthalmol. 2016;169:162–167. doi:10.1016/j.ajo.2016.06.030 | ||
Farukhi AM, Stagg BC, Ronquillo C Jr, et al. Effect of phaco tip diameter on efficiency and chatter. J Cataract Refract Surg. 2014;40:811–817. doi:10.1016/j.jcrs.2013.09.021 | ||
Georgescu D, Payne M, Olson RJ. Objective measurement of postocclusion surge during phacoemulsification in human eye-bank eyes. Am J Ophthalmol. 2007;143:437–440. doi:10.1016/j.ajo.2006.11.017 | ||
Garff K, Jensen JD, Cahoon J, et al. Impact of micropulsed ultrasound power settings on the efficiency and chatter associated with lens-fragment removal. J Cataract Refract Surg. 2015;41:1264–1267. doi:10.1016/j.jcrs.2014.09.049 | ||
Wright DD, Wright AJ, Boulter TD, et al. Optimization of transversal phacoemulsification settings in peristaltic mode using a new transversal ultrasound machine. J Cataract Refract Surg. 2017;43:1202–1206. doi:10.1016/j.jcrs.2017.06.043 | ||
Schriefl SM, Stifter E, Menapace R. Impact of low versus high fluidic settings on the efficacy and safety of phacoemulsification. Acta Ophthalmol. 2014;92:e454–e457. doi:10.1111/aos.12200 | ||
Singh A, Strauss GH. High-fidelity cataract surgery simulation and third world blindness. Surg Innov. 2015;22:189–193. doi:10.1177/1553350614537120 | ||
Bourne RR, Minassian DC, Dart JK, et al. Effect of cataract surgery on the corneal endothelium: modern phacoemulsification compared with extracapsular cataract surgery. Ophthalmology. 2004;111:679–685. doi:10.1016/j.ophtha.2003.07.015 | ||
Wright A, Thomson R, Bohner A, et al. Optimization of venturi mode phacoemulsification settings of the Abbott Medical Optics WhiteStar Signature Pro in a porcine lens model. Int J Ophthalmol Clin Res. 2017;4:077. doi:10.23937/2378-346X/1410077 | ||
Payne M, Waite A, Olson RJ. Thermal inertia associated with ultrapulse technology in phacoemulsification. J Cataract Refract Surg. 2006;32:1032–1034. doi:10.1016/j.jcrs.2006.02.040 |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.