")
Back to Journals » International Medical Case Reports Journal » Volume 15
Open Surgical Repair of Traumatic Subclavian Artery Pseudoaneurysm: A Case Report
Authors Almadwahi N, Halboob E
Received 7 September 2022
Accepted for publication 17 November 2022
Published 24 November 2022 Volume 2022:15 Pages 671—675
DOI https://doi.org/10.2147/IMCRJ.S388186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ronald Prineas
Nabeel Almadwahi,1,2 Emad Halboob1
1Department of Vascular Surgery, Al-Thawra Modern General Hospital, Sana’a, Yemen; 2Faculty of Medicine and Health Sciences, Sana’a University, Sana’a, Yemen
Correspondence: Nabeel Almadwahi, Department of vascular surgery, Al-Thawra Modern General Hospital, Faculty of Medicine and Health Sciences, Sana’a University, Sana’a, Yemen, Tel +967770983231, Email [email protected]
Abstract: Penetrating trauma involving the subclavian vessels is rare but associated with life- threatening sequelae, including hemomediastinum, formation of pseudoaneurysm and limb ischemia. Conventional open surgery and endovascular repairs are effective treatment modalities for subclavian-related injuries, but the latter has become more attractive owing to being less invasive and less procedure-related complications. We report a case with left subclavian artery pseudoaneurysm secondary to a bomb blast. The patient was successfully treated by surgical repairs using a combination of supra- and infraclavicular approaches. The patient recovered completely and discharged home on the third day. In a resource-limited setting, traditional surgical repair is an effective therapy for posttraumatic pseudoaneurysm, especially when the adjacent organs are compressed by the pseudoaneurysm. Vascular injury should be suspected once a patient presents with localized pulsatile mass in the clavicular region following roadside bomb blasts injuries.
Keywords: subclavian artery, pseudoaneurysm, open surgery repair, aneurysm
Background
Traumatic subclavian artery pseudoaneurysm is rare and only account for 1–2% of all vascular injuries but mortality is still high due to the risk of rupture, thrombosis and thromboembolism if the pseudoaneurysm is left untreated.1 Apart from iatrogenic etiology, penetrating trauma including gunshot, and bomb blast injuries are the leading cause of subclavian artery pseudoaneurysm.2–4 According to systematic review, traumatic pseudoaneurysm represented the most common type of aneurysm which attributed to different mode of injuries, including iatrogenic trauma, fall from height, motor-vehicle accident, stabbin, gunshot and other non-specified types.7
Treatment options for subclavian artery pseudoaneurysm have evolved from traditional open surgical interventions to minimally invasive endovascular repairs. However, surgical intervention remains a vital choice in a resource-limited country despite the presence of critical nerves and bony thoracic structures that restrict and slow exposure.5,6 Herein, we report case of an adolescent male with a left subclavian artery pseudoaneurysm, which was formed weeks after a bomb blast injury and was successfully managed by combined infra- and supraclavicular surgical repairs.
Informed Consent
Written informed consent was provided by the patient’s father to have the case details and the accompanying images published. Institutional approval for publishing this case report was not required.
Case Presentation
A 17-year-old previously healthy male patient attended to the vascular clinic of Al-Thawra Modern General Hospital with neck mass six weeks prior to admission, as a victim of roadside bomb blast with wound to the left supraclavicular region at the parasternal line (Figure 1A). The mass started to progress gradually just from the second day after the bomb blast, and by days it turned visible to the naked eyes. The patient did not seek any medical advice for any other illness or trauma-related complications until the 6th week post bomb blast when he started to complain of mass-related implausible heaviness in the left shoulder associated with numbness and tingling sensation that extend to include the whole left upper limb secondary to brachial compression by the large mass. The pain interfered with daily activities leading to limitation of limb movements but regaining the function temporary by analgesics. Patient did not complain of any other symptoms like dysphagia, syncopal attack, or dyspnea. He had no past history of any medical or surgical diseases. He is living in Saada Governorate which takes 5 hours to reach to Sana’a, the capital of Yemen.
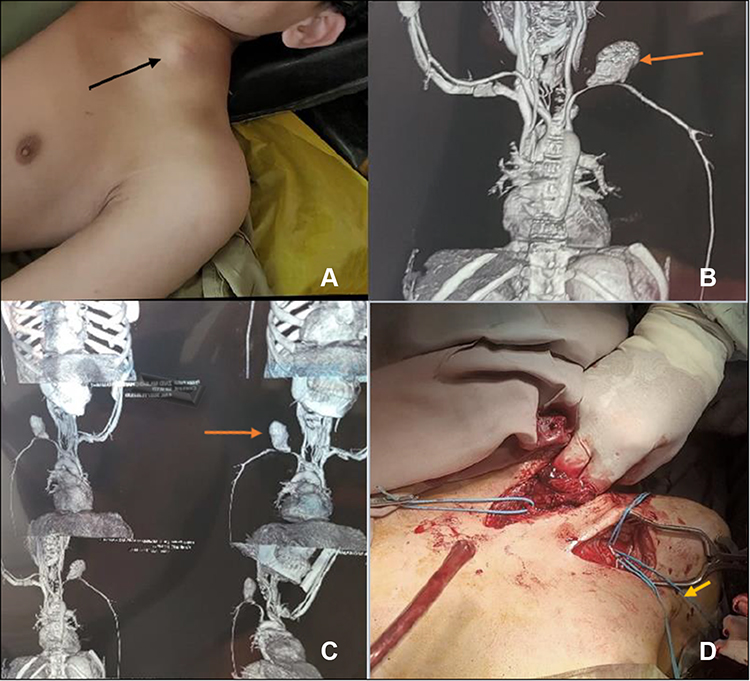 |
Figure 1 (A) Shows a mass located on the left supraclavicular region at the parasternal line; (B and C) CT angiography shows the left subclavian pseudoaneurysm (arrow) as a large supraclavicular clotted hematoma of about 8.4×7.2 cm on the origin of the left subclavian artery just beyond the origin of the left common carotid artery; (D) shows insertion of a size 5 Fogarty catheter (arrow) through the axillary artery to the origin of the left subclavian artery. |
On examination, patient was conscious, oriented, cooperative, alert, patent airway, spontaneous breathing, afebrile, no jaundice, no pallor, no lower limb edema. The pulses were equally detected in the lower limbs, but diminished in the left upper limb compared to the contralateral limb. Physical examination also revealed a healed wound scar with a diameter of 0.5×0.3 mm on the top of a pulsatile, compressible, but not hot or movable oval mass with a diameter of 5×7 cm extended from the left med supraclavicular area to the root of the anterolateral aspect of the neck. The pulsatile mass was associated with tenderness but no skin discoloration pointing to a circulatory disorder. Chest computed tomography angiography revealed a large pseudoaneurysm (8.4 x 7.2 cm) originated from the middle part of the subclavian artery (Figure 1B and C). There was no hemothorax or pneumothorax in the affected side. There were no other associated injuries nearby or far away from the site of injury. No foreign body was seen during imaging nor during hematoma evacuation.
Treatment
Since the pseudoaneurysm was large and the patient had symptoms that were related to its compression to the adjacent brachial plexus nerve, surgical repairs through two approaches were carried out after obtaining a written informed consent from the father. The first approach was performed in order to obtain proximal and distal control (Figure 1D). Proximal control of the left subclavian artery was obtained by insertion of a size 5 Fogarty catheter (FC5) using the infraclavicular approach through a healthy distance-away from the site of injury over the left axillary artery. The catheter was inserted retrogradely to be inflated in the origin of the left subclavian artery; likewise, distal control was obtained by using vascular clamp distal to the site of injury over the axillary artery too. The second approach was carried out via supraclavicular incision to expose the first part of the subclavian artery and remove the hematoma and to make primary repair of the injured artery without effect on the nearby structures (Figure 2A). After removing the hematoma, an injury of 4 mm size with active bleeding was identified on the wall of the subclavian artery (Figure 2B) for which polypropylene suture (proleneTM 6–0) was utilized to repair the injury and vacuum drain was installed. After good hemostasis, infra- and supraclavicular incisions were closed as layers, Vicryl (polyglactin 910, Ethicon, Inc.) for both fascia and subcutaneous tissue and stapler for the skin (Figure 2C). The patient did not suffer from any serious complication during any phase of the surgery, and he was transferred for one day to ICU for close monitoring and observation during heparin infusion. On the second day, the patient was transferred to the male surgical ward and discharged home on the third day of operation after removing the drain and Foley’s catheter. Patient’s neurovascular status revealed normal sensory and motor functions, and the pulses were detected distally. Follow up visits to the clinic were scheduled along with advice of not holding heavy objects, especially by the affected limb. Since the patient travelled to a far rural area, follow up was obtained via telephone when possible, no ultrasound was done. The last follow up was obtained 3 months after discharge (Figure 2D).
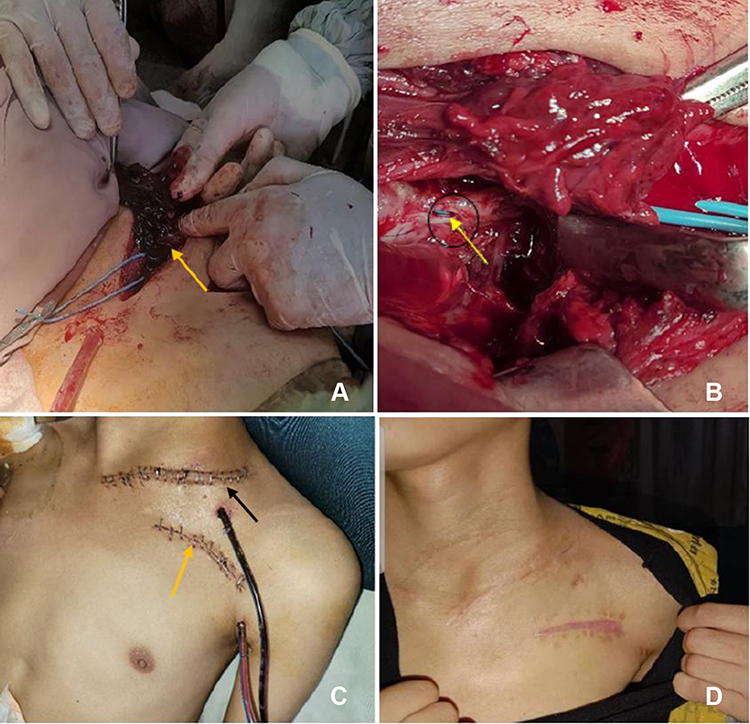 |
Figure 2 (A) Shows evacuation of a big hematoma (arrow); (B) shows a 4 mm injury in the wall of the artery (circle), the Fogarty catheter (arrow) appear through the injury; (C) shows, the supra (black arrow) and infraclavicular (Orange arrow) approaches’ incisions with vacuum drain installed; (D) last follow up (3 months after discharge). |
Discussion
Pseudoaneurysm is a hematoma resulted from leakage of blood following a breach in the arterial wall. Traumatic injuries are the leading cause of pseudoaneurysm.5,7 The most common site of penetrating artery pseudoaneurysm is the common femoral artery, followed by radial and brachial arteries, but subclavian artery is extremely rare because it is well protected by the clavicle thus a significant mechanism is required to cause injury.8,9
In all patients with traumatic injuries, a detailed history and physical examination are the key points to reach the mechanism of subclavian injury. Subclavian pseudoaneurysm should be suspected in posttraumatic injuries in a patient who presents with pulsatile mass in the clavicular region. Once the clinician suspects pseudoaneurysm, CT angiography is needed to confirm the diagnosis. CT angiography is a gold diagnostic technique as it provides more details about arterial injuries and useful information regarding the site and size of the pseudoaneurysm and the relationship to surrounding structures. Delaying the decision for immediate evaluation could lead to possible serious consequence which in turn might completely exchange the surgeon options and make the guaranteed surgery a challenging one. To clarify this, as the orifice of the subclavian artery becomes fragile and dilated and/or infected, the outcomes of reconstruction by either primary anastomosis or direct closure of the artery with patch graft will be questionable.
Evidence showed that traumatic subclavian pseudoaneurysm may be symptomatic or asymptomatic.6 The pulsatile mass in the subclavian region has been reported as the most common presentation, which appears 2–12 weeks after the primary injury.5,10 In the present case, the patient presented with a roadside bomb blast injury to the left subclavian artery. These types of injuries are frequently encountered in regions that suffer from long-term instability and conflict.5 The patient in this case initially had no symptoms, and thus he did not seek any healthcare facility, but later it became symptomatic. Our patient was complaining of pulsatile mass that was growing with each passing day and lately felt of heaviness and tingling that hindered daily activities. These symptoms might be related to the large size of the subclavian pseudoaneurysm which compressed the adjacent nerve leading to neurologic pain as reported by the patient.
Choosing a treatment option for subclavian pseudoaneurysm depends on several factors including endovascular-capable facility, patients’ affordability, expertise, size and location of the pseudoaneurysm.5,11 In a patient with large subclavian pseudoaneurysm when long-term follow-up is difficult, open surgical repair is a reasonable option.12 In our case, the patient had a large pseudoaneurysm and lived in a rural area approximately 5-hour far from an equipped hospital, making periodic follow-up very difficult. Therefore, a combined infra- and supraclavicular approach was the primary method for the successful treatment in this case. Moreover, in resource-limited countries, non-affordability is highlighted as the main reason behind choosing the traditional surgical intervention instead of endovascular repairs.3,5,13 In our country, due to the political conflicts and decades of continued war, the majority of patients are unable to afford the large expense of endovascular techniques, making surgical intervention an excellent choice. Furthermore, endoleak is a prominent complication that occurs after endovascular repair which necessitates periodic follow-up and another intervention may require if this complication occurs,7 although this complication may occur after surgical repairs, the exact prevalence among patients with subclavian pseudoaneurysm is unknown. These issues make the surgical option more favorable for the patient and surgeon. Although this type of intervention is associated with complications, such as bleeding, infection, and losing the limb function, it is less invasive and less procedure-related complications compared with trap-door approach.14 Despite that, trap-door approach may be a reasonable option when more exposure is needed to save patients’ life or when the Fogarty catheter is not available to obtain proximal control.15
Conclusion
Traumatic vascular injury should be suspected in a patient after a bomb blast accident and the subclavian pseudoaneurysm is highly suspected when the patient presents with either symptomatic or asymptomatic pulsatile mass located the clavicular region. Traditional surgical repair of subclavian pseudoaneurysm using supra- and infraclavicular approaches is an effective treatment modality and remains the first choice in resource-limited countries, especially when the patient presents with symptoms-related to a large pseudoaneurysm.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Grigorian A, Wilson SE, de Virgilio C, et al. Humerus fracture and combined venous injury increases limb loss in axillary or subclavian artery injury. Vascular. 2019;27(3):252–259. PMID: 30426848. doi:10.1177/1708538118811231
2. Serrano JA, Rodríguez P, Castro L, Serrano P, Carpintero P. Acute subclavian artery pseudoaneurysm after closed fracture of the clavicle. Acta Orthop belg. 2003;69(6):555–557. PMID: 14748115.
3. Malik A, Shah SMA, Waseem N, et al. Association of aetiology, presentation and post-operative complications of post-traumatic peripheral artery pseudoaneurysm. J Postgrad Med Instit. 2009;23(4):363–368.
4. Champion HR, Holcomb JB, Young LA. Injuries from explosions: physics, biophysics, pathology, and required research focus. JTrauma. 2009;66(5):1468–1477. doi:10.1097/TA.0b013e3181a27e7f
5. Yousuf KM, Khan FH. Pseudoaneurysm of head and neck vessels has been frequently observed in road side bomb blast victims. Surgeon. 2016;14(3):142–146. doi:10.1016/j.surge.2014.09.004
6. Naz I, Zia-Ur-Rehman AM, Sophie Z, Sophie Z. Subclavian artery aneurysms: management implications in a resource-limited setting. Vascular. 2012;20(6):301–305. doi:10.1258/vasc.2011.oa0307
7. Maskanakis A, Patelis N, Moris D, et al. Stenting of subclavian artery true and false aneurysms: a systematic review. Ann Vas Surg. 2018;47:291–304. doi:10.1016/j.avsg.2017.08.013
8. Smith AA, Gupta N. Subclavian artery trauma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. PMID: 32119358.
9. Koza Y, Kaya U. Retrospective analysis of 120 cases of iatrogenic and traumatic peripheral arterial pseudoaneurysms. Eurasian J Med. 2020;52(2):180. doi:10.5152/eurasianjmed.2019.18422
10. Saydam O, Şerefli D, Atay M, Sert C. Endovascular management of right subclavian artery pseudoaneurysm due to war injury in adolescent patient. Case Rep Vasc Med. 2017;2017:9030457. doi:10.1155/2017/9030457
11. Atay M, Saydam O, Açıkgöz B, Türkyılmaz S. Hybrid procedure of a subclavian artery pseudoaneurysm by shrapnel injury: a case report. Turk J Vasc Surg. 2021;30(1):60–62. doi:10.9739/tjvs.2021.004
12. Lee KS, Jung Y, Jeong IS, Song SY, Na KJ, Oh SG. Open surgical treatment of subclavian artery pseudoaneurysm after endovascular repair: a case report. J Cardiothorac Surg. 2022;17(1):1–4. PMID: 35219322. doi:10.1186/s13019-022-01775-0
13. Amirjamshidi A, Abbassioun K, Rahmat H. Traumatic aneurysms and arteriovenous fistulas of the extracranial vessels in war injuries. Surg Neurol. 2000;53(2):136–145. doi:10.1016/s0090-3019(99)00181-0
14. Demetriades D, Chahwan S, Gomez H, et al. Penetrating injuries to the subclavian and axillary vessels. J Am Coll Surg. 1999;188(3):290–295. PMID: 10065818. doi:10.1016/s1072-7515(98)00289-0
15. Fabregues Olea A, Zarain Obrador L, Perez-Diaz D, Turégano Fuentes F. Trap-door incision for penetrating thoracic trauma: an obsolete approach? Case Rep Surg. 2014;2014:798242. PMID: 25165611; PMCID: PMC4137611. doi:10.1155/2014/798242
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.