")
Back to Journals » Journal of Pain Research » Volume 16
Opioid-Sparing Effects of Flurbiprofen Axetil as an Adjuvant to Ropivacaine in Pre-Emptive Scalp Infiltration for Post-Craniotomy Pain: Study Protocol for a Multicenter, Randomized Controlled Trial
Authors Zhang W, Li C, Zhao C , Ji N , Luo F
Received 2 December 2022
Accepted for publication 20 April 2023
Published 26 April 2023 Volume 2023:16 Pages 1415—1427
DOI https://doi.org/10.2147/JPR.S399454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
Wei Zhang,1,* Chunzhao Li,2,* Chunmei Zhao,3 Nan Ji,2 Fang Luo3
1Department of Day Surgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China; 2Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China; 3Department of Day Surgery and Pain Management, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100070, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Luo, Department of Day Surgery and Pain Management, Beijing Tiantan Hospital, Capital Medical University, No. 119 West Road, South 4th Ring Road, Fengtai District, Beijing, 100070, People’s Republic of China, Tel +86 10 59976664, Fax +86 10 67050177, Email [email protected] Nan Ji, Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, No. 119 West Road, South 4th Ring Road, Fengtai District, Beijing, 100070, People’s Republic of China, Email [email protected]
Background: Pain after craniotomy remains a poorly controlled problem that is mainly caused by the inflammatory reaction at the incision site. Nowadays, systemic opioids use, as first-line analgesics, is often limited because of adverse effects. Flurbiprofen axetil (FA) is a non-steroidal anti-inflammatory drug merged into emulsified lipid microspheres, which represent a strong affinity to inflammatory lesions. Local administration of flurbiprofen into a surgical wound has induced enhanced analgesic efficacy and few systemic or local adverse effects after oral surgery. However, the impact of local FA, as a non-opioid pharmacologic alternative, remains elusive on postoperative pain in craniotomy. In this study, we presume that pre-emptive infiltration of scalp with FA as an adjuvant to ropivacaine can lead to less sufentanil consumption postoperatively in patient controlled intravenous analgesia (PCIA) compared with ropivacaine alone.
Methods/Design: We design a multicenter, randomized controlled study that will enroll 216 subjects who are planned to receive supratentorial craniotomy. Patients will receive pre-emptive infiltration of scalp either with 50 mg FA and 0.5% ropivacaine, or with 0.5% ropivacaine alone. Primary outcome is total consumption of sufentanil with PCIA device at 48 h postoperatively.
Discussion: This is the first study attempting to explore the analgesic and safety profile of local FA as an adjuvant to ropivacaine for incisional pain in patients undergoing craniotomy. It will provide additional insights into the opioid-sparing analgesia pathways by local administration of NSAIDs for neurosurgery.
Keywords: flurbiprofen axetil, pre-emptive analgesia, scalp infiltration, opioid-sparing, craniotomy, postoperative pain
Introduction
Post-craniotomy pain remains a major challenge for patients’ outcome after neurosurgery. Recent studies reported that 55% to 80% of patients have experienced a moderate to severe pain within 48 h immediately after supratentorial craniotomy,1 which may induce abrupt increases in blood pressure (BP) and heart rate (HR), even leading to an elevated intracranial pressure. Moreover, severe or prolonged acute pain following craniotomy is a significant predictor for the development of chronic pain states.2,3 Nowadays, post-craniotomy pain is often insufficiently controlled due to the absence of international guidelines4 and concerns for analgesic-related side effects.5 The use of opioids, as the main-stray analgesics, can lead to profound neurological risks such as sedation, respiratory depression, nausea, vomiting, etc.6 There has also been a well-recognized opioid tolerance induced by the widespread use of remifentanil in neurosurgery.7 Furthermore, perioperative opioid prescriptions are associated with a substantial risk for chronic opioid-use disorders.8 Consequently, opioids limitation imposed by the nature of neurosurgery has led to a suboptimal post-craniotomy pain management, which is associated with increased inpatient morbidity and mortality, prolonged hospital stay or higher 30-day readmission rate. Therefore, an optimal approach to pain control is paramount to minimize the requirement for opioids and to improve postprocedural comfort.
Pain following craniotomy originates predominately from inflammatory sequelae after incisional damage in peri-cranial muscles and soft tissue.9 Ropivacaine, as a long-acting reginal analgesic, has been popularly administrated for scalp infiltration. It has been demonstrated to reduce the demand for opioids and other rescue analgesics after craniotomy.10,11 However, even with the addition of adrenaline, one single anesthetic would only be able to relieve the postoperative pain within the first 2 hours.12 Scalp infiltration with local anesthetics and anti-inflammatory drugs such as glucocorticoids has been proposed as a simple and effective analgesic approach, which reduces postoperative sufentanil consumptions or pain scores in a longer duration than local anesthetics alone for both adult and pediatric craniotomy patients in our previous research.13–15 However, the optimal concentration of glucocorticoids, which can be locally used without concern about complications such as local aseptic tissue atrophy or infection, remains controversial.
Non-steroidal anti-inflammatory drugs (NSAIDs), as the widely used perioperative analgesics, could effectively relieve postoperative pain and reduce opioid demands by 25–50% in a great diversity of surgical settings, and thus reduce the adverse effects associated with opioids.8,16 However, systemic NSAIDs might be associated with adverse effects including gastrointestinal disorders, bleeding, heart attacks or renal abnormalities. Notably, for patients receiving neurosurgery, systemic NSAIDs have required caution due to their anti-platelet action and concern about intra-cerebral bleeding.17 Previous studies have indicated that peripheral NSAIDs infiltration (or combined with regional anesthetics) significantly reduced consumption of supplementary analgesics by approximately 50–65% within 24 h postoperatively, with a delayed request for analgesic request by about 4–9 h than systemic route in arthroscopy or herniorrhaphy.18–22 Furthermore, it has been demonstrated that local NSAID could achieve its therapeutic tissue concentration with a plasma concentration at only <5% of that for systemic administration, so there is a lower incidence of undesirable effects secondary to systemic distribution of NSAIDs. Also, the local adverse effects are very few and transient, which may be attributed to the preservative or adhesive of NSAIDs. Therefore, NSAIDs might be considered a preferential adjuvant option for local infiltration, and those formulated in a targeted and sustained-release carrier may be more advantageous.23
Flurbiprofen axetil (FA), is an injectable NSAID commonly used for treatment of postoperative pain. FA is highly lipophilic by merging into a lipid microsphere carrier, which has a strong affinity to the surgical lesions and inflammatory tissues to achieve targeted drug therapy and prolonged duration of action, thus providing a basis for its local use to achieve efficiency and safety comparable or superior to systemic administration.24 In the oral surgery model, direct application of flurbiprofen microparticle at the incision leads to an almost 50% decrease in plasma drug level, as well as a superior analgesic effect in comparison to oral administration.25 The lower blood concentrations might predict less toxicity than that with systemic drug exposure, for example, the coagulation dysfunction. Furthermore, no increased incidence of oozing, hemorrhage or delayed healing has been observed at the surgical site. At present, no published studies are available concerning the efficiency of local FA on alleviating postoperative pain associated with craniotomy. In the study, we attempt to clarify the opioid-sparing efficacy of local FA as an adjunct in pre-emptive scalp infiltration. We hypothesize that this local FA/ropivacaine regimen could synergistically reduce opioid requirements with fewer side effects than ropivacaine alone after craniotomy.
Material and Methods
Study Design
This is an open labeled, randomized controlled, multi-center superiority trial with a two-group parallel design. Beijing Tiantan Hospital of Capital Medical University associated with the other two hospitals, Beijing Puhua International Hospital and Sanbo Brain Hospital of Capital Medical University, is responsible for this trial. Hospitalized patients will be randomized and enrolled from January 2023. According to the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) reporting guidelines,26 we have finished the SPIRIT checklist (Supplementary Files: Supplementary File 1). The study will involve 216 subjects who are scheduled for supratentorial craniotomy. Eligible and consenting patients will be assigned to receive pre-incisional scalp infiltration with ropivacaine plus FA or with ropivacaine alone at an allocation ratio of 1:1. The flow diagram is described in Figure 1. The participants’ schedule is displayed in Table 1.
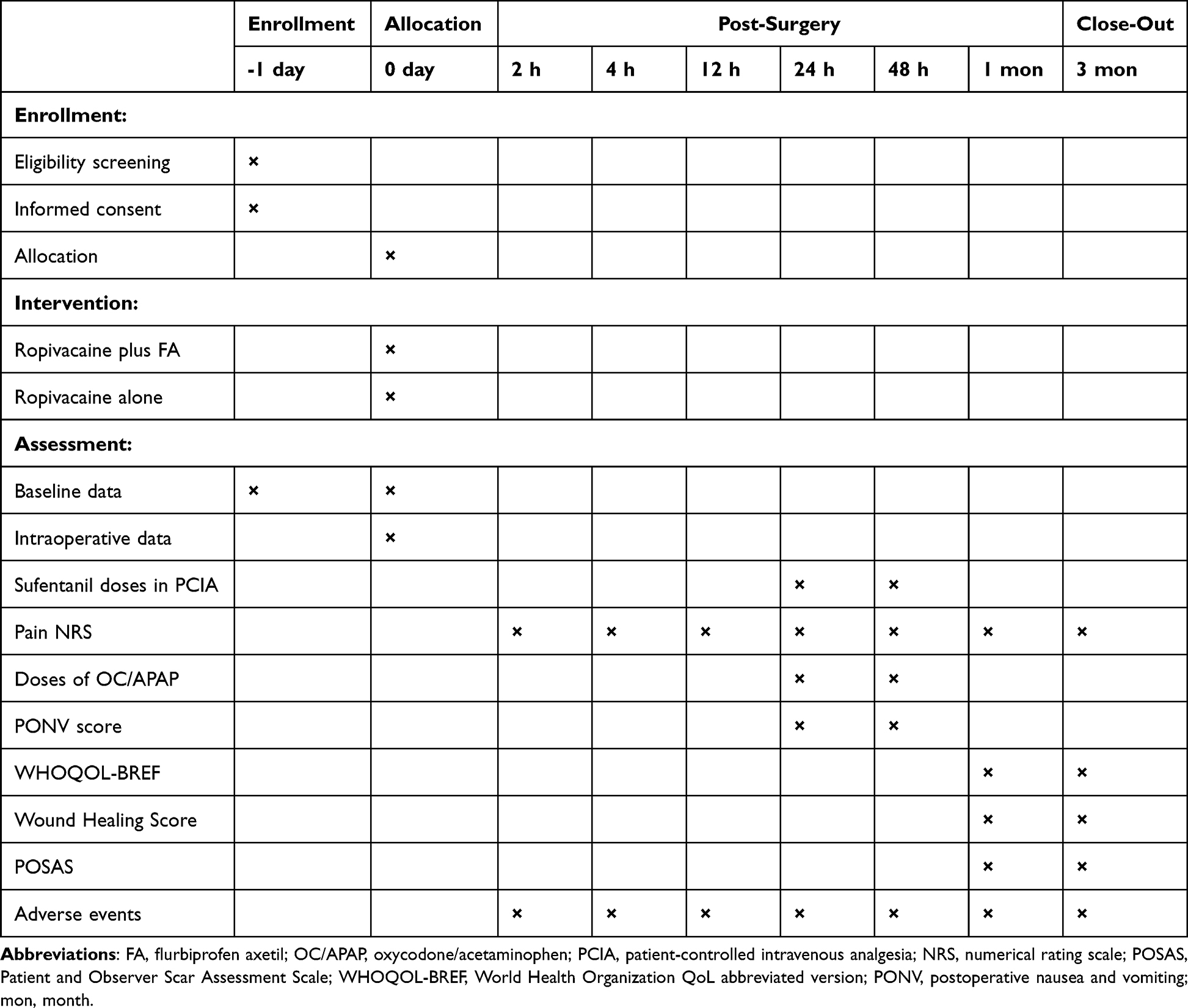 |
Table 1 The Schedule for Enrollment, Intervention and Assessments |
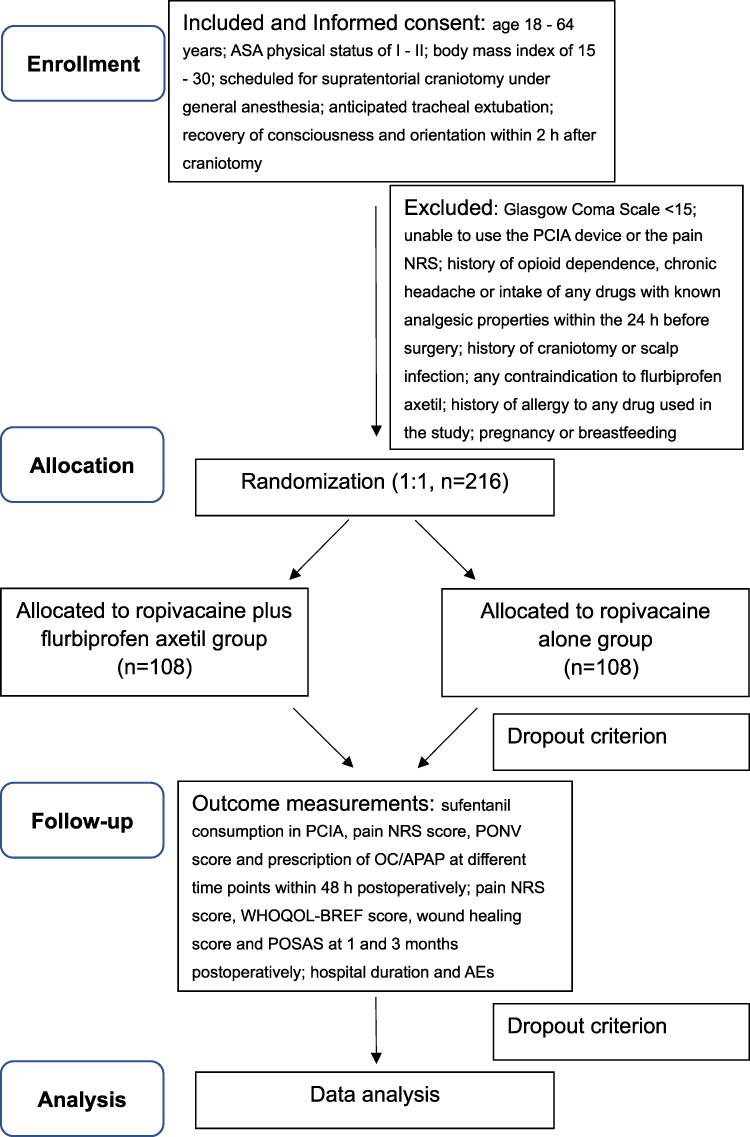 |
Figure 1 Flow diagram of the study design. Abbreviations: PCIA, patient-controlled intravenous analgesia; NRS, numerical rating scale; OC/APAP, oxycodone/acetaminophen; PONV, postoperative nausea and vomiting; WHOQOL-BREF, World Health Organization QoL abbreviated version; POSAS, Patient and Observer Scar Assessment Scale; AE, adverse events. |
Objectives
The study aims to determine whether the opioid-sparing effects of FA as an adjuvant to ropivacaine are superior to ropivacaine alone in pain relief for craniotomy. Based on the observation that PCIA (not administrated by nurse) opioids are the desirable option for studies on analgesia, this objective will be measured by calculating the consumption of sufentanil in PCIA pump within 48 h postoperatively.6 Secondary study objectives include comparisons of pain Numerical Rating Scale (NRS), number of PCIA button presses, timing of first rescue analgesia, incidence of AEs and patients’ recovery quality between the two groups.
Recruitment and Ethics
The trial is designed in accordance with the Declaration of Helsinki. The protocol has been approved by the Ethics Committee of Beijing Tiantan Hospital (KY-2018-034-02-10) and registered at ClinicalTrials.Gov (NCT 05624359; Principal investigator: Fang Luo; Registration date: November 07, 2022). Once commenced, all interventions will not be modified. This strategy will not collect or store biological specimens.
Neurosurgeons from the coordinating centers will perform an initial screening of all prospective patients in the department for neurosurgery. If the patients fulfill the eligibility criteria, they are referred to an independent researcher in each hospital, who will perform the final eligibility assessment. Eligible patients will be presented with a concise and key information about this trial by this researcher. The written informed consent (IC, Supplementary File 2), which meets the ethical requirements of our institutions, is requested from all subjects before surgery. This IC has been reviewed by Ethics Committee of the coordinating centers. Every subject will be given enough time to raise any questions regarding any intervention carried out during the research, and then decide whether to sign this IC. Participants will also agree to the storage and publication of their data by signing the IC. Participants can drop out of the current study anywhere and anytime.
Eligibility Criteria
Inclusion Criteria
- Age 18–64 years;
- ASA physical status of I–II;
- Body mass index (BMI) of 15–30;
- Planned to receive supratentorial craniotomy during general anesthesia;
- Recovery of consciousness and orientation, and tracheal extubation within 2 h after craniotomy.
Exclusion Criteria
- History of opioid dependence, chronic headache or intake of any other analgesic within the 24 h prior to surgery;
- History of craniotomy or scalp infection;
- Not able to use PCIA device or comprehend pain NRS;
- Glasgow Coma Scale of <15;
- Any contraindication to flurbiprofen axetil, such as gastrointestinal ulcer, coagulation disorders, renal dysfunction, severe cardiovascular diseases;
- Allergic to the drugs used in this trial;
- Pregnancy or breastfeeding.
Elimination Criteria
● Not extubated or not awake within 2 h postoperatively;
● Postoperative hematoma or brain swelling requiring urgent revision within 48 h postoperatively;
● GCS <15 or poor cognitive function within 48 h postoperatively;
● Lost in follow-up or voluntary withdrawal within 48 h postoperatively.
Randomization and Blinding
The allocation sequence as per a random number table will be generated using the block randomization method by SPSS 26.0 (SPSS Inc., Chicago, IL, USA) in each study center. On surgery day, a staff not participating in data collecting and processing provides this random assignment of each eligible patient (in a 1:1 ratio) to the attending neurosurgeon following a method based on opaque sealed envelopes. This neurosurgeon is in charge of preparing the respective infiltration solution. FA is a lipid emulsion and the solution is clear in ropivacaine alone group. So neurosurgeons, anesthesiologists and nurses will be aware of group assignations, while patients and the staff who are responsible for data processing and follow-up visit are blinded. This is an open label study and thus unblinding will not occur.
Dosing of Local FA
There has been an explicit association between drug dose and its analgesic effect in NSAIDs.27 FA could alleviate the pain induced by propofol injection at a dose of ≥50 mg; however, there is no significant difference at a dose of <50 mg compared to placebo groups.28 A single 50-mg dose of flurbiprofen has been demonstrated effective to control postoperative pain by systemic administration in different surgical settings, with no serious adverse effects reported.17,25,29–32 Furthermore, a retrospective analysis of 9915 cases has recommended FA of low dose (50–100mg) as the protective factor for acute kidney injury postoperatively, while larger dose (≥250 mg) has been regarded as the risk factor for noncardiac or non-neurologic surgery.33 As concerned for local use, direct wound infiltration of flurbiprofen microparticle (25 and 50 mg) has lowered the intensity and delayed the onset of postoperative pain in a dose-related manner than the same doses administered orally for patients undergoing molar extraction.25 On the basis of these results, we intend to choose a single dose of 50 mg FA diluted to 30 mL for local anesthetic infiltration in this study. Notably, the anticipated infiltration volume will usually be less than 30 mL due to the small incision length commonly chosen in all centers. So it seems to be relatively safe to administrate a local FA dose of < or = 50 mg.
Intervention Description
Scalp Infiltration
The neurosurgeons will prepare and administrate the infiltration solution in a sterile manner: 5 mL FA (50 mg; by Beijing Taide Pharmaceutical Co., Ltd) and 15 mL ropivacaine (10 mg/mL; by AstraZeneca AB, Sweden) in ropivacaine combined with FA group; 15 mL ropivacaine in ropivacaine alone group. Both solutions are diluted with normal saline to 30 mL. Since the average time-to-onset of FA is 30 min, we intend to perform scalp infiltration 30 min before surgical incision to make sure their pre-emptive treatment to cover both the incisional and inflammatory phases of craniotomy-induced pain.34 The assigned solution will be injected along the planned incision and pins’ locations for the Mayfield head holder with a needle of 22-gauge introduced at a 45° angle. The total dose of anesthetic infiltration will be determined on the length of skin incision, with a maximum consumption of 150 mg for ropivacaine and of 50 mg for FA, respectively.
Perioperative Interventions
Supratentorial craniotomy will be meticulously performed and fully integrated within the hospital’s routine clinical practice. All patients will receive midazolam 0.05 mg/kg, and then general anesthesia is induced with propofol 1.5–2 mg/kg, sufentanil 0.3–0.5 μg/kg, and rocuronium 0.6 mg/kg before being orotracheally intubated. The tidal volume is 6–8 mL/kg for mechanical ventilation. To achieve normocapnia, respiratory rate is adjusted ranging 12–15/min. Sevoflurane (0.4 MAC) and propofol (2–4 mg/kg∙h) will be used to maintain the anesthesia and to achieve a bispectral (BIS) index of 40–60. Standard monitoring, including electrocardiography, blood pressure (BP), heart rate (HR), output and input volumes, pulse oximetry (SpO2) and body temperature, will be continuously established. Remifentanil (0.05–0.2 μg/kg∙min) is used for intraoperative analgesia and will be discontinued when neurosurgeons remove the Mayfield head pins. No additional provision of analgesics will be planned throughout the surgery. Fluid management will be performed with balanced crystalloids and colloids to maintain normovolemia. Treatments such as supplying blood volume or using vasoactive agents will be applied to keep HR and MAP within 30% of the baseline values. Patients are admitted into Post Anesthesia Care Unit (PACU) when leaving the operating room.
PACU Interventions
A postoperative Patient Controlled Intravenous Analgesia (PCIA) pump is administered from admission into PACU. The pump will contain sufentanil 200 μg in 100 mL saline. The parameters will be set at 0.5 mL bolus doses with 15 min as the lockout time. There will be no continuous infusion or initial dose. The maximum dose will be limited to 2.0 mL (sufentanil 4 μg) per hour. Patients are instructed to press the button every 15 min until a satisfactory pain relief is obtained. Each press, including both valid and invalid, is stored in an electronic system.
Pain intensity is determined using a NRS scale at both the PACU and ward within 48 h after surgery, in which 0 denotes no pain and 10 denotes the most severe pain imaginable. Patients’ cognitive status is measured with the Short Orientation Memory Concentration test (SOMC).35 In this test, the cognitive function is rated as good, fair or poor if patients can recall and calculate with 1–2 mistakes, ≥3 mistakes or not able to recall at all, respectively. If the grading remains poor at 2 h postoperatively, the patient will be considered unfit for follow up and thus withdrawn from the study.36 Patients achieving an Aldrete score scoring of 9 or greater are eligible to be transferred to the neurosurgery ward.
Hospital Ward Interventions
In the ward, if a patient scores >4 in pain NRS after receiving a maximum dose of 2 mL per hour from PCIA device, a tablet of oxycodone (OC)/acetaminophen (APAP) (5/325 mg; by MallinckrodtInc, US) will be prescribed and supplemented as an oral rescue analgesic at an interval of at least 6 h.
Follow-Up
Follow-up is performed by two independent and experienced outcome assessors blinded to the grouping assignment. The PCIA sufentanil consumption, time to first PCIA press, pain NRS scores, OC/APAP requirements, scores of wound healing and PONV, Patient and Observer Scar Assessment Scale (POSAS) scores,37 World Health Organization QoL abbreviated version (WHOQOL-BREF) are assessed. The duration of follow-up visit lasts for 3 months to check the adverse events (AE) related to the administered agents and the perioperative care. It will be conducted by telephone interviews after patients’ discharge from hospital.
Strategies to Improve Adherence to Interventions
Before the trial, all investigators from three centers should be trained on standard trial implementation, quality control and outcomes assessment by online sessions, so as to ensure smooth operations and consistency. All the interventions in the current study will be implemented adhering to clinical practice guidelines. All patients will be guided on how to evaluate pain NRS and how to manage a PCIA device during a preoperative visit.
Outcome Measures
Baseline Characteristics
Patients’ demographic data consist of ASA grading, gender, age, BMI and comorbidities. Neurosurgical classification for elective craniotomy is based on ICD-9-CM-3 (International Classification of Diseases, Ninth Revision, Clinical Modification), including the resections of meningioma (01.512), cerebral convexity meningiomas (01.514), parasagittal meningioma (01.515), tentorial meningioma (01.516), cyst (01.591), encephaloma (01.594) and so on. Other perioperative characteristics are as follows, including incisional site, infiltration volume, surgery duration, anesthesia duration, intraoperative consumption of opioids (sufentanil and remifentanil), hemodynamic variables, etc.
Primary Outcome
Total sufentanil consumption in PCIA pump at 48 h after craniotomy.
Secondary Outcome
Total sufentanil consumption in PCIA pump at 24 h after craniotomy;
Time to first PCIA button press after craniotomy;
Acute pain NRS scores at 2, 4, 12, 48 h and 1 month after craniotomy;
Chronic pain NRS scores at 3 months after craniotomy;
The time to first prescription of OC/APAP after craniotomy;
Hospital duration after craniotomy;
WHOQOL-BREF score at 1 month and 3 months postoperatively, which represents a questionnaire referring to the general status of social, physical and psychological health, as well as the overall QoL. Each domain has a mean score ranging within 4–20. The larger number indicates the better quality of life;
PONV score at 24 and 48 h after craniotomy: 0, no PONV; 1, nausea, but no requiring treatment; 2, nausea, requiring treatment; 3, vomiting;
Patient and Observer Scar Assessment Scale (POSAS) at 1 month and 3 months postoperatively,38 consisting of the scales for components of both observer and patient;
Wound healing score at 1 month and 3 months postoperatively, which is rated as excellent, good and suboptimal;
The occurrence of other AEs during the treatment period and follow-up visit, which include cerebral hematoma, respiratory depression, gastrointestinal ulcerations and perforation, renal risks, coagulation dysfunction, allergic reaction and wound infection, oozing, hemorrhage, mild pruritus and burning sensation at the injection site.
Safety Assessment
In the study, all AEs will be assessed and documented in the case report form (CRF) until the end of 3 months’ follow-up. The safety data will include event type, onset time, duration, severity, possible causes, outcomes, as well as the association with study interventions. All AEs should be reported to Data Monitoring Committee (DMC) without delay, and all AEs should be treated immediately. This study should be terminated by the Institutional Review Board and DMC in case of AEs resulting in serious complications or even death.
Data Collection and Management
Two experienced outcome assessors in each center, who are blinded to the study arms, will perform follow-up assessments either by a face-to-face interview (within hospitalization) or in a telephone-based survey (after discharge). An independent researcher will be in charge of the collection of baseline data from the hospitalized medical record system. A consensus standard for both collection and assessment of all outcome variables will be decided on by the assessors and researcher before the study.
The primary investigator is responsible for the data completeness and preciseness. For patients who discontinue or deviate from study, their data will be retained until termination, except for those who cannot be assessed for total sufentanil consumption in PCIA pump at 48 h after craniotomy (primary outcome).
All data are recorded into the CRFs, which will be assigned identification codes to ensure anonymization. These paper-based files will be stored in a secure area under lock and key throughout the trial to guarantee strict confidentiality for research purposes only. A participant identification list (a code corresponding to a participant name), together with other records containing personal identifiers, such as IC forms, will be kept separately from the CRFs. Two independent staff will establish a database with double-checking, on a computer protected by double passwords. Only the independent statistician, the primary investigator, and the DMC can access to patients’ database. Participants will have the right to obtain their own data, to transfer the data to a third party or cancel the data during the trial.
Data Monitoring Committee (DMC)
The DMC is composed by specialists in methodology, statistics and ethics. All members will be required to sign a conflict-of-interest statement. Regular interviews and audit meetings, which will be independent from all investigators, are devoted to verifying the data collection and assessment, as well as the adverse events reports. There will be an interim analysis carried out after 50% of patient inclusion. DMC will audit the results and decide if the early stopping rule should be effectuated. Every adverse event or reaction will be reported to DMC, which will determine the relatedness of an incident to the study interventions. This trial is to be immediately terminated in case of life-threatening AEs, which could lead to serious comorbidities or mortality.
Dissemination Plans
Our results will be published in an international scientific journal and presented at medical conferences related to postoperative pain management.
Missing Data
Missing data are handled by multiple imputations to complete the data set throughout the study.
Sample Size
The sample size is calculated to test the superiority of local FA plus ropivacaine protocol over ropivacaine alone protocol in the opioid-sparing effects after craniotomy, which is measured by sufentanil consumption in PCIA pump at 48 h postoperatively (primary outcome). No data are available for the requirement dose of analgesics for postoperative pain following local administration of FA. However, a previous study has demonstrated that wound infiltration with lidocaine plus another NSAID drug (ketorolac) has led to a reduction of 51% in analgesic consumption following hand surgery, as compared to lidocaine alone.39 Our team have reported that the sufentanil requirement has been reduced by 25–87% with the addition of anti-inflammatory glucocorticoid as an adjuvant to ropivacaine in pre-incisional infiltration for postoperative pain in craniotomy.13–15 Taken together, we try to obtain a discrepancy of 50% in sufentanil consumption for the current protocol. Thus, a sample of 86 patients for each arm is calculated using PASS V.11 software (NCSS, Kaysville, Utah, USA), with the two-sided significance level set at 0.05, as well as a 90% power. Assuming a 20% dropout rate, 216 subjects are required in the current study (n = 108 for each group).
Statistics
All statistical analyses will be carried out using SPSS 26.0 by an independent statistician. He is totally blinded to the grouping. Statistical analyses will follow the intention-to-treat principle and we consider a P-value of <0.05 as statistically significant. Baseline demographic and clinical characteristics will be displayed in both groups. After checking for normal distribution by Kolmogorov–Smirnov test, the normally distributed quantitative variables are defined as mean ± SD. The abnormally distributed quantitative variables are defined as median (interquartile ranges, IQRs). Qualitative variables are described as proportions.
The primary outcome is the total consumption of sufentanil within PCIA pump at 48 h postoperatively. For normally distributed data, it will be analyzed using independent two-tailed t tests. For skewed data, it will be analyzed using Mann–Whitney U-test. The secondary quantitative variables, including pain NRS scores, scores of wound healing and PONV, POSAS scores, WHOQOL-BREF, and the duration of hospitalization are compared by similar methods. Time to first PCIA button press, as well as the time to first rescue analgesic, are analyzed by Log rank test, with Kaplan–Meier curves using the hazard ratio (HR) with 95% confidence interval (CI). As a secondary analysis, the AEs incidence is compared by Fisher’s exact test or Chi-square test.
An interim analysis will be conducted when half of the participants (n = 108) have completed the follow-up. Based on the O’Brien-Fleming technique for benefits or harms, an early stopping rule will be applied when a P value achieves <0.001 in comparisons for primary outcome or incidence of AEs between the two groups.
Discussion
To our knowledge, very few reports have evaluated the efficacy of local NSAIDs as a component of the standard post-surgical pain management regimen for patients undergoing craniotomy. Flurbiprofen, as a member of the NSAIDs commonly used for the treatment of inflammation, could reduce the biosynthesis of prostaglandins, control pain associated with endogenous inflammatory mediators, and depress peripheral and central sensitization.28 There has been evidence that preemptive systemic FA results in a pain relief within 24 h after surgery, as well as significant decreased plasma levels of TNF-α and IL-6 at 24 and 48 h after surgery.29,32,40 Locally applied flurbiprofen, with similar or lower doses of systemic route, has led to a higher drug concentration and bioavailability at the original point of inflammatory process, as well as a lower plasma concentration. This could subsequently contribute to more effective analgesic and anti-inflammatory potentials over a longer duration.25,41,42 The lower plasma concentrations also indicate lower risk for systemic side effects. Therefore, we support the local use of FA, a formulation of flurbiprofen encapsulated in lipid microspheres, as an adjunct in the standard pain relief regimen for patients undergoing craniotomy. We hypothesize that pre-incisional infiltration with FA and ropivacaine could spare the consumption of opioids by exerting their anti-inflammatory and analgesic effects directly on the peri-incisional tissues than with ropivacaine alone.
Administration of FA into a surgical site could raise concerns regarding local adverse sequelae. However, a systematic review has confirmed that the local adverse effects of NSAIDs are very few and seem constricted to mild pruritus or burning sensation for a short duration.43 Furthermore, there has been no increased incidence of local complications by direct administration of flurbiprofen at the extraction site after an oral surgery.25 Also, to our knowledge, there have been no reports of serious AEs associated with mixture of NASIDs and ropivacaine. However, it should be noted that there has been a limited number of trials. In this study, local FA-related soft-tissue damage will be evaluated as measured by wound healing scores and POSAS scores, and serious safety concerns will provide the recommendations on stopping the study. Also, drug-related bleeding complications, including cerebral hematoma, coagulation dysfunction and wound hemorrhage will be observed. But future studies specifically concerning the effects of local NSAIDs on coagulation are needed before final recommendations can be made. Thus, this protocol will hold promise for addressing the potential safety profile of local NSAIDs in postoperative pain management.
There might be concern about the cost of adjunctive FA for our patients. However, it is reported that opioid consumption has been decreased by nearly 50% with the use of flurbiprofen,8 so as to reduce opioid-related AEs that could otherwise lead to substantially worse outcomes, for example, an increased mortality, a prolonged stay, higher care cost, or a higher incidence of 30-day readmission.44 Conversely, NSAIDs-related AEs were few overall. Therefore, substantial cost savings of health care could be realized by using FA. Maybe further evaluation should focus on its economic impact on cost benefit.
Previous studies have indicated that opioids such as sufentanil and fentanyl are commonly used in anesthesia and postoperative analgesia for neurosurgery.45–48 In the current study, the reasons we chose sufentanil as a standard care for neurosurgery are as follows. First, it is reported that induction of anesthesia with sufentanil generally offered an optimal profile of haemodynamics that was comparable or even superior to that of fentanyl following intubation and operation intervention, an advantage especially desirable for neurosurgical scenarios.49 Furthermore, the induction time was significantly shorter because sufentanil has a faster onset of action than fentanyl. Secondly, sufentanil exhibits shorter elimination half-life and context sensitive half-time than fentanyl after repeated or prolonged administration.49,50 Thus, sufentanil was preferred to provide a fast track awakening after neurosurgery and allow for a rapid emergence for prompt neurologic assessment and cognitive recovery.51 Thirdly, it has been demonstrated that sufentanil-related side effects, including PONV, sedation and so on, usually occurred in up to 30% of patients, which were comparable to those with fentanyl.45,52 Sufentanil is a potent analgesic with marked protein binding, higher lipid solubility, shorter distribution or elimination half-life, and faster onset of action than routinely used fentanyl and morphine for postoperative pain.53 Therefore, it has provided a greater selection for pain control after craniotomy.
Some limitations can be detected from our protocol. Firstly, both surgeons and anesthesiologists are not blinded because FA is a non-transparent emulsion. Therefore, non-transparent syringes are in urgent need. However, this limitation should be acceptable as outcome assessing is blinded and adequate training is provided. Secondly, although surgical approach is limited to supratentorial on account of the fact that craniotomy site could influence the intensity and incidence of postoperative pain in craniotomy, this will involve a variety of incision sites that could undoubtedly produce a range of postoperative pain.54 However, specifying the accurate location further, for example, craniotomy involving temporal muscle incision, could have weakened the generalizability and feasibility of our trial. Thirdly, one single dose of FA is selected in the study. Further attempts will be warranted to evaluate the dose-dependent effect of FA for local use. Fourthly, we do not recruit neurosurgical patients with ASA grading of 3 or more in this multi-center study, who may account for a higher proportion of population in many other institutions. Therefore, future study should focus on these patients to enrich our understandings of the opioid-sparing effects of local NSAIDs for neurosurgical patients with higher ASA grades. Finally, PCAs are uncommon for patients who are not awake postoperatively in many neurological scenarios, where we could tally the morphine equivalents and correlate to pain scores for assessment. Our exclusion of these patients might limit the generalizability of this trial, and thus indicating an urgent recommendation for more specific and expanded surgical stratifying in our future study.
In conclusion, post-craniotomy pain is a common disorder posing significant clinical, psychological and economic implications. No optimal analgesic strategy is available at present. If this study obtained a substantial decline in postoperative opioid consumption for patients receiving pre-incision infiltration with ropivacaine plus local FA than with ropivacaine alone, it will definitely optimize neurosurgical patients’ pain outcome, and thus help to inform the future studies and guidelines.
Abbreviations
FA, flurbiprofen axetil; NSAIDs, nonsteroidal anti-inflammatory drugs; PCIA, patient-controlled intravenous analgesia; IC, informed consent; BMI, body mass index; CRF, case report form; HR, heart rate; BP, blood pressure; BIS, bispectral index; SpO2, pulse oximetry; PACU, Post Anesthesia Care Unit; NRS, numerical rating scale; SOMC, Short Orientation Memory Concentration; POSAS, Patient and Observer Scar Assessment Scale; WHOQOL-BREF, World Health Organization QoL abbreviated version; PONV, postoperative nausea and vomiting; OC/APAP, oxycodone/acetaminophen; DMC, Data Monitoring Committee; AE, adverse events.
Data Sharing Statement
The datasets used and analyzed during this study are available from corresponding author Fang Luo on request.
Ethics Approval and Informed Consent
This trial will be performed in accordance with “Declaration of Helsinki”. The ethics approval (KY-2018-034-02-10) has been obtained from the Ethics Committee of Beijing Tiantan Hospital. All participants will sign the IC to participate before enrollment.
Author Contributions
Wei Zhang and Chunzhao Li have equally contributed to the protocol. They are regarded as co-first authors. All authors have made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. All authors have taken part in drafting, revising or critically reviewing the article and approved the final manuscript to be published. All authors have agreed on the journal to which the article has been submitted and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare that they have no competing interests.
References
1. Gaudray E, Martin E, Martin E, et al. Efficacy of scalp nerve blocks using ropivacaine 0.75% associated with intravenous dexamethasone for postoperative pain relief in craniotomies. Clin Neurol Neurosurg. 2020;197:106125. doi:10.1016/j.clineuro.2020.106125
2. Richebe P, Julien M, Brulotte V. Potential strategies for preventing chronic postoperative pain: a practical approach: continuing professional development. Can J Anaesth. 2015;62(12):1329–1341. doi:10.1007/s12630-015-0499-4
3. de Gray LC, Matta BF. Acute and chronic pain following craniotomy: a review. Anaesthesia. 2005;60(7):693–704. doi:10.1111/j.1365-2044.2005.03997.x
4. Tsaousi GG, Logan SW, Bilotta F. Postoperative pain control following craniotomy: a systematic review of recent clinical literature. Pain Pract. 2017;17(7):968–981. doi:10.1111/papr.12548
5. Gottschalk A, Berkow LC, Stevens RD, et al. Prospective evaluation of pain and analgesic use following major elective intracranial surgery. J Neurosurg. 2007;106(2):210–216. doi:10.3171/jns.2007.106.2.210
6. Jones SJ, Cormack J, Murphy MA, Scott DA. Parecoxib for analgesia after craniotomy. Br J Anaesth. 2009;102(1):76–79. doi:10.1093/bja/aen318
7. Vinik HR, Kissin I. Rapid development of tolerance to analgesia during remifentanil infusion in humans. Anesth Analg. 1998;86(6):1307–1311. doi:10.1213/00000539-199806000-00033
8. Martinez L, Ekman E, Nakhla N. Perioperative opioid-sparing strategies: utility of conventional NSAIDs in adults. Clin Ther. 2019;41(12):2612–2628. doi:10.1016/j.clinthera.2019.10.002
9. Puntis M, Garner A. Management of pain following craniotomy. Br J Nurs. 2015;24(14):740–744. doi:10.12968/bjon.2015.24.14.740
10. Law-Koune JD, Szekely B, Fermanian C, Peuch C, Liu N, Fischler M. Scalp infiltration with bupivacaine plus epinephrine or plain ropivacaine reduces postoperative pain after supratentorial craniotomy. J Neurosurg Anesthesiol. 2005;17(3):139–143. doi:10.1097/01.ana.0000171730.41008.da
11. Leone S, Di Cianni S, Casati A, Fanelli G. Pharmacology, toxicology, and clinical use of new long acting local anesthetics, ropivacaine and levobupivacaine. Acta Biomed. 2008;79(2):92–105.
12. Saringcarinkul A, Boonsri S. Effect of scalp infiltration on postoperative pain relief in elective supratentorial craniotomy with 0.5% bupivacaine with Adrenaline 1:400,000. J Med Assoc Thai. 2008;91(10):1518–1523.
13. Zhao C, Wang S, Pan Y, Ji N, Luo F. Pre-emptive incision-site infiltration with ropivacaine plus dexamethasone for postoperative pain after supratentorial craniotomy: a prospective randomized controlled trial. J Pain Res. 2021;14:1071–1082. doi:10.2147/JPR.S300943
14. Han X, Ren T, Wang Y, Ji N, Luo F. Postoperative analgesic efficacy and safety of ropivacaine plus diprospan for preemptive scalp infiltration in patients undergoing craniotomy: a prospective randomized controlled trial. Anesth Analg. 2022;135(6):1253–1261. doi:10.1213/ANE.0000000000005971
15. Zhao C, Zhang N, Shrestha N, Liu H, Ge M, Luo F. Dexamethasone as a ropivacaine adjuvant to pre-emptive incision-site infiltration analgesia in pediatric craniotomy patients: a prospective, multicenter, randomized, double-blind, controlled trial. Paediatr Anaesth. 2021;31(6):665–675. doi:10.1111/pan.14178
16. Schug SA, Manopas A. Update on the role of non-opioids for postoperative pain treatment. Best Pract Res Clin Anaesthesiol. 2007;21(1):15–30. doi:10.1016/j.bpa.2006.12.002
17. Jian M, Li X, Wang A, Zhang L, Han R, Gelb AW. Flurbiprofen and hypertension but not hydroxyethyl starch are associated with post-craniotomy intracranial haematoma requiring surgery. Br J Anaesth. 2014;113(5):832–839. doi:10.1093/bja/aeu185
18. Reuben SS, Connelly NR. Postoperative analgesia for outpatient arthroscopic knee surgery with intraarticular bupivacaine and ketorolac. Anesth Analg. 1995;80(6):1154–1157. doi:10.1097/00000539-199506000-00015
19. Lin CF, Wong KL, Chan YL, Wang JM, Wu KH, Wei TT. Comparison of local infiltration of tenoxicam and intravenous tenoxicam for postoperative analgesia in herniorrhaphy. Acta Anaesthesiol Sin. 1998;36(1):23–29.
20. Connelly NR, Reuben SS, Albert M, Page D. Use of preincisional ketorolac in hernia patients: intravenous versus surgical site. Reg Anesth. 1997;22(3):229–232. doi:10.1016/S1098-7339(06)80006-4
21. Reuben SS, Connelly NR. Postarthroscopic meniscus repair analgesia with intraarticular ketorolac or morphine. Anesth Analg. 1996;82(5):1036–1039. doi:10.1097/00000539-199605000-00027
22. Ben-David B, Baune-Goldstein U, Goldik Z, Gaitini L. Is preoperative ketorolac a useful adjunct to regional anesthesia for inguinal herniorrhaphy? Acta Anaesthesiol Scand. 1996;40(3):358–363. doi:10.1111/j.1399-6576.1996.tb04445.x
23. Romsing J, Moiniche S, Ostergaard D, Dahl JB. Local infiltration with NSAIDs for postoperative analgesia: evidence for a peripheral analgesic action. Acta Anaesthesiol Scand. 2000;44(6):672–683. doi:10.1034/j.1399-6576.2000.440607.x
24. Yao H, Luo X, Zhang H, An H, Feng W, Feng Y. The comparison of plasma and cerebrospinal fluid R(-)- and S(+)-flurbiprofen concentration after intravenous injection of flurbiprofen axetil in human subjects. Front Pharmacol. 2021;12:646196. doi:10.3389/fphar.2021.646196
25. Dionne RA, Haynes D, Brahim JS, Rowan JS, Guivarch PH. Analgesic effect of sustained-release flurbiprofen administered at the site of tissue injury in the oral surgery model. J Clin Pharmacol. 2004;44(12):1418–1424. doi:10.1177/0091270004265703
26. Chan AW, Tetzlaff JM, Gotzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
27. Collins SL, Moore RA, McQuay HJ, Wiffen PJ. Oral ibuprofen and diclofenac in post-operative pain: a quantitative systematic review. Eur J Pain. 1998;2(4):285–291. doi:10.1016/S1090-3801(98)90027-1
28. Zhang L, Zhu J, Xu L, et al. Efficacy and safety of flurbiprofen axetil in the prevention of pain on propofol injection: a systematic review and meta-analysis. Med Sci Monit. 2014;20:995–1002. doi:10.12659/MSM.890102
29. Chen JQ, Wu Z, Wen LY, Miao JZ, Hu YM, Xue R. Preoperative and postoperative analgesic techniques in the treatment of patients undergoing transabdominal hysterectomy: a preliminary randomized trial. BMC Anesthesiol. 2015;15:70. doi:10.1186/s12871-015-0046-4
30. Li X, Yu L, Yang J, Tan H. Multimodal analgesia with ropivacaine wound infiltration and intravenous flurbiprofen axetil provides enhanced analgesic effects after radical thyroidectomy: a randomized controlled trial. BMC Anesthesiol. 2019;19(1):167. doi:10.1186/s12871-019-0835-2
31. Sultan A, McQuay HJ, Moore RA, Derry S. Single dose oral flurbiprofen for acute postoperative pain in adults. Cochrane Database Syst Rev. 2009;2009(3):CD007358. doi:10.1002/14651858.CD007358.pub2
32. Wang K, Luo J, Zheng L, Luo T. Preoperative flurbiprofen axetil administration for acute postoperative pain: a meta-analysis of randomized controlled trials. J Anesth. 2017;31(6):852–860. doi:10.1007/s00540-017-2409-0
33. Wang D, Yang SK, Zhao MX, et al. Low dose of flurbiprofen axetil decrease the rate of acute kidney injury after operation: a retrospective clinical data analysis of 9915 cases. BMC Nephrol. 2020;21(1):52. doi:10.1186/s12882-020-1711-5
34. Nakayama M, Ichinose H, Yamamoto S, Nakabayashi K, Satoh O, Namiki A. Perioperative intravenous flurbiprofen reduces postoperative pain after abdominal hysterectomy. Can J Anaesth. 2001;48(3):234–237. doi:10.1007/BF03019751
35. Katzman R, Brown T, Fuld P, Peck A, Schechter R, Schimmel H. Validation of a short orientation-memory-concentration test of cognitive impairment. Am J Psychiatry. 1983;140(6):734–739.
36. Vallapu S, Panda NB, Samagh N, Bharti N. Efficacy of dexmedetomidine as an adjuvant to local anesthetic agent in scalp block and scalp infiltration to control postcraniotomy pain: a double-blind randomized trial. J Neurosci Rural Pract. 2018;9(1):73–79. doi:10.4103/jnrp.jnrp_310_17
37. Jia Y, Zhao C, Ren H, Wang T, Luo F. Pre-emptive scalp infiltration with dexamethasone plus ropivacaine for postoperative pain after craniotomy: a protocol for a prospective, randomized controlled trial. J Pain Res. 2019;12:1709–1719. doi:10.2147/JPR.S190679
38. Fearmonti R, Bond J, Erdmann D, Levinson H. A review of scar scales and scar measuring devices. Eplasty. 2010;10:e43.
39. Reuben SS, Duprat KM. Comparison of wound infiltration with ketorolac versus intravenous regional anesthesia with ketorolac for postoperative analgesia following ambulatory hand surgery. Reg Anesth. 1996;21(6):565–568.
40. Geng W, Hong W, Wang J, et al. Flurbiprofen axetil enhances analgesic effects of sufentanil and attenuates postoperative emergence agitation and systemic proinflammation in patients undergoing tangential excision surgery. Mediators Inflamm. 2015;2015:1–6. doi:10.1155/2015/601083
41. Yang C, Li T. Transdermal delivery of flurbiprofen from polyoxypropylene-polyoxyethylene block copolymer stabilized reduced graphene oxide to manage pain in spondylitis: in vitro and in vivo studies. Eur J Pharm Sci. 2021;165:105929. doi:10.1016/j.ejps.2021.105929
42. Amemiya M, Nakagawa Y, Yoshimura H, et al. Comparison of tissue pharmacokinetics of esflurbiprofen plaster with flurbiprofen tablets in patients with knee osteoarthritis: a multicenter randomized controlled trial. Biopharm Drug Dispos. 2021;42(9):418–426. doi:10.1002/bdd.2302
43. Brubaker L, Kendall L, Reina E. Multimodal analgesia: a systematic review of local NSAIDs for non-ophthalmologic postoperative pain management. Int J Surg. 2016;32:158–166. doi:10.1016/j.ijsu.2016.07.003
44. Shafi S, Collinsworth AW, Copeland LA, et al. Association of opioid-related adverse drug events with clinical and cost outcomes among surgical patients in a large integrated health care delivery system. JAMA Surg. 2018;153(8):757–763. doi:10.1001/jamasurg.2018.1039
45. Jamali S, Archer D, Ravussin P, Bonnafous M, David P, Ecoffey C. The effect of skull-pin insertion on cerebrospinal fluid pressure and cerebral perfusion pressure: influence of sufentanil and fentanyl. Anesth Analg. 1997;84(6):1292–1296. doi:10.1213/00000539-199706000-00022
46. Grundy BL, Pashayan AG, Mahla ME, Shah BD. Three balanced anesthetic techniques for neuroanesthesia: infusion of thiopental sodium with sufentanil or fentanyl compared with inhalation of isoflurane. J Clin Anesth. 1992;4(5):372–377. doi:10.1016/0952-8180(92)90158-W
47. Su S, Ren C, Zhang H, Liu Z, Zhang Z. The opioid-sparing effect of perioperative dexmedetomidine plus sufentanil infusion during neurosurgery: a retrospective study. Front Pharmacol. 2016;7:407. doi:10.3389/fphar.2016.00407
48. Craen RA, Gelb AW. The anaesthetic management of neurosurgical emergencies. Can J Anaesth. 1992;39(5 Pt 2):R29–R39. doi:10.1007/BF03008841
49. Clotz MA, Nahata MC. Clinical uses of fentanyl, sufentanil, and alfentanil. Clin Pharm. 1991;10(8):581–593.
50. Djian MC, Blanchet B, Pesce F, et al. Comparison of the time to extubation after use of remifentanil or sufentanil in combination with propofol as anesthesia in adults undergoing nonemergency intracranial surgery: a prospective, randomized, double-blind trial. Clin Ther. 2006;28(4):560–568. doi:10.1016/j.clinthera.2006.04.001
51. Gerlach K, Uhlig T, Huppe M, et al. Remifentanil-propofol versus sufentanil-propofol anaesthesia for supratentorial craniotomy: a randomized trial. Eur J Anaesthesiol. 2003;20(10):813–820. doi:10.1097/00003643-200310000-00007
52. Hassani E, Mahoori A, Sane S, Tolumehr A. Comparison the effects of paracetamol with sufentanil infusion on postoperative pain control after craniotomy in patients with brain tumor. Adv Biomed Res. 2015;4:64. doi:10.4103/2277-9175.152610
53. Scholz J, Steinfath M, Schulz M. Clinical pharmacokinetics of alfentanil, fentanyl and sufentanil. An Update Clin Pharmacokinet. 1996;31(4):275–292. doi:10.2165/00003088-199631040-00004
54. Thibault M, Girard F, Moumdjian R, Chouinard P, Boudreault D, Ruel M. Craniotomy site influences postoperative pain following neurosurgical procedures: a retrospective study. Can J Anaesth. 2007;54(7):544–548. doi:10.1007/BF03022318
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.