")
Back to Journals » Cancer Management and Research » Volume 14
Optimal Management of Dysphagia in Patients with Inoperable Esophageal Cancer: Current Perspectives
Authors Mohapatra S, Santharaman A, Gomez K, Pannala R, Kachaamy T
Received 12 July 2022
Accepted for publication 8 November 2022
Published 23 November 2022 Volume 2022:14 Pages 3281—3291
DOI https://doi.org/10.2147/CMAR.S362666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Seema Singh
Sonmoon Mohapatra,1 Aadhithyaraman Santharaman,2 Krista Gomez,3 Rahul Pannala,1 Toufic Kachaamy3
1Department of Gastroenterology and Hepatology, Mayo Clinic, Phoenix, AZ, 85054, USA; 2Department of Internal Medicine, Saint Peter’s University Hospital, Rutgers Robert Wood Johnson School of Medicine, New Brunswick, NJ, 08901, USA; 3Department of Gastroenterology and Hepatology, Cancer Treatment Centers of America, Phoenix, AZ, 85338, USA
Correspondence: Toufic Kachaamy, Cancer Treatment Centers of America, Phoenix, AZ, 85338, USA, Tel +1 919-451-5404, Fax +1 623-932-8633, Email [email protected]
Abstract: The majority of patients with esophageal cancer are diagnosed at an advanced, incurable stage. Palliation of symptoms, specifically dysphagia, is a crucial component to improve quality of life and optimize nutritional status. Despite multiple available treatment modalities, there is not one accepted or recommended to be the preferred treatment option. Palliative management is often decided by a multidisciplinary team considering factors including local availability, preference, patient life expectancy, and symptom severity. Systemic therapies such as chemotherapy are the most commonly used palliative modalities. Oncologists are most familiar with radiation for dysphagia palliation, especially for advanced metastatic cancer patients with good performance status. One common approach used by endoscopist is self-expandable metal stents. This is preferred for patients with short-term survival and poor functional status as it provides rapid relief of dysphagia. Cryotherapy is a relatively new endoscopic ablative modality and appears to be a promising option for dysphagia palliation, but more data is needed for wider adoption. This review summarizes the current literature on endoscopic and non-endoscopic treatment options for malignant dysphagia.
Keywords: esophageal cancer, self-expandable metal stent, cryotherapy, external beam radiation therapy
Introduction
Esophageal cancer is the seventh most frequent cancer worldwide.1 In the United States (US) in 2022, it is estimated that nearly 20000 patients will be newly diagnosed with esophageal cancer and about 16410 patients will die from it.2 Despite advances in diagnosis and treatment, the prognosis of esophageal cancer remains poor, with a dismal 5-year survival rate of <20%.3 Dysphagia is the primary presenting symptom in esophageal cancer patients. This is secondary to the cancer obstructing the esophageal lumen. On presentation, at least 50% of the patients with esophageal cancer have locally advanced disease or disease with distant metastasis making the chance of long-term remission or cure very low.4 Untreated dysphagia from esophageal cancer often worsens with time contributing to malnutrition, regurgitation, chest pain, poor performance status, and poor quality of life (QoL). The focus of care in non-curable patients with esophageal cancer is on prolonging survival, improving quality of life and minimizing the impact of dysphagia.
The optimal strategy for improving QoL and palliation of dysphagia in these patients depends on multiple factors including location, tumor stage, age, performance status, comorbidities, nutritional status, and expected patient survival. Given the lack of clear best practice guidelines, the optimal strategy is often determined by patient preference and the local multidisciplinary team expertise. Several treatment modalities are available and include systemic and local therapies. The gastroenterologist has multiple endoscopic modalities available including include laser ablation, photodynamic therapy (PDT), argon plasma coagulation (APC), self-expandable metal stents (SEMS), and, more recently, liquid nitrogen spray cryoablation. Non-endoscopic options include intraluminal brachytherapy, external beam radiation therapy (EBRT), chemotherapy, or combined modalities. Some of the risks and benefits of the available modalities are summarized in Table 1.
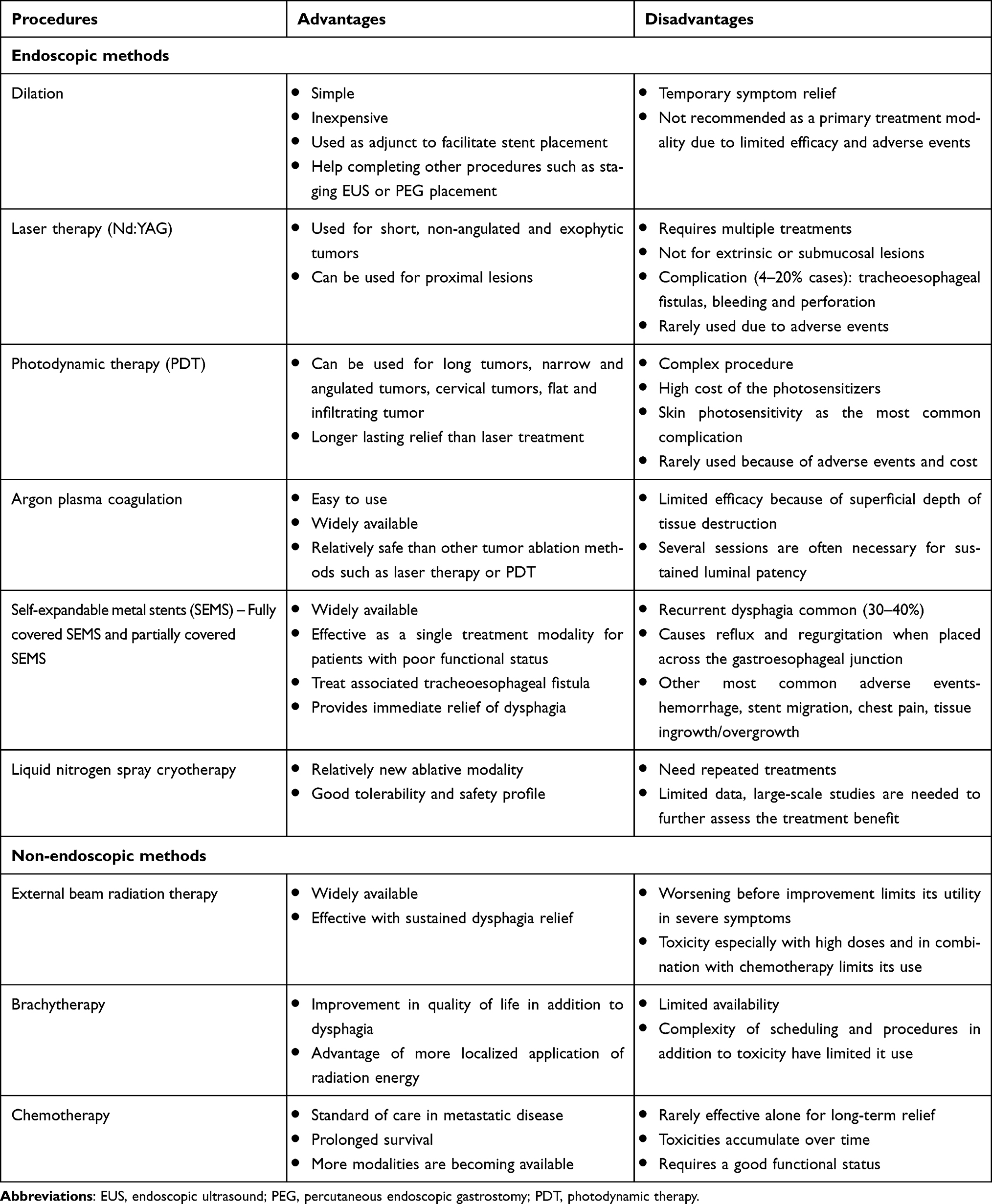 |
Table 1 Advantages and Disadvantages of Various Treatment Modalities for Palliation of Dysphagia |
Recent data and updated guidelines no longer support the use of laser, PDT, or APC as a primary modality because of their limited durability in maintaining esophageal patency for dysphagia palliation or rate of adverse events. Esophageal stenting, radiotherapy, or a combination of these therapies are the most used palliative methods in the current clinical practice. Even though a few reviews were published on this topic in the last decades, new data have emerged related to therapies and treatment approaches since their publication.5–8 In this review, we summarize the current evidence and offer an updated review and perspectives of the therapeutic options for managing dysphagia in patients with inoperable esophageal cancer.
Endoscopic Modalities of Palliation of Dysphagia
Laser Therapy
Laser ablation with neodymium–yttrium–aluminum–garnet (Nd-YAG) provides rapid improvement but only temporary relief of dysphagia if not followed by complementary therapy. Palliation with laser ablation is usually performed for treating short segment, exophytic, and discrete strictures. In addition, it can be used for treating proximal strictures in which endoscopic stenting is not possible due to tolerability or tracheal compression. Based on the results of small retrospective studies. The success rate in restoring luminal patency has been reported up to 97% with laser therapy, although multiple treatment sessions are often necessary to produce satisfactory relief of dysphagia.9–11
A small randomized control study comparing laser therapy and radiotherapy (n = 21), laser therapy followed by SEMS insertion (n = 8) or SEMS insertion alone (n = 10), showed no statistically significant difference in the mean dysphagia scores in patients with inoperable esophageal malignancy. Recurrent dysphagia was more commonly seen in the laser and radiotherapy group than in the SEMS plus laser group and the SEMS only group (43% vs 16.6% vs 5.5%, p = 0.001, respectively).12 In advanced esophageal cancer patients receiving multimodal therapy, the addition of Nd: YAG laser therapy has shown a better patient survival than those who did not receive laser therapy (30.1 months vs 16.5 months; p = 0.047).5 In a retrospective study including 227 inoperable esophageal cancer patients, laser therapy with esophageal stenting reported a significantly worse dysphagia score than laser therapy alone (p < 0.01), while the overall survival remained similar between the two groups.13
Complications such as esophageal perforation, bleeding, pneumomediastinum and tracheoesophageal fistula may occur in up to 20% of the patients which has limited its use in current clinical practice.14
Photodynamic Therapy
PDT is another ablative technique based on a photochemical reaction created by injecting a photosensitizing agent activated by a non-thermal light causing release of molecular oxygen with a direct toxic effect on malignant cells. PDT is used for exophytic or flat long lesions that might be difficult to treat with laser therapy. Additionally, PDT can be used for treatment of tumor ingrowth or overgrowth of expandable metal stents. Compared to laser therapy, PDT was more beneficial for debulking proximal, circumferential and large tumors.15 PDT has shown to produce a long-lasting relief of dysphagia but with equivalent efficacy and patient survival when compared to the laser therapy.16,17 Conflicting data exist on the benefit of PDT combined with chemotherapy or chemoradiation therapy for non-operable EC patients.18,19 Severe complications are more frequent in patients treated with PDT, including skin photosensitivity, perforation, stricture formation in nearly 4–34% of the patients.4 The high cost and adverse events rate resulted in PDT being uncommonly used in the present practice.4
Argon Plasma Coagulation
APC is a type of ablative endoscopic therapy that uses electrically conductive argon gas (“plasma”) to cause tissue coagulation and destruction. The thermally induced tissue necrosis caused by APC is often superficial to a depth of 1–2 mm, limiting its efficacy in the palliation of obstructing cancer.20–22 A 30–50% higher effectiveness with no increased risk of adverse events was reported using high-frequency APC.23 Minor complications such as bleeding, pain, or asymptomatic gas accumulation in the intestinal wall can be observed in up to 13% of the patients.4 Major complications such as perforation, abdominal abscess, mediastinitis, or fistula formation may occur but rare.4,23 Similar to other ablative methods, the results of APC are generally not durable, requiring multiple additional treatment sessions, limiting its use in clinical practice. A combination of APC with other palliative treatment modalities has demonstrated a sustained restoration of luminal patency compared to APC alone in a few studies.24,25
Cryoablation
Liquid nitrogen spray cryotherapy is a relatively new ablative modality that has successfully been used to palliate dysphagia in patients with inoperable esophageal cancers. Spray cryotherapy uses liquid nitrogen at –196° to effectively freeze and destroy esophageal tumors by inducing tumor necrosis and apoptosis in addition to possible immunologic mechanisms. Cryoablation is shown to have an excellent tolerability and safety profile.26–28 In a multicenter retrospective study (n=49), endoscopic liquid nitrogen spray cryotherapy showed a significant improvement in dysphagia score from 2.4 pre cryotherapy to 1.7 post cryotherapy (P<0.001) when used to palliate dysphagia in patients with inoperable EC.27 Adverse events were noted in 6.7% (8/120) patients, majority of which were considered minor including chest pain, intraprocedural bradycardia and post procedural stricture. Perforation was noted in one patient which was associated with dilation before cryotherapy.27 More recent studies published to date only in abstract form found cryotherapy to be associated with an improvement in dysphagia, quality of life and social functioning without reflux symptoms which is an advantage over stenting.29,30
Esophageal Stenting
Self-expanding metal stents are commonly used for palliation of malignant dysphagia to restore the luminal patency and help support oral intake in these patients. Over the past 25 years, SEMS has evolved considerably and has undergone numerous modifications. Multiple varieties of SEMS are commercially available at present. They differ in-stent material, design, covering, luminal diameter, radial force, degree of shortening after deployment, and anti-migration features. Partially covered SEMS (PCSEMS) and fully covered SEMS (FCSEMS) are the most commonly used esophageal stents in the current clinical practice. There are no data comparing different stent designs showing the clinical superiority of one stent over the other. Therefore, selecting a specific SEMS is often based on the availability or endoscopist’s preference and experience.
SEMS are favored for inoperable patients with expected short-term survival, limited functional status and those intolerant to chemoradiation. SEMS have been shown in many RCT to have better outcomes than PDT, laser and surgery.31 Therefore, the European and American gastrointestinal endoscopy societies recommend FCSEMS or PCSEMS for palliation of malignant dysphagia over laser therapy, photodynamic therapy, esophageal bypass, and expandable plastic stent.32–34 Newly designed irradiation stents, combining the advantages of SEMS and radiation therapy, are currently being studied. The stent is impregnated with iodine 125 (125I) beads for intraluminal brachytherapy which provides an immediate and more durable effect on dysphagia compared to the conventional SEMS.35 However, this technique is not widely available, and an accurate radiation dosimetry with such stent is difficult to precisely measure and plan.
SEMS-related adverse events can be seen in up to 40–50% of the patients with severe adverse event rate up to 20%.36 The most common early adverse events noted are stent migration, chest pain, bleeding, perforation, reflux, and globus sensation. The rate of adverse events after SEMS placement increases over time.37,38 The reported late adverse events are tissue overgrowth/ingrowth, reflux, perforation, tracheoesophageal fistula (higher for mid-esophageal stents), stent migration, aortoesophageal fistula, and paraspinal abscess formation. Recurrent dysphagia was frequently encountered in about one-third of patients after a median of 56 days (range 1–779) of SEMS placement.36 No statistical difference has been noted regarding the rate of stent migration and stent obstruction with FCSEMS or PCSEMS in palliative treatment of malignant esophageal strictures.39,40 The result of a recent meta-analysis including eight randomized controlled trials (RCTs) showed similar outcomes and rate of complications with traditional SEMS when compared to anti-reflux stent with valve.41 One study has demonstrated increased stent-related complications in patients with prior chemoradiation, although this finding needs further validation.36
A tracheoesophageal fistula may develop as a result of tumor penetration or complication of radiation therapy in about 5% to 15% of EC patients.42 Insertion of a SEMS frequently provides complete esophageal sealing in EC with an established airway fistula. However, caution should be taken while placing a SEMS through a large bulky retro bronchial tumor, as acute airway obstruction can occur because of the compression of the tracheal wall from SEMS expansion.32 A multidisciplinary case discussion and concomitant airway management should be considered before performing such procedure. Placement of a tracheal or bronchial stent in conjunction with an esophageal stent (double stenting) has also been described for palliation of the tracheoesophageal fistula.43 However, an increase in the original fistula size due to compression of tracheal and esophageal walls between the two stents is a concern.42 Insertion of one stent is preferable in these situations.
Non-Endoscopic Modalities for Palliation of Dysphagia
Radiation Therapy
Radiation therapy is a commonly used modality for dysphagia palliation that uses ionizing radiation causing DNA damage and cell death resulting in tumor debulking. Radiation therapy can be provided either intraluminal as brachytherapy using a endoluminal applicator or externally through EBRT and typically results in a durable relief of dysphagia. A few limitations experienced include initial worsening of dysphagia and delayed onset of symptom relief.
Brachytherapy
Brachytherapy allows delivery of high doses of radiation directly to the luminal tumor with minimal exposure to the adjacent organs. It requires an endoscopic procedure along with coordination with radiation oncology. Due to risk of fistula formation, it is contraindicated in patients with tracheal or bronchial involvement. A meta-analysis of six prospective studies showed that brachytherapy is very effective in treating dysphagia with complete resolution of symptoms in 87% of the cases after 1 month, 66% of the patients in 3 months, and 50% of the cases after 6 months.44 Guidelines from European Society of Gastrointestinal Endoscopy strongly recommend brachytherapy for patients with longer life expectancy as they may have a survival advantage and possible a better QoL compared to SEMS alone.33
Brachytherapy can be given via single or multiple fractions. A median dysphagia-free survival of 10 months and median overall survival of 7 months has been reported in patients given 2 fractions of 6 Gy each.45 Better results were associated with two fractions, while the addition of a third did not improve outcomes.46 Surveys show that brachytherapy continues to be underutilized due to treatment complexity, unavailability, lack of awareness, experience, and local expertise.47,48 Complications of brachytherapy include fistula formation (8–34%), strictures (11–42%) and esophagitis or ulceration (10–12.5%).49 The relatively high adverse event rate and the need for coordinating an endoscopy with radiation have limited the use of brachytherapy.
External Beam Radiation Therapy
EBRT causes delivery of ionizing radiation externally in a non-invasive manner. EBRT has been shown to provide long-term dysphagia palliation; however, compared to brachytherapy, it is less selective not only causing damage to the tumor but also surrounding tissue. Due to cumulative exposure of normal tissue, total dose is often limited. The higher the doses, the higher the risk of adverse events.50 The onset of relief is delayed for weeks compared to the immediate relief seen with stenting.51 There can be initial worsening before improvement due to the acute inflammatory response seen from radiation. A retrospective review concluded a short course with lower doses of 20 Gy in 5 fractions, without chemotherapy lead to improvement in dysphagia in 75% of the patients.49 Higher doses such as 50 Gy showed a similar overall improvement in dysphagia score in patients receiving EBRT but with a significantly higher risk of adverse events including up to 40% of stricture formation.52
EBRT has been compared to brachytherapy and is also used in combination. In a study that compared EBRT of 20 Gy in five fractions of 4 Gy versus single dose of 12Gy of brachytherapy showed improvement of dysphagia in 83% of the patients after EBRT vs 64% after brachytherapy (p=0.04).53 Conflicting outcomes have been reported on the effect of combination of EBRT and brachytherapy for palliation of dysphagia.54–57 The result of a retrospective study has shown that EBRT + brachytherapy is superior to brachytherapy alone. The 6-months dysphagia-free survival was 90 ± 4% after EBRT, 92 ± 5% after EBRT + brachytherapy and 37 ± 7% after brachytherapy alone (p<0.001).56 But as noted, dysphagia-free survival scores of patients treated with EBRT alone were no different than the combination therapy, suggestive that adding brachytherapy to EBRT did not affect the study outcome.56 In contrast, Rosenblatt et al conducted a RCT that demonstrated that the addition of EBRT to brachytherapy led to a significantly improved dysphagia-relief experience with an absolute benefit of +18% at 200 days from randomization (p = 0.019).55 There was no statistical difference in overall survival and adverse events between the two study arms in that study.
Adverse effects of radiation include acute toxicity such as worsening dysphagia, odynophagia, nausea, vomiting, bleeding and cytopenia. The side effects are more frequent at higher doses. Worsening of dysphagia from radiotherapy-induced edema and radiation esophagitis has been reported in 22–28% of the patients.49,58 Another major adverse event noted is stricture formation, which can occur in 30–44% after radiotherapy especially with high doses.59 These adverse events, combined with the delay in onset of relief has limited its use in stage 4 esophageal cancer patients. Doses that seem to be well tolerated are 20Gr over 2 weeks, especially in patients who have been stabilized on systemic therapy and have a good functional status.
Systemic Therapy
Systemic chemotherapy is recommended for palliation in patients with locally advanced or metastatic disease by the National Comprehensive Cancer Network (NCCN) clinical practice guideline.60 The data on systemic therapy and dysphagia improvement are mostly from old studies. Systemic therapy results in dysphagia improvement in 72–90% of the patients 2–6 weeks after initiation of therapy. The duration of relief tends to correlate with the extent of relief and can last from a few weeks to a few months or longer if the patient continues to respond to therapy.61,62 Cwikiel et al retrospectively compared the improvement of dysphagia in patients receiving radiotherapy, chemotherapy, and stent. They showed that up to 50% of the patients still experienced some degree of dysphagia after three courses of 5-fluorouracil (5-FU) plus cisplatin (9 weeks after the start of treatment).63 Palliative chemoradiotherapy is especially important for patients with cervical esophageal tumors, as stenting in this area can be problematic due to pain and discomfort when close to the cricopharyngeus. Other endoscopic options such as cryotherapy and PDT can also be used in the upper esophagus. A more recent RCT comparing palliative chemoradiation therapy with radiotherapy alone showed only a modest increase in dysphagia relief (not statistically significant) in the chemoradiotherapy group with an increased risk of toxicity.64 In addition to affecting the QoL, toxic side effects of the combined therapy are severe in 44% and life-threatening in 20% of the patients, compared to 25% and 3%, respectively, of those treated with radiation alone.65
A Cochrane review on systemic for esophageal cancer concluded that systemic therapy improves dysphagia; however, the impact on quality of life is less clear mostly due to poor quality of data. They recommended against using chemotherapy alone for dysphagia palliation in esophageal cancer due to the high incidence of recurrent symptoms.31 However, systemic therapy is evolving rapidly with addition of targeted agents and immunotherapy, and it is expected that the treatment outcomes for dysphagia palliation will greatly improve in the future with the newer agents.66,67
Esophageal Stent in Comparison or Combination with Other Therapies
A combination of therapies or different therapies sequentially are utilized specifically in patients with longer than average survival. Two RCTs have compared the outcomes of stent insertion and intraluminal brachytherapy as palliative treatment of dysphagia.68,69 When compared to stent group, brachytherapy was shown to provide a longer duration of dysphagia relief (115 days vs 82 days, P=0.015) with fewer rate of adverse events (21% vs 33%, P<0.05).68 This observation was thought to be because of a higher rate of dysphagia recurrence in the stent group caused by stent migration, tissue ingrowth or overgrowth, or food bolus obstruction. Compared to the stent group, QoL scores favored the brachytherapy group with overall the rate of adverse events being high in both groups.68 Another RCT demonstrated similar results in long-term relief of dysphagia and showed that the health-related QoL was more stable in the brachytherapy group than with SEMS.69 There was no survival difference noted between the stent and brachytherapy groups.68,69 Cost-effective analysis comparing SEMS and single-dose brachytherapy has been performed and showed higher initial costs in the stent group compared to brachytherapy. However, the total medical costs were similar (stent11195euro vs brachytherapy10078euro, P>0.20).70
Combining single-dose brachytherapy and SEMS has been explored in a small RCT comparing a combination of SEMS and brachytherapy (n=21) vs brachytherapy alone (n=20) showed significant improvement in dysphagia scores in the combined group after 3 weeks of treatment (71% vs 39%, P<0.05). However, this difference gradually decreased in 7 weeks following the treatment. No difference was noted regarding severe adverse events or survival between the groups.50 Further studies on this topic have not been published since then.
There are a few studies that have compared SEMS versus SEMS with EBRT.58,71–74 Of those, one study had randomized patients between SEMS group (n=37) and SEMS followed by EBRT (n=42).58 The result of this study showed a more sustained relief of dysphagia in the EBRT after SEMS group (7 vs 3 months, p = 0.002).58 A survival benefit has been noted in the combined therapy versus stenting alone.58,71,72 However, despite the prolonged relief of dysphagia and improvement of overall survival in the SEMS+EBRT group, it has been shown that the combined approach has higher rates of adverse events such as formation or worsening of esophageal fistulas and massive gastrointestinal bleeding.75
A prospective comparative study on chemotherapy (5-FU and cisplatin) vs SEMS showed that chemotherapy alone is effective in relieving dysphagia in 67% of the patients after 4 weeks and precludes the use of a stent in about half of the patients.76 However, results from other studies are conflicting. They do not support chemotherapy alone as a sole modality for palliation of dysphagia in patients with locally advanced and incurable or metastatic esophageal cancer.31
The data on whether stent placement in patients with prior chemotherapy and/or radiation therapy is associated with a high risk of adverse events are controversial. While several studies have reported an increased risk of serious adverse events in patients with prior chemotherapy ± radiation therapy, other studies have shown a similar risk of adverse events in these patients. Major complications such as pneumonia and fistula formation can occur in up to 50% of the patients.77
Cryotherapy has been used safely and effectively in patients receiving systemic therapy. The data on it is still evolving. Safety and tolerability are advantages of cryotherapy and further high-quality data are needed for wider adoption.
Current Perspectives and Recommendations
Esophageal cancer continues to be a disease diagnosed at late stages and is associated with significant morbidity and high mortality. Palliative treatment is often the focus either because of the advanced incurable stage or the poor surgical candidacy of patients with multiple comorbidities and/or significant malnutrition. The ideal palliative approach will focus on dysphagia palliation and improve quality of life and nutritional status.
- Dilation, laser therapy, and photodynamic therapy have fallen out of favor due to limited efficacy for dilation, adverse events for laser therapy, and both cost and adverse events for PDT.
- SEMS insertion is the most common endoscopic treatment for dysphagia palliation. SEMS is preferable for patients with a short life expectancy because of the immediate symptom relief. They are associated with significant reflux symptoms with mixed results on quality of life. The risk of adverse events increases over time, including the rate of stent migration or tissue overgrowth requiring further interventions.
- Liquid nitrogen spray cryoablation therapy is a promising treatment option for dysphagia palliation and seems to have a low rate of adverse events. Data on cryoablation are relatively new, with some recent data available only in an abstract form showing improvement in quality of life without reflux symptoms. Cryotherapy seems to be safe and effective in combination with systemic therapy. More data is needed before its wide adoption.
- Esophageal brachytherapy (if available) or EBRT can be considered for patients with a longer life expectancy and mild-to-moderate symptoms. The time to onset of symptom relief and adverse events limit their uses, especially in patients with stage 4 disease.
- Chemotherapy is standard of care and recommended for most patients with a good functional status because of the increased survival. Chemotherapy improves dysphagia with onset within a few weeks; however, most patients will need another form of palliation.
- Chemoradiotherapy is the standard of care for patients with stage 3 disease because of the potential for complete clinical response in some patients. Its use for pure palliative purposes, especially in patients with stage 4 disease, is associated with significant morbidity and occasionally mortality.
Esophageal cancer is a complex disease requiring multidisciplinary care. The best palliative approach is often determined by a multidisciplinary team depending on the local expertise, patient preferences, life expectancy, patient comorbidities, the extent of the disease, and anticipated acute and late toxicities. Multiple modalities are often used in the same patient in sequence or combinations. In addition, systemic therapy is rapidly evolving and has significantly changed since the above-referenced studies’ publications make their applicability to current practice somewhat limited. As more effective systemic treatment becomes increasingly available, the authors believe that reliance on other forms of palliative treatment will become less needed and likely limited to modalities with a favorable adverse event rate to complement and augment the effect of systemic therapy.
Abbreviations
QoL, Quality of life; SEMS, Self-expandable metal stent; PCSEMS, Partially covered self-expandable metal stent; FCSEMS, Fully covered self-expandable metal stent; EBRT, External beam radiation therapy; PDT, Photodynamic therapy; RCTs, Randomized controlled trial; HDRILBT, High-dose-rate intraluminal brachytherapy.
Funding
There is no funding to report.
Disclosure
Toufic Kachaamy: Consultant for Medtronic, Steris, Pentax, Microtech. Receives educational support from Boston Scientific and Cook. Rahul Pannala: Research funding from ERBE, USA, consulting fees from HCL technologies, personal fees from Bluestar Genomics and Nestle Health Sciences, and grants from Fractyl Labs. All other authors have no financial disclosures.
References
1. Thrift AP. Global burden and epidemiology of Barrett oesophagus and oesophageal cancer. Nat Rev Gastroenterol Hepatol. 2021;18(6):432–443. doi:10.1038/s41575-021-00419-3
2. Howlade N, NooneAM, Krapcho M et al. SEER Cancer Statistics Review, 1975-2016, National Cancer Institute. Bethesda, MD. Available from: https://seer.cancer.gov/csr/1975_2016/.
3. Kauppila JH, Mattsson F, Brusselaers N, Lagergren J. Prognosis of oesophageal adenocarcinoma and squamous cell carcinoma following surgery and no surgery in a nationwide Swedish cohort study. BMJ Open. 2018;8(5):e021495. doi:10.1136/bmjopen-2018-021495
4. Allum WH, Blazeby JM, Griffin SM, Cunningham D, Jankowski JA, Wong R; Association of Upper Gastrointestinal Surgeons of Great, t. B. S. o. G. Ireland and O. The British Association of Surgical. Guidelines for the management of oesophageal and gastric cancer. Gut. 2011;60(11):1449–1472. doi:10.1136/gut.2010.228254
5. Alexander P, Mayoral W, Reilly HF, Wadleigh R, Trachiotis G, Lipman TO. Endoscopic Nd: YAG laser with aggressive multimodality therapy for locally advanced esophageal cancer. Gastrointest Endosc. 2002;55(6):674–679. doi:10.1067/mge.2002.123270
6. Javle M, Ailawadhi S, Yang GY, Nwogu CE, Schiff MD, Nava HR. Palliation of malignant dysphagia in esophageal cancer: a literature-based review. J Support Oncol. 2006;4(8):365–373, 379.
7. Rabenstein T. Palliative endoscopic therapy of esophageal cancer. Viszeralmedizin. 2015;31(5):354–359. doi:10.1159/000441175
8. Levy A, Wagner AD, Chargari C, et al. Palliation of dysphagia in metastatic oesogastric cancers: an international multidisciplinary position. Eur J Cancer. 2020;135:103–112. doi:10.1016/j.ejca.2020.04.032
9. Mellow MH, Pinkas H. Endoscopic laser therapy for malignancies affecting the esophagus and gastroesophageal junction. Analysis of technical and functional efficacy. Arch Intern Med. 1985;145(8):1443–1446.
10. Rutgeerts P, Vantrappen G, Broeckaert L, et al. Palliative Nd: YAG laser therapy for cancer of the esophagus and gastroesophageal junction: impact on the quality of remaining life. Gastrointest Endosc. 1988;34(2):87–90. doi:10.1016/s0016-5107(88)71269-9
11. Mason RC, Bright N, McColl I. Palliation of malignant dysphagia with laser therapy: predictability of results. Br J Surg. 1991;78(11):1346–1347. doi:10.1002/bjs.1800781125
12. Konigsrainer A, Riedmann B, De Vries A, et al. Expandable metal stents versus laser combined with radiotherapy for palliation of unresectable esophageal cancer: a prospective randomized trial. Hepatogastroenterology. 2000;47(33):724–727.
13. Pozza A, Erroi FR, Scarpa M, Polese L, Rampazzo L, Norberto L. Palliative therapy for esophageal cancer: laser therapy alone is associated with a better functional outcome. Updates Surg. 2015;67(1):61–67. doi:10.1007/s13304-015-0277-4
14. Gevers AM, Macken E, Hiele M, Rutgeerts P. A comparison of laser therapy, plastic stents, and expandable metal stents for palliation of malignant dysphagia in patients without a fistula. Gastrointest Endosc. 1998;48(4):383–388. doi:10.1016/s0016-5107(98)70007-0
15. Marcon NE. Photodynamic therapy and cancer of the esophagus. Semin Oncol. 1994;21(6 Suppl 15):20–23.
16. Heier SK, Rothman KA, Heier LM, Rosenthal WS. Photodynamic therapy for obstructing esophageal cancer: light dosimetry and randomized comparison with Nd: yAGlaser therapy. Gastroenterology. 1995;109(1):63–72. doi:10.1016/0016-5085(95)90269-4
17. Lightdale CJ, Heier SK, Marcon NE, et al. Photodynamic therapy with porfimer sodium versus thermal ablation therapy with Nd: YAGlaser for palliation of esophageal cancer: a multicenter randomized trial. Gastrointest Endosc. 1995;42(6):507–512. doi:10.1016/s0016-5107(95)70002-1
18. Lecleire S, Di Fiore F, Antonietti M, et al. Nonoperable patients with superficial esophageal cancer treated by photodynamic therapy after chemoradiotherapy have more severe complications than patients treated in primary intent. Am J Gastroenterol. 2008;103(9):2215–2219. doi:10.1111/j.1572-0241.2008.02042.x
19. Li LB, Xie JM, Zhang XN, et al. Retrospective study of photodynamic therapy vs photodynamic therapy combined with chemotherapy and chemotherapy alone on advanced esophageal cancer. Photodiagnosis Photodyn Ther. 2010;7(3):139–143. doi:10.1016/j.pdpdt.2010.06.002
20. Wahab PJ, Mulder CJ, den Hartog G, Thies JE. Argon plasma coagulation in flexible gastrointestinal endoscopy: pilot experiences. Endoscopy. 1997;29(3):176–181. doi:10.1055/s-2007-1004159
21. Heindorff H, Wojdemann M, Bisgaard T, Svendsen LB. Endoscopic palliation of inoperable cancer of the oesophagus or cardia by argon electrocoagulation. Scand J Gastroenterol. 1998;33(1):21–23. doi:10.1080/00365529850166158
22. Akhtar K, Byrne JP, Bancewicz J, Attwood SE. Argon beam plasma coagulation in the management of cancers of the esophagus and stomach. Surg Endosc. 2000;14(12):1127–1130. doi:10.1007/s004640000266
23. Eickhoff A, Jakobs R, Schilling D, et al. Prospective nonrandomized comparison of two modes of argon beamer (APC) tumor desobstruction: effectiveness of the new pulsed APC versus forced APC. Endoscopy. 2007;39(7):637–642. doi:10.1055/s-2007-966571
24. Rupinski M, Zagorowicz E, Regula J, et al. Randomized comparison of three palliative regimens including brachytherapy, photodynamic therapy, and APC in patients with malignant dysphagia (CONSORT 1a) (Revised II). Am J Gastroenterol. 2011;106(9):1612–1620. doi:10.1038/ajg.2011.178
25. Kofoed SC, Lundsgaard M, Ellemann AC, Svendsen LB. Low morbidity after palliation of obstructing gastro-oesophageal adenocarcinoma to restore swallowing function. Dan Med J. 2012;59(6):A4434.
26. Greenwald BD, Dumot JA, Abrams JA, et al. Endoscopic spray cryotherapy for esophageal cancer: safety and efficacy. Gastrointest Endosc. 2010;71(4):686–693. doi:10.1016/j.gie.2010.01.042
27. Kachaamy T, Prakash R, Kundranda M, et al. Liquid nitrogen spray cryotherapy for dysphagia palliation in patients with inoperable esophageal cancer. Gastrointest Endosc. 2018;88(3):447–455. doi:10.1016/j.gie.2018.04.2362
28. Shah T, Kushnir V, Mutha P, et al. Neoadjuvant cryotherapy improves dysphagia and may impact remission rates in advanced esophageal cancer. Endosc Int Open. 2019;7(11):E1522–E1527. doi:10.1055/a-0957-2798
29. Swathi Eluri VK, Sharma NR, Gordon SR, et al. Palliative endoscopic spray cryotherapy to prevent worsening of dysphagia and improve quality of life in esophageal cancer [Abstract].
30. Kachammy T, Shaw SN, Mohapatra S, et al. Cryotherapy is safe and effective without causing reflux symptoms in esophageal cancer patients receiving systemic therapy; intensive therapy showed greater benefit: a prospective multicenter study [Abstract].
31. Dai Y, Li C, Xie Y, et al. Interventions for dysphagia in oesophageal cancer. Cochrane Database Syst Rev. 2014;(10):CD005048. doi:10.1002/14651858.CD005048.pub4
32. Evans JA, Early DS, Chandraskhara V, et al.; Committee, A. S. o. P. American Society for Gastrointestinal. The role of endoscopy in the assessment and treatment of esophageal cancer. Gastrointest Endosc. 2013;77(3):328–334. doi:10.1016/j.gie.2012.10.001
33. Spaander MC, Baron TH, Siersema PD, et al. Esophageal stenting for benign and malignant disease: European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline. Endoscopy. 2016;48(10):939–948. doi:10.1055/s-0042-114210
34. Spaander MCW, van der Bogt RD, Baron TH, et al. Esophageal stenting for benign and malignant disease: European Society of Gastrointestinal Endoscopy (ESGE) guideline - update 2021. Endoscopy. 2021;53(7):751–762. doi:10.1055/a-1475-0063
35. Guo JH, Teng GJ, Zhu GY, et al. Self-expandable esophageal stent loaded with 125I seeds: initial experience in patients with advanced esophageal cancer. Radiology. 2008;247(2):574–581. doi:10.1148/radiol.2472070999
36. Reijm AN, Didden P, Schelling SJC, Siersema PD, Bruno MJ, Spaander MCW. Self-expandable metal stent placement for malignant esophageal strictures - changes in clinical outcomes over time. Endoscopy. 2019;51(1):18–29. doi:10.1055/a-0644-2495
37. Wang MQ, Sze DY, Wang ZP, Wang ZQ, Gao YA, Dake MD. Delayed complications after esophageal stent placement for treatment of malignant esophageal obstructions and esophagorespiratory fistulas. J Vasc Interv Radiol. 2001;12(4):465–474. doi:10.1016/s1051-0443(07)61886-7
38. Homann N, Noftz MR, Klingenberg-Noftz RD, Ludwig D. Delayed complications after placement of self-expanding stents in malignant esophageal obstruction: treatment strategies and survival rate. Dig Dis Sci. 2008;53(2):334–340. doi:10.1007/s10620-007-9862-9
39. Persson J, Smedh U, Johnsson A, et al. Fully covered stents are similar to semi-covered stents with regard to migration in palliative treatment of malignant strictures of the esophagus and gastric cardia: results of a randomized controlled trial. Surg Endosc. 2017;31(10):4025–4033. doi:10.1007/s00464-017-5441-0
40. Wang C, Wei H, Li Y. Comparison of fully-covered vs partially covered self-expanding metallic stents for palliative treatment of inoperable esophageal malignancy: a systematic review and meta-analysis. BMC Cancer. 2020;20(1):73. doi:10.1186/s12885-020-6564-6
41. Pandit S, Samant H, Morris J, Alexander SJ. Efficacy and safety of standard and anti-reflux self-expanding metal stent: a systematic review and meta-analysis of randomized controlled trials. World J Gastrointest Endosc. 2019;11(4):271–280. doi:10.4253/wjge.v11.i4.271
42. Shamji FM, Inculet R. Management of malignant tracheoesophageal fistula. Thorac Surg Clin. 2018;28(3):393–402. doi:10.1016/j.thorsurg.2018.04.007
43. Nomori H, Horio H, Imazu Y, Suemasu K. Double stenting for esophageal and tracheobronchial stenoses. Ann Thorac Surg. 2000;70(6):1803–1807. doi:10.1016/s0003-4975(00)02042-7
44. Fuccio L, Mandolesi D, Farioli A, et al. Brachytherapy for the palliation of dysphagia owing to esophageal cancer: a systematic review and meta-analysis of prospective studies. Radiother Oncol. 2017;122(3):332–339. doi:10.1016/j.radonc.2016.12.034
45. Sharma V, Mahantshetty U, Dinshaw KA, Deshpande R, Sharma S. Palliation of advanced/recurrent esophageal carcinoma with high-dose-rate brachytherapy. Int J Radiat Oncol Biol Phys. 2002;52(2):310–315. doi:10.1016/s0360-3016(01)01822-3
46. Sur RK, Levin CV, Donde B, Sharma V, Miszczyk L, Nag S. Prospective randomized trial of HDR brachytherapy as a sole modality in palliation of advanced esophageal carcinoma--an International Atomic Energy Agency study. Int J Radiat Oncol Biol Phys. 2002;53(1):127–133. doi:10.1016/s0360-3016(02)02702-5
47. Suntharalingam M, Moughan J, Coia LR, et al.; Patterns of Care. The national practice for patients receiving radiation therapy for carcinoma of the esophagus: results of the 1996–1999 Patterns of Care Study. Int J Radiat Oncol Biol Phys. 2003;56(4):981–987. doi:10.1016/s0360-3016(03)00256-6
48. Fuccio L, Guido A, Hassan C, et al. Underuse of brachytherapy for the treatment of dysphagia owing to esophageal cancer. An Italian survey. Dig Liver Dis. 2016;48(10):1233–1236. doi:10.1016/j.dld.2016.07.003
49. Murray LJ, Din OS, Kumar VS, Dixon LM, Wadsley JC. Palliative radiotherapy in patients with esophageal carcinoma: a retrospective review. Pract Radiat Oncol. 2012;2(4):257–264. doi:10.1016/j.prro.2011.12.002
50. Bown SG. Palliation of malignant dysphagia: surgery, radiotherapy, laser, intubation alone or in combination? Gut. 1991;32(8):841–844. doi:10.1136/gut.32.8.841
51. Hanna WC, Sudarshan M, Roberge D, et al. What is the optimal management of dysphagia in metastatic esophageal cancer? Curr Oncol. 2012;19(2):e60–e66. doi:10.3747/co.19.892
52. Suzuki G, Yamazaki H, Aibe N, et al. Palliative Radiotherapy in the Local Management of Stage IVB Esophageal Cancer: factors Affecting Swallowing and Survival. Anticancer Res. 2017;37(6):3085–3092. doi:10.21873/anticanres.11664
53. Jeene PM, Vermeulen BD, Rozema T, et al. Short-course external beam radiotherapy versus brachytherapy for palliation of dysphagia in esophageal cancer: a matched comparison of two prospective trials. J Thorac Oncol. 2020;15(8):1361–1368. doi:10.1016/j.jtho.2020.04.032
54. Sur R, Donde B, Falkson C, et al. Randomized prospective study comparing high-dose-rate intraluminal brachytherapy (HDRILBT) alone with HDRILBT and external beam radiotherapy in the palliation of advanced esophageal cancer. Brachytherapy. 2004;3(4):191–195. doi:10.1016/j.brachy.2004.09.004
55. Rosenblatt E, Jones G, Sur RK, et al. Adding external beam to intra-luminal brachytherapy improves palliation in obstructive squamous cell oesophageal cancer: a prospective multi-centre randomized trial of the International Atomic Energy Agency. Radiother Oncol. 2010;97(3):488–494. doi:10.1016/j.radonc.2010.09.001
56. Welsch J, Kup PG, Nieder C, et al. Survival and symptom relief after palliative radiotherapy for esophageal cancer. J Cancer. 2016;7(2):125–130. doi:10.7150/jca.13655
57. Vermeulen BD, Jeene PM, Sijben J, et al. Low-dose versus high-dose radiation therapy for the palliation of dysphagia from esophageal cancer: a multicenter retrospective cohort study. Pract Radiat Oncol. 2020;10(4):e255–e263. doi:10.1016/j.prro.2019.10.010
58. Javed A, Pal S, Dash NR, et al. Palliative stenting with or without radiotherapy for inoperable esophageal carcinoma: a randomized trial. J Gastrointest Cancer. 2012;43(1):63–69. doi:10.1007/s12029-010-9206-4
59. Ng TM, Spencer GM, Sargeant IR, Thorpe SM, Bown SG. Management of strictures after radiotherapy for esophageal cancer. Gastrointest Endosc. 1996;43(6):584–590. doi:10.1016/s0016-5107(96)70196-7
60. Ajani JA, D’Amico TA, Bentrem DJ, et al. Esophageal and esophagogastric junction cancers, version 2.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(7):855–883. doi:10.6004/jnccn.2019.0033
61. Ilson DH, Saltz L, Enzinger P, et al. Phase II trial of weekly irinotecan plus cisplatin in advanced esophageal cancer. J Clin Oncol. 1999;17(10):3270–3275. doi:10.1200/JCO.1999.17.10.3270
62. Ilson DH, Forastiere A, Arquette M, et al. A phase II trial of paclitaxel and cisplatin in patients with advanced carcinoma of the esophagus. Cancer J. 2000;6(5):316–323.
63. Cwikiel M, Cwikiel W, Albertsson M. Palliation of dysphagia in patients with malignant esophageal strictures. Comparison of results of radiotherapy, chemotherapy and esophageal stent treatment. Acta Oncol. 1996;35(1):75–79. doi:10.3109/02841869609098483
64. Penniment MG, De Ieso PB, Harvey JA, et al.; T. C. E. group. Palliative chemoradiotherapy versus radiotherapy alone for dysphagia in advanced oesophageal cancer: a multicentre randomised controlled trial (TROG 03.01). Lancet Gastroenterol Hepatol. 2018;3(2):114–124. doi:10.1016/S2468-1253(17)30363-1
65. Herskovic A, Martz K, Al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med. 1992;326(24):1593–1598. doi:10.1056/NEJM199206113262403
66. Alsina M, Moehler M, Lorenzen S. Immunotherapy of esophageal cancer: current status, many trials and innovative strategies. Oncol Res Treat. 2018;41(5):266–271. doi:10.1159/000488120
67. Kakeji Y, Oshikiri T, Takiguchi G, et al. Multimodality approaches to control esophageal cancer: development of chemoradiotherapy, chemotherapy, and immunotherapy. Esophagus. 2021;18(1):25–32. doi:10.1007/s10388-020-00782-1
68. Homs MY, Steyerberg EW, Eijkenboom WM, et al. Single-dose brachytherapy versus metal stent placement for the palliation of dysphagia from oesophageal cancer: multicentre randomised trial. Lancet. 2004;364(9444):1497–1504. doi:10.1016/S0140-6736(04)17272-3
69. Bergquist H, Wenger U, Johnsson E, et al. Stent insertion or endoluminal brachytherapy as palliation of patients with advanced cancer of the esophagus and gastroesophageal junction. Results of a randomized, controlled clinical trial. Dis Esophagus. 2005;18(3):131–139. doi:10.1111/j.1442-2050.2005.00467.x
70. Polinder S, Homs MY, Siersema PD, Steyerberg EW, Dutch SSG. Cost study of metal stent placement vs single-dose brachytherapy in the palliative treatment of oesophageal cancer. Br J Cancer. 2004;90(11):2067–2072. doi:10.1038/sj.bjc.6601815
71. Song HY, Lee DH, Seo TS, et al. Retrievable covered nitinol stents: experiences in 108 patients with malignant esophageal strictures. J Vasc Interv Radiol. 2002;13(3):285–293. doi:10.1016/s1051-0443(07)61722-9
72. Eldeeb H, El-Hadaad HA. Radiotherapy versus stenting in treating malignant dysphagia. J Gastrointest Oncol. 2012;3(4):322–325. doi:10.3978/j.issn.2078-6891.2012.011
73. Rueth NM, Shaw D, D’Cunha J, Cho C, Maddaus MA, Andrade RS. Esophageal stenting and radiotherapy: a multimodal approach for the palliation of symptomatic malignant dysphagia. Ann Surg Oncol. 2012;19(13):4223–4228. doi:10.1245/s10434-012-2459-3
74. Qiu G, Tao Y, Du X, et al. The impact of prior radiotherapy on fatal complications after self-expandable metallic stents (SEMS) for malignant dysphagia due to esophageal carcinoma. Dis Esophagus. 2013;26(2):175–181. doi:10.1111/j.1442-2050.2012.01348.x
75. Nishimura Y, Nagata K, Katano S, et al.; Japanese Society for Esophageal. Severe complications in advanced esophageal cancer treated with radiotherapy after intubation of esophageal stents: a questionnaire survey of the Japanese Society for Esophageal Diseases. Int J Radiat Oncol Biol Phys. 2003;56(5):1327–1332. doi:10.1016/s0360-3016(03)00198-6
76. Touchefeu Y, Archambeaud I, Landi B, et al. Chemotherapy versus self-expanding metal stent as primary treatment of severe dysphagia from unresectable oesophageal or gastro-oesophageal junction cancer. Dig Liver Dis. 2014;46(3):283–286. doi:10.1016/j.dld.2013.10.012
77. Didden P, Spaander MC, Kuipers EJ, Bruno MJ. Safety of stent placement in recurrent or persistent esophageal cancer after definitive chemoradiotherapy: a case series. Gastrointest Endosc. 2012;76(2):426–430. doi:10.1016/j.gie.2012.03.004
78. Gaspar LE, Nag S, Herskovic A, Mantravadi R, Speiser B. American Brachytherapy Society (ABS) consensus guidelines for brachytherapy of esophageal cancer. Clinical Research Committee, American Brachytherapy Society, Philadelphia, PA. Int J Radiat Oncol Biol Phys. 1997;38(1):127–132. doi:10.1016/s0360-3016(97)00231-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.