")
Back to Journals » Patient Preference and Adherence » Volume 14
Oncologist and Patient Preferences for Attributes of CDK4/6 Inhibitor Regimens for the Treatment of Advanced/Metastatic HR Positive/HER2 Negative Breast Cancer: Discrete Choice Experiment and Best–Worst Scaling
Authors Maculaitis MC, Liu X , Will O , Hanson M, McRoy L, Berk A, Crastnopol M
Received 21 March 2020
Accepted for publication 25 September 2020
Published 5 November 2020 Volume 2020:14 Pages 2201—2214
DOI https://doi.org/10.2147/PPA.S254934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Martine C Maculaitis,1 Xianchen Liu,2 Oliver Will,3 Madelyn Hanson,4 Lynn McRoy,2 Alexandra Berk,1 Melissa Crastnopol3
1Kantar, Health Division, New York, NY, USA; 2Pfizer Oncology, Pfizer Inc, New York, NY, USA; 3Kantar, Health Division, Horsham, PA, USA; 4Kantar, Health Division, St. Louis, MO, USA
Correspondence: Martine C Maculaitis
Kantar, Health Division, 175 Greenwich Street, 35th Floor, New York, NY 10007, USA
Tel +1 212-896-8184
Email [email protected]
Purpose: To understand and compare preferences for dosing- and toxicity-related attributes associated with selective cyclin-dependent 4/6 kinase inhibitors regimens among US oncologists and patients.
Materials and Methods: Oncologists and patients with mBC participated in an internet-based survey that included a discrete choice experiment (DCE) and a best–worst scaling (BWS) exercise. For the DCE, participants chose between two hypothetical treatment profiles, each with seven attributes: risk of dose reduction due to adverse events (AEs), risk of diarrhea, risk of abdominal pain, need for electrocardiogram (ECG) monitoring to assess heart function, risk of Grade 3/4 neutropenia, dosing regimen, and dosing schedule. The BWS exercise assessed the relative prioritization of a larger set of 16 attributes. Hierarchical Bayesian models were used to estimate preference weights for each attribute level.
Results: Oncologists (N=209) and patients (N=304) rated risks of diarrhea (25% each) and Grade 3/4 neutropenia (20% and 24%, respectively) as the most important attributes for treatment choice. The risks of diarrhea and Grade 3/4 neutropenia were 1.8 to 2.3 times (oncologists: 25% and 20%, respectively vs 11%) and 2.4 to 2.5 times (patients: 25% and 24%, respectively vs 10%) higher in relative importance than the risk of dose reduction due to AEs. Oncologists placed greater importance on the risk of dose reduction due to AEs and the need for ECG monitoring, whereas patients placed greater importance on the risk of Grade 3/4 neutropenia (all, p< 0.05). The BWS exercise results were largely consistent with those from the DCE.
Conclusion: The risks of diarrhea and Grade 3/4 neutropenia were key drivers of both oncologist and patient preferences. Overall, the palbociclib + aromatase inhibitor (AI) profile was most preferred, due to its association with a lower risk of diarrhea and no ECG monitoring, compared with abemaciclib + AI and ribociclib + AI profiles, respectively.
Keywords: adverse events, metastatic HR positive/HER2 negative breast cancer, selective cyclin-dependent 4/6 kinase inhibitors, stakeholder preferences, treatment administration, treatment choice
Introduction
Women in the United States (US) have a 12.4% lifetime risk of breast cancer (BC).1 BC risk has increased across the past four decades, which may be attributable to longer life expectancy, reproductive pattern changes, hormone use, higher obesity rates, and contributions from increased screening and detection.1 Up to 10% of initial BC diagnoses are metastatic at presentation, and roughly 30% of patients treated with endocrine therapy (ET) in the adjuvant setting eventually progress to metastatic disease.3 Overall five-year relative survival is 27% for those diagnosed with advanced or metastatic BC (mBC) in the US.2 Treatment for mBC continues as long as a patient is alive or elects only supportive care. For hormone receptor positive, HER2 negative (HR+/HER2-) mBC, ETs, namely selective estrogen receptor modulators (including tamoxifen), aromatase inhibitors (AIs), and selective estrogen receptor down regulators (including fulvestrant) are used for disease control, to delay the need for chemotherapy, and maintain quality of life (QoL).4
There has been considerable progress in treatment options for patients with HR+/HER2- mBC with the advent of a new class of drugs with selective inhibition of the cyclin-dependent 4/6 kinases (CDK4/6i; including palbociclib, ribociclib, and abemaciclib) now available to treat these patients.4 CDK4/6i regimens have been shown to improve overall survival, progression-free survival, and overall response rate in women with HR+/HER2- mBC, compared with ET alone.5–8 While all CDK4/6i have demonstrated efficacy in randomized controlled trials (RCTs), corresponding toxicities, dosing schedules, and label-required monitoring differ among the class.4,9–14 All CDK4/6i regimens have the dose-limiting toxicity of neutropenia and require regular complete blood counts. However, for abemaciclib, the risk of diarrhea determined the recommended dose in dose-finding studies. In RCTs, abemaciclib was associated with higher risk of thromboembolic disease, compared with the unexposed control arms.4,8 Ribociclib and abemaciclib also require regular monitoring of liver functions; ribociclib requires the monitoring of electrolytes and electrocardiograms (ECGs) to asses for prolongation of the QT interval, both prior to and during treatment, and is contraindicated for use with tamoxifen.
For the practicing oncologist, determining the optimal CDK4/6i regimen may be challenging. Often, comorbidities, physician familiarity, and physician preferences can determine which CDK4/6i regimen is selected.4 However, it is vital to consider patient values and preferences in treatment decisions.
Patients and physicians do not always share the same treatment values or preferences,15 and discrepancies in patient/physician views may predict lower treatment adherence.16 In turn, treatment nonadherence is associated with disease progression and mortality among patients with BC.17,18 Patient involvement in decision-making has been linked to better health outcomes and lower costs, as patients who were involved in the decision-making process, chose their treatment, or received their preferred treatment reported higher treatment satisfaction, higher rates of treatment completion, and better clinical outcomes across health conditions.19 Furthermore, greater healthcare engagement among patients is associated with lower medical costs over time via fewer emergency room visits and hospitalizations.20 Determining the extent to which patients and physicians are aligned in their preferences is warranted, particularly in an oncology setting, where available treatment options may be more limited, and it becomes increasingly important to understand what patients value and are willing to endure regarding toxicity risk and inconvenience.16
Prior research in the US and other countries has examined patient preferences regarding the characteristics of cancer treatments, including those with mBC or other advanced cancers.15,21–25 No studies to date have examined or compared the preferences of oncologists and patients regarding the clinical and non-clinical attributes of CDK4/6i regimens. A better understanding of oncologist and patient preferences may help to facilitate both clinical and payer decision-making regarding the selection of CDK4/6i regimens for HR+/HER2- mBC.
To potentially improve communication among oncologists and patients and to inform payer decisions regarding treatment for mBC, this study examined the treatment preferences of oncologists and patients with HR+/HER2- mBC, based on attributes associated with available CDK4/6i regimens. Specifically, this study sought to assess the trade-offs in benefits and risks that oncologists and patients are willing to accept, heterogeneity in preferences among oncologists and patients, and rank order of preferences for treatment attributes.
Materials and Methods
Data Source
The study was conducted in two phases and included four separate, but complementary, studies with oncologists and postmenopausal patients with HR+/HER2- mBC. Study data were collected in two phases: oncologist and patient responses in pilot interviews to test and refine the study instruments (phase 1), and oncologist and patient preferences reported in an online survey (Phase 2).
To be eligible, all participants were required to be able to read and understand English, able to operate a computer to access the online survey, located in the US, aged ≥18 years, and able and willing to provide informed consent. All eligible participants were contacted through e-mail. The study was conducted in accordance with the recommendations of the International Society for Pharmacoeconomics and Outcomes Research Good Research Practices for Conjoint Analysis Task Force.26 The study protocol was granted an exemption from full or expedited review by Pearl Institutional Review Board (Indianapolis, Indiana) prior to starting data collection based on FDA 21 CFR 56.104 and 45 CFR 46.104(b)(2). Participants provided their informed consent electronically.
Study Samples
The target sample sizes for patients and oncologists were first established by using the formula provided by Orme.27 Target sample sizes were further verified through a simulation study. Specifically, we simulated random choice for samples of the same size and fit a logit regression to the simulated data. This process confirmed that the errors for the preference levels were less than 0.05, which indicated that preference weights would be estimated with adequate precision.
Patients
Patients were recruited using convenience sampling from the Endeavour database, which accrues participants via referrals from physician sites and relationships with patient advocacy groups. Patient recruitment was concurrent with oncologist recruitment. Patient recruitment was also stratified with a mix of 109 patients on first line therapy (de novo Stage IIIB, IIIC, IV; previously-treated, recurrent Stage IIIB, IIIC, IV) and 195 patients on second or later line therapy. To be eligible to participate, patients were required to be female, diagnosed with HR+/HER2- mBC (stage IIIB, IIIC, IV), and postmenopausal. Patients who did not meet all inclusion criteria were considered ineligible.
Oncologists
Oncologists were recruited from Lightspeed Research’s All Global physician panel. All Global proprietary panel members are telephone-recruited to become members using hospital books and directories, medical directories, and yellow pages as original sample sources; panel demographics are generally representative of American Medical Association membership. Members undergo a double opt-in process, including a registration process followed by activation through email. To be eligible for the current study, oncologists were required to be board certified or board eligible, have been in practice between 2 and 35 years, spend at least 75% of time in direct patient care, have been providing services for ≥5 patients with mBC with systemic treatments at time of study participation, and have experience using CDK4/6i regimens. Oncologists who were unwilling or unable to comply with study procedures were excluded.
Measures
Variables included sociodemographic, disease, and treatment characteristics for patients, practice characteristics for oncologists, and treatment profile choices, as measured via discrete choice experiment (DCE) and best–worst scaling (BWS) exercise.
Study Design
Two preference elicitation methods using hypothetical scenarios that mimic real-world decision-making were employed (DCE and BWS). The use of two elicitation methods allowed insight into whether preference data would converge.
Discrete Choice Experiment
A DCE was used to assess patient and oncologist preferences regarding CDK4/6i + AI regimen attributes and levels. The DCE modeling approach is designed to assess respondents’ willingness to accept trade-offs among hypothetical treatment profiles providing information on key factors (eg, toxicities, efficacy, etc.) that drive treatment choice. DCE has a strong foundation in psychology and economics.28 This approach is based on the principle that treatment options can be decomposed into attributes of interest. The attractiveness of a treatment to individuals will depend on their relative preferences for these attributes, as expressed by the frequency with which they choose profiles with the preferred features; these values are then used to estimate the predictive probabilities that determine whether respondents will be more likely to choose one hypothetical treatment over another. Although there are alternatives for eliciting preferences (eg, revealed preferences, direct ratings/rankings, etc.), DCE is one of the most common approaches for assessing preferences in a healthcare context, and it has become of increasing interest to health authorities and clinicians to facilitate shared decision-making.29
In the DCE, participants considered two hypothetical CDK4/6i + AI regimen profiles, shown side-by-side, and were then asked to choose the one that they preferred. There was no “none” option, so the respondent was forced to make a choice. Each hypothetical treatment profile consisted of combinations of characteristics (“attributes”) and “levels” reflecting the attributes for each hypothetical treatment profile. Respondents’ selections allowed for an assessment of the trade-offs they were willing to make between positive and negative aspects of the treatment profiles. Respondents made several hypothetical treatment decisions over a series of scenarios involving two alternatives, which varied in the levels of each attribute. For example, one medication may have conferred a 33% risk of dose reduction due to AEs, while the other may have conferred a 45% risk. In total, each respondent saw 12 choice tasks. We used a balanced, overlap design to select what combination of levels were shown to a respondent. We generated more choice sets than respondents per survey, so that no respondent saw the same set of choice tasks.
The DCE method is superior to other approaches because it mimics a real-world situation where a medication’s attributes do not occur in isolation. For example, one must weigh both efficacy and toxicities simultaneously among available therapies when selecting treatment. In this study, the seven attributes and their corresponding levels for CDK4/6i + AI regimens (see Table 1) were carefully chosen based on clinical trial data, literature review, and qualitative interviews. No actual medication names were shown in the DCE. A sample DCE item is shown in Appendix 1. To help familiarize respondents with the DCE attributes and levels prior to completing the choice tasks, they were asked to rate the levels for each attribute on a scale from 1=very bad to 5=very good.
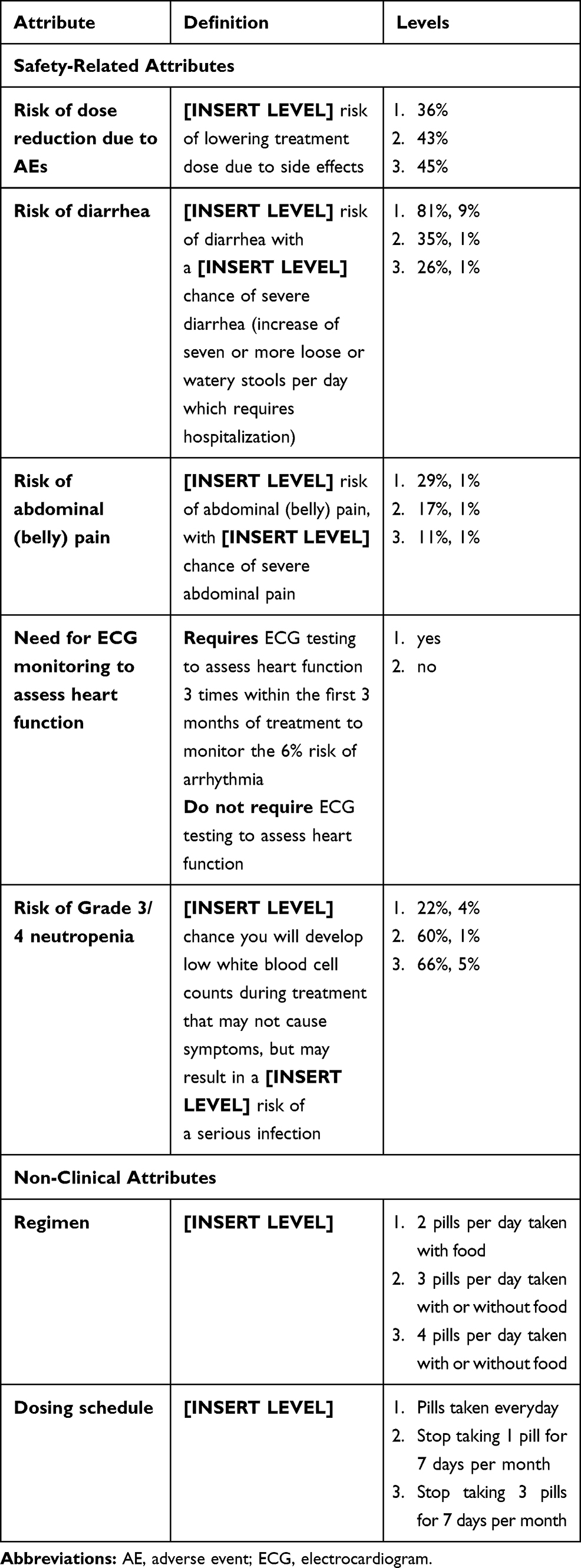 |
Table 1 Attributes and Levels Included in the DCE |
Best–Worst Scaling
Participants completed a separate BWS exercise, which enabled the ranking of a larger set of attributes in order of importance and included attributes associated with CDK4/6i + AI and CDK4/6i + fulvestrant regimens. There was some overlap between items in the DCE and BWS exercise, which provided the opportunity to examine multiple attributes and compare those that were in both exercises. In the BWS exercise, a list of 16 attributes was presented to oncologists and patients, four at a time. To avoid any bias due to ordering effects, randomization was used to select the four attributes in each set presented to respondents in the BWS exercise. The participants selected the most important and least important attribute from among the four presented.
Procedure
Phase 1, Survey Development
Survey content was pilot tested among oncologists and patients in a qualitative study via hour-long telephone interviews and a desktop sharing platform. Eight oncologists and eight patients completed the qualitative study. Interviews assessed comprehension of the DCE/BWS items and appropriate screening thresholds. Pre-testing of the online survey was also conducted to ensure that the language was appropriate for, and could be easily understood by, respondents. Based on qualitative interview results, the survey content was further refined.
Issues were identified among two patients in the comprehension of the instructions for the first task; specifically, they were unsure what we meant by “very bad/very good”. The final survey instructions were revised to clarify that “very good” means “very appealing”. As some respondents mistakenly thought they were supposed to rank the attributes in order of importance, even though they were instructed to rank the most and least important, we programmed the final survey to force respondents to select one attribute per column. After the pilot testing, we also added further details to describe the percentage risk of developing a serious infection after developing a low white blood cell count, as we believed that preferences would be more accurate if this risk was explicitly noted in the attribute definition.
Phase 2, Final Survey Administration
Potential participants were pre-screened for eligibility before being invited to participate in the study. In total, 488 oncologists and 400 patients were eligible to participate. Overall, 209 oncologists and 304 patients with mBC completed the final survey.
Statistical Analysis
Descriptive analyses were used to characterize the oncologist and patient samples. Descriptive statistics (means, standard deviations (SDs), medians, and interquartile ranges (IQR) for continuous variables and frequencies and percentages for categorical variables) were calculated for all study measures on the total samples of oncologists and patients. This analysis of the distributions was a part of testing of model assumptions and helped inform the appropriate modeling techniques.
For the DCE, to estimate preference weights for each attribute level, a hierarchical Bayesian (HB) model was fitted to the choice data. The fit for the HB model was done with a Markov Chain Monte Carlo. The underlying HB choice-probability model was conditional logit, using effects coding for the attribute levels. The results were then used to construct the joint posterior distribution of preference weights over the entire sample, including the mean and SD for each level. Independent-samples t-tests were used to evaluate whether the importance estimates differed across stakeholder groups. The BWS data were analyzed as frequencies.30 Specifically, two rates were calculated: the rate that the attribute was selected as the most important for considering a treatment and the rate that an attribute was selected as least important. The difference between these rates was used to rank order the attributes and to estimate the magnitude of attribute preference for oncologists and patients.
HB modeling was performed using Sawtooth’s Choice-Based Conjoint HB Lighthouse Studio software, 2018. Descriptive and bivariate analyses were performed using SPSS v23.0.
Relative Preference Weights for Each Attribute Level
Point estimates of HB model coefficients, representing mean utility weights at the aggregate level, SDs, and 95% confidence intervals, were calculated. The HB model produced utility estimates for each respondent. The 95% confidence interval was estimated from the individual utilities with a t-distribution. These utility weights measure relative preference; thus, only changes between attribute-level estimates and the relative size of those changes across attributes have meaningful interpretations. The magnitude of the trade-offs that stakeholders are willing to make among the attribute levels were assessed via these weights.
Relative Importance of Each Attribute
Relative importance estimates demonstrate the unique contribution of each attribute to the total utility of a treatment profile. These were calculated at the respondent level by dividing the range of each attribute (utility of the most favorable level minus utility of the least favorable level) by the sum of the ranges of all attributes and multiplying by 100 to convert to a percentage. The resulting estimates reflect the importance of each attribute, relative to the others. Importance estimates are ratio-scaled; an attribute with an importance of 20% is twice as important as an attribute with an importance of 10%.
Profile Comparisons
Participants evaluated three CDK4/6i + AI regimen profiles corresponding to the specific attributes and levels within the DCE. The utilities for each respondent were derived from their DCE data and then summed to compute a total mean utility for each profile. This enabled head-to-head comparisons of patient preferences among palbociclib + AI, abemaciclib + AI, and ribociclib + AI profiles.
Results
Oncologist Characteristics
Oncologist characteristics (N=209) are presented in Table 2. Most specialized in medical oncology (82.3%) and had been practicing for a median of 15.0 (IQR: 10.0–20.0) years. The largest proportion practiced in community-based private groups (42.5%) or academically-based practices (38.7%). Oncologists reported spending most of their time in direct patient care (93.3%), and they saw a median of 75.0 (IQR: 50.0–99.0) patients with BC during the past three months, including a median of 40.0 (IQR: 24.0–60.0) patients with mBC.
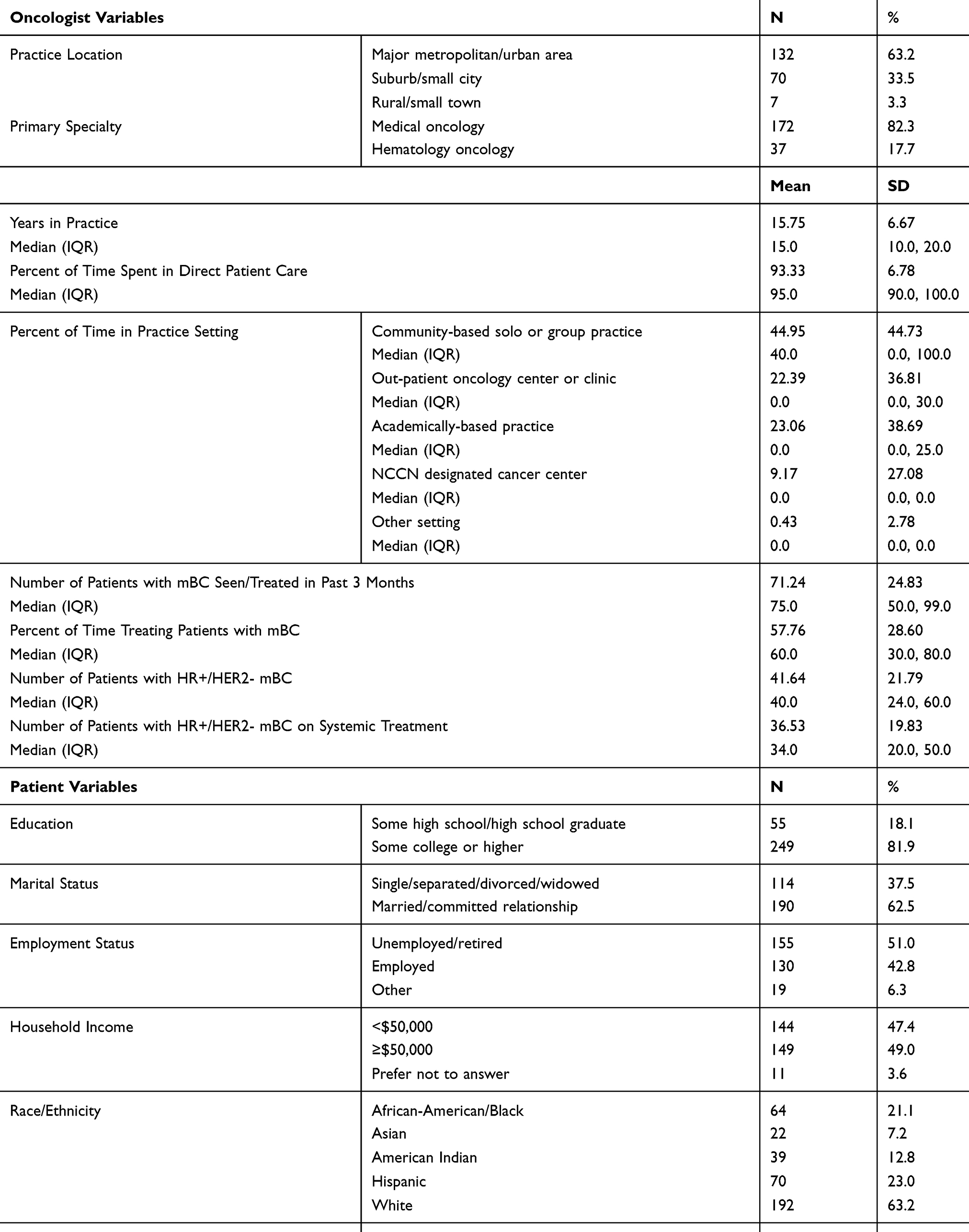 |
Table 2 Sample Characteristics |
Patient Characteristics
Patient characteristics (N=304) are shown in Table 2. The median age was 47.0 (IQR: 40.0–55.0) years old. Most were married/in a committed relationship (62.5%), White (63.2%), had completed at least some college (81.9%), were unemployed or retired (51.0%), and had a household income of ≥$50,000 (52.7%). Most (62.7%) had initially been diagnosed with BC between one to five years prior to study participation, and the cancer had become metastatic a median of 15.0 (IQR: 8.0–26.5) months from initial diagnosis.
Oncologist and Patient Preferences
Attribute level preference weights by stakeholder group are shown in Figure 1. Among oncologists, the difference between level estimates allowed for the evaluation of the effect of a change within an attribute. For example, lowering the risk of diarrhea/severe diarrhea from 81%/9% to 35%/1% (0.35-[−1.39]=1.74) outweighed lowering the risk of abdominal (belly) pain/severe abdominal pain from 29%/1% to 11%/1% (0.25-[−0.41]=0.66) in importance. Lowering the risk of Grade 3/4 neutropenia/serious infection from 60%/1% to 22%/4% was 6.8 times more important to treatment choice than lowering the risk of dose reduction due to AEs from 43% to 36% (0.88 vs 0.13). Lowering the risk of diarrhea/severe diarrhea from 81%/9% to 35%/1% was 2.1 times more influential to treatment choice than lowering the risk of Grade 3/4 neutropenia/severe infection from 66%/5% to 60%/1% (1.74 vs 0.82).
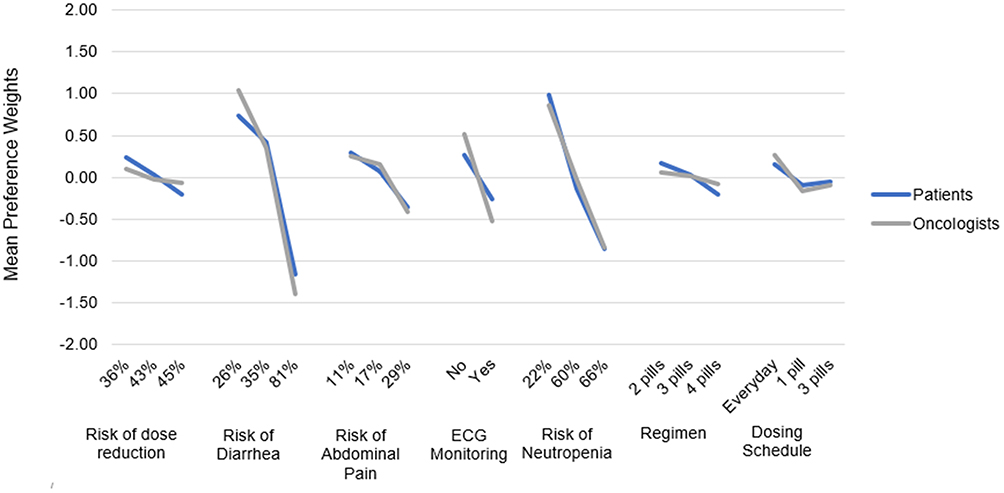 |
Figure 1 Attribute-level preference weights for oncologists and patients. |
A similar pattern of results was observed among patients. Specifically, lowering the risk of diarrhea/severe diarrhea from 81%/9% to 35%/1% was 2.2 times more important to treatment choice than lowering the risk of Grade 3/4 neutropenia/serious infection from 66%/5% to 60%/1% (1.58 vs 0.71) and 5.9 times more important than lowering the risk of dose reduction due to AEs from 43% to 36% (1.58 vs 0.27). Lowering the risk of Grade 3/4 neutropenia/serious infection from 60%/1% to 22%/4% was 4.2 times more important to treatment choice than lowering the risk of dose reduction due to AEs from 43% to 36% (1.13 vs 0.27). Appendix 2 shows estimates of the relative importance for each attribute by stakeholder group.
Overall, the risks of diarrhea/severe diarrhea and Grade 3/4 neutropenia/serious infection were rated as the most important attributes by both oncologists and patients, and these two attributes were each approximately twice as important as the other attributes included in the DCE. Compared with patients, oncologists rated dose reduction due to AEs (10% vs 11%), need for ECG monitoring to assess heart function (9% vs 11%), and regimen (9% vs 11%) as significantly more important (all, p<0.05). However, patients rated risk of Grade 3/4 neutropenia/serious infection as significantly more important than oncologists did (24% vs 20%, p<0.001). There were no significant differences by stakeholder group on the relative importance of risks of diarrhea/severe diarrhea or abdominal (belly) pain/severe abdominal pain.
Treatment Profile Comparisons
The treatment profiles for the three CDK4/6i + AI regimens are shown in Table 3. Abemaciclib + AI was associated with a lower preference weight than the other CDK4/6i + AI profiles on the risk of diarrhea/severe diarrhea, and palbociclib + AI and ribociclib + AI were associated with lower preference weights than the abemaciclib + AI profile on the risk of Grade 3/4 neutropenia/serious infection. Based on the total utility weights for each treatment profile, oncologists and patients preferred the overall combination of safety and non-clinical attributes associated with palbociclib + AI. However, the palbociclib + AI (0.97 vs 0.75) and ribociclib + AI (0.50 vs 0.17) profiles were more preferred by oncologists than patients (both, p<0.05).
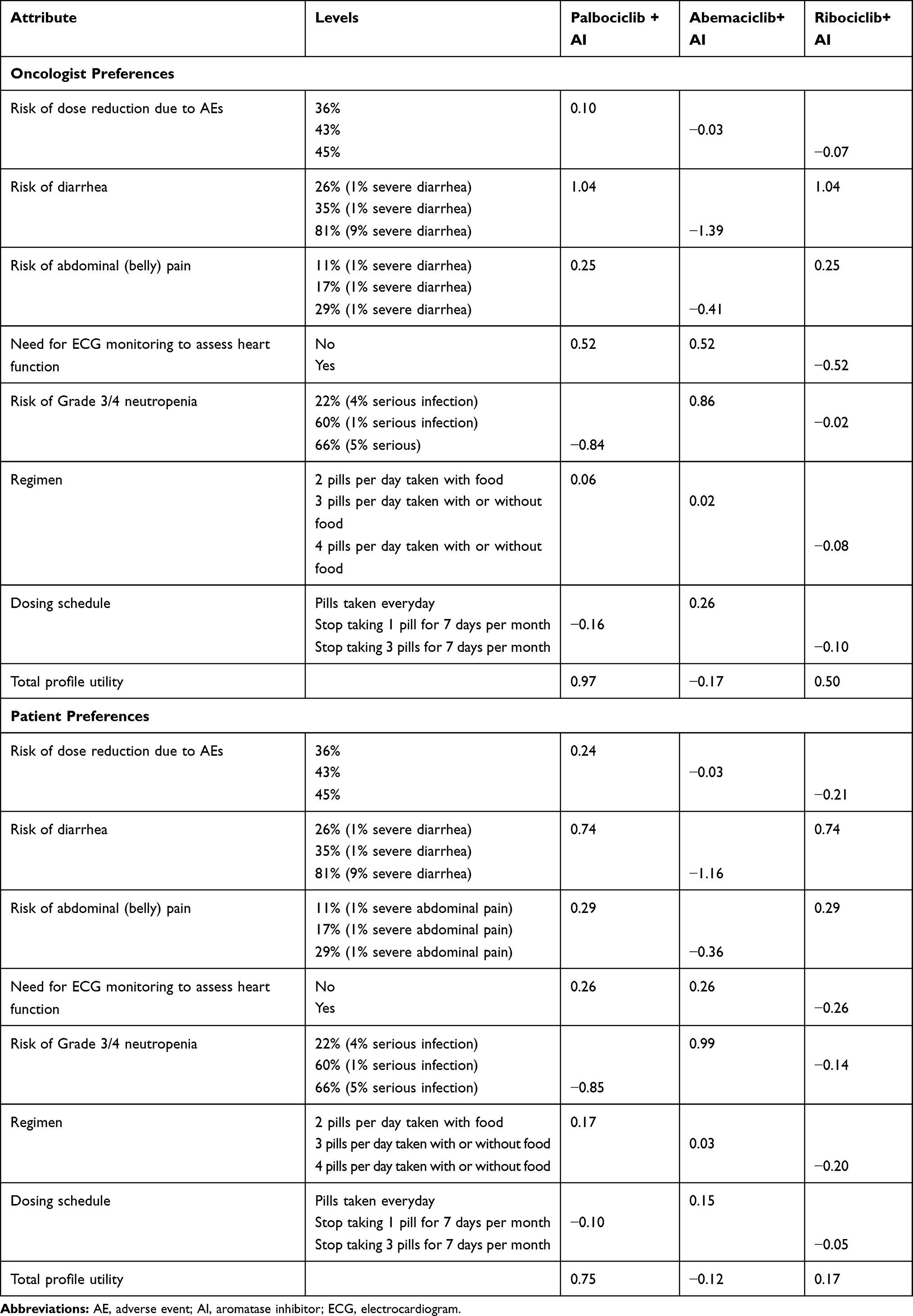 |
Table 3 Preferences Among Oncologists and Patients for Selected CDK4/6i Treatment Profiles |
Best–Worst Scaling
Figure 2 illustrates the BWS exercise results for patients and oncologists, which included attributes of CDK4/6i + AI and CDK4/6i + fulvestrant regimens. While lower risks of moderate diarrhea and Grade 3/4 neutropenia, which may lead to serious infection, were still near the top in importance for patients, three attributes that were not in the DCE were also rated as very high in importance: lower risk of heart dysfunction, which involves having a sudden irregular heartbeat, real-world effectiveness data are available, and patient-reported benefits have been published. For oncologists, the most important attributes were consistent with the results from the DCE. Specifically, lower risks of Grade 3/4 neutropenia, which may lead to serious infection, moderate diarrhea, and heart dysfunction, which involves having a sudden irregular heartbeat, were the top three most important attributes. Monitoring of liver function is required (16% vs 25%) and lower risks of moderate diarrhea (40% vs 32%) and heart dysfunction, which involves having a sudden irregular heartbeat (49% vs 42%), had the largest absolute differences in importance when comparing the ratings of oncologists and patients, respectively. However, these differences did not reach statistical significance.
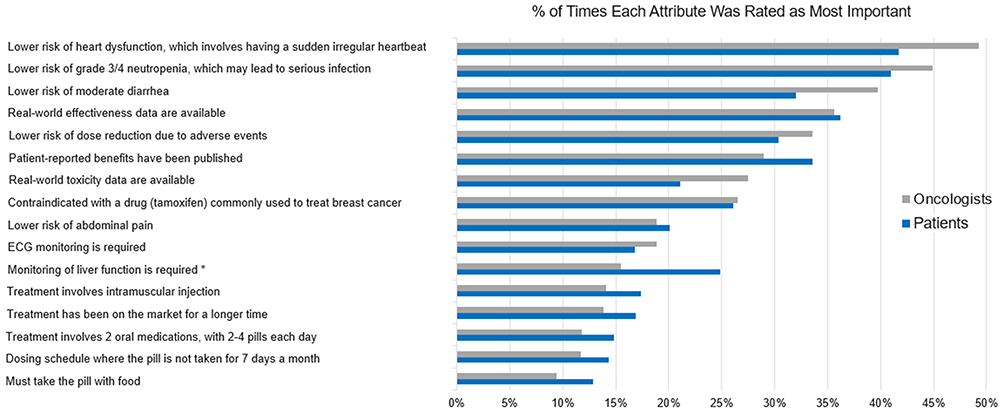 |
Figure 2 BWS exercise ratings for oncologists and patients. |
Discussion
For both oncologists and patients, the most important attributes for selecting from among currently available CDK4/6i + AI regimens were the risks of diarrhea and Grade 3/4 neutropenia, with diarrhea being the most important. Patients placed greater importance than oncologists on the risk of Grade 3/4 neutropenia, whereas oncologists placed greater importance than patients on the risk of dose reduction due to AEs and the need for ECG monitoring. Overall, the palbociclib + AI profile was most preferred, due to its association with a lower risk of diarrhea and no ECG monitoring, compared with abemaciclib + AI and ribociclib + AI profiles, respectively.
Among the attributes explored with the BWS exercise, the risks of Grade 3/4 neutropenia and diarrhea were perceived as near the top in importance by both stakeholder groups. However, oncologists also highly valued a lower risk of heart dysfunction, and patients also placed importance on the treatment having real-world effectiveness data and published patient-reported benefits. Findings regarding both preference “agreements” (risks of diarrhea and Grade 3/4 neutropenia being considered most important by both stakeholder groups) and “disagreements” (level of importance regarding: Grade 3/4 neutropenia, risk of dose reduction due to AEs, need for ECG monitoring, having real-world effectiveness data, and published patient-reported benefits) may potentially help facilitate fruitful conversations between oncologists and patients when selecting a CDK4/6i + AI regimen to treat mBC.
To our knowledge, this is the first study to assess treatment preferences of oncologists and patients with mBC across currently available CDK4/6i regimens. Oncologists’ preference for less risk of toxicities is not an unexpected finding and has been well documented in the literature.15,21,23,24,31 Little data are available regarding patient treatment preferences in the mBC setting. This examination of the decision-influencing attributes of CDK4/6i regimens supports the existing body of literature that describes oncologist and patient preferences for other treatments across cancer sites.
Results of the current study showed diarrhea to be one of the most important drivers of preferences for both stakeholder groups. Although infrequently life-threatening, treatment-induced diarrhea nevertheless has important implications, as it can frequently necessitate supportive therapy, dose reductions, treatment delays, switches, and discontinuations.32 Moreover, among patients using systemic cancer therapy, experiencing moderate to severe diarrhea (vs no diarrhea) was associated with significantly worse QoL.21 Dosing frequency was not a key factor in patient and oncologist preferences, which further supports the finding that toxicity-related attributes primarily underlie stakeholder preferences among available CDK4/6i regimens.
When treatment decisions are aligned with patient preferences, patients report higher treatment satisfaction and adherence and have better clinical outcomes.19 Prior longitudinal research has found that oncologists, relative to their patients with advanced cancer, place stronger emphasis on survival (vs QoL) as the treatment goal that would be best for patients.33 A systematic literature review of prior DCE studies across 26 disease conditions (including eight types of cancer) reported that mortality was more important to healthcare providers, while medication safety, delivery and timing of treatment, and treatment accessibility were more important to patients.34 Thus, prior research suggests that patients prioritize treatment aspects that can impact their QoL, whereas physicians may prioritize prolonging a patient’s life;19,33,34 this discordance has implications in the metastatic setting, as patients may potentially be less willing to endure inconvenient treatment regimens with high toxicity risks that could negatively impact the quality of their remaining time. Although there was largely agreement in stakeholder preferences in this study, oncologists should consider those treatment aspects that are most important to patients when making treatment recommendations. Moreover, patients who are more engaged in decisions about their healthcare have fewer emergency room visits and hospitalizations over time.20 This suggests that including the patient perspective in treatment decision-making may also help to reduce healthcare expenditures, especially those incurred from high-cost medical events.
Limitations
Younger patients and those interested in research may have been more likely to participate in the study. The average age of participants in this study is significantly younger than the average age of a patient with mBC in the US, limiting the generalizability of the results. Therefore, results may not generalize to the entire population of patients with mBC and/or to the population of oncologists who treat these patients. The DCE also may not reflect the same clinical, financial, or emotional consequences of actual decisions, although the DCE was carefully designed to include the feedback of the stakeholder groups of interest, to mimic realistic treatment choices, and to closely align with clinical evidence. BWS is also purported to be an “easier” task comparatively, although this issue was addressed by including two preference elicitation methods to determine the convergence of results. Discrepancies between DCE and BWS results may also reflect that the former only included CDK4/6i + AI regimen attributes, whereas the latter additionally included attributes of CDK4/6i + fulvestrant regimens.
Stated preferences may differ from actual treatment decisions. Moreover, all study variables were reported directly from participants without independent verification; it is possible that patients may have an incomplete understanding of the attributes presented. Self-reported data may potentially be subject to response bias, which can increase measurement error. Because the rate of any grade diarrhea is much higher than that of Grade 3/4, this may have resulted in the overestimation of the importance of the risk of diarrhea, relative to the risk of Grade 3/4 neutropenia, particularly among patients. Oncologists’ relative ranking of these two attributes may reflect that Grade 3/4 neutropenia is typically asymptomatic, while patients may not be aware of whether or not symptoms are associated with this AE.
Cost data were not included in the DCE or BWS. Cost can be a predominant factor in treatment choice, thereby greatly overshadowing the effects of other attributes in the model, resulting in biased estimates. Efficacy data were likewise not included in the DCE or BWS, as CDK4/6i + AI regimens were assumed to have similar efficacy, based on clinical data available when the study was conducted. However, we cannot exclude the possibility that incorporating both efficacy and toxicity-related attributes would have a more meaningful impact on stakeholder preferences. Additionally, it is possible that estimated preferences for the CDK4/6i regimens of interest could differ from those observed had we included an alternative to opt-out of treatment in the choice tasks. Future research should ascertain whether those individuals who would choose to opt-out of mBC treatment systematically differ in demographics, clinical status, attitudes, and other characteristics from those would not opt-out of treatment.
Conclusions
For patients and physicians, the risks of diarrhea and Grade 3/4 neutropenia were the most important attributes driving treatment preferences. The results of the DCE and BWS exercise largely converged regarding the attributes most valued by oncologists and patients. When considering all attributes collectively, the palbociclib + AI profile was most preferred, overall, due to its association with a lower risk of diarrhea and no ECG monitoring, compared with abemaciclib + AI and ribociclib + AI profiles, respectively. Patients and oncologists were willing to make similar trade-offs in potential risks and benefits associated with different treatment profiles, although results revealed subtle differences in attribute importance. This study’s findings highlight the importance of understanding oncologist and patient preferences when making mBC treatment decisions in clinical practice.
Abbreviations
AE, adverse event; AI, aromatase inhibitor; BC, breast cancer; BWS, best–worst scaling; CDK4/6i, selective cyclin-dependent 4/6 kinase inhibitor; DCE, discrete choice experiment; ECG, electrocardiogram; ET, endocrine therapy; HB, hierarchical Bayesian; HR+, hormone receptor positive; IQR, interquartile range; mBC, metastatic breast cancer; NCCN, National Comprehensive Cancer Network; QoL, quality of life; RCT, randomized clinical trial; SD, standard deviation; US, United States.
Data Sharing Statement
Upon request, and subject to certain criteria, conditions, and exceptions (see https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information), Pfizer will provide access to individual de-identified participant data from Pfizer-sponsored global interventional clinical studies conducted for medicines, vaccines, and medical devices (1) for indications that have been approved in the US and/or EU or (2) in programs that have been terminated (ie, development for all indications has been discontinued). Pfizer will also consider requests for the protocol, data dictionary, and statistical analysis plan. Data may be requested from Pfizer trials 24 months after study completion. The de-identified participant data will be made available to researchers whose proposals meet the research criteria and other conditions, and for which an exception does not apply, via a secure portal. To gain access, data requestors must enter into a data access agreement with Pfizer.
Acknowledgments
The authors acknowledge Ernest Law (Pfizer Inc.) for his feedback on the manuscript draft, Jeffrey Trocio (Pfizer Inc.) and Colleen M. Carpinella (Kantar) for their assistance developing the study design, and Schuler Research, LLC for assistance with the literature review. A portion of the results reported on in this manuscript were presented at the 36th Annual Miami Breast Cancer Conference, which was held March 7–10, 2019 in Miami Beach, Florida, and at the Academy of Managed Care Pharmacy (AMCP) Nexus Conference, which was held October 29-November 1, 2019 in National Harbor, MD.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was sponsored by Pfizer.
Disclosure
Martine C. Maculaitis, Oliver Will, Madelyn Hanson, Alexandra Berk, and Melissa Crastnopol are employees of Kantar, who were paid consultants to Pfizer in connection with the development of this manuscript. Xianchen Liu and Lynn McRoy are employees of Pfizer. The authors report no other conflicts of interest in this work.
References
1. American Cancer Society. Breast cancer facts & figures 2017–2018. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-facts-and-figures/breast-cancer-facts-and-figures-2017-2018.pdf.
2. American Cancer Society. Survival rates for breast cancer. Available from: https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/breast-cancer-survival-rates.html.
3. Reinert T, Barrios CH. Optimal management of hormone receptor positive metastatic breast cancer in 2016. Ther Adv Med Oncol. 2015;7(6):304–320. doi:10.1177/1758834015608993
4. Ballinger TJ, Meier JB, Jansen VM. Current landscape of targeted therapies for hormone-receptor positive, HER2 negative metastatic breast cancer. Front Oncol. 2018;8:1–11. doi:10.3389/fonc.2018.00308
5. Finn RS, Crown JP, Lang I, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015;16(1):25–35. doi:10.1016/S1470-2045(14)71159-3
6. Turner NC, Ro J, André F, et al. Palbociclib in hormone-receptor–positive advanced breast cancer. N Engl J Med. 2015;373(17):209–219. doi:10.1056/NEJMoa1505270
7. Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18):1738–1748. doi:10.1056/NEJMoa1609709
8. Boyle F, Beith J, Burslem K, et al. Hormone receptor positive, HER2 negative metastatic breast cancer: impact of CDK4/6 inhibitors on the current treatment paradigm. Asia-Pac J Clin Oncol. 2018;14:3–11. doi:10.1111/ajco.13064
9. Abraham J, Coleman R, Elias A, Holmes F, Kalinsky K, Kittaneh M. Use of cyclin-dependent kinase (CDK) 4/6 inhibitors for hormone receptor-positive, human epidermal growth factor receptor 2-negative, metastatic breast cancer: a roundtable discussion by The Breast Cancer Therapy Expert Group (BCTEG). Breast Cancer Res Treat. 2018;171(1):11–20. doi:10.1007/s10549-018-4783-1
10. Guo Q, Lin X, Ye L, et al. Comparative efficacy of CDK4/6 inhibitors plus aromatase inhibitors versus fulvestrant for the first-line treatment of hormone receptor-positive advanced breast cancer: a network meta-analysis. Target Oncol. 2019;14(2):139–148. doi:10.1007/s11523-019-00633-9
11. Ding W, Li Z, Wang C, Ruan G, Chen L, Tu C. The CDK4/6 inhibitor in HR-positive advanced breast cancer: a systematic review and meta-analysis. Medicine (Baltimore). 2018;97(20):e10746. doi:10.1097/MD.0000000000010746
12. Petrelli F, Ghidini A, Pedersini R, et al. Comparative efficacy of palbociclib, ribociclib and abemaciclib for ER+ metastatic breast cancer: an adjusted indirect analysis of randomized controlled trials. Breast Cancer Res Treat. 2019;174(3):597–604. doi:10.1007/s10549-019-05133-y
13. Ramos-Esquivel A, Hernández-Steller H, Savard MF, Landaverde DU. Cyclin-dependent kinase 4/6 inhibitors as first-line treatment for post-menopausal metastatic hormone receptor-positive breast cancer patients: a systematic review and meta-analysis of Phase III randomized clinical trials. Breast Cancer. 2018;25(4):479–488. doi:10.1007/s12282-018-0848-6
14. Im SA, Lu YS, Bardia A, et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N Engl J Med. 2019;381:307–316. doi:10.1056/NEJMoa1903765
15. Krammer R, Heinzerling L, Slominski AT. Therapy preferences in melanoma treatment - willingness to pay and preference of quality versus length of life of patients, physicians and healthy controls. PLoS One. 2014;9:11. doi:10.1371/journal.pone.0111237
16. DiBonaventura MD, Copher R, Basurto E, Faria C, Lorenzo R. Patient preferences and treatment adherence among women diagnosed with metastatic breast cancer. Am Heal Drug Benefits. 2014;7(7):386–396.
17. Hershman DL, Shao T, Kushi LH, et al. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res Treat. 2011;126(2):529–537. doi:10.1007/s10549-010-1132-4
18. Chirgwin JH, Giobbie-Hurder A, Coates AS, et al. Treatment adherence and its impact on disease-free survival in the breast international group 1-98 trial of tamoxifen and letrozole, alone and in sequence. J Clin Oncol. 2016;34(21):2452–2459. doi:10.1200/JCO.2015.63.8619
19. Lindhiem O, Bennett CB, Trentacosta CJ, McLear C. Client preferences affect treatment satisfaction, completion, and clinical outcome: a meta-analysis. Clin Psychol Rev. 2014;34(6):506–517. doi:10.1016/j.cpr.2014.06.002
20. Greene J, Hibbard JH, Sacks R, Overton V, Parrotta CD. When patient activation levels change, health outcomes and costs change, too. Health Aff. 2015;34(3):431–437. doi:10.1377/hlthaff.2014.0452
21. Liu FX, Witt EA, Ebbinghaus S, et al. Patient and oncologist preferences for attributes of treatments in advanced melanoma: a discrete choice experiment. Patient Prefer Adherence. 2017;14:1389–1399. doi:10.2147/PPA.S140226
22. Uemura H, Matsubara N, Kimura G, et al. Patient preferences for treatment of castration-resistant prostate cancer in Japan: a discrete-choice experiment. BMC Urol. 2016;16:63–72. doi:10.1186/s12894-016-0182-2
23. Kunneman M, Pieterse AH, Stiggelbout AM, et al. Treatment preferences and involvement in treatment decision making of patients with endometrial cancer and clinicians. Br J Cancer. 2014;111(4):674–679. doi:10.1038/bjc.2014.322
24. Kilbridge KL, Weeks JC, Sober AJ, et al. Patient preferences for adjuvant interferon alfa-2b treatment. J Clin Oncol. 2001;19(3):812–823. doi:10.1200/JCO.2001.19.3.812
25. Wong Y-N, Egleston BL, Sachdeva K, et al. Cancer patients’ trade-offs among efficacy, toxicity, and out-of-pocket cost in the curative and noncurative setting. Med Care. 2013;51(9):838–845. doi:10.1097/MLR.0b013e31829faffd
26. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Heal. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
27. Orme B. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research.
28. McFadden D. Conditional logit analysis of qualitative choice behavior. In: Zarembka P, editor. Frontiers in Econometrics. New York: Academic Press; 1974:104–142.
29. Clark MD, Determann D, Petrou S, Moro D, de Bekker-grob EW. Discrete choice experiments in health economics: a review of the literature. Pharmacoeconomics. 2014;32:883–902.
30. McIntosh E, Louviere J Separating weight and scale value: an exploration of best-attribute scaling in health economics.
31. Shafey M, Lupichuk SM, Do T, Owen C, Stewart D. Preferences of patients and physicians concerning treatment options for relapsed follicular lymphoma: a discrete choice experiment. Bone Marrow Transplant. 2011;46(7):962–969. doi:10.1038/bmt.2010.225
32. Arbuckle RB, Huber SL, Zacker C. The consequences of diarrhea occurring during chemotherapy for colorectal cancer: a retrospective study. Oncologist. 2000;5(3):250–259. doi:10.1634/theoncologist.5-3-250
33. Douglas SL, Daly BJ, Meropol NJ, Lipson AR. Patient-physician discordance in goals of care for patients with advanced cancer. Curr Oncol. 2019;26(6):370–379. doi:10.3747/co.26.5431
34. Harrison M, Milbers K, Hudson M, Bansback N. Do patients and health care providers have discordant preferences about which aspects of treatments matter most? Evidence from a systematic review of discrete choice experiments. BMJ Open. 2017;7(5):e014719. doi:10.1136/bmjopen-2016-014719
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.