")
Back to Journals » Patient Preference and Adherence » Volume 13
Oncologists’ perspectives on adherence/non-adherence to adjuvant endocrine therapy and management strategies in women with breast cancer
Authors Eraso Y
Received 12 April 2019
Accepted for publication 21 June 2019
Published 31 July 2019 Volume 2019:13 Pages 1311—1323
DOI https://doi.org/10.2147/PPA.S211939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yolanda Eraso
School of Social Professions, London Metropolitan University, London, UK
Purpose: Adherence to adjuvant endocrine therapy (AET) is suboptimal, and a range of variables have been explored for understanding patients’ experiences and motivations for medication-taking. However, oncologists’ views on adherence are poorly understood. The aim of this study was to explore oncologists’ perspectives on adherence/non-adherence and their strategies to ensure patients continue with treatments to inform the development of potential modifiable interventions.
Methods: A qualitative study using in-depth, semi-structured interviews with 16 oncologists was conducted in Argentina. A stratified purposive sampling was used to recruit female and male participants from 3 health subsystems (private, social security, and public). Data were analyzed using the Framework approach.
Results: Oncologists believed patients’ adherence was overall high and associated it with good tolerance of AET in comparison to chemotherapy, information provided, and patients feeling reassured (fear of recurrence). Non-adherence was not perceived as a major source of concern, and it was related to rare cases of severe side effects, young age, refusing treatment, losing the insurance plan, lack of education, and social circumstances. Patients’ complaints of bothersome side effects were not identified as a main reason to discontinuation. Public and private sector patients, however, were perceived as having different attitudes toward side effects. Management strategies included medicine change, referral to support services, and a supportive relationship with the oncologist.
Conclusion: Oncologists’ perspectives on adherence/non-adherence to AET show similarities and significant differences with those in the literature based on patient-reported factors. Overall adherence was considered high, but the likelihood of unintentional non-adherence seems important in public sector patients. Information to patients should provide clear explanations on both severe and unpleasant side effects. Interventions to improve communication skills in oncologists and specialists responsible for survivorship care should be considered to strengthen patients’ self-efficacy and effective medication-taking. Reliable data on adherence are needed.
Keywords: female cancer, hormonal therapy, medication-taking, professional perspectives, health system provider, follow-up care
Introduction
Adherence to adjuvant endocrine therapy (AET) in clinical practice is considered as suboptimal in developed countries, with a systematic review study indicating a continued decline between the first and fifth year of treatment,1 and a meta-regression analysis estimating only a 53% of the adherers to 5 years of treatment.2 In addition, some studies differentiate between adherence and persistence, the former indicating “a measure of how well the patient takes the medication compared with the instructions given by the clinician, which is daily for endocrine therapy” (p. 1516),3 and the latter as completion of treatment over a 5-year course. The study by Makubate et al3 first demonstrated that only patients with high annual adherence (taking no less than 80% of the medication given) had better survival rates than those who took medication for 3 years or less.
According to WHO, developing countries are considered to have a lower percentage of medication adherence in chronic diseases in comparison to the 50% average estimated for developed countries.4 In South America, only a handful of small sample studies have analyzed adherence to hormonal therapy for breast cancer (BC).5–8 A recent quantitative study in Rio de Janeiro (Brazil), based on a large sample, reported a high rate (69%) of women being non-persistent with 5-year treatment, measured as interrupting or abandoning treatment for 60+days.9 Argentina has the highest age-standardized incidence (73×100.000) and the second highest mortality rate (18×100.000) from BC in South America,10 which makes it a relevant country to explore in terms of adherence given its association to mortality and recurrence; however, relevant data on AET adherence are missing.
Non-adherence to medication in chronic conditions is multifaceted including societal, medical, and individual factors: social and economic factors; the health care team and system; the characteristics of the disease; disease therapies and patient-related factors.4 Despite this range of influences, most quantitative and qualitative studies on AET have primarily concentrated on patients’ behaviors and beliefs while seeking to explore reasons for continuation and discontinuation of treatments. Recent AET literature11,12 has drawn attention to a necessary distinction between patients’ intentional adherence (a conscious decision of not taking medication) and unintentional adherence (individual and environmental limitations that prevent taking medication as prescribed).13 The “necessity-concern” model14 has been instrumental in analyzing medication beliefs in BC explaining that patients weigh up perceptions about the importance they attribute to a drug in preventing disease recurrence against concerns with bothersome side effects. AET is a standard treatment for women with estrogen-positive BC (stages I–IV) and have proven to be effective in reducing the risk of recurrence and in extending survival from the disease: in postmenopausal women, 5 years of the anti-estrogen drug Tamoxifen (TAM) reduces the risk of recurrence by about a half and mortality by about 30%, and aromatase inhibitors (AIs) such as anastrozole and letrozole reduce recurrence by about two-thirds and mortality rate by around 40%, during 10 years after initiation of treatment.47,48 TAM and AIs, however, have a number of significant adverse effects. Common side effects to TAM are hot flushes, depression, weight gain, and low libido, and less common but severe conditions such as increased risk of venous thromboembolism and endometrial disorders including cancer. AIs can cause joint pain, hot flushes, and an increased risk of fractures and osteoporosis.15
Although more evidence is needed in relation to environmental factors influencing non-adherence (drug costs, health system organization, patients’ socioeconomic status),43,44 there is consistent evidence that side effects play an important role in patients’ decision making, either to adhere and endure treatment16 or to intentionally discontinue treatment.1,17 Patient-reported factors influencing adherence/non-adherence include effective communication,18,19 indicating that women value oncologists’ information exchange on how the drugs work and, in particular, their side effects, and professionals’ active support on how to ameliorate discomfort. In addition, patient-centered communication and higher patient’s self-efficacy have been shown as positive predictors of persistence with AET.20,21 Furthermore, a recent systematic review found that persistence with AET was related to seeing a specialist (oncologist or mastologist) rather than a GP,9,22 suggesting that trust and expert advice may play a positive role.
The perspectives of health care providers on AET adherence and its management, however, has been little explored worldwide,23 and if we are to consider adherence not only as a patient problem, there is clearly a need to analyze oncologists and health care providers’ perspectives and roles from AET initiation to long-term follow-up care. The latter varies across countries where primary health care providers such as general practitioners and/or BC nurses are the main point of contact once women are discharged from hospital. In the case of Argentina, clinical oncologists are the chief prescribers of AET and are responsible for follow-up care, although other cancer specialists (mastologists, gynecological oncologists, radiation oncologists) can also do so for early BC, thus making all these specialists relevant to analyze in relation to patients’ adherence to medication. Whether specialists consider drug side effects significant or not or how they facilitate discussion on medication-taking or manage patients’ complaints and concerns with AET could have an impact on adherence. In addition, researchers have identified the health system organization, amongst other modifiable social factors, as a driver for different outcomes in cancer treatments between affluent and disadvantaged groups.46,49 The fragmented nature of Argentina’s health system, comprising the public sector (free of charge), social security (through employment), and private health insurance, poses a challenge to seamless access to cancer treatments46 despite the national coverage of free of charge, protocol-approved oncological drugs. Problems identified in relation to AET were limited availability of hormonal lines in the public sector in comparison to the private sector, difficulties in accessing expensive drugs in the social security system, and in prescribing drugs outside the protocol in the public sector.24 Although the most common drugs (TAM and anastrozole) seem to be easily accessible, it is worth noting that the population groups assisted by providers of the three-health subsystems vary in terms of their socioeconomic status (from most deprived to most affluent groups). Therefore, the perceptions that oncologists may have of patients’ characteristics, including challenges encountered and strategies to overcome them, can shed light on modifiable factors in relation to adherence, especially in health systems with multiple providers.1
As we know more about patients’ preferences, experiences, and behaviors toward AET adherence, and what patients’ value in their oncologists, this study sought to fill an important gap in the literature on adherence which is to gain an in-depth understanding of the perspectives of oncologists themselves. Hence, the aim of this qualitative study was to explore oncologists’ perspectives on adherence/non-adherence to AET and the factors influencing continuation/discontinuation of treatments, their perceptions of medication side effects, and their management strategies in supporting patients’ adherence and persistence.
Materials and methods
This paper reports on data from a larger study of male and female oncologists’ roles and practices in AET in contexts of public/private health system providers. While findings on prescribing practices have been reported in detail elsewhere,24 this article focuses on perspectives and management strategies related to adherence. A stratified purposeful sample was used to obtain representatives of male/female oncologists working at three different health subsystems, public, private, and social security, in the city of Córdoba, Argentina.
Participants were identified and recruited through the Website of the largest social security provider,41 and initial contact with heads of services and a hospital director. The main oncology institute (public), three private clinics (social security), and three private hospitals (private health) were purposively selected. All oncologists interviewed were asked to further identify other potential participants with personal contacts, to whom the researcher contacted via telephone and email. As clinical oncologists are the main specialists involved in administering adjuvant therapy (chemotherapy and hormonal treatment), they constitute the majority of the sample (13) whilst other oncology subspecialties (3) were included if they regularly prescribed AET and managed patients’ treatment. The sample size was initially planned for around 20 participants following the concept of ‘information power’25 given the intrinsic features of this study: a narrow aim, the salient knowledge of the participants, and the availability of a theoretical background indicating that health system provider and physician’s gender could explain differences in treatment outcomes.39,49 It was considered that these features would offer sufficient focus for the interviews. Eighteen oncologists were approached and only 16 participated (1 interested but did not provide interview dates; 1 non-respondent). For characteristics of the sample, see Table 1.
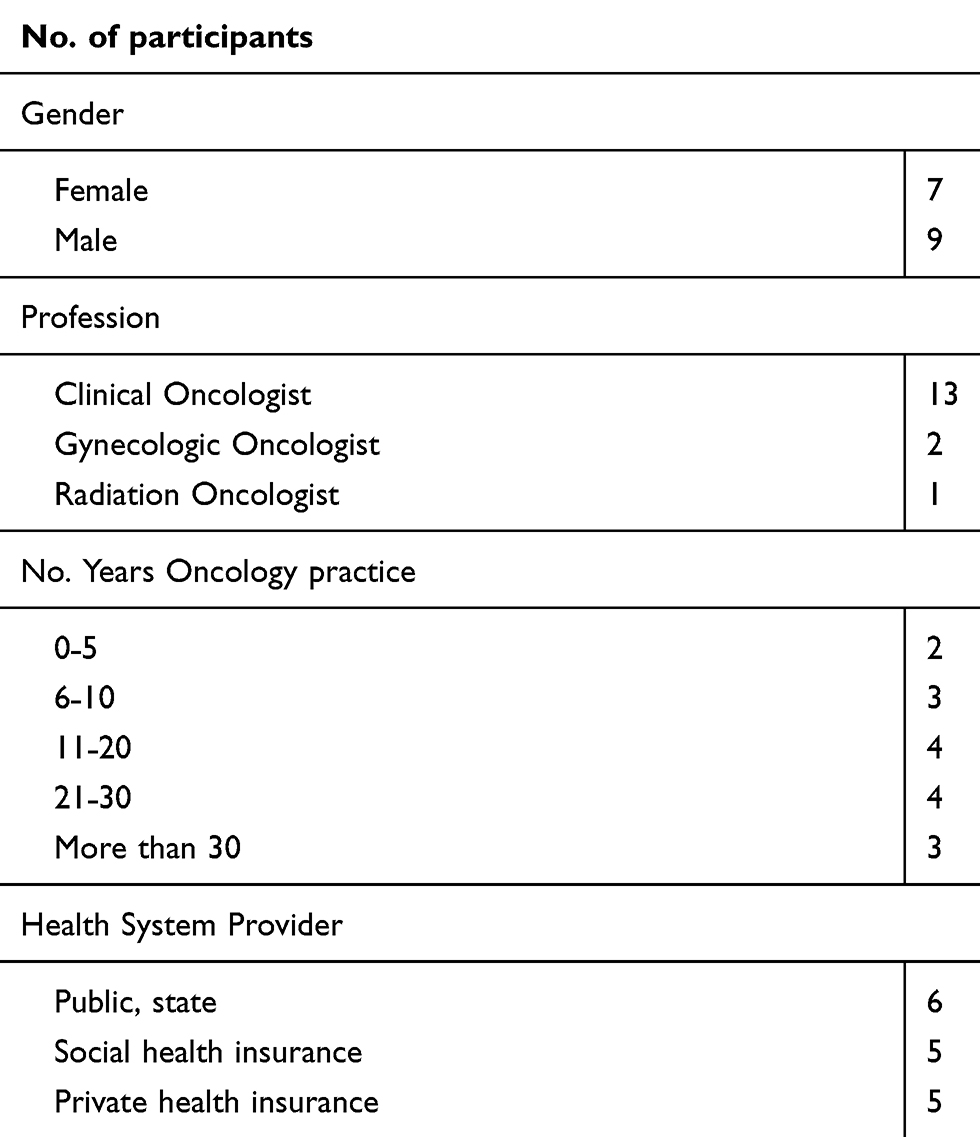 |
Table 1 Participant characteristics |
All interviews were conducted in Spanish by the author, who is a native speaker with a research background in medical humanities and was familiar with the local health system organization and guidelines on clinical management of BC hormonal treatment. All interviews were digitally recorded with participants’ written informed consent and took place at oncologists’ consulting rooms and hospital offices during July 2016. Interviews lasted between 37 and 101 mins and were transcribed verbatim by a research assistant with experience in qualitative data management. The author subsequently checked transcripts for accuracy, anonymized data, and translated it into English. An interview guide was designed using open-ended questions and probes and consisted of questions such as, how oncologists considered adherence to AET; what factors they thought influenced adherence/non-adherence; what were the patients’ complaints regarding side effects; and how they managed patients to ensure they remained adherent to treatment (see full details Appendix 1). After preliminary analysis of the data, it was considered that sufficient information power25 regarding relevant patterns of adherence perceptions and management strategies was obtained before completing the 16 interviews.
Data analysis drew on the Framework approach, following its five methodological steps (familiarization with the data, identification of a thematic framework, indexing, charting, and mapping and interpretation of themes).42 After familiarization with the data and identification of common patterns across the data set (themes), YE coded two transcripts (male and female oncologists) from each of the three health system providers. A working analytical framework was created after grouping codes into categories, which were both generated by a deductive approach informed by the interview guide and through an inductive process based on participants’ accounts. The working analytical framework was subsequently applied by indexing the rest of the transcripts manually, using textual codes. For the charting process, an Excel spreadsheet was used to develop a matrix, consisting of a case chart for each respondent where notes and extracts of relevant passages were included for all identified categories and codes. This allowed for further identification of patterns and associations (ie, similarities and differences in relation to oncologists’ gender and health system provider) during the mapping and interpretation process. The process was completed through the generation of themes and sub-themes that emerged from the data and the research questions. To ensure reliability and confirmability of data analyzed by a single researcher, the processes of indexing and charting were conducted in two different stages. First, indexing and charting were developed by using the Spanish version of the transcripts. After translation into English, a second round of indexing and charting took place fourth months after the first one. The cross-checking of the two versions enhanced the process of refining themes and subthemes and ensured the elimination of ambiguity of coded terms.
Results
A total of 16 individual semi-structured in-depth interviews were conducted with oncologists, 9 male and 7 female doctors, with specialization in clinical oncology, radiation oncology, and gynecological oncology. The 16 oncologists interviewed worked at 3 different health subsystems (see Table 1). The population of women assisted by these providers, according to data from 2010, were as follows: 69% of women were insured – by the social security (50%), private health (17%), or state plan (2%) – whilst a 31% were uninsured, which means they only had access to public sector cancer services.40
The analysis identified four themes: perceptions of adherence; perceptions of non-adherence; patients’ complaints; and management strategies. Each of these have sub-themes. Data interpretation is reported here by using relevant verbatim quotes to illustrate.
Perceptions of adherence
The majority of participants from all health system providers reported that adherence to AET was quite high and considered that treatments were, overall, well tolerated. Participants’ responses were remarkably consistent. Some of them used expressions such as “adherence is perfect”, “no problems”, others provided estimates of 90–95% of the adherers. In terms of long-term persistence with treatment, only one oncologist estimated 40% of the patients discontinuing AET by the 10th year. The reasons they provided to explain a high level of adherence were varied.
Good tolerance, comparison to chemotherapy
Some of them argued that in comparison to acute treatments, especially, chemotherapy, AET was well tolerated:
“Hormonal side effects are quite limited, though it is true that there are women who suffer a lot, and also women in a very low percentage, that discontinue treatment because of side-effects. I am not sure, but must be a 1–2% of cases. It is unusual, very low”. (10, male, social security)
“Adherence is, in general, very good, either TAM or AIs, nothing to do with chemotherapy! as they don’t produce hair loss, nauseas, vomits, we may have had a patient with nauseas, but nothing to do with chemo. AET has far fewer adverse reactions than chemo”. (15, male, public sector)
Information provided
For some respondents, good adherence had a direct relation to the information provided. However, oncologists strongly varied in their definition of “information”. As the expressions below illustrate, one participant valued communication about risks and benefits of treatment, while another positively emphasized the transition between active, more aggressive treatment, and chronic treatment with medication.
“Adherence is quite high. In my view, adherence is influenced by the idiosyncrasies of the patient who decides to adhere to a particular treatment, and the type of information that she receives, and the contention that she has from the service, from doctors, administrative staff, mental health, nursing … You need to inform the person about her disease with the risks and benefits of taking a treatment and reassure her that if she has an adverse effect you will be able to support her, that the she won’t feel helpless”. (2, female, public sector)
“Adherence? it is perfect […] One explains treatments at the beginning. We tell [the patient] she will undergo surgery; chemo (if she needs it) and we explain its adverse effects; and then radiotherapy, where she will come every day. And after that, we tell them there is the little pill that she will take once a day like for any other disease (hypothyroidism or hypertension). We tell her that she won’t feel anything or very little. So, the truth is that patients get to the hormonal treatment with a very good adaptation”. (6, male, private sector)
Cancer patient attitude
Some referred to cancer patient’ attitudes toward the disease, in terms of the protection and reassurance that anti-cancer drugs offered to control the disease:
“If you tell the patient that the current trend is 10 years, she will be happy, she will feel protected”. (01, female, social security)
“In general, the hormonal patients hang on to medication. There is no desertion with TAM” [.] The majority don’t want to stop treatment they want to continue for 5 more years. They hang on to the drug because they feel they are being treated with something”. (05, male, private sector)
Perceptions of non-adherence
When asked about what were the reasons for patients’ non-adherence, respondents provided a range of clinical and social factors. Some of them referred to severe side effects, whilst others expressed other non-clinical factors such as women’s fertility concerns, losing the insurance plan, low education (lack of understanding), and attitudes towards the disease where patients refused any type of cancer treatments.
Severe side effects
Oncologist felt that severe side effects such as thromboembolism, fractures, hemorrhages, and changes in the endometrium were a concern and a reason to discontinue medication, although they thought these were rare cases. They also indicated how they routinely controlled severe effects through different tests and medications.
“With TAM, the most common is enlargement of the endometrium, circulatory disorders, a handful with digestive ones … Anastrozole, I follow-up bone issues with densitometry. I haven’t seen that they are worst by anastrozole; by taking calcium they control it perfectly”. (01, female, social security)
“You can have higher risk of fractures with aromatase inhibitors, with TAM a 2% risk of endometrial cancer”. (2, female, public sector)
“We haven’t seen many side effects recently. With TAM we are mainly concerned with vascular toxicities”. (6, male private sector)
Refusing treatment
Other participants described that some patients were non-adherers because they refused any type of cancer treatment.
“Some people with advanced cases they don’t want treatment and they only ask for pain-control medication”. (13, female, public sector)
“On very few occasions we have had patients that have abandoned treatment. I had two patients only, but they didn’t adhere to any treatment: chemo, AET, nothing!”. (15, male, public sector)
Fertility concerns
Pre-menopausal women who wanted to have children were mentioned by some oncologists as presenting a challenging situation that could lead to discontinuation. Especially women in their late 30 s for whom a 5-year course of treatment may leave them childless.
“It is difficult in pre-menopausal women without children”. (10, male social security)
“The problems with TAM are posed by women who want to have children. And that is very complicated”. (4, female, social security)
Low education, life circumstances
Oncologists across the different providers stated that patients in the public sector had more difficulties in keeping up with their treatments and often lacked understanding of medication regimes. However, public sector oncologists said that patients continued attending appointments, and therefore they did not perceive them as completely discontinuing treatment.
“In the public sector, non-adherence happens quite often. Mainly because of lack of education. Patients don’t understand the disease, the treatment. […] Many times, it has happened to us that we give them the medication and they return in three months and they say, ‘I took it only once, Dr.’ […] It is challenging … You need to constantly ask them if they have taken the medication”. (13, female, public sector)
“There are very few cases [of non-adherence] because of disease denial or family problems that mean that they put their disease in a second place. Patients abandon appointments for two-three months, in occasions for one-two years, and they resume treatment later. But they are a minority, less than 10% of patients”. (12, female, public sector)
Oncologists in the social security and private sector also acknowledged that patients’ socioeconomic status had an impact on their adherence to AET medication.
“Of course, there is the fact of being a private center, where we have a different patient population from the public sector, with a high intellectual and social level to whom we can more easily explain and for them to understand, because these are chronic treatments. It is not easy for a person to remember to take a pill every day of her life, during 5, 8 or 10 years. And I have spoken to colleagues that work in the public sector and they said that, sometimes, these chronic treatments are very difficult, especially as the patient has to take them alone in their home. Sometimes it is difficult due to the social circumstances, of understanding and so on, of that patient”. (6, male, private sector)
An oncologist who primarily worked in the private sector but simultaneously worked for a few hours in a public hospital commented:
“In the public sector [adherence] is a bit more erratic. Yes, it is clear that there is a difference between the public and private sector with a gap difference of no less than 20–30%. In the public sector, patients rely on someone to accompany them, on someone who can collect their medication, on whether they live in the city, because we receive patients from other provinces and they need to cover transport costs … there are a series of factors to consider”. (5, male, private sector)
Lack of insurance coverage
In the private sector, losing the insurance plan was seen as a reason for discontinuation, especially in times of employment uncertainty.
“Adherence here is very good. The only problem would be that the patient losses her private health insurance, due to a job change, or because the husband was made redundant. The most important issue is that the patient keeps her private health insurance”. (5, male, private sector)
Patients’ complaints
Oncologists were asked about what were the most common complaints they received from patients in relation to the medicines prescribed. Most respondents were familiar with side effects affecting women’s quality of life, and they distinguished them from other severe side effects that they controlled through routine follow-up tests. Notably, and unlike the large body of literature reporting on patients’ perspectives, bothersome side effects were not perceived as influencing non-adherence. Only one respondent identified them as causing treatment discontinuation in a small group of patients.
Physical symptoms
The most common physical complaints oncologists referred to were hot flushes, weight gain, joint pain, and dyspareunia. There were also a range of other physical and psychological symptoms mentioned; however, the majority of respondents did not see them as a reason to discontinue treatment.
“Everything changes, they have vaginal dryness, diminished libido, obesity, they change their bodies, they become menopausal”. (3, female, public sector)
“Inflammation, cellulitis in legs, varicose veins with TAM, a small fluid retention in the legs. But this is something cosmetic, not a functional complication. But yes, they complain a lot about this. […] Joint pain generated by anastrozole/letrozole that patients refer to in consultations. But nothing serious, let’s say, there are no complications such as fractures”. (12, female, public sector)
“The most upsetting are hot flushes and weight gain, these are by far their biggest complaints. But they don’t abandon treatment”. (5, male private sector)
Only one oncologist clearly acknowledged that a small group of patients had to stop the medication due to side effects affecting women’s quality of life.
“With aromatase inhibitors not so much complaints with hot flashes, but they can give other inconveniences such as articular pain or metabolic disorders to which we need to control. Very occasionally these are a reason for discontinuation. Well, I have women that could not be treated with TAM, and others that could not continue treatment with AIs because of these upsetting symptoms. I insist, it is a very low percentage, but there is a small group”. (10, male social security)
Some oncologists directly associated patients’ complaints with their socioeconomic status and the health system provider they had access to:
“The public sector patient, people with a poor economic condition, they may have a headache, a hot flush and they won’t mention it! You have to ask them and insist a bit. […] Only when we ask them and explain that there are solutions for vaginal dryness, for example, only then they will talk about it. […] A woman from another social class or in the private sector the first thing they’d tell you is, ‘I won’t take this pill, I soak the bed, I have to pull the covers off, my husband complains … ’ Therefore, a patient from a low socio-economic position has different priorities, and the manifestation of symptoms affect them differently. The public sector patient very rarely will complain”. (14, male public sector)
Psychological symptoms and partner relationships
Depression, anxiety, and mood swings were the most common physiological symptoms described. Low libido was also seen as affecting partner relationships.
“We have experienced many times that patients came and told us ‘my mood is lower, I cry all the time, I realized about my disease and what I went through’ […] But I started to see more and more cases, and they all happened when they started TAM, we have a report of 3 or 4 cases with these crises, but when we took them out of TAM and changed for an AIs, it is incredible the change they made at psychological level”. (6, male private sector)
“We know our patients, we know how they start, how they continue, how they evolve. So, if during a check-up they start crying, something that they hadn’t done before, we know is due to TAM”. (13, female, public sector)
“Many patients are abandoned by their partners because of lack of sexual relationships”. (3, female, public sector)
Management strategies
Medication change
Male doctors, in particular, expressed that they dealt with side effects by a change in medication.
“When we have complaints with joint pain, we can change the medication from anastrozole to letrozole or otherwise we can change to TAM. Sometimes changing the AI the patient tolerates it well, and there is no problem”. (15, male, public sector)
However, another oncologist in the public sector was cautioned about changing medication too often as access to drugs was rather restricted.
“The treatment guidelines always say that one has to be energetic, to put emphasis on the management of toxicities in order not to skip a [hormonal] line. If the patient comes and says that the pill gives them headache, and you change the drug, then she complains of articular pain, when you realized, you have exhausted all resources! And here in the public sector we have very few resources [hormonal lines]”. (14, male, public sector)
In the private sector, male oncologists were more certain about switching medication to deal with unpleasant symptoms.
“In young women with dyspareunia, who tell us, ‘I have an active sexual life, and I don’t like this’, we can change drugs. When they change to anastrozole the truth is that they improve. This is a minority of cases, 1 or 2 patients that one remembers. One knows that there is another medication for that patient, so she won’t discontinue hormonal treatment”. (6, male, private sector)
Support services
In comparison to male doctors, female doctors often described the use of support services for mental health and menopause symptoms, including the prescription of adjunctive medications that offered some symptom relief.
“We refer them to a center that deals with menopausal services, within public maternities, to see which medication can be given, anxiolytics or anti-depressants for hot flushes, so it can be managed and the patient can improve. […] In general, it hasn’t happened to me that there was a need to change medication for an intolerance that the patient has expressed. The cosmetic, joint pain, we manage”. (12, female, public)
“I am sure this is related to TAM, but we cannot stop the medication, we have to treat the depression, so we advise them psychological therapies, or to take a break from work if possible, or sometimes a change of diet alongside physical activities”. (16, female, private sector)
Supportive relationship with oncologist
Some female doctors highlighted the importance of their relationship with patients in managing women who might want to abandon treatment and described the support they offered to motivate them.
“Complaints? No problems. I convince them. I have a very good relationship with them. I am very proactive, for the patient to be stimulated, to feel good, to be a woman […] If they don’t want to take TAM or another drug, well I give them a ‘holiday’, I tell them: ‘when you want it you will come and pick it up’ (the drug) and they come back […] In intermediate patients [not a high risk], I give them time to think about it”. (3, female, public sector)
Another female doctor referred to the importance of monitoring emotional symptoms such as anxiety and depression, something that she also considered needed to be informed to patients at the time of treatment initiation.
“I closely observe patients in relation to depression, I have a lot of attention to detail with my patients. It is a reaction to TAM, and we need to bear this in mind. And we need to let patients know, tell them not to feel bad, that it is due to the medication, that is part of the treatment. We often say this at the beginning of treatment, that is something that can happen”. (13, female, public sector)
Some oncologists in the private and social security sector referred to other challenges they experienced such as extending hormonal therapy to 10 years, whereby they felt that expert trust was a relevant factor in managing continuation.
“The main complaint at the moment is a sub-group of patients to whom we tell they need to take the medication for 10 years. In these cases, it is like the patient had mentalized herself that treatment was for 5 years, and sometimes this shocks them, and some express a bit of irritation, but nothing that we couldn’t manage. And in general, they end up doing what we suggest to them”. (7, male private)
Discussion
This study explored oncologists’ perspectives on adherence/non-adherence to AET and the management strategies they use to ensure treatment continuation in women with early BC. Oncologists believed patients’ adherence was high overall and explained that it was associated with good tolerance of AET in comparison to chemotherapy, information provided, and patients’ feeling reassured because of treatment. Non-adherence was not perceived as a major source of concern, and it was related to rare cases of severe side effects, fertility issues, refusing treatment, losing the insurance plan, lack of education, and social circumstances. Patients’ complaints over bothersome side effects were not identified as the main reason for discontinuation. Public and private sector patients, however, were perceived as having different attitudes toward side effects. Management strategies included medicine change, referral to support services, and a supportive relationship with the oncologist.
Although most respondents considered adherence as very high, none of them mentioned how this was estimated. In the absence of a monitoring strategy, adherence to treatment based on patients’ attendance to follow-up appointments and self-reported attitudes toward medication can create a false sense of treatment adherence that cannot account for medication-taking behavior, ie, missing drugs, or taking breaks, as it has been reported in other studies.26 Although oncologists did not explicitly differentiate between intentional and unintentional non-adherence, their accounts indicate that intentional non-adherence is low, but unintentional non-adherence is rather high, especially in public sector patients. This finding is consistent with a quantitative study on patients taking TAM that reported a high proportion of unintentional non-adherence12 and adds weight to the role of social factors affecting adherence in low-income women.
The perception of adherence as related to cancer patient attitudes of feeling reassured and protected while in treatment (fear of recurrence) is consistent with studies reporting on anastrozole30 and TAM,31 where adherers expressed an imperative and a necessity to keep themselves on the treatment regardless of bothersome side effects. In addition, information on AET provided to patients at the time of treatment initiation was acknowledged as relevant only by some oncologists. Yet the content of the information given substantially varied: from reassurance that AET was more tolerated than chemotherapy, to an explanation of risks and benefits of treatments. Timely information about side effects has been identified in the literature as a relevant factor associated with adherence,32 however, and similarly to this study, a European survey reported that women were more likely to receive information about the benefits of AET (68%) than information about side effects (57%).33
Socioeconomic status and patients’ behavior observed through users of the private and public health subsystems is another factor respondents identified as affecting non-adherence and patients’ complaints, which has been under-explored in the literature. This was specifically linked to two related instances: health literacy and self-efficacy. On the one hand, health literacy has been associated to unintentional non-adherence when individuals “struggle to comprehend instructions on prescribed medicines and consequently may take the wrong dosage at the wrong time or mix up medicines” (p.12).27 In this study, “lack of education” and “understanding” of medication-taking were expressed as a concern by oncologists assisting low-income patients. On the other, self-efficacy, here considered as the confidence of patients to ask questions in medical encounters, indicates that affluent users of the private health system were identified as more complaining and able to express discomfort and to demand a change of medication. Conversely, most deprived women were described as being disempowered to express undesirable symptoms. The later can lead to unintentional non-adherence, as a previous study has associated high self-efficacy in low-income women with greater adherence.21
It is also noteworthy that oncologists’ perceptions of non-adherence contrast with those in the literature based on patient-reported experiences (see Table 2). Revealingly, many respondents considered non-adherence a medical concern with severe side effects, indicating that patients’ continuation with one drug was dependent on clinical observations of other medical pathologies, ie, increased risk of thromboembolism, osteoporosis, or engrossment of the endometrium. Non-adherence in this sense was perceived as a doctor’s responsibility for routine check-ups rather than dependent on patients’ own experiences with medication. This corresponds with the overall perception that intentional non-adherence was low. However, it contrasts with the large body of research that associates non-adherence to patients’ burdensome experiences with drug side effects. Oncologists seemed aware and concerned with the monitoring and management of severe side effects (medical, objective and life-threatening), but they were less so in relation to the unpleasant ones (personal, subjective, affecting quality of life). Although some retrospective studies on AIs associate the likelihood of unpleasant side effects to previous chemotherapy treatment,28 it still remains difficult to predict which patients will suffer them more15 which can lead doctors to regard them as less relevant. In this study, and despite one doctor referring to “some women” as being seriously affected, only rarely they viewed these symptoms as a reason to discontinue treatment. It may also be the case that unpleasant side effects, in comparison to the risk-assessed severe ones, are highly subjective, in that women can experience them and decide to tolerate them for the benefit of cure/protection.16 Oncologists’ perceptions of unpleasant side effects also resonate with findings from a Dutch observational study where oncologists often made use of “implicit persuasion” (ie, inducing patients’ choice) during consultations about treatment options, by underreporting and downplaying the impact of AET in patients’ quality of life.45 If oncologists tend to minimize these side effects during follow-up care, as it seems that is the case in this study, then expectations of adherence could have negative implications for both patients (if symptoms are worse than initially thought) and professionals (overestimating tolerance and adherence). Finally, it is also important to consider the context of survivorship care whereby the Argentinian recommendation guidelines on follow-up appointments,29 state the clinical tests a patient should have (annual mammography, pelvic exam, bone densitometry), but surprisingly, they state nothing about monitoring adherence to medication or discussing with patients the management of adverse effects.
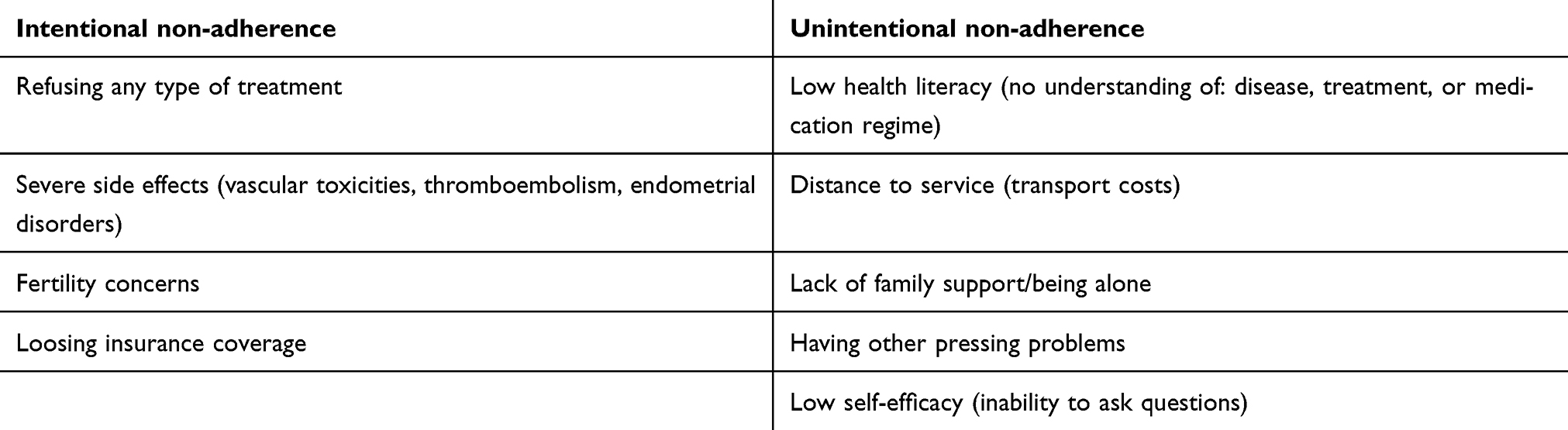 |
Table 2 Participants’ perceptions of intentional and unintentional non-adherence |
Management strategies reported by oncologists to ensure adherence and persistence in this study appeared to differ according by gender. As reported previously during AET prescribing,24 female oncologists seemed to develop more partnership-building behaviors. The identification of patients’ depression and mood swings, as well as the nature of communication exchange (partner relationships, cosmetic concerns), reveals a more empathetic, person-centered type of communication.38,39 From attention to detail to proactive motivation, female oncologists expressed greater awareness of unpleasant side effects, whilst allowing them to use different strategies, ie, support services, adjunctive medicines, and medication breaks. With few exceptions, male oncologists referred to initiatives that drew more on drug effectiveness and resorted to switching medication (to AIs or TAM or to different brands of the same drug) in follow-up care appointments. This approach was often mentioned in the private health system where access to a larger number of hormonal lines was reported as less complicated.
The findings of this study have a number of recommendations for managing adherence. First, the need for data on adherence and persistence in Argentina, collected through a reliable measurement (prescription refills) across the health system providers; private, public, and social security. Lack of statistics was felt as a need by some oncologists, and having this information will certainly provide a better understanding of the magnitude of the adherence/persistence problem as well as identification of which one is in need of effective interventions.
Information to patients should consider clear explanations on both severe and unpleasant side effects so women are prepared for and understand the symptoms that are likely to occur and are reassured on the different types of support available. There is evidence that indicates that switching medication (from TAM to AIs or vice versa) can lead to poor adherence;1,34 therefore, other effective coping strategies should be explored.35
Interventions to improve communication skills in oncologists and specialists responsible for survivorship care such as motivational interviewing strategies and techniques36,37 could offer health care professionals with a better identification of barriers to medication-taking (intentional and unintentional) and women with opportunity to discuss symptoms and problems, thus strengthening their self-efficacy and effective medication-taking over a long-term course of therapy.
Recommendation guidelines on follow-up appointments should incorporate discussion on AET medication-taking, unpleasant side effects, and coping mechanisms, so women are encouraged to discuss emerging problems during follow-up. In addition, interventions aiming at coordination of care,18 such as signposting women to a telephone communication with an oncology nurse could be considered as part of the supporting strategies between scheduled appointments.
Strengths and limitations
To our knowledge, this is the first study to explore oncologists’ perceptions of adherence/non-adherence to AET in Argentina. The study sample was representative of the three sector providers within the Argentinian health system and of professionals’ gender, and their accounts elicited some interesting differences and similarities within and between services. In terms of limitations, there is a paucity of qualitative and quantitative studies in this field of research in the Latin American context, and hence contextual comparisons were rather limited. As with all qualitative studies, a small sample size means that results may not be generalizable. Yet, in-depth interviews offer a distinct insight into the way adherence to AET is perceived and managed by professionals, especially in contexts where little research is available, allowing us to advance the knowledge based in this area.
Conclusion
Overall, the findings of this study on oncologists’ perspectives on adherence/non-adherence to AET show similarities and significant differences with those in the literature based on patient-reported factors. It is crucial that oncologists consider providing information to patients on both severe and unpleasant side effects and that they monitor adherence and offer support strategies in follow-up appointments. Although reliable statistics on adherence and persistence are needed, oncologists accounts have indicated concern with unintentional non-adherence.
Recommendations include motivational interviewing strategies, engagement with an oncology nurse, and changing national recommendation guidelines to ensure the monitoring of adherence in follow-up care.
Abbreviation list
AET, adjuvant endocrine therapy; AI, aromatase inhibitors; BC, breast cancer; TAM, Tamoxifen.
Ethics approval and informed consent
Ethics approval for this study was obtained from London Metropolitan University Research Ethics Committee (4053016). Written consent was obtained from participants for publication of the data collected in academic journals.
Acknowledgments
I would like to express gratitude to the participants of this study, without their contribution this research would have not been possible. I also gratefully acknowledge the help of the anonymous referees and journal editors in the preparation of this manuscript. This study was funded by the School of Social Professions, London Metropolitan University.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Murphy CC, Bartholomew LK, Carpentier MY, Bluethmann SM, Vernon SW. Adherence to adjuvant hormonal therapy among breast cancer survivors in clinical practice: a systematic review. Breast Cancer Res Treat. 2012;134(2):459–478. doi:10.1007/s10549-012-2114-5
2. Huiart L, Ferdynus C, Giorgi R. A meta-regression analysis of the available data on adherence to adjuvant hormonal therapy in breast cancer: summarizing the data for clinicians. Breast Cancer Res Treat. 2013;138(1):325–328. doi:10.1007/s10549-013-2422-4
3. Makubate B, Donnan PT, Dewar JA, Thompson AM, McCowan C. Cohort study of adherence to adjuvant endocrine therapy, breast cancer recurrence and mortality. Br J Cancer. 2013;108(7):1515–1524. doi:10.1038/bjc.2012.494
4. Sabate E, ed. Adherence to Long-term Therapies: Evidence for Action. Geneva: The World Health Organisation; 2003. Available from: http://www.who.int/chp/knowledge/publications/adherence_report/en/. Accessed June 12, 2018
5. Ehrenzweig Sánchez Y. Modelos de cognición social y adherencia terapéutica en pacientes con cancer. Avances En Psicología Latinoamericana. 2007;25(1):7–21. Spanish.
6. Souza BF, Moraes JA, Inocenti A, Santos MA, Silva AEBC, Miasso AI. Mujeres con cáncer de mama en tratamiento con quimioterapéuticos: síntomas depresivos y adhesión al tratamiento. Rev Latino-Am Enfermagem. 2014;22(6):866–873. Spanish. doi:10.1590/0104-1169.3564.2491
7. Oliveira RS, Menezes JTL, Gonçalves MGL. Adesão à terapia hormonal adjuvante oral em pacientes com câncer de mama. Revista Brasileira De Cancerologia. 2012;58(4):593–601. Portuguese.
8. Peper FE, Esteban S, Terrasa SA. Evaluación de la adherencia primaria a medicamentos en pacientes con enfermedades crónicas afiliados al Seguro de Salud del Hospital Italiano de Buenos Aires: estudio de cohorte retrospectiva. Aten Primaria. 2018;50(2):96–105. Spanish. doi:10.1016/j.aprim.2017.01.013
9. Brito C, Portela MC, Teixeira Leite de Vasconcellos M. Factors associated to persistence with hormonal therapy in women with breast cancer. Rev Saúde Pública. 2014;48(2):284–295. doi:10.1590/s0034-8910.2014048004799
10. GLOBOCAN: Cancer Today.. Estimated age-standardized incidence rates (World) in 2018, all cancers, both sexes, all ages; 2018. Available from: http://gco.iarc.fr/today/home.
11. Brett J, Fenlon D, Boulton M, et al. Factors associated with intentional and unintentional non-adherence to adjuvant endocrine therapy following breast cancer. Eur J Cancer Care (Engl). 2018;27(1):(201801)e12601. doi:10.1111/ecc12601.
12. Moon Z, Moss-Morris R, Hunter MS, Hughes LD. More than just side-effects: the role of clinical and psychosocial factors in non-adherence to tamoxifen. Br J Health Psychol. 2017;22(4):998–1018. doi:10.1111/bjhp.12274
13. Horne R, Weinman J, Barber N, et al. Concordance, adherence and compliance in medicine taking – report for the National Coordinating Centre for NHS Service Delivery and Organisation Research and Development; 2005. Available from: http://www.netscc.ac.uk/netscc/hsdr/files/project/SDO_FR_08-1412-076_V01.pdf.
14. Horne R, Weinman J. Patient’s beliefs about prescribed medicines and their role in chronic physical illness. J Psychosom Res. 1998;47:555–567. doi:10.1016/S0022-3999(99)00057-4
15. Henry NL. Endocrine therapy toxicity: management options. Am Soc Clin Oncol Educ Book. 2014;e25–e30. doi:10.14694/EdBook_AM.2014.34.e25
16. Harrow A, Dryden R, McCowan C, et al. A hard pill to swallow: a qualitative study of women’s experiences of adjuvant endocrine therapy for breast cancer. BMJ Open. 2014;4(6):e005285. doi:10.1136/bmjopen-2014-005285
17. Wuensch P, Hahne A, Haidinger R, et al. Discontinuation and non-adherence to endocrine therapy in breast cancer patients: is lack of communication the decisive factor? J Cancer Res Clin Oncol. 2015;141(1):55–60. doi:10.1007/s00432-014-1779-z
18. Lambert L, Balneaves LG, Fuchsia HA, Gotay CC. Patient reported factors associated with adherence to adjuvant endocrine therapy after breast cancer: an integrative review. Breast Cancer Res Treat. 2018;167(3):615–633. doi:10.1007/s10549-017-4520-1
19. Farias AJ, Ornelas IJ, Hohl SD, et al. Exploring the role of physician communication about adjuvant endocrine therapy among breast cancer patients on active treatment: a qualitative analysis. Support Care Cancer. 2017;25(1):75–83. doi:10.1007/s00520-016-3389-6
20. Kahn KL, Schneider EC, Malin JL, Adams JL, Epstein AM. Patient centered experiences in breast cancer: predicting long-term adherence to tamoxifen use. Med Care. 2007;45(5):431–439. doi:10.1097/01.mlr.0000257193.10760.7f
21. Liu Y, Malin JL, Diamant AL, Thind A, Maly RC. Adherence to adjuvant hormone therapy in low-income women with breast cancer: the role of provider-patient communication. Breast Cancer Res Treat. 2013;137(3):829–836. doi:10.1007/s10549-012-2387-8
22. Moon Z, Moss-Morris R, Hunter MS, Carlisle S, Hughes LD. Barriers and facilitators of adjuvant hormone therapy adherence and persistence in women with breast cancer: a systematic review. Patient Prefer Adherence. 2017;11:305–322. doi:10.2147/PPA.S134792
23. Wheeler SB, Roberts MC, Bloom D, et al. Oncology providers’ perspectives on endocrine therapy prescribing and management. Patient Prefer Adherence. 2016;10:2007–2019. doi:10.2147/PPA.S95594
24. Eraso Y. Factors influencing oncologists’ prescribing hormonal therapy in women with breast cancer: a qualitative study in Córdoba, Argentina. Int J Equity Healxth. 2019; 18 (1):35. doi:10.1186/s12939-019-0936-z
25. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
26. Greer JA, Amoyal N, Nisotel LA, et al. Systematic review of adherence to oral antineoplastic therapies. Oncologist. 2016;21(3):354–376. doi:10.1634/theoncologist.2015-0405
27. Roberts J. Local Action on Health Inequalities. Improving Health Literacy to Reduce Health Inequalities. London:Public Health England; 2015. Available from: http://www.instituteofhealthequity.org/resources-reports/local-action-on-health-inequalities-health-literacy-to-reduce-health-inequalities/health-literacy-improving-health-literacy-to-reduce-health-inequalities-full.pdf. Accessed August 10, 2018.
28. Henry NL, Azzouz F, Desta Z, et al. Predictors of aromatase inhibitor discontinuation due to treatment-emergent symptoms in early-stage breast cancer. J Clin Oncol. 2012;30:936–942. doi:10.1200/JCO.2011.38.0261
29. Consenso Nacional Inter-Sociedades sobre Cáncer de Mama: Pautas para el seguimiento de pacientes asintomáticas luego del tratamiento primario con intención curativa; 2007. Available from: https://www.ama-med.org.ar/images/uploads/files/consenso%20pacientes%20asintom%C3%A1ticos%202007.pdf.
30. Wickersham K, Happ MB, Bender CM. “Keeping the boogie man away”: medication self-management among women receiving anastrozole therapy. Nurs Res Pract. 2012;2012:462121. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3543807/. Accessed Feb 4, 2019.
31. Grunfeld EA, Hunter MS, Sikka P, Mittal S. Adherence beliefs among breast cancer patients taking tamoxifen. Patient Educ Couns. 2005;59(1):97–102. doi:10.1016/j.pec.2004.10.005
32. Brett J, Boulton M, Fenlon D, et al. Adjuvant endocrine therapy after breast cancer: a qualitative study of factors associated with adherence. Patient Prefer Adherence. 2018;12:291–300. doi:10.2147/PPA.S176067
33. Wengström Y, Aapro M, Leto Di Priolo S, Cannon H, Georgiou V. Patients’ knowledge and experience of adjuvant endocrine therapy for early breast cancer: a European study. Breast. 2007;16(5):462–468. doi:10.1016/j.breast.2007.02.007
34. Farias AJ, Hansen RN, Zeliadt SB, Ornelas IJ, Li CI. Thompson B factors associated with adherence to adjuvant endocrine therapy among privately insured and newly diagnosed breast cancer patients: a quantile regression analysis. J Manag Care Spec Pharm. 2016;22(8):969–978.
35. Pan Y, Heisig SR, von Blanckenburg P, et al. Facilitating adherence to endocrine therapy in breast cancer: stability and predictive power of treatment expectations in a 2-year prospective study. Breast Cancer Res Treat. 2018;168(3):667–677. doi:10.1007/s10549-017-4637-2
36. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;11:CD000011.
37. Zomahoun HTV, Guénette L, Grégoire JP, et al. Effectiveness of motivational interviewing interventions on medication adherence in adults with chronic diseases: a systematic review and meta-analysis. Int J Epidemiol. 2017;46(2):589–602. doi:10.1093/ije/dyw317
38. Ramirez AG, Wildes KA, Nápoles-Springer A, Pérez-Stable E, Talavera G, Rios E. Physician gender differences in general and cancer-specific prevention attitudes and practices. J Cancer Educ. 2009;24(2):85–93. doi:10.1080/08858190802664396
39. Jefferson L, Bloor K, Birks Y, Hewitt C, Bland M. Effect of physicians’ gender on communication and consultation length: a systematic review and meta-analysis. J Health Serv Res Policy. 2013;18(4):242–248. doi:10.1177/1355819613486465
40. Dirección General de Estadísticas y Censos Provincia de la Córdoba. [https://estadistica.cba.gov.ar/] Provincia de Córdoba según departamentos. Población según cobertura de salud en mujeres por grandes grupos de edad; 2010. Available from: https://datosestadistica.cba.gov.ar/dataset/cobertura-de-salud.
41. APROSS Cartilla de Prestadores – Oncología. Available from: http://www.apross.gov.ar/cartilla-de-prestadores.aspx. 2016.
42. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Huberman M, Miles M, editors. The Qualitative Researcher’s Companion. London: Sage; 2002:305–329.
43. Camacho FT, Tan X, Alcalá HE, Shah S, Anderson RT, Balkrishnan R. Impact of patient race and geographical factors on initiation and adherence to adjuvant endocrine therapy in Medicare breast cancer survivors. Medicine (Baltimore). 2017;96(24):e7147. doi:10.1097/MD.0000000000007147
44. Tan X, Camacho F, Marshall VD, Donohoe J, Anderson RT, Balkrishnan R. Geographic disparities in adherence to adjuvant endocrine therapy in Appalachian women with breast cancer. Res Social Adm Pharm. 2017;13(4):796–810. doi:10.1016/j.sapharm.2016.08.004
45. Engelhardt EG, Pieterse AH, van der Hout A, et al. Use of implicit persuasion in decision making about adjuvant cancer treatment: a potential barrier to shared decision making. Eur J Cancer. 2016;66:55–66. doi:10.1016/j.ejca.2016.07.011
46. The Economist Intelligence Unit. Cancer control, access and inequality in Latin America: a tale of light and shadow; 2017. Available from: https://perspectives.eiu.com/sites/default/files/Cancercontrol,accessandinequalityinLatinAmerica.pdf.
47. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365(9472):1687–1717. doi:10.1016/S0140-6736(05)66544-0
48. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Aromatase inhibitors versus tamoxifen in early breast cancer: patient-level meta-analysis of the randomised trials. Lancet. 2015;386(10001):1341–1352. doi:10.1016/S0140-6736(15)61074-1
49. Karanikolos M, Ellis L, Coleman MP, McKee M. Health systems performance and cancer outcomes. J Natl Cancer Inst Monogr. 2013;46:7–12. doi:10.1093/jncimonographs/lgt003
Supplementary materials
Interview question guide
- How do you consider patient adherence to AET in your clinic?
- Do you have access to data on adherence?
- What factors do you think can influence patients’ decision to adhere? (probes: information provided, cancer fear, trust in treatment).
- What factors do you think can influence patients’ decision to not initiate AET medication?
- Do patients discontinue medication before completing the 5 years? If so, can you identify their reasons? (probes side effects, socio-economic factors u others).
- How often do you see your patients after they are discharged from clinic?
- What are the main complaints regarding side effects that you receive from your patients? (probes physical symptoms, psychological symptoms).
- How do you manage patients’ complaints about medication? (probes change of drugs, social services, non-medical treatment).
These questions correspond to a section of the interview guide regarding adherence to treatments. These questions were preceded by a set of questions about oncologists prescribing AET by Eraso.1
Reference
1. Eraso Y. Factors influencing oncologists’ prescribing hormonal therapy in women with breast cancer: a qualitative study in Córdoba, Argentina. Int J Equity Health. 2019; 18(1):35. doi:10.1186/s12939-019-0936-z
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.