")
Back to Journals » Clinical Interventions in Aging » Volume 15
Opioid Poisoning and Opioid Use Disorder in Older Trauma Patients
Authors Daoust R , Paquet J , Moore L, Cournoyer A , Émond M, Gosselin S, Lavigne GJ, Boulanger A, Mac-Thiong JM, Chauny JM
Received 7 March 2020
Accepted for publication 9 May 2020
Published 27 May 2020 Volume 2020:15 Pages 763—770
DOI https://doi.org/10.2147/CIA.S252849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Raoul Daoust,1,2 Jean Paquet,1 Lynne Moore,3,4 Alexis Cournoyer,1,2 Marcel Émond,5 Sophie Gosselin,6,7 Gilles J Lavigne,8,9 Aline Boulanger,10,11 Jean-Marc Mac-Thiong,2,12 Jean-Marc Chauny1,2
1Centre d’Étude en Médecine d’Urgence, Hôpital du Sacré-Coeur de Montréal, Montréal, Quebec, Canada; 2Département Médecine Familiale et Médecine d’Urgence, Faculté de Médecine, Université de Montréal, Montréal, Quebec, Canada; 3Département de médecine sociale et préventive, Faculté de médecine, Université Laval, Quebec, Quebec, Canada; 4Axe de recherche en traumatologie-urgence-soins intensifs du Centre de recherche FRQS du CHU-Québec, Quebec, Quebec, Canada; 5Département de médecine familiale et de médecine d’urgence, Faculté DE médecine, Université Laval, Quebec, Quebec, Canada; 6Department of Emergency Medicine, McGill University Health Centre, McGill University, Montréal, Quebec, Canada; 7Département de médecine d’urgence, CISSS-Montérégie-Centre, Greenfield Park, Québec, Canada; 8Faculties of Dental Medicine and Medicine, Université de Montréal, Montréal, Quebec, Canada; 9Center for Advanced Research in Sleep Medicine, Hôpital du Sacré-Coeur de Montréal (CIUSSS du Nord de-l’Île-de-Montréal), Montréal, Quebec, Canada; 10Centre de recherche du Centre Hospitalier de l’Université de Montréal (CRCHUM), Montréal, Quebec, Canada; 11Département d’anesthésiologie, Faculté de médecine, Université de Montréal, Montréal, Quebec, Canada; 12Research Centre, Hôpital du Sacré-Coeur (CIUSSS du Nord de-l’île-de-Montréal), Montréal, Quebec, Canada
Correspondence: Raoul Daoust Email [email protected]
Background: Patients hospitalized following a traumatic injury will be frequently treated with opioids during their stay and after discharge. We examined the relationship between acute phase (< 3 months) opioid use after discharge and the risk of opioid poisoning or use disorder in older trauma patients.
Methods: In a retrospective multicenter cohort study conducted on registry data, we included all patients ≥ 65 years admitted (hospital stay > 2 days) for injury in 57 trauma centers in the province of Quebec (Canada) between 2004 and 2014. We searched for opioid poisoning and opioid use disorder from ICD-9 to ICD-10 code diagnosis after their initial injury. Patients that filled an opioid prescription within a 3-month period after sustaining the trauma were compared to those who did not, using Cox proportional hazards regressions.
Results: A total of 70,314 admissions were retained for analysis; median age was 82 years (IQR: 75– 87), 68% were women, and 34% of the patients filled an opioid prescription within 3 months of the initial trauma. During a median follow-up of 2.6 years (IQR: 1– 5), 192 participants (0.27%; 95% CI: 0.23%-0.31%) were hospitalized for opioid poisoning and 73 (0.10%; 95% CI: 0.08%-0.13%) were diagnosed with opioid use disorder. Having filled an opioid prescription within 3 months of injury was associated with an increased hazard ratio of opioid poisoning (2.8; 95% CI: 2.1– 3.8) and opioid use disorder (4.2; 95% CI: 2.4– 7.4) after the injury. However, history of opioid poisoning (2.6; 95% CI: 1.1– 5.8), of substance use disorder (4.3; 95% CI: 2.4– 7.7), or of the opioid prescription filled (2.8; 95% CI: 2.2– 3.6) before the trauma, was also related to opioid poisoning or opioid use disorder after the injury.
Conclusion: Opioid poisoning and opioid use disorder are rare events after hospitalization for trauma in older patients. However, opioids should be used cautiously in patients with a history of substance use disorder, opioid poisoning or opioid use.
Keywords: prescription opioids, opioid poisoning, opioid use disorder, trauma, injury, older adults
Introduction
As a consequence of the rise in opioid prescriptions over the last 20 years, prescription opioid dependence and overdose have increased to epidemic proportions, in both the United States (US) and Canada.1–4 A 2015 US national survey reported that 0.8% of the general population had opioid use disorder with a higher prevalence among prescription opioid users (2.1%) and among US chronic pain patients (8–12%).5,6 A registry of almost 400,000 individuals who filled at least one opioid prescription showed over a 3-year follow-up similar rate of opioid misuse (2.7%) and a very low rate of opioid overdose (0.28%).7 Rates of emergency department visits and hospitalizations due to opioid poisoning and opioid use disorder have also increased substantially from 2013 to 2017 in Canada.8,9
Given the greater prevalence of chronic pain in older adults, they may be more exposed to prescription opioids.10 Indeed, an increase in prescription opioid use, misuse, and overdose has been observed among older adults in the past 10 years in the US.10,11 Furthermore, in 2017, the rate of opioid poisoning hospitalizations was estimated at 16 cases per 100,000 in the general Canadian population, and around 18 per 100,000 population in individuals aged 65 or more.8
Patients suffering from traumatic injury (eg, vehicle accidents, falls, penetrating wounds) are often treated with opioid analgesics during the acute phase and some of them will develop long-term opioid use and/or chronic pain.12 Older trauma patients are at risk of long-term opioid use, especially if they have a history of preinjury or early postinjury opioid consumption.13 It has also been shown that a significant portion of older trauma patients (15.3%) will develop chronic pain 12 months following injury.14 Therefore, elderly trauma patients may be more at risk of opioid misuse.
Several opioid overdose or misuse risk factors have been identified in the chronic pain or trauma populations; male sex, younger age, comorbid medical or psychiatric conditions, opioid prescriptions used before and after trauma discharge, history of substance use disorder, and opioid overdose in the past 12 months.15–19 However, risk factors specific to older trauma patients have not been determined, and these could help health professionals choose more wisely those who will benefit from opioid treatment without major risk of opioid poisoning or opioid use disorder.
The primary objective of the study was to establish the incidence of opioid poisoning and opioid use disorder in an older trauma population. The secondary objectives were to identify risk factors of opioid poisoning or opioid use disorder in the same trauma population, particularly the association with opioid use during the acute phase after hospital discharge. We hypothesized that rates of opioid poisoning and opioid use disorder would be more likely to occur in older trauma patients that use opioids in the acute phase following injury.
Methods
Study Design and Population
We conducted a retrospective multicenter cohort study using medical consultations and medications from three governmental population databases (the Quebec Trauma Registry, the Maintenance et exploitation des données pour l’étude de la clientèle hospitalière [MED-ECHO] and the Régie de l’Assurance Maladie du Québec [RAMQ]). We selected patients 65 years and older admitted for injury in any of the 57 adult trauma centers (3 level I, 5 level II, 21 level III, and 28 level IV) in the province of Quebec (Canada) between January 1, 2004 and March 31, 2014. These patients are automatically covered by the RAMQ program for their health care and medications. However, a small proportion of older patients are covered by a private medication insurance and were excluded because their data were not available for our study.
Study Databases
The Quebec Trauma Registry was developed in 1993 and involves mandatory prospective data collection for patients admitted to any trauma center for an injury according to the following criteria: death following injury, hospital stay greater than 2 days, intensive care unit, or transfer from another hospital. Medical archivists extract registry data from patients’ medical files using standardized coding protocols. Anatomic injuries are coded with the Abbreviated Injury Scale (AIS) according to guidelines published by the Association for the Advancement of Automotive Medicine.20 The registry is centralized at the RAMQ of the Quebec Ministry of Health and is subject to periodic validation.
The RAMQ medical consultations and prescription medication database is an administrative database maintained by the Quebec Ministry of Health and contains diagnostic information of all medical consultations and medication prescriptions filled for every patient covered by the government RAMQ medication insurance in the province of Quebec, which represents 84% of our sample. Only patients with private insurance are not included in this database. The medication database contains the date of dispensation, common drug denominations, form, dosage, and quantity prescribed by physicians. The medical consultation database contains the date of visit and ICD-9 codes diagnosis.
MED-ECHO (Maintenance et exploitation des données pour l’étude de la clientèle hospitalière) is a medico administrative database managed by the Quebec Ministry of Health. It contains information on primary and secondary ICD-9 or ICD-10 code diagnoses and medical interventions for all hospitalizations in the province of Quebec.
The three databases were linked using unique anonymous identification numbers provided by the RAMQ. Access to these databases required the approval of the ethics review boards of the [Commission d’accès à l’information du Québec] and of the [Responsable de l’accès à l’information et de la protection des renseignements personnels de la RAMQ]. Patient information for the three databases was available for the time period ranging from 1-year before the trauma to 8 years after hospital discharge (maximum allowed).
Primary Outcomes
Opioid poisoning was searched for separately in the hospital discharge and physician billing databases (not hospitalized), since the former represent more severe episodes. Opioid poisoning codes retained for analysis were ICD-9 (965.00 or 965.80), or ICD-10 (T40.0, T40.1, T40.2, T40.3, T40.4, or T40.6). Opioid use disorder was searched for in the hospital discharge and physician billing databases and the codes retained were ICD-9 (304.00, 304.70 or 305.50), or ICD-10 (F11.0, F11.1, F11.2, F11.3, F11.4, F11.5, F11.6, F11.7, F11.8, or F11.9). For both outcomes, the diagnosis needed to be made after the index trauma.
We also searched in the prescription medication database for filled opioid prescriptions including codeine, hydromorphone, meperidine, oxycodone, methadone, fentanyl, tramadol, pentazocine, morphine and their combination with acetaminophen. Hydrocodone is not used for pain management in Canada. Opioid use during the acute phase was defined as filling at least one opioid prescription during the first 90 days after discharge of the index hospitalisation for injury.
Database Variables
From the three databases, we extracted the following: age, sex, injury mechanisms (fall, motor vehicle accident, penetrating injury, or other), injury severity score (ISS), abbreviated injury scale (AIS), number of injuries, length of emergency department and hospital stay, surgeries, intensive care unit (ICU) admission. A score greater than 15 on the ISS was used to define major trauma or multisystem trauma.21 The MED-ECHO and RAMQ medical consultation databases were used to identify patients who had an ICD-9 or ICD-10 code for depression, anxiety, alcohol use disorder, opioid prescriptions filled, substance use disorder, or opioid poisoning in the year before the target trauma.
Statistical Analyses
Since small differences can result in statistically significant results in very large populations, the characteristics of the included sample and those of patients who were excluded were compared using Cohen’s effect sizes.22 Small, medium, and large effect sizes for Chi-square and Mann–Whitney U-tests are 0.1, 0.3, and 0.5, respectively. Medium and higher effect sizes were considered clinically significant for these analyses. Associations between filling an opioid prescription during the acute phase after the trauma and opioid poisoning or opioid use disorder (controlling for other clinical characteristics) were evaluated using Cox proportional hazards regression analyses. Time to opioid poisoning or opioid use disorder was used as survival time and duration of follow-up (or time to death) was used for censored data. Hazard ratios (HR) were calculated with 95% confidence intervals. Alpha levels were set at 0.05, and all analyses were performed using SPSS version 25 (IBM, Somers, NY).
Results
Cohort Characteristics
The Quebec Trauma Registry included a total of 84,241 adult patients aged 65 and older admitted for a trauma between 2004 and 2014. Of these patients, 16.5% were excluded because they were not covered by the RAMQ medication insurance (data from patients with private insurance were not available), leaving 70,314 subjects for the final sample. Excluded patients were similar in all aspects to the selected sample (Table 1). In our cohort, the median age was 82 (IQR: 75–87) years and 68% were female. The most common mechanism of injury was falls (89%), 59% had surgery, median hospital stay was 12 days, and the median follow-up was 2.6 years (IQR: 1–5). The percentage of patients who filled an opioid prescription within 3 months after the target injury was 34.0% (95% CI: 33.6%-34.4%). Opioid use during the index hospitalization was not available.
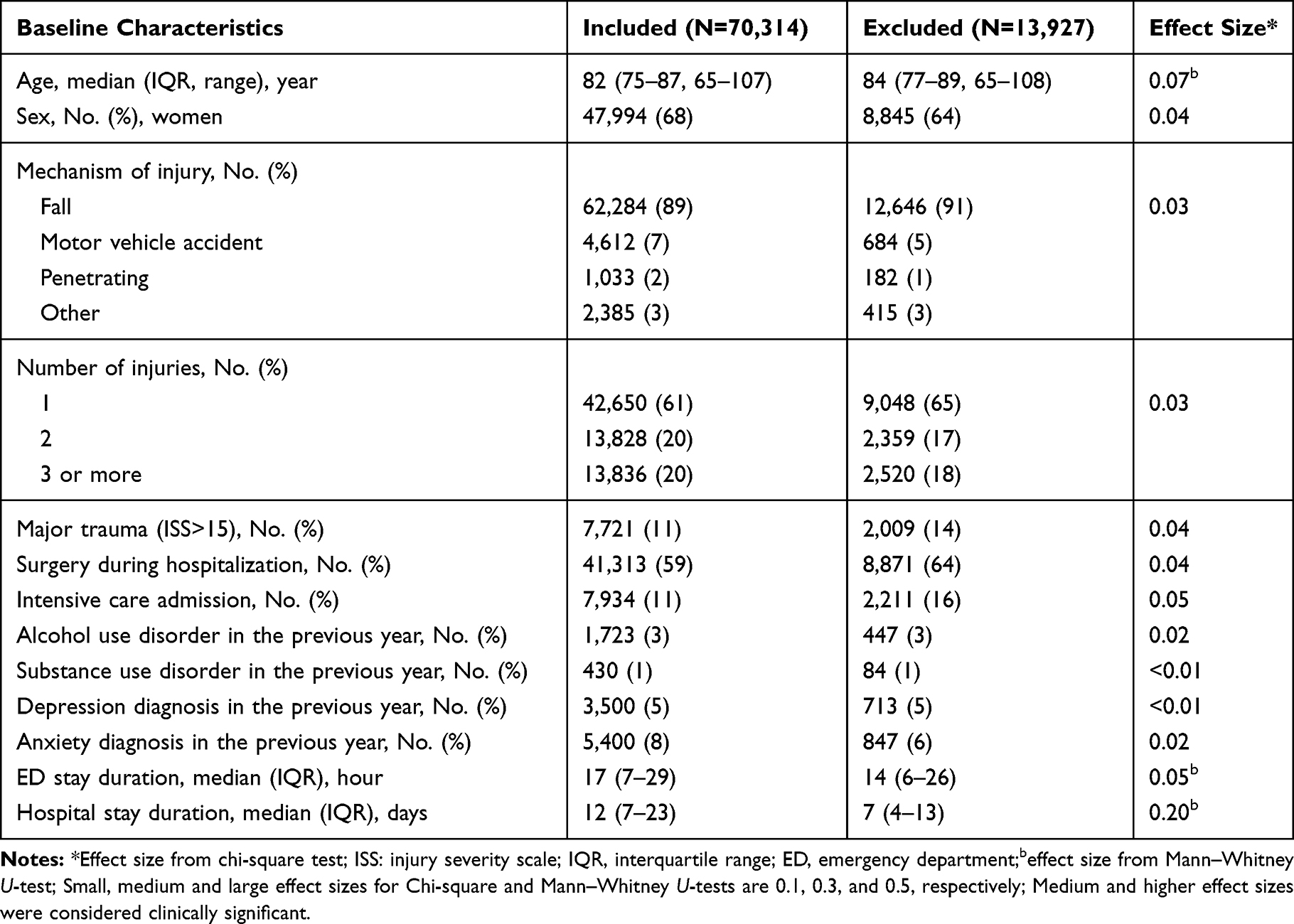 |
Table 1 Baseline Characteristics of Included and Excluded Patients |
Opioid Poisoning Following Injury
After a trauma-related hospitalisation, 207 (0.29%; 95% CI: 0.25%-0.33%) patients were diagnosed with opioid poisoning, 192 (0.27%) were hospitalized and only 15 (0.02%) patients had this diagnosis without hospitalization. The median time of occurrence of opioid poisoning was 15.3 months (IQR: 5.4–31.7). Table 2 shows the adjusted hazard ratios for patient characteristics of hospitalized opioid poisoning. We did not include opioid poisoning without hospitalization because they could be only minor side effects from opioids. Controlling for all other variables, being younger, having a substance abuse disorder diagnosis the year before the trauma, having an opioid prescription filled the year before the trauma, having opioid poisoning in the year before the trauma, having a longer follow-up and hospital stay, and having filled an opioid prescription within 3 months after the injury were all significantly associated with opioid poisoning. Notably, patients who filled an opioid prescription within 3 months after the injury were 2.8 (95% CI: 2.1–3.8) times more likely to suffer from opioid poisoning. Opioid poisoning in the year before trauma (2.7; 95% CI: 1.1–7.4), substance use disorder the year before trauma (3.1; 95% CI: 1.4–7.3), and opioid prescription filled in the year before trauma (2.4; 95% CI: 1.8–3.3) were also associated to opioid poisoning with similar strength.
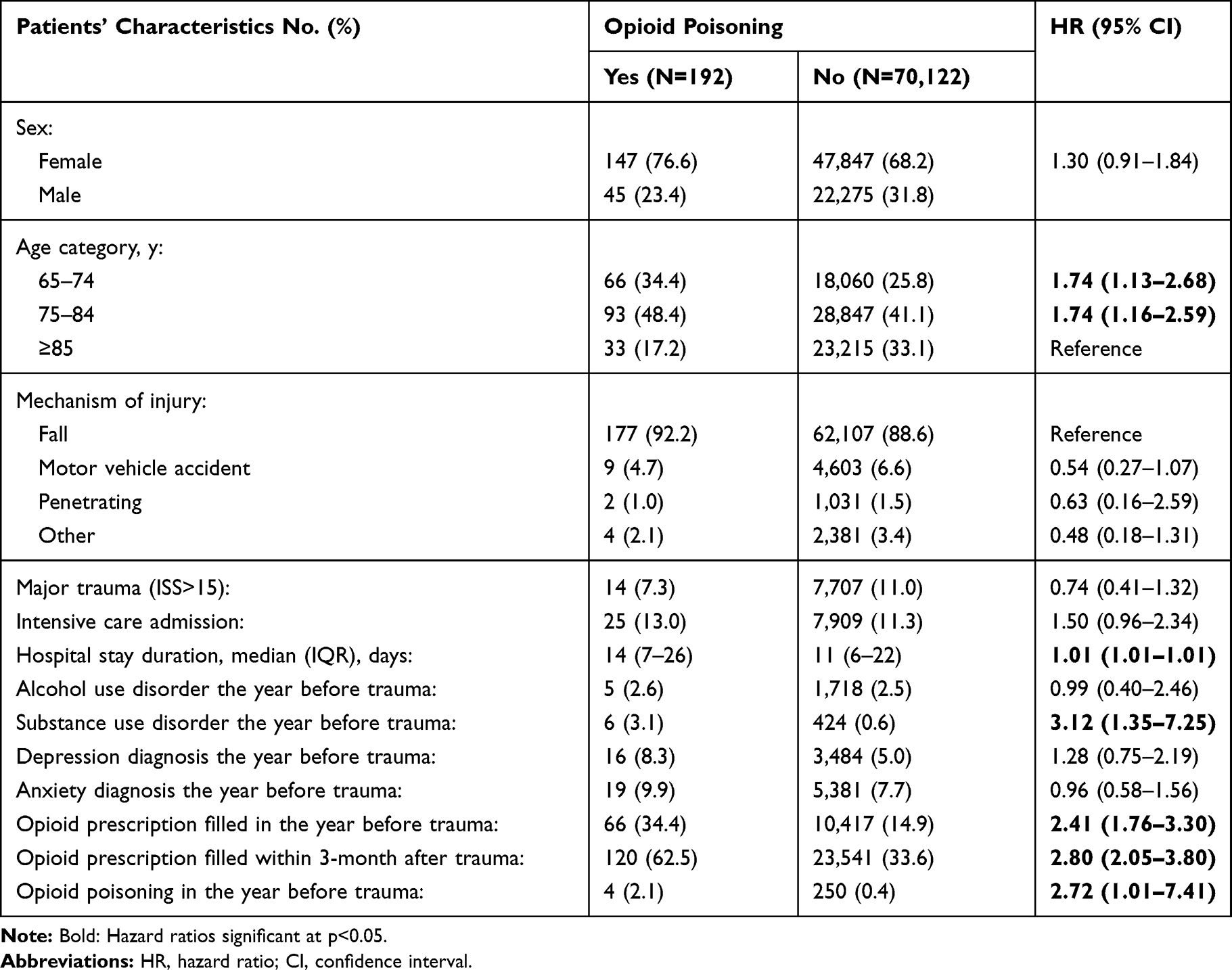 |
Table 2 Associations Between Patients’ Characteristics and Opioid Poisoning Hospitalization |
Opioid Use Disorder Following Injury
During the follow-up, only 73 participants (0.10%; 95% CI: 0.07%-0.13%) were diagnosed with opioid use disorder. The median time of occurrence of opioid use disorder was 17.3 months (IQR: 4.4–38.2). Table 3 shows the adjusted hazard ratios of opioid use disorder for patient characteristics. Controlling for all other variables, having substance abuse disorder diagnosis the year before the trauma, having an opioid prescription filled the year before the trauma, having a longer follow-up, and having filled an opioid prescription within 3 months after the injury were all significantly associated with opioid use disorder. Particularly, patients who filled an opioid prescription within 3 months after the injury were 4.0 (95% CI: 2.5–6.6) times more likely to have suffered from opioid use disorder after the injury. Again, substance use disorder the year before trauma (7.1; 95% CI: 3.1–16.5), and opioid prescription filled in the year before trauma (4.0; 95% CI: 2.5–6.6) were also highly related to opioid use disorder after the injury.
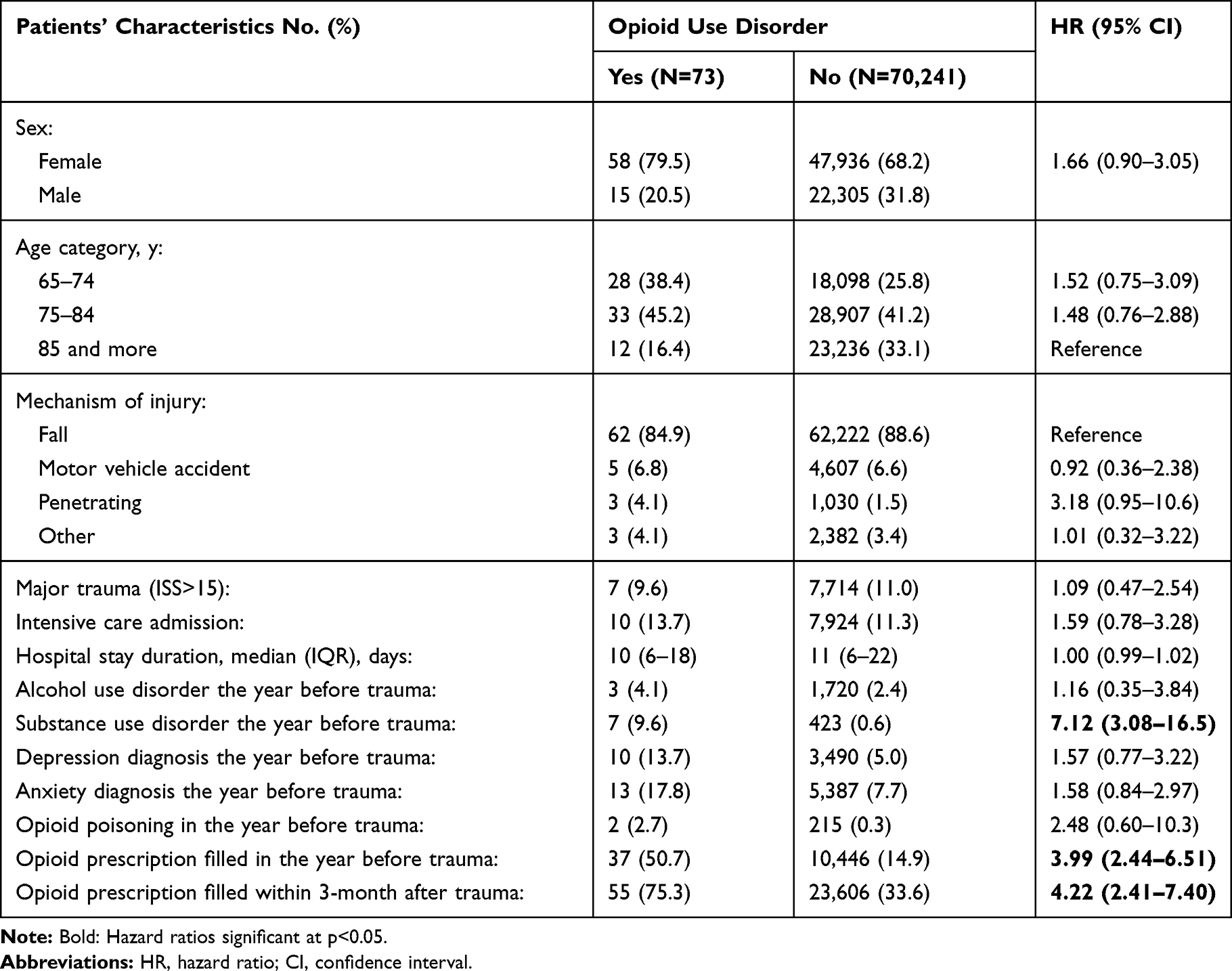 |
Table 3 Associations Between Patients’ Characteristics and Opioid Use Disorder |
Opioid Poisoning or Opioid Use Disorder Following Injury
A total of 273 (0.4%; 95% CI: 0.35%-0.45%) patients suffered from opioid poisoning or opioid use disorder during the follow-up and, after controlling for the other variables, patients who filled an opioid prescription within 3 months after the injury were 3.2 (95% CI: 2.4–4.2) times more likely to have suffered from one or both disorders after the injury. Again, opioid poisoning in the year before trauma (2.8; 95% CI: 2.2–3.6), substance use disorder the year before trauma (4.3; 95% CI: 2.4–7.7), and opioid prescription filled in the year before trauma (2.8; 95% CI: 2.2–3.6) were also associated with opioid poisoning or opioid use disorder after the injury. Only seven patients suffered from both opioid poisoning and opioid use disorder.
Discussion
Even though one third of the older patients included in the trauma registry had filled at least one opioid prescription in the acute period after trauma, the incidence of opioid poisoning and opioid use disorder remained low during the 2.6-year follow-up. Nevertheless, this study confirms an association between acute phase opioid use and future opioid poisoning or opioid use disorder in the older trauma population. History of opioid poisoning, substance use disorder, or opioid prescriptions filled the year before trauma demonstrated similar associations.
The rate of opioid poisoning hospitalization (105 cases per 100,000/year) is substantially higher than that observed in the Canadian general older population (18 per 100,000/year in 2017),8 but similar to the one reported in a US study on a registry of 400,000 individuals who filled at least one opioid prescription (0.3%).7 Therefore, the fact that our older population used opioids because of their injury further increased the risk of opioid poisoning compared to a Canadian general older population.
The rate of opioid use disorder observed in our data (0.1%) is substantially lower than that reported in a US national survey of the general population in 2015 (0.8%).5 However, the population and study design are different in both studies and the opioid crisis is greater in the US than in Canada (especially in the Quebec province). However, the rate of opioid poisoning or opioid use disorder observed in our cohort (15 cases per 10,000 persons/y) is similar to that reported in a study on US older patients in 2014 (15 cases per 10,000 persons).11
The risk factors for opioid poisoning or opioid use disorder identified in our older trauma population are generally the same as those reported in other studies.15–19 Acute opioid prescription filling after trauma was related to opioid poisoning but a history of substance use disorders, previous opioid use, and history of opioid poisoning also contributed to the prediction of opioid poisoning. Our results also showed that younger patients (<84 y.o.) had a higher incidence of opioid poisoning than the oldest group (≥85 y.o.). This is in line with other studies reporting that younger individuals (<40 y.o.) are more prone to opioid overdose compared to patients aged 65 and older.7,11,19
Risk factors for opioid use disorder were slightly different than those observed in opioid poisoning; no age effect was detected. However, substance use disorder in the previous year was the most important predictor of an opioid use disorder, as reported in other studies.15–19 Since only seven patients were diagnosed with opioid poisoning and opioid use disorder, we could hypothesise that most opioid poisonings are accidental.
In recent years, the mainstream in pain management be it for chronic or acute conditions, is to avoid opioid use as much as possible. However, opioids remain an important treatment for acute, severe pain.23 In February 2018, the International Association for the Study of Pain strongly advocates for access to opioids for the humane treatment of severe short-lived pain, using reasonable precaution to avoid misuse, diversion, and other adverse outcomes.24 In our cohort of older trauma patients, we observed an association between acute opioid use after a trauma and opioid poisoning or opioid use disorder. However, the median delay of occurrence of opioid poisoning was 15 months after the target trauma and the incidence of opioid poisoning or opioid use disorder was low (0.4%) and associated with a history of substance abuse disorder or previous opioid use. The low level of opioid misuse observed justifies the use of opioids in older trauma population suffering from acute pain. However, it is therefore preferable to use opioids during the acute phase after trauma more cautiously in older patients with a history of substance use disorder, opioid poisoning or opioid use during the past year.
Our study captured a very large cohort of older patients from a robust registry that includes the vast majority of trauma cases of the province of Quebec using validated and objective inclusion criteria over a period of 10 years. Since every resident of the province is covered by free universal health insurance, our study includes all medical consultations and hospitalizations diagnoses. It also contains all prescription medications filled for the study period for patients that were covered by the RAMQ medication insurance plan (a small proportion were not covered and were excluded). The exhaustive information on the health care services received in this cohort allowed the determination of precise and accurate rates and risk factors of opioid poisoning and opioid use disorder, which constitutes the major strength of our study.
Study Limitations
Pain medications administered during the target trauma hospitalization were not available and therefore could not be considered in the present study. Analgesics available without a prescription were not in the database and could have influenced how opioids were consumed. Also, patients could have filled their opioid prescriptions but not consumed them. As well, it is possible that opioid use disorder is underreported in these databases. The advanced age of the participants may limit the duration of the follow-up for an important part of the cohort. Reports of alcoholism, substance abuse disorder, depression, anxiety, prescription opioid filling, and opioid poisoning were limited to the year preceding the target injury. Therefore, the association of these conditions and opioid consumed with opioid poisoning or opioid use disorder could have been underestimated. Some opioid prescription guidelines (acute and chronic) were published after our data were obtained and could possibly affect the rates of opioid misuse in the future. However, this should not affect the risk factors of opioid poisoning or opioid use disorder after trauma.
Conclusions
In summary, opioid poisoning and opioid use disorder are relatively rare events in the older trauma population, including patients who were prescribed opioids after hospitalization for injury. This supports the use of opioids in older trauma population suffering from acute pain. It also suggests that opioids should be used cautiously in older patients with a history of substance use disorder, opioid poisoning or opioid use.
Acknowledgments
The authors want to thank Jeanne Teitelbaum and Martin Marquis for their contributions to the revision of the manuscript. We also thank Manon Choinière for her contribution to the designing of this study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hasegawa K, Espinola JA, Brown DF, Camargo CA
2. CDC. Opioid overdoses in the United States. J Pain Palliat Care Pharmacother. 2012;26(1):44–47. doi:10.3109/15360288.2011.653875
3. Dhalla IA, Mamdani MM, Sivilotti ML, Kopp A, Qureshi O, Juurlink DN. Prescribing of opioid analgesics and related mortality before and after the introduction of long-acting oxycodone. CMAJ. 2009;181(12):891–896. doi:10.1503/cmaj.090784
4. Fischer B, Argento E. Prescription opioid related misuse, harms, diversion and interventions in Canada: a review. Pain Physician. 2012;15(3 Suppl):Es191–203.
5. Han B, Compton WM, Blanco C, Crane E, Lee J, Jones CM. Prescription opioid use misuse, and use disorders in U.S. adults: 2015 national survey on drug use and health. Ann Intern Med. 2017;167(5):293–301. doi:10.7326/M17-0865
6. Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, van der Goes DN. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569–576. doi:10.1097/01.j.pain.0000460357.01998.f1
7. Campbell CI, Bahorik AL, VanVeldhuisen P, Weisner C, Rubinstein AL, Ray GT. Use of a prescription opioid registry to examine opioid misuse and overdose in an integrated health system. Prev Med. 2018;110:31–37. doi:10.1016/j.ypmed.2018.01.019
8. Canadian Institute for Health Information. Opioid-Related Harms in Canada, December 2018. Ottawa, ON: CIHI; 2018.
9. Ontario Agency for Health Protection and Promotion (Public Health Ontario); Leece P. Evidence Brief: Mortality Following Non-Fatal Opioid Overdose. Toronto, ON: Queen’s Printer for Ontario; 2017.
10. West NA, Severtson SG, Green JL, Dart RC. Trends in abuse and misuse of prescription opioids among older adults. Drug Alcohol Depend. 2015;149:117–121. doi:10.1016/j.drugalcdep.2015.01.027
11. Wei YJ, Chen C, Schmidt SO, LoCiganic WH, Winterstein AG. Trends in prior receipt of prescription opioid or adjuvant analgesics among patients with incident opioid use disorder or opioid-related overdose from 2006 to 2016. Drug Alcohol Depend. 2019;204:107600. doi:10.1016/j.drugalcdep.2019.107600
12. Berube M, Choiniere M, Laflamme YG, Gelinas C. Acute to chronic pain transition in extremity trauma: A narrative review for future preventive interventions (part 1). Int J Orthop Trauma Nurs. 2016;23:47–59. doi:10.1016/j.ijotn.2016.04.002
13. Daoust R, Paquet J, Moore L, et al. Incidence and risk factors of long-term opioid use in elderly trauma patients. Ann Surg. 2018;268(6):985–991. doi:10.1097/SLA.0000000000002461
14. Daoust R, Paquet J, Moore L, et al. Early factors associated with the development of chronic pain in trauma patients. Pain Res Manag. 2018;2018:7203218. doi:10.1155/2018/7203218
15. Baird J, Faul M, Green TC, et al. A retrospective review of unintentional opioid overdose risk and mitigating factors among acutely injured trauma patients. Drug Alcohol Depend. 2017;178:130–135. doi:10.1016/j.drugalcdep.2017.04.030
16. Sullivan MD, Edlund MJ, Fan MY, Devries A, Brennan Braden J, Martin BC. Risks for possible and probable opioid misuse among recipients of chronic opioid therapy in commercial and medicaid insurance plans: the TROUP Study. Pain. 2010;150(2):332–339. doi:10.1016/j.pain.2010.05.020
17. White AG, Birnbaum HG, Schiller M, Tang J, Katz NP. Analytic models to identify patients at risk for prescription opioid abuse. Am J Manag Care. 2009;15(12):897–906.
18. Webster LR. Risk factors for opioid-use disorder and overdose. Anesth Analg. 2017;125(5):1741–1748. doi:10.1213/ANE.0000000000002496
19. Cragg A, Hau JP, Woo SA, et al. Risk factors for misuse of prescribed opioids: a systematic review and meta-analysis. Ann Emerg Med. 2019;74(5):634–646. doi:10.1016/j.annemergmed.2019.04.019
20. Association for the Advancement of Automotive Medecine. Abbreviated Injury Scale (AIS). Illinois: AAAM Publications; 1990.
21. Copes WS, Champion HR, Sacco WJ, Lawnick MM, Keast SL, Bain LW. The injury severity score revisited. J Trauma. 1988;28(1):69–77. doi:10.1097/00005373-198801000-00010
22. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
23. Shipton EA, Shipton EE, Shipton AJ. A review of the opioid epidemic: what do we do about it? Pain Ther. 2018;7(1):23–36. doi:10.1007/s40122-018-0096-7
24. International Association for the Study of Pain. IASP statement on opioids; 2018. Available from: https://www.iasp-pain.org/Advocacy/Content.aspx?ItemNumber=7194.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.