")
Back to Journals » Patient Preference and Adherence » Volume 13
Once-Monthly Subcutaneously Administered Risperidone in the Treatment of Schizophrenia: Patient Considerations
Authors Tchobaniouk LV , McAllister EE , Bishop DL, Carpentier RM, Heins KR , Haight RJ, Bishop JR
Received 7 September 2019
Accepted for publication 3 December 2019
Published 12 February 2020 Volume 2019:13 Pages 2233—2241
DOI https://doi.org/10.2147/PPA.S192418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lesia V Tchobaniouk,1 Erin E McAllister,2 Danielle L Bishop,3 Rachel M Carpentier,4 Katharine R Heins,4 Robert J Haight,5 Jeffrey R Bishop6,7
1Department of Pharmacy, North Memorial Health Hospital, Robbinsdale, MN, USA; 2Department of Pharmacy, Clement J. Zablocki VA Medical Center, Milwaukee, WI, USA; 3Department of Pharmacy, M Health Fairview St. Joseph’s Hospital, St. Paul, MN, USA; 4Department of Pharmacy, Fairview Pharmacy Services, Minneapolis, MN, USA; 5Pharmacy Services, University of Minnesota Medical Center, Minneapolis, MN, USA; 6Department of Experimental and Clinical Pharmacology, College of Pharmacy, University of Minnesota, Minneapolis, MN, USA; 7Department of Psychiatry, Medical School, University of Minnesota, Minneapolis, MN, USA
Correspondence: Jeffrey R Bishop
Department of Experimental and Clinical Pharmacology, College of Pharmacy, University of Minnesota, Minneapolis, MN, USA
Email [email protected]
Abstract: Adherence to antipsychotic medications is a major challenge in schizophrenia. Long-acting injectable antipsychotics have been shown to offer advantages over oral formulations. A new extended release formulation of risperidone for subcutaneous injection was developed to address issues of non-adherence. The aim of this manuscript was to compare the new subcutaneous formulation to currently available formulations of injectable risperidone and paliperidone to determine whether the novel delivery by subcutaneous injection may provide substantial benefits. A literature search was conducted using PubMed, OVID, and Cochrane Library electronic databases to assess the advantages and disadvantages of long-acting formulations of risperidone. Potential advantages of risperidone for subcutaneous injection include a simplified dosing and ease of administration. Potential disadvantages include injection site pain and medication cost.
Keywords: adherence, long-acting injections, antipsychotic medications, RBP-7000, risperidone
Introduction
Schizophrenia is a severe and chronic mental disorder associated with cognitive, behavioral, and emotional dysfunction.24 Recurrent episodes are associated with progressive psychosocial deterioration, reduced treatment response, family and societal burden, and reduced quality of life.18 Antipsychotic medications are the primary treatment for schizophrenia and continuous, long-term treatment and adherence has shown improvements in clinical symptoms and functioning.24
Medication non-adherence is a major barrier to treatment and is associated with a higher risk of relapse and subsequent hospitalization.36 Researchers have found non-adherence rates to oral antipsychotics as high as 40–57%.4,8,21 Long-acting injectable antipsychotics (LAIAs) were developed as an alternative method of drug delivery to improve adherence. Current expert consensus and treatment guidelines recommend LAIAs as an option for maintenance treatment and in patients with recurrent relapses related to poor adherence.19,22,24 LAIAs may also be advantageous for patients in the early course of their illness due to a higher risk of relapse.33
Tiihonen and colleagues found only 58.2% of the patients with first-episode schizophrenia filled a prescription for their initial antipsychotic and 45.7% continued their treatment for 30 days or longer after hospital discharge (n = 2588).33 Weiden and colleagues identified high acceptance rates (73%) in first episode schizophrenia participants randomized to receive the option of long-acting risperidone through IM injection as compared to an oral antipsychotic, and higher adherence rates in those who accepted the LAIA option.35
LAIAs have several advantages compared to oral antipsychotics, including consistent pharmacokinetics and plasma levels, avoidance of first-pass metabolism, and less frequent drug administration. Patient preferences for LAIAs are, in part, dependent on their experiences with the formulations. Patients who tried LAIAs preferred these formulations over oral, stating they “feel better,” have a more “normal life” and felt injections were “easier to remember”.5,11,25–27,32,34 Nine LAIAs are available in the United States and can be administered every 2–12 weeks depending on their specific pharmacokinetics and dosing recommendations (Table 1).1,2,10,12,13,28–30,37 Second-generation LAIAs are generally preferred due to the lower risk of extrapyramidal side effects compared to first-generation agents.6
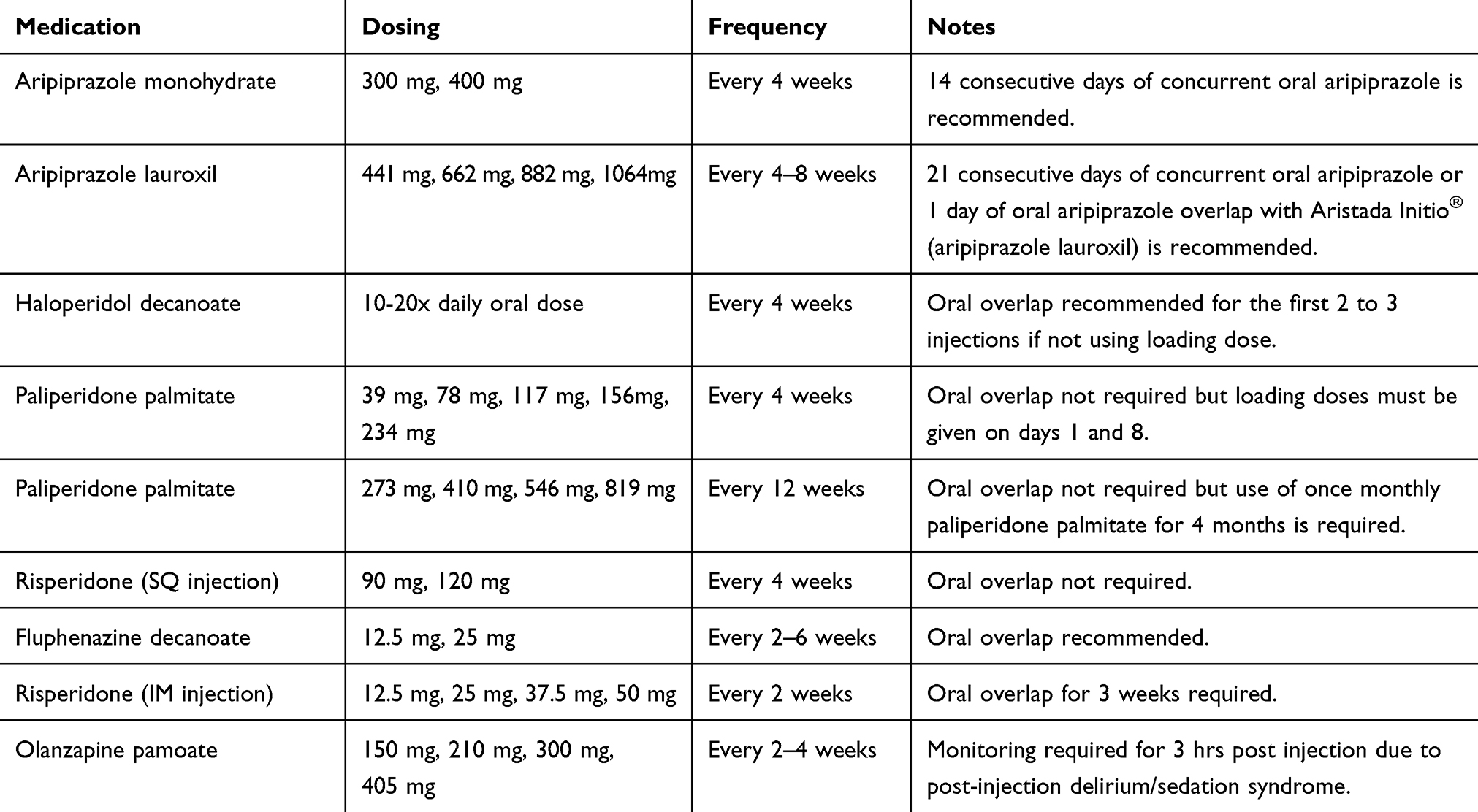 |
Table 1 Dosing Strategies of Long-Acting Injectable Antipsychotics Currently Available on the Market |
Risperidone was the first second-generation antipsychotic approved as an intramuscular (IM) depot injection given every 2 weeks (henceforth noted as risperidone-IM).30 The delivery system utilizes microspheres to provide a delayed release formulation with less than 1% of the total dose released at the time of injection.21 The microspheres must be reconstituted in diluent before being injected. Oral supplementation is required for at least 3 weeks after the first injection.21 Paliperidone (9-hydroxyrisperidone), the primary active metabolite of risperidone, was developed into two LAI formulations that can be administered through IM injection either monthly or every 3 months.12 One-month paliperidone palmitate requires two loading doses to be given on day 1 and day 8 to diminish the need for oral supplementation at the beginning of therapy.12 Three-month paliperidone palmitate is only indicated for patients who have been adequately treated for at least 4 months with 1-month paliperidone palmitate.13
While the availability of second-generation LAIAs was a significant therapeutic advance, the delayed onset of release of risperidone-IM and complicated dosing requirements with paliperidone palmitate presented a significant challenge in the transition to these formulations from oral medication. A new extended release formulation of risperidone for subcutaneous (SQ) injection was approved in July 2018 for the treatment of schizophrenia.45 The aim of this review is to compare the currently available formulations of injectable risperidone to determine whether the novel delivery by SQ injection may provide substantial benefits.
Methods
A literature search of clinical trials between January 2009 and November 2019 was conducted using the search terms “RBP-7000 and Perseris” in the PubMed, OVID Medline, and Cochrane Library electronic databases. Additional sources of information included the manufacturer package insert.
A total of 13 articles were found on PubMed, 12 on OVID Medline, 0 on Cochrane Library databases. Duplicates, articles not in English, and News articles were removed (n = 12), leaving 13 articles. The authors then reviewed the articles for relevance to the subject of schizophrenia. One paper that focused on therapeutic drug monitoring studies for risperidone-IM and a paper on dose equivalents for injectable IM antipsychotics was excluded. A total of 11 articles remained.
Drug Properties
Pharmacokinetics
Long-acting risperidone for subcutaneous injection (henceforth noted as risperidone-SQ) uses the ATRIGEL® delivery system.9 This system contains a biodegradable copolymer, poly D,L-lactide-co-glycolide, and biocompatible solvent, N-methyl-2-pyrrolidone.9 When mixed with risperidone powder a polymeric solution containing both dissolved and suspended risperidone is created.9,14 Upon contact with body fluids, the solvent dissipates and the copolymer solidifies into a biodegradable depot.21,43 The depot degrades over time to allow a sustained-release of risperidone.21,43 In contrast, risperidone-IM utilizes a microsphere delivery system with less than 1% of the total dose released at the time of injection.21
Risperidone-SQ has two absorption peaks following injection, both of similar magnitude.20,21 The first peak occurs 4 to 6 hrs post-injection as a result of an initial release of the risperidone from the depot.14,28 The second peak occurs 10 to 14 days post-injection due to the delayed release of risperidone from the depot.14,28 The active metabolite of risperidone, 9-hydroxyrisperidone, also has two absorption peaks.20,21 The first peak occurs 4 to 48 hrs post-injection and the second peak occurs 7 to 11 days post-injection.20,21 Steady-state plasma concentrations are reached by the end of the second injection and maintained for at least 4 weeks after the last injection.20
After injection, the volume of distribution for risperidone is large.28 There is a high degree of protein binding to both albumin and α1-acid glycoprotein.28 Risperidone is extensively metabolized in the liver via cytochrome CYP2D6 with minor metabolism by CYP3A4.28 The half-life of risperidone is 9 to 11 days and 8 to 9 days for 9-hydroxyrisperidone.28 Elimination occurs primarily through the urine, and to a much lesser extent, through the feces.28 Age, sex, and race were not found to have a clinically meaningful effect on the pharmacokinetics.28
Dosing and Administration
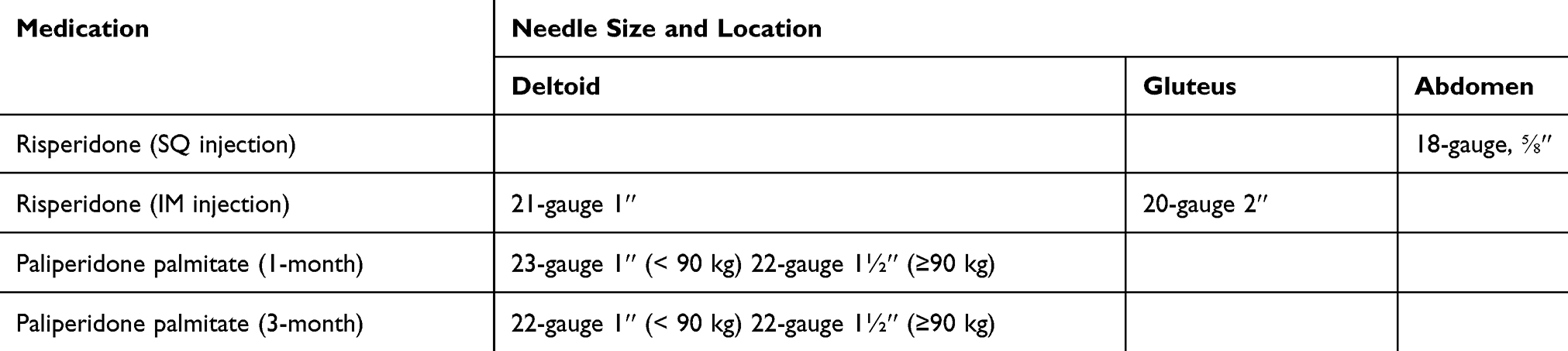
Risperidone-SQ is supplied as an injection kit consisting of two syringes.28 One syringe contains the ATRIGEL® delivery system, a liquid copolymer dissolved in the water-miscible solvent, while the other syringe contains risperidone powder.28 Similar to risperidone-IM, the SQ formulation of risperidone must be refrigerated and allowed to come to room temperature for at least 15 mins before mixing.28,44 Only a health-care professional can administer risperidone-SQ into the abdomen using an 18-gauge, 5/8-in. length needle.28 Regarding missed doses, the patient is instructed to receive the next dose as soon as possible.28
In contrast to the IM formulations of risperidone and paliperidone, the SQ formulation of risperidone does not require oral supplementation or loading doses (Table 1).28 However, it is recommended to establish tolerability with oral risperidone prior to starting treatment for risperidone-naive patients.28 After tolerability is established, risperidone-SQ can be dosed monthly, with either a 90-mg or 120-mg dose.28 The 90-mg dose corresponds to 3 mg/day of oral risperidone while the 120-mg dose corresponds to 4 mg/day of oral risperidone (Table 2).28 Conversion from oral risperidone at doses lower than 3 mg/day or higher than 4 mg/day have not been studied.28 Patients stable on these doses may not be candidates for risperidone-SQ. There is no dosage adjustment based on renal impairment, hepatic impairment, or the phenotypic variation in CYP2D6 enzyme metabolism.28
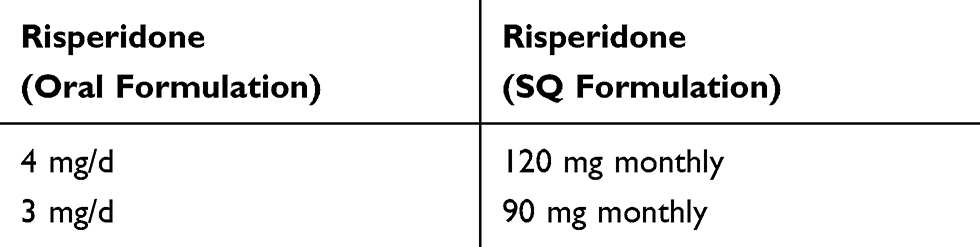 |
Table 2 Dose Conversion from Oral Risperidone to Subcutaneously Administered Long-Acting Risperidone |
Clinical Studies
Efficacy Assessments
An 8-week randomized, double-blind, placebo-controlled study (NCT02109562) evaluated the efficacy and safety of risperidone-SQ (formerly RBP-7000) in acutely ill patients with schizophrenia.23 Patients, age 18 to 55 years, were randomized to receive monthly treatment with 90- or 120-mg of RBP-7000 or placebo in an inpatient setting.23 Inclusion criteria included a diagnosis of acute exacerbation of schizophrenia, a Positive and Negative Syndrome Scale (PANSS) total score between 80 and 120, and a score of >4 or ≥2 of the following 4 PANSS items: hallucinatory behavior, delusions, conceptual disorganization, or suspiciousness/persecution.23 Excluded were patients that had been treated with clozapine at any time for treatment-resistant schizophrenia, were taking ≥6 mg/day of oral risperidone, met the criteria for substance dependence, or had ≥20% improvement in their PANSS total score between the initial screening visit and the day of the first injection.23 During the initial screening period (week prior to Day 1) patients were tapered off their current oral antipsychotic(s) and received a 0.25-mg of oral risperidone for two consecutive days to assess tolerability.23 Clinical assessment for efficacy included the PANSS rating scale, as the primary outcome measure, and the Clinical Global Impression-Severity (CGI-S) rating scale, as the secondary outcome measure.23 A total of 354 patients were randomized to receive 90 mg of RBP-7000 (n=116), 120 mg of RBP-7000 (n=119), or the delivery system only as a placebo group (n=119).23
Both RBP-7000 groups were superior to the placebo group and showed significant improvement in the mean change from baseline in the PANSS total scores (−6.1 and −7.2 points for the 90- and 120-mg groups, respectively) at each time point (Days 15, 29, 43, and at the end of the study).23 Both RBP-7000 groups also showed significant improvement on the CGI-S total scores compared to placebo (−0.35 and −0.40 points for the 90-mg and 120-mg groups, respectively).23 Additional analysis showed significant advantages of the RBP-7000 groups compared to placebo for the PANSS positive and general psychopathology subscales, but not for the PANSS negative subscale.23 Discontinuation rates were lower for both RBP-7000 groups compared to placebo (22.4%, 28.6%, 29.4% for the 90-mg, 120-mg RBP-7000 groups, and placebo group, respectively).23 The most common reason for discontinuation was withdrawal of consent (17.2%, 21%, and 17.6% in the 90-mg, 120-mg RBP-7000 groups, and placebo group, respectively).23 In contrast, the discontinuation rate due to insufficient clinical response was low for all groups (1.7%, 0%, and 3.4% in the 90-mg, 120-mg RBP-7000 groups, and placebo group, respectively).23
Long-term effectiveness was assessed in a 52-week, multi-center, Phase 3, open-label, outpatient study (NCT02203838).46 The study consisted of subjects from a rollover cohort and de novo cohort.46 The rollover cohort enrolled subjects that had previously completed an 8-week double-blind trial (NCT02109562) in which they had received two monthly injections of either placebo, 90-mg or 120-mg of RBP-7000.23,46 These subjects entered the outpatient study directly with their third injection on day 146 The de novo cohort consisted of subjects with stable schizophrenia as evidenced by a PANSS total score ≤70 at baseline, aged 18 to 65 years, had no prior exposure to RBP-7000, and were otherwise healthy.46 Excluded were subjects that had suicidal ideation or behavior within 1 year or had a significant risk of suicide based on investigator opinion.46 Subjects in the de novo cohort receiving oral risperidone at a dosage other than 3 mg or 4 mg/day entered a 7-day conversion period to titrate oral risperidone to 3 mg or 4 mg/day.46 De novo subjects on an oral antipsychotic other than risperidone entered a 14-day run-in period where their antipsychotic was tapered off and oral risperidone was titrated to 3 mg or 4 mg/day.46 A total of 500 subjects were enrolled (n = 92 and n = 408 in the rollover and de-novo cohorts, respectively) with rollover participants receiving 11 injections of 120-mg RBP-7000 over 40 weeks and de novo participants receiving three injections of 120-mg RBP-7000 over a period of 52 weeks.46 Overall 234 subjects (46.8%) completed the study with the most common reasons for discontinuation being withdrawal of consent (22.4%), adverse events (11.4%), and lost to follow-up (9.0%).46
Over 12 months of treatment, average PANSS total and subscale scores continued to decrease from baseline to end of study for the rollover participants.46 The average change in the PANSS total score were −20.2 (15.6), −12.5 (15.5), and −10.9 (13.2) for rollover participants previously treated with placebo, 90-mg RBP-7000, or 120-mg RBP-7000.46 The average change in the PANSS Positive Scale score were −7.8 (5.5), −3.7 (4.1), and −3.7 (3.5) for rollover participants previously treated with placebo, 90-mg RBP-7000, or 120-mg RBP-7000.46 The average change in the PANSS Negative Scale score were −4.0 (5.9), −4.1 (4.6), and −0.9 (3.8) in rollover participants previously treated with placebo, 90-mg RBP-7000, or 120-mg RBP-7000.46 For the PANSS General Psychopathology Scale score, the mean change was −8.3 (7.0), −4.7 (9.0), and −6.4 (7.9) in rollover participants treated with placebo, 90-mg RBP-7000, or 120-mg RBP-7000.46 For de novo participants the PANSS total and subscale scores remained stable throughout the study.46 CGI-S scores also remained stable in all treatment groups throughout the study.46 The overall discontinuation rate was 53.2%, which is consistent with clinical studies of similar duration with second-generation antipsychotics.46
Safety Assessments
During the 8-week study, the most common adverse effects (incidence ≥ 5%) were headache, weight gain, injection-site pain, constipation, back pain, musculoskeletal pain, sedation, somnolence, akathisia, and anxiety.23 The injection-site reactions were mild in intensity and the frequency was similar across all treatment groups (Table 3).23 The most common reaction was injection-site pain (Table 3).23 The overall incidence of extrapyramidal side effects was low and similar across all treatment groups with akathisia being the most common (2.6%, 6.8%, and 4.2% for the 90-mg, 120-mg RBP-7000 groups, and placebo group, respectively).23 The number of subjects with a ≥7% increase in weight from baseline was higher in both 90-mg and 120-mg RBP-7000 groups (32.7% and 42.1%, respectively) compared to the placebo group (18%).23 The average amount of weight gained was 2.83 kg and 5.15 kg for the 90-mg and 120-mg RBP-7000 mg groups and 4.69 kg for the placebo group.23 There was a higher incidence of elevated prolactin levels in both RBP-7000 groups while the prolactin levels for the placebo group remained stable.23 The differences were dose-dependent with a larger increase in prolactin level for the 120-mg RBP-7000 group.23 There were no clinically relevant differences in mean values for glucose, cholesterol parameters, ECG intervals in subjects at rest, or vitals between all three treatment groups.23 Discontinuation rates due to adverse effects were low: 0%, 1.7%, and 2.5% in the 90-mg, 120-mg RBP-7000 groups, and placebo group, respectively.23
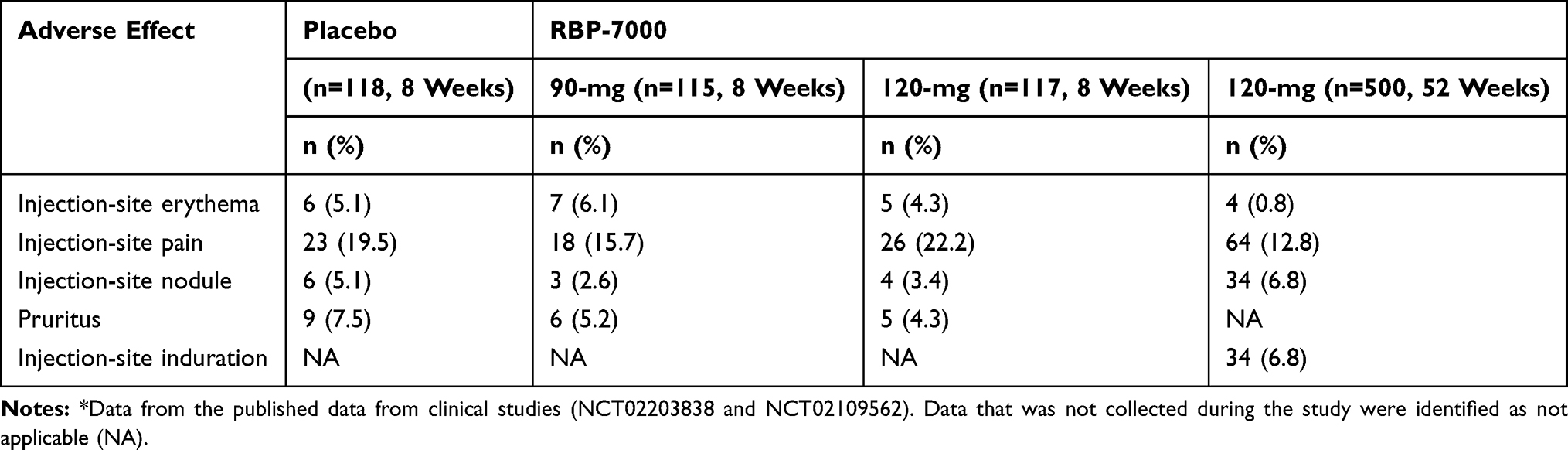 |
Table 3 Injection-Site Reactions Reported with Subcutaneously Administered Risperidone* |
During the 52-week study, the common adverse effects (incidence ≥ 5%) were injection-site pain, weight increase, schizophrenia, insomnia, injection-site nodule, akathisia, injection-site induration, upper respiratory tract infection, and headache.46 Most subjects (>80%) did not experience injection-site reactions (Table 3).23 The number of subjects with a ≥ 7% increase in weight from baseline was 22.1% with de novo participants (24.6%) having a higher incidence of weight gain than rollover participants (9.5%, 13.8%, and 10% for placebo, 90-mg, and 120-mg RBP-7000 groups, respectively).23 The average amount of weight gained was modest at 1.9 kg and 1.6 kg for the de novo and rollover groups, respectively.23 Small average changes from baseline to end of study was observed in glucose, HbA1c, and cholesterol levels with unknown clinical significance.23 There was a higher incidence of elevated prolactin levels at the end of the study in males and females (3.8% and 28.8%, respectively).23 Fifty-eight subjects (11.6%) withdrew from the study due to adverse effects, most commonly owing to schizophrenia symptoms (2%), akathisia (0.8%), weight increases (0.8%), tremor (0.6%), and galactorrhea (0.6%).23 No clinically relevant changes were observed in the laboratory or electrocardiogram values, vital signs, extrapyramidal symptoms, or suicidality.23
Quality of Life and Well-being Assessments
Data collected from the 8-week and 52-week clinical studies measured the impact of RBP-7000 on quality of life and overall well-being.15,42 The health-related quality of life (HRQoL) was assessed using the EuroQol 5D 5-Level (EQ-5D-5L) and Short-Form 36-item Questionnaire, Version 2 (SF-36v2).15,42 The EQ-5D-5L descriptive system consists of five dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) with five levels of severity, which is used to generate an index score anchored at 0 for death and 1 for full health.42 The VAS records the subjects' self-rated health with the “the worst health you can imagine” being 0 and “the best health you can imagine” being 100.42 The SF-36v2 is a 36-item, self-reported survey that measures eight domains of health.42 The score ranges from 0 to 100, with higher scores indicating a better HRQoL.42 Well-being was assessed using the Subjective Well-being Under Neuroleptic Treatment – Short Version (SWN-S).15,42 The SWN-S is a 20-item, patient-rated instrument with each item scored from 1 to 6 on a Likert scale.42 The scores range from 20 to 120, with higher scores representing good subjective well-being.42 Medication satisfaction and preference were assessed using the Medication Satisfaction Questionnaire (MSQ) and Preference of Medication (POM) Questionnaire, respectively.15,42
During the 8-week study, the overall quality of life improved in both RBP-7000 groups compared to placebo with the 120-mg group showing a statistically significant improvement.15 There was a significant improvement in the SWN-S total score for the 120-mg RBP-7000 group and a modest improvement for the 90-mg RBP-7000 group (10.95 points, 9.10 points, and 6.94 points in the 120 mg, 90 mg, and placebo groups, respectively).15 By the end of the study, subjects reported greater medication satisfaction in both the RBP-7000 groups (73% and 73.7% in the 90-mg and 120-mg groups, respectively) compared to the placebo group (50.9%).15 Compared to the most recent pre-study antipsychotic, subjects reported a significant improvement in medication preference for both RBP-7000 groups (63.1% and 45.6% for the 90-mg and 120-mg groups, respectively) rating their medication as “Slightly Better” or “Much Better” compared to the placebo group (33%).15
During the 52-week study, the average quality of life and well-being scores remained stable between baseline (EQ-5D-5L index: 0.83; SF-36v2 Physical Component Score: 50; SF-36v2 Mental Component Score: 46; total SWN-S score: 90) and end of study (EQ-5D-5L index: 0.86; SF-36v2 Physical Component Score: 49; SF-36v2 Mental Component Score: 47; total SWN-S score: 90).42 Subjects reported an increase in medication satisfaction between week 4 (66%) and the end of study (81%).42 An increase in medication preference was also seen between week 4 (66%) and the end of the study (72%).42
Discussion
Based upon the published clinical studies risperidone-SQ appears to be well tolerated and resulted in either improved or stable clinical outcomes.23,42 The overall tolerability of risperidone-SQ was found to be comparable to the known safety profile of oral risperidone with no new safety signals reported.23,42 Risperidone-SQ is a treatment option for patients who would benefit from a LAI antipsychotic medication.2 Eligible populations include patients with recurrent relapses related to poor medication adherence, patients with first-episode schizophrenia, and patients who prefer LAIAs. Patients who are stabilized on oral or injectable risperidone may benefit from the decreased frequency of administration and longer treatment effect. Currently, risperidone is the only second-generation antipsychotic available in a SQ formulation. A first-generation antipsychotic, fluphenazine decanoate, is also available by SQ injection.7
The novel delivery of risperidone-SQ may provide substantial benefits over the currently available IM administration. The needle size of risperidone-SQ is significantly shorter and wider than risperidone-IM, 1-month paliperidone palmitate, and 3-month paliperidone palmitate (Table 4).12,13,28,30 The shorter needle may be easier to administer, but the wider bore could produce injection-site pain in some patients. In clinical trials, risperidone-IM was well tolerated with <2% of the subjects reporting injection-site reactions.30 However, both 1-month paliperidone palmitate and 3-month paliperidone palmitate reported injection-site reactions with ≥5% incidence rate that occurred at least twice as often as placebo.12,13 In addition, studies of non-antipsychotic drugs that compared formulations found patients prefer the SQ route compared to the IM route.3,16,17,31 Spratt and colleagues found a mild or marked preference for the SQ formulation of testosterone with no patients preferring IM injections due to less pain associated with a smaller needle size.31 Studies also found a strong preference for the SQ route of methotrexate for rheumatoid arthritis due to less pain.3,16,17
 |  |
In addition, several studies have found a significantly low rate of IM injection success ranging from 32% to 52% using CT scan or ultrasound for non-antipsychotic drugs.38–41 Variables associated with an increased rate of IM injection failure included obesity, site of injection, subcutaneous fat depth, female sex, and nurse experience levels.38–41 The inadvertent administration of an IM injection within the SQ tissue may result in subtherapeutic drug concentrations, slower absorption rate, localized tissue damage, and reduced drug efficacy.38 The delivery of risperidone through SQ injection may, therefore, be advantageous for obese patients.
Patients and health-care professionals may prefer the simplified dosing and administration of risperidone-SQ. Avoiding oral supplementation may reduce the confusion regarding the duration and tapering of oral overlap required with risperidone-IM. Additionally, not needing to select needle size based on location simplifies injection preparation by health-care professionals. The needle size, while shorter than those required for other LAIAs, is wider. While the shorter needle size may be easier to administer, it may also influence injection-site irritation. The initiation of risperidone-SQ also requires fewer clinical visits for injection administration compared to 1-month paliperidone palmitate which requires two loading doses.12
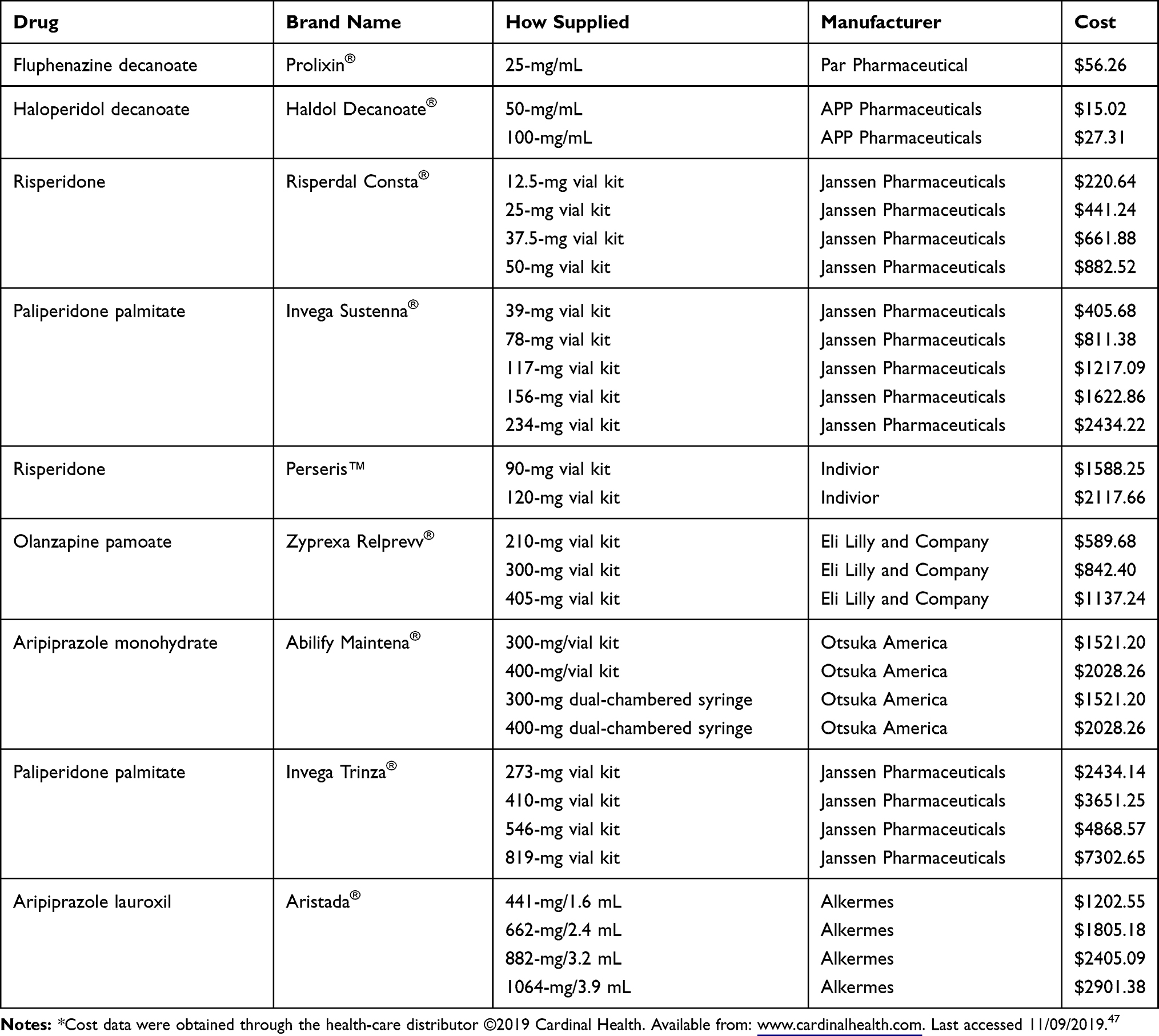
The cost of LAIAs may continue to present a barrier for treatment initiation and adherence.1,2,10,12,13,28–30,37 Presently, the cost of risperidone-SQ is over $1500 for the 90 mg and 120 mg doses. The INSUPPORT™ Copay Assistance Program may reduce the patient out-of-pocket cost for prescriptions; however, this program is only available to patients with private insurance. There are no inpatient hospital financial assistance programs available currently. Confirmation of outpatient insurance will be necessary to determine the approximate medication cost and patient financial burden.
Conclusion
Risperidone is the first second-generation antipsychotic to be available in a SQ LAI formulation. Potential advantages over existing long-acting formulations of risperidone or paliperidone include the ease of transition from oral to long-acting injection as well as ease of administration. Potential disadvantages include injection-site pain and medication cost. However, additional clinical experience with this new formulation and future research is needed to determine whether medication non-adherence rates and related clinical outcomes differ between SQ versus IM injection of risperidone.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abilify Maintena (aripiprazole monohydrate extended-release injectable) [prescribing information]. Otsuka America Pharmaceutical, Incorporated; July 2017.
2. Aristada (aripiprazole monohydrate extended-release injectable) [prescribing information]. Alkermes, Incorporated; September 2017.
3. Brooks PJ, Spruill WJ, Parish RC, Birchmore DA. Pharmacokinetics of methotrexate administered by intramuscular and subcutaneous injections in patients with rheumatoid arthritis. Arthritis Rheumatol. 1990;33:91–94. doi:10.1002/art.1780330112
4. Byerly MJ, Thompson AM, Carmody T, Bugno R, Erwin T. Validity of electronically monitored medication adherence and conventional adherence measures in schizophrenia. Psychiatr Serv. 2007;58:844–847. doi:10.1176/ps.2007.58.6.844
5. Caroli F, Raymondet P, Izard I, Plas J, Gall B, Delago A. Opinions of French patients with schizophrenia regarding injectable medication. Patient Prefer Adherence. 2011;5:165–171. doi:10.2147/PPA.S15337
6. Dammerman R, Kim S, Adera M, Schwarz A. Pharmacokinetics and safety of risperidone subcutaneous implants in stable patients with schizophrenia. Clin Pharmacol Drug Develop. 2018;7(3):298–310. doi:10.1002/cpdd.428
7. Glazer W, Maynard C, Berkman S. Injection site leakage of depot neuroleptics: intramuscular versus subcutaneous injection. J Clin Psychiatry. 1987;48(6):237–239.
8. Glazer WM. Who receives long-acting antipsychotic medications? Psychiatry Serv. 2007;58:437. doi:10.1176/ps.2007.58.4.437
9. Gomeni R, Heidbreder C, Fudala PJ, Nasser AF. A model-based approach to characterize the population pharmacokinetics and the relationship between the pharmacokinetic and safety profiles of RBP-7000, a new, long-acting sustained-release formulation of risperidone. J Clin Pharmacol. 2013;53(10):1010–1019. doi:10.1002/jcph.141
10. Haldol Decanoate (haloperidol decanoate long-acting injection) [prescribing information]. Janssen Pharmaceuticals, Incorporated; March 2017.
11. Heres S, Schmitz FS, Leucht S, Pajonk FG. The attitude of patients towards antipsychotic depot treatment. Int Clin Psychopharmacol. 2007;22(5):275–282. doi:10.1097/YIC.0b013e3280c28424
12. Invega Sustenna (paliperidone palmitate extended-release injectable) [prescribing information]. Janssen Pharmaceuticals, Incorporated; July 2017.
13. Invega Trinza (paliperidone palmitate extended-release injectable) [prescribing information]. Janssen Pharmaceuticals, Incorporated; March 2017.
14. Ivaturi V, Gopalakrishnan M, Gobburu J, et al. Exposure-response analysis after subcutaneous administration of RBP-7000, a once-a-month long-acting Atrigel formulation of risperidone. Br J Clin Pharmacol. 2017;83(7):1476–1498. doi:10.1111/bcp.v83.7
15. Isitt J, Nadipelli R, Kouassi A, Fava M, Heidbreder C. Health-related quality of life in acute schizophrenia patients treated with RBP-7000 once monthly risperidone: an 8-week, randomized, double-blind, placebo-controlled, multicenter phase 3 study. Schizophr Res. 2016;174(1–3):126–131. doi:10.1016/j.schres.2016.03.020
16. Jin J, Zhu L, Chen M, et al. The optimal choice of medication administration route regarding intravenous, intramuscular, and subcutaneous injection. Patient Prefer Adherence. 2015;9:923–941. doi:10.2147/PPA.S87271
17. Jundt JW, Browne BA, Fiocco GP, Steele AD, Mock D. A comparison of low dose methotrexate bioavailability: oral solution, oral tablet, subcutaneous and intramuscular dosing. J Rheumatol. 1993;20(11):1845–1849.
18. Kane JM, Correll CU. Past and present progress in the pharmacologic treatment of schizophrenia. J Clin Psychiatry. 2010;71:1115–1124. doi:10.4088/JCP.10r06264yel
19. Kane J, Garcia-Ribera C. Clinical guideline recommendations for antipsychotic long-acting injections. Br J Psychiatry Suppl. 2009;52:63–67. doi:10.1192/bjp.195.52.s63
20. Laffont CM, Gomeni R, Zheng B, Heidbreder C, Fudala PJ, Nasser AF. Population pharmacokinetic modeling and simulation to guide dose selection for RBP-7000, a new sustained-release formulation of risperidone. J Clin Pharmacol. 2015;55(1):93–103. doi:10.1002/jcph.v55.1
21. Laffont CM, Gomeni R, Zheng B, Heidbreder C, Fudala PJ, Nasser AF. Population pharmacokinetics and prediction of dopamine D2 receptor occupancy after multiple doses of RBP-7000, a new sustained-release formulation of risperidone, in schizophrenia patients on stable oral risperidone treatment. Clin Pharmacokinet. 2014;53(6):533–543. doi:10.1007/s40262-014-0132-7
22. Lehman AF, Lieberman JA, Dixon LB, et al; American Psychiatric Association; steering committee on practice guidelines. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry. 2004;161(S2):1–56.
23. Nasser AF, Henderson DC, Fava M, et al. Efficacy, safety, and tolerability of RBP-7000 once-monthly risperidone for the treatment of acute schizophrenia: an 8-week, randomized, double-blind, placebo-controlled, multicenter phase 3 study. J Clin Psychopharmacol. 2016;36(2):130–140. doi:10.1097/JCP.0000000000000479
24. National Institute for Health and Clinical Excellence. Psychosis and Schizophrenia in Adults: Treatment and Management. Alden Press UK. Edn. London: The British Psychological Society and the Royal College of Psychiatrists; 2014.
25. Olfson M, Mechanic D, Hansell S, Boyer CV, Walkup J. Prediction of homelessness within three months of discharge among inpatients with schizophrenia. Psychiatry Serv. 1999;50:667–673. doi:10.1176/ps.50.5.667
26. Patel M, David A. Why aren’t depot antipsychotics prescribed more often and what can be done about it? Adv Psychiatric Treat. 2005;11:203–213. doi:10.1192/apt.11.3.203
27. Patel MX, de Zoysa N, Bernadt M, David A. Depot and oral antipsychotics: patient preferences and attitudes are not the same thing. J Psychopharmacol. 2009;23:789–796. doi:10.1177/0269881108092124
28. Perseris (risperidone) [package insert]. North Chesterfield (VA): Indivior, Incorporated; 2018.
29. Prolixin (fluphenazine decanoate Injection) [prescribing information]. West-Ward Pharmaceuticals Corporation; October 2017.
30. Risperdal Consta (risperidone microspheres long-acting injectable) [prescribing information]. Janssen Pharmaceuticals, Incorporated; February 2017.
31. Spratt D, Stewart I, Savage C, et al. Subcutaneous injection of testosterone is an effective and preferred alternative to intramuscular injection: demonstration in female-to-male transgender patients. J Clin Endocrinol Metab. 2017;102(7):2349–2355. doi:10.1210/jc.2017-00359
32. Svedberg B, Backenroth-Ohsako G, Lützén K. On the path to recovery: patients’ experiences of treatment with long-acting injections of antipsychotic medication. Int J Ment Health Nurs. 2003;12:110–118. doi:10.1046/j.1440-0979.2003.00277.x
33. Tiihonen J, Haukka J, Taylor M, Maddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168:603–609. doi:10.1176/appi.ajp.2011.10081224
34. Waddell L, Taylor M. Attitudes of patients and mental health staff to antipsychotic long-acting injections: systematic review. Br J Psychiatry Suppl. 2009;52:S43–S50. doi:10.1192/bjp.195.52.s43
35. Weiden PJ, Schooler NR, Weedon JC, Elmouchtari A, Sunakawa A, Goldfinger SM. A randomized controlled trial of long-acting injectable risperidone vs continuation on oral atypical antipsychotics for first-episode schizophrenia patients: initial adherence outcome. J Clin Psychiatry. 2009;70:1397–1406. doi:10.4088/JCP.09m05284yel
36. Zipursky RB, Menezes NM, Streiner DL. Risk of symptom recurrence with medication discontinuation in first-episode psychosis: a systematic review. Schizophr Res. 2014;152:408–414. doi:10.1016/j.schres.2013.08.001
37. Zyprexa Relprevv (olanzapine pamoate long-acting injection) [prescribing information]. Eli Lilly and Company; July 2017.
38. Soliman E, Ranjan S, Xu T, et al. A narrative review of the success of intramuscular gluteal injections and its impact in psychiatry. Bio-Design Manuf. 2018;1(3):161–170. doi:10.1007/s42242-018-0018-x
39. Chan VO, Colville J, Persaud T, Buckley O, Hamilton S, Torreggiani WC. Intramuscular injections into the buttocks: are they truly intramuscular? Eur J Radiol. 2006;58(3):480–484. doi:10.1016/j.ejrad.2006.01.008
40. Boyd AE, DeFord LL, Mares JE, et al. Improving the success rate of gluteal intramuscular injections. Pancreas. 2013;42(5):878–882. doi:10.1097/MPA.0b013e318279d552
41. Garris JL, DeFord LL, Dagohoy CG, et al. Gender related issues in gluteal intramuscular injections. Pancreas. 2010;39(2):27. doi:10.1097/01.mpa.0000363915.17360.04
42. Dhanda R, Varghese D, Nadipelli VR, et al. Patient-reported outcomes in schizophrenia patients treated with once-monthly extended-release risperidone in a long-term clinical study. Patient Prefer Adherence. 2019;13(1):1037–1050. doi:10.2147/PPA
43. Karas A, Burdge G, Rey JA. Perseris: a new and long-acting, atypical antipsychotic drug-delivery system. Drug Forecast. 2019;44(8):460–466.
44. Citrome L. Sustained-release risperidone via subcutaneous injection: a systematic review of RBP-7000 (Perseris) for the treatment of Schizophrenia. New Drug Rev. 2018;1(1):130–141.
45. Krogmann A, Peters L, Von Hardenberg L, Bodeker K, Nohles V, Correl C. Keeping up with the therapeutic advances in schizophrenia: a review of novel and emerging pharmacological entities. Int J Neuropsychiatr Med. 2019;24(4):38–69. doi:10.1017/S109285291900124X
46. Andorn A, Graham J, Csernansky J, et al. Monthly extended-release risperidone (RBP-7000) in the treatment of schizophrenia. Results from the phase 3 program. J Clin Psychopharmacol. 2019;39(5):428–433. doi:10.1097/JCP.0000000000001076
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.