")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Once-monthly galcanezumab for the prevention of migraine in adults: an evidence-based descriptive review and potential place in therapy
Authors Lupi C, Guerzoni S, Negro A , Benemei S
Received 28 August 2018
Accepted for publication 10 February 2019
Published 11 April 2019 Volume 2019:15 Pages 557—569
DOI https://doi.org/10.2147/TCRM.S159690
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Garry Walsh
Chiara Lupi,1 Simona Guerzoni,2 Andrea Negro,3 Silvia Benemei1
1Headache Centre, Careggi University Hospital, Department of Health Sciences, University of Florence, Florence, Italy; 2Medical Toxicology Unit, Headache and Drug Abuse Centre, Department of Biomedical, Metabolic and Neural Sciences, University of Modena e Reggio Emilia, Modena, Italy; 3Department of Clinical and Molecular Medicine, Regional Referral Headache Centre, Sant’Andrea Hospital, Sapienza University, Rome
Abstract: In the last 15 years relevant efforts have been made to demonstrate that calcitonin gene-related peptide (CGRP) antagonism is a valuable and druggable mechanism for treatment or prevention of migraine. Galcanezumab is one of the antibodies developed and studied to prevent migraine by targeting CGRP. The scope of this review is to report data currently available on galcanezumab. According to available data, galcanezumab is safe and efficacious in preventing migraine in episodic migraine patients, also reducing disability and functional impairment due to the disorder. In September 2018, galcanezumab was approved in the USA for the prevention of migraine in adults. The placement of galcanezumab into the current therapeutic scenario will be a revolution for migraine patients, and probably in a less near future also for patients affected by other primary headaches.
Keywords: calcitonin gene-related peptide, headache, LY2951742, monoclonal antibody prophylaxis, CGRP
Introduction
Migraine is one of the most common neurological disorders observed in clinical practice, affecting over 14% of adults worldwide.1 In 2016, the last release of data from the Global Burden of Disease (GBD) established migraine as the second leading cause of years lived with disability (YLDs).2 Accordingly, migraine has a strong social impact with an economic burden estimated at around €27 billion per year in Europe and presumably similar in the USA.3
Migraine pharmacological treatment is based on acute therapy, aimed to abort ongoing pain and reduce migraine-related symptoms, and on preventive therapy that is required when the frequency of attacks is ≥4 per month and aims to both lower attack frequency and severity and to decrease associated disability.4
In some patients, especially in those not taking preventive therapies or in the case of treatment failure, the natural course of migraine is toward an increase of headache frequency with a transition into and out of four distinct stages: no migraine, low-frequency episodic migraine (EM) (<10 days/month), high-frequency EM (10–14 days/month), and chronic migraine (CM) (>15 days/month).5 It has been estimated that every year approximately 2.5% of patients with EM develop new-onset CM5 and that, as a whole, 1%–4% of the general population develops CM.1 Nonmodifiable (eg, female sex, old age, Caucasian race, low education level, worse socioeconomic status, and genetic factors) and modifiable (eg, caffeine use/misuse, stressful life events, bad lifestyle, family or personal history of mood disorders, sleep disorders, and substance use) risk factors are involved in migraine progression from EM to CM.6 In particular, the increase in headache frequency translates into an increase of acute treatment utilization and may associate with the development of medication-overuse headache (MOH). All acute treatments, both specific (ie, triptans and ergot alkaloids) and not specific (ie, nonsteroidal anti-inflammatory drugs [NSAIDs], simple and combination analgesics, opioids, barbiturates, antinausea medications, antihistamines and muscle relaxants), when overused, can be associated with MOH, which in turn decreases responsiveness to acute or prophylactic drugs.7
Nowadays, migraine is still a treatable rather than a curable disorder. The preventive treatment armamentarium is quite old, nonspecific, and to a large extent built up on drugs borrowed from other medical indications, such as: antihypertensive agents (eg, angiotensin-converting enzyme [ACE] inhibitors, angiotensin receptor blockers, beta blockers), calcium channel blockers (eg, flunarizine), antiepileptic drugs (eg, topiramate, sodium valproate, gabapentin), tricyclic antidepressants (eg, amitriptyline, nortriptyline), serotonin receptor antagonists (eg, pizotifene), and selective norepinephrine reuptake inhibitors (SNRIs).6 Preventive therapies may be prescribed to both EM and CM patients. With the exceptions of topiramate and onabotulinum toxin A (the latter authorized only for CM prevention), the use of which is supported by several randomized clinical trials, proof of efficacy for the other medications often comes from single trials8–13 or open-label studies, and their use is in some cases empirical instead of evidence based.14 Comparative trials are lacking, similar to evidence about predictive factors or biomarkers of responsiveness. Treatment decision-making should always be driven by clinical considerations, taking into account comorbidities, such as psychiatric and cardiovascular disorders, fibromyalgia, myofascial pain syndromes, and various forms of visceral pain.15 A certain therapy could be contraindicated in the presence of a specific comorbid disease, while another treatment could be effective to treat both migraine and the other condition, at the same time reducing the medication intake and, consequently, the risk of drug–drug interactions.16
Despite the progress in migraine management, a significant portion of patients has unmet needs. Many patients needing prevention do not receive it,17 and even when it is prescribed, adherence rates are quite low (~35%–50%),18 mainly due to relatively unsatisfactory efficacy and to side effects.19–21 Another major reason for the scarce adherence is the requirement for daily intake, often twice or three times per day, to reach the therapeutic dosages. Similar to other therapeutic areas, also in headache medicine, the more complicated the treatment is in terms of the number of daily intakes and/or drugs, the higher the chance that a patient will interrupt the treatment.22
In order to be successful, when advising about prophylaxis, the point of view of migraine patients should be borne in mind. Patients need to be open to advice and information, and interventions have to be offered timely in the course of migraine.23 Migraine patients ask for a preventive treatment that is effective, with an easy route of administration combined with a wide time lag between intakes, also being safe and well tolerated.24–27 Physicians would add to this list the wish for a treatment with few contraindications and interactions, if any.
As already stated, the preventive therapies currently available are not migraine specific and the development of drugs acting on the crucial steps of migraine pathogenesis will radically change migraine prophylaxis.
Migraine pathophysiology is multifactorial, complex, and not yet completely understood. Currently, the most accredited pathogenic hypothesis is based on the trigeminovascular theory that, although considering a central nervous system dysfunction as the primum movens of the genesis of the attacks, indicates a peripheral mechanism as fundamental for pain.28,29 The mechanism of pain has been identified with neurogenic inflammation, a sterile inflammation phenomenon mediated by the activation of trigeminal perivascular fibers that release neuropeptides, such as substance P, and calcitonin gene-related peptide (CGRP),30 that are directly responsible for increased blood flow, edema, recruitment of inflammatory cells, and release of proinflammatory and inflammatory molecules.31 Finally, the activation of meningeal nociceptors could further stimulate the sensory trigeminal fibers, thus perpetuating the release of vasoactive peptides, including CGRP.30 In this cascade of events, CGRP appears to play a fundamental role.32
CGRP is a neuropeptide produced from alternative splicing of the calcitonin gene. CGRP is a highly potent vasodilator and has been identified as a relevant player in mammalian biology, acting a crucial role both in physiological and pathological conditions. In particular, it may potentially be involved in the physiological regulation of the vascular tone and blood pressure, and some evidence has also been collected for some cardiovascular diseases, such as heart failure and ischemia.33 Finally, data are accumulating about involvement of CGRP in extracardiovascular conditions such as diabetes and arthritis, in addition to the well-known involvement in pain and neurogenic inflammation.33
There are two forms of CGRP differently expressed in humans: 1) alpha-CGRP is prevalent in primary sensory neurons of the dorsal root ganglia, in vagal ganglia, and throughout the trigeminal system; and 2) beta-CGRP is prevalent in intrinsic enteric neurons.34–36 Accordingly, alpha-CGRP is primarily involved in migraine pathogenesis. The CGRP acts by targeting a G protein-coupled receptor of the B-type constituted by the calcitonin receptor-like receptor (CLR) and receptor activity-modifying protein 1 (RAMP1), both necessary for the functional CGRP receptor.37
Several findings support the involvement of CGRP in migraine pathophysiology: 1) CGRP levels are increased during a migraine attack38 and in CM patients also in the pain-free interval,39 but return to normality after triptan administration and consequent headache resolution;40–43 2) intravenous infusion of CGRP can induce migraine-like attacks in migraine patients,44,45 as well as dilatation of the middle meningeal arteries and the middle cerebral arteries that reverses after sumatriptan administration;46 and, finally, 3) animal data suggest that CGRP can induce the generation of light intolerance (photophobia), a typical feature of a migraine attack.47 Accordingly, in the last 15 years relevant efforts have been made to demonstrate that CGRP antagonism, by means of different drug classes (ie, small molecule antagonists of CGRP receptor,48–53 anti-CGRP receptor antibody54–56 and anti-CGRP antibodies,57–61) is a valuable mechanism to treat or prevent migraine. Galcanezumab,62–65 together with erenumab,54–56 eptinezumab,57 and fremanezumab,58–61 is one of the antibodies developed and studied to prevent migraine by targeting CGRP.
Pharmacology of galcanezumab
Pharmacodynamics
Galcanezumab, initially named LY2951742, is a fully humanized IgG4 anti-CGRP monoclonal antibody (MAb). It binds to the human CGRP, thus preventing its binding to receptors. Affinity of the MAb to the ligand is relatively high, with an equilibrium dissociation constant (KD) of 31 pM.66 In early clinical development, the evaluation of the target engagement and dose selection of galcanezumab was performed with the capsaicin-induced dermal blood flow (DBF) model.67 Capsaicin-induced DBF represents a useful pharmacodynamic model to assess “scavenging” of CGRP in vivo.68 The model concerns the topical application of capsaicin onto the skin, which by the activation of the Transient Receptor Potential Vanilloid 1 (TRPV1) channel expressed by primary sensory neurons provokes the release of CGRP, the key mediator of capsaicin-induced DBF in humans.69 The Doppler laser scanning technique, utilized to quantify the variations in DBF, demonstrated the reversal of capsaicin-induced DBF by the CGRP blocking agents.67,70
To support the clinical development of galcanezumab, a capsaicin-induced DBF model was initially applied in nonhuman primates. Galcanezumab inhibited capsaicin-induced vasodilation for at least 29 days after a single intravenous injection,71 a promising attribute for the prophylactic treatment of migraine. In humans, in a Phase I study, a single subcutaneous administration of 5 mg of galcanezumab inhibited the capsaicin-induced DBF from the 28th day after injection, while at higher doses (75, 200, and 600 mg) the effect was already evident from the third day.72 Inhibition of the capsaicin-induced DBF was observed until the 42nd day, when the last assessment following the single-dose administrations was performed. When galcanezumab was administered in four subcutaneous consecutive doses (150 mg), with a 14-day dosing interval, the inhibition was visible up to 130 days after the last dose.72 Serum concentrations of galcanezumab closely correlated with the inhibition of capsaicin-induced DBF, corroborating a strong dose–response relationship.
Pharmacokinetics
The pharmacokinetic profile of galcanezumab is different from that of drugs traditionally used in migraine prophylaxis. Like other MAbs, it has considerable dimensions (144.1 kDa) and must be administered parenterally, because of its low permeability through cell membranes and its instability in the gastrointestinal tract. During lactation, the amount of galcanezumab in milk is likely to be very low due to its dimensions, and absorption is unlikely because it is probably destroyed in the infant’s gastrointestinal tract.73 The plasma half-life (25–30 days) allows the drug to be administered every 2 weeks, or every month.62,63,74 This attribute is particularly suitable for a variable condition like migraine that does not favor adherence to oral prophylactic therapies on a daily basis.18 Furthermore, galcanezumab is not apparently metabolized by the hepatic cytochromes, because it follows the antibody elimination routes, via catabolism in smaller peptides and individual amino acids,75 that can be used for the synthesis of other proteins. Importantly, the metabolism of MAbs does not generate noxious intermediates and, therefore, they are unlikely to induce drug-induced liver injury. Even pharmacological interactions on the liver metabolism or kidney clearance pathways are minimized.
Pharmacokinetic properties of galcanezumab have been characterized by a Phase I study, after a single dose and multiple doses of subcutaneous injection in healthy male volunteers.72 After subcutaneous administration of a single dose, the mean serum half-life (t1/2) of galcanezumab is between 25 and 30 days.72 The absorption rate is slow with a median time to peak concentration (Tmax) between the 7th and 14th day after administration. The peak serum concentration (Cmax) and the area under the concentration–time curve (AUC) are proportional to the dose. Most of the previous pharmacokinetic parameters do not differ following administration of four consecutive subcutaneous doses of 150 mg, with a 14-day dosing interval.72 The median Tmax was equal to 3 days and much shorter than for the single-dose administration, while the t1/2 was in accordance with forecasts, corresponding to 31.9 days.72
In an open-label, double-arm, randomized, parallel-group study, MAb serum concentrations were similar after subcutaneous administration of galcanezumab 240 mg solution via a prefilled syringe and an autoinjector, in healthy subjects.76 Similarly, the site of injection (arm, thigh, or abdomen) did not influence the Cmax or AUC. A statistically significant difference in median Tmax for the autoinjector (5 days) compared to the prefilled syringe (7 days) was registered; however, this is likely to not be of any clinical relevance, considering that galcanezumab is intended to be administered once monthly as a preventive treatment for migraine. Furthermore, substantial overlap in the range of Tmax values across the devices was observed.76
Mode of action
The site of action of MAbs is still debated.77,78 Most prophylactic treatments for migraine are supposed to have various effects on the central nervous system, but galcanezumab, similar to other MAbs, seems to not penetrate the blood–brain barrier under physiological conditions. Therefore, the efficacy demonstrated in Phase II and Phase III clinical trials, together with other results obtained with triptans and CGRP receptor antagonists, suggest the presence of peripheral mechanisms.62,63,74 In addition, there is no evidence that the blood–brain barrier is breeched in patients with migraine, either during or between attacks.77 Importantly, Schankin et al79 have demonstrated that the blood–brain barrier remains tight for 11C-dihydroergotamine during acute glyceryl trinitrate-induced migraine attacks, both ictally and interictally. However, considering the ability of some large molecules such as insulin and transferrin to enter the brain because of the expression of transporters,80 it is too early to declare the debate closed.
There is limited information about any difference in action between MAbs targeting CGRP. In a poster presented at the 2016 Annual Scientific Meeting of the American Headache Society, the first divergences regarding the CGRP intrinsic binding features of eptinezumab, fremanezumab, and galcanezumab were hypothesized.81 Surface plasmon resonance binding analysis was conducted to characterize the binding of the MAbs to CGRP. Galcanezumab appears to reversibly antagonize its target with rapid CGRP engagement and dissociation. On the contrary, fremanezumab and eptinezumab engage CGRP with an undetectable dissociation, with the latter being able to neutralize CGRP activities twice as rapidly as fremanezumab. Notwithstanding, no significant differences have emerged in anti-CGRP MAbs, in both Phase II and Phase III clinical trials conducted so far.82
Efficacy
Galcanezumab induced a strong, dose-dependent, and durable inhibition of capsaicin-induced DBF increase, supporting the clinical development of this drug for prophylaxis in migraine patients.72
The efficacy of galcanezumab as a preventive treatment for migraine has been primarily evaluated in subjects affected by EM.
In 2014, Dodick et al62 published the results of ART-01 (NCT01625988), a randomized, double-blind, placebo-controlled, Phase IIa proof-of-concept study conducted in 35 American centers, the first ever reported efficacy trial with a MAb against CGRP in the prevention of migraine.83 In ART-01, from 2012 to 2013, 218 adult subjects, with at least a 1-year history of migraine, migraine onset prior to age 50, and 4–14 migraine headache days (MHD), were randomly (1:1) assigned to receive 150 mg galcanezumab or placebo as subcutaneous injections every 2 weeks for 12 weeks. One-hundred and fifty milligrams of galcanezumab was considered the therapeutic dose, according to the assessment of maximum inhibition of the capsaicin-induced DBF effect.72 During the 28-day baseline period, individuals in the galcanezumab arm reported a mean of 7.0 MHD vs 6.7 MHD in the placebo arm. The primary efficacy endpoint was the mean change from baseline in the number of MHD in a 4-week period (weeks 9–12), as assessed at the 12-week timepoint. Galcanezumab induced a reduction of 4.2 and placebo of 3.0 in MHD from baseline (P=0.0030), with a significant difference of 1.2 MHD in favor of galcanezumab. Moreover, galcanezumab generated statistically significant reduction in headache days (−4.9 vs −3.7, P=0.012) and migraine attacks (−3.1 vs −2.3, P=0.0051). In a post hoc efficacy analysis, 49% of subjects in the galcanezumab group had a 75% response compared to 27% in the placebo group, and a complete response was observed in 32% of patients treated with galcanezumab vs 17% of patients on placebo treatment. As a whole, the results of this study provided the first preliminary report of efficacy of galcanezumab as a preventive therapy for migraine.62
In a following dose-ranging, randomized clinical trial (NCT02163993),63 410 adult patients affected by EM were randomly assigned in a 2:1:1:1:1 ratio to placebo, 5, 50, 120, or 300 mg galcanezumab subcutaneously injected once monthly for a 3-month period. The study was conducted in the USA in clinics of 37 licensed physicians. The inclusion criteria were identical to those of ART-01. For the primary endpoint, galcanezumab 120 mg significantly reduced the mean number of MHD compared with placebo (−4.8 vs −3.7 days compared to the baseline values of 6.7 and 6.6 days). The overall change from baseline to month 3 in the number of MHD was significant for both the 120 mg and 300 mg dose arms compared with placebo. Galcanezumab 120 mg was also superior to placebo at month 3 for all key secondary efficacy outcomes (ie, number of MHD plus probable MHD, probable MHD, migraine attacks, proportion of patients reporting 50% and 100% reduction in the number of MHD). Despite the relatively short duration of the study, these data provided sufficient efficacy data to justify further development of galcanezumab, 120 and 240 mg, in larger Phase III clinical trials.63
Recently, the results of EVOLVE-1 (NCT02614183) and EVOLVE-2 (NCT02614196), two Phase III randomized controlled trials with galcanezumab and placebo in people with EM, have been published.64,65 These studies were characterized by similar study design. Between January 2016 and March 2017, EVOLVE-1 was conducted at 90 centers in the USA, Puerto Rico, and Canada. At the same time, EVOLVE-2 was performed in 109 study sites in the USA, Europe, Argentina, Korea, Taiwan, and Mexico. In both trials, patients were randomized to receive either placebo or one galcanezumab dose regimen (120 or 240 mg) once a month for 6 months and they were followed for 5 months, after the last injection, in the posttreatment period. At baseline, the mean monthly MHD were 9.1. The primary endpoint was the reduction of MHD per 4 weeks over the entire 6-month double-blind period. With an onset of the effect at month 1, treatment with galcanezumab significantly reduced monthly MHD by 4.7 days (120 mg) and 4.6 days (240 mg) compared with placebo (2.8 days) in EVOLVE-1, and by 4.3 (120 mg) and 4.2 days (240 mg) compared with placebo (2.3 days) in EVOLVE-2. It is noteworthy that no meaningful differences between galcanezumab 120 mg and galcanezumab 240 mg doses were seen on measures of efficacy. Both MAb doses were statistically superior to placebo for monthly MHD with acute medication use and for the mean percentage of patients with at least 50%, at least 75%, and 100% reduction from baseline in monthly MHD during treatment (Table 1).64,65 A post hoc analysis from pooled data of the two trials showed that around 40% of the galcanezumab-treated patients achieved 100% response in MHD reduction for at least 1 month. More patients had a 100% monthly response in the last 3 months, suggesting that the duration of the treatment plays a role in determining a full clinical answer. Although very few patients (0.7% and 1.4% for galcanezumab 120 mg and 240 mg, respectively) achieved 100% response for all 6 months, it seems encouraging that ~13% of the patients had at least 3 months free from MHD across the 6-month phase.84 Taken together, the results of EVOLVE-1 and EVOLVE-2 confirmed the data collected in Phase II studies, demonstrating a clinically meaningful level of long-term efficacy of galcanezumab as prophylactic treatment for EM.64,65
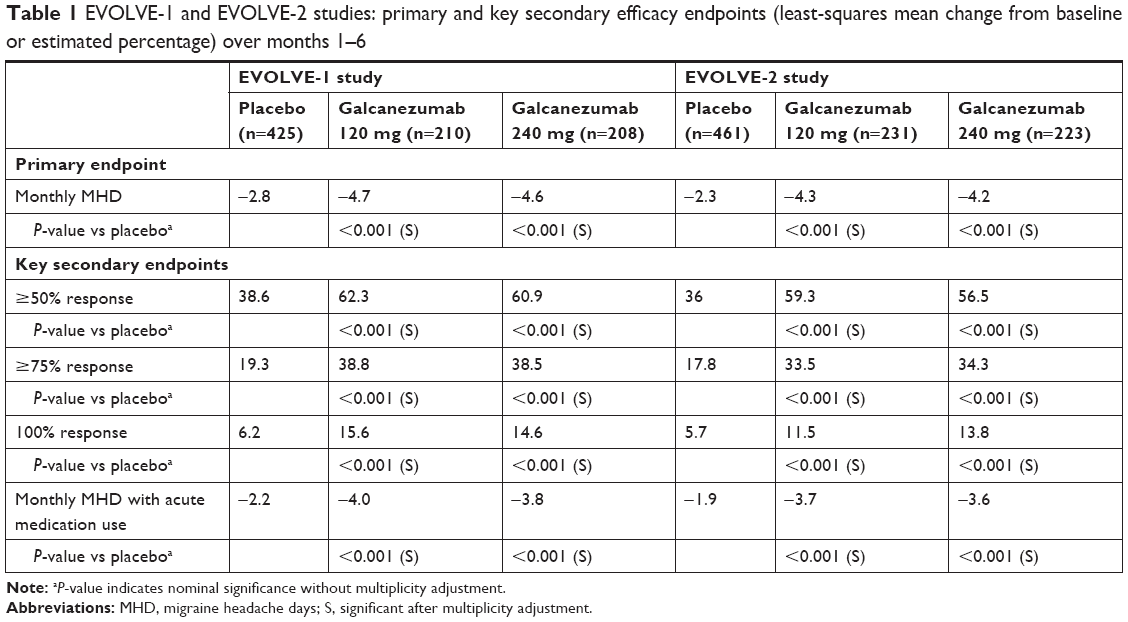 | Table 1 EVOLVE-1 and EVOLVE-2 studies: primary and key secondary efficacy endpoints (least-squares mean change from baseline or estimated percentage) over months 1–6 |
Galcanezumab also provided effective migraine prevention in patients with CM.
During the 3-month double-blind treatment phase of the Phase III REGAIN study (NCT02614261)85 in adults with CM, once-monthly galcanezumab 120 and 240 mg were both associated with significantly greater reductions from the baseline mean number of monthly MHD (19.4 for the total sample) compared to placebo (overall mean change −4.8 and −4.6 vs −2.7). Galcanezumab 120 mg had statistical improvement vs placebo on the primary endpoint and the ≥50% response rate, while galcanezumab 240 mg demonstrated statistical improvement compared to placebo on the primary endpoint and all key secondary endpoints, except for the 100% response rate (Table 2). As seen in EVOLVE-1 and EVOLVE-2, there were no statistical differences between doses on any efficacy measures. The results of the 9-month open-label extension of the trial are still not available.85
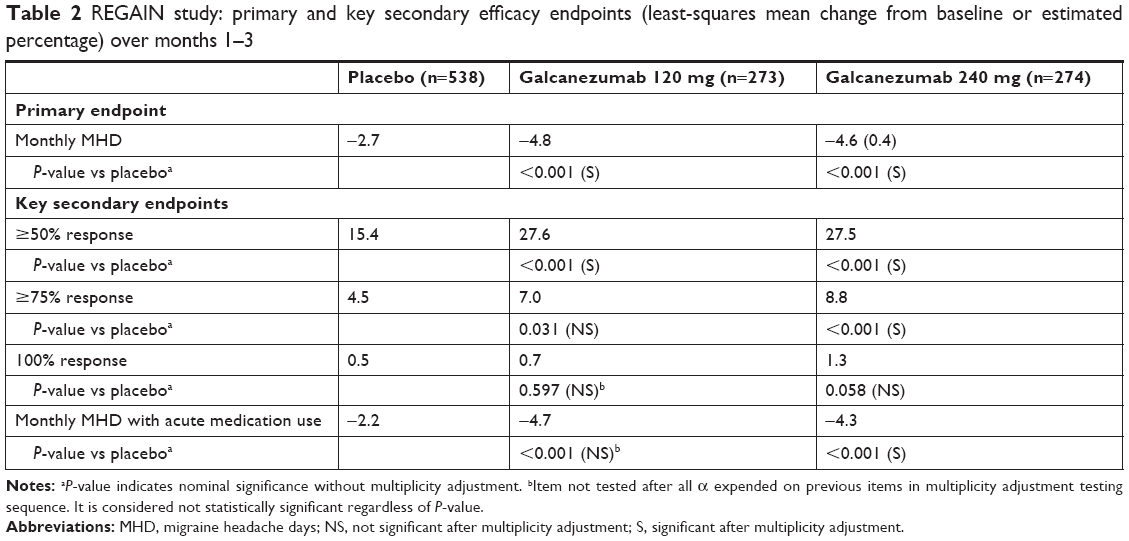 | Table 2 REGAIN study: primary and key secondary efficacy endpoints (least-squares mean change from baseline or estimated percentage) over months 1–3 |
A Phase III, long-term, open-label safety study (NCT02614287)86 included, as the secondary objective, the evaluation of efficacy measures to assess the long-term effectiveness of galcanezumab 120 or 240 mg, administered subcutaneously once monthly for a year, in adult patients with EM and CM. At baseline, MHD per month were 10.6. In both galcanezumab dose groups (n=135 in each arm), there were statistically significant within-group reductions from baseline in the monthly MHD (−5.6 for 120 mg and −6.5 for 240 mg). Reduction in the mean monthly MHD was apparent as early as the first month and was sustained throughout the 12-month treatment period.86 There were also significant and meaningful decreases in acute headache medication use from baseline at each monthly visit during the treatment period (overall change from baseline: −5.1 days).87
Further relevant efficacy data on galcanezumab in the prophylaxis of migraine come from post hoc analysis of integrated EVOLVE-1 and EVOLVE-2 results in EM patients and REGAIN results in CM patients.
The persistence of the effect during the double-blind phase was evaluated in a total of 1,773 adult patients with EM (n=444 for galcanezumab 120 mg; n=435 for galcanezumab 240 mg; n=894 for placebo for two studies pooled) and 1,113 patients with CM (n=278 for galcanezumab 120 mg; n=277 for galcanezumab 240 mg; n=558 for placebo). In EM patients, ≥50% response was maintained in 41.5% and 41.1% of galcanezumab-treated patients (120 mg and 240 mg, respectively) for ≥3 consecutive months and in 19.0% and 20.5%, respectively, for 6 consecutive months; the response was significantly greater than that of the placebo arm (21.4% and 8.0% for ≥3 and 6 consecutive months, respectively). In CM patients, 29% of galcanezumab-treated patients maintained ≥30% response all 3 months compared to 16% of placebo patients, while ≥50% response was maintained in 16.8% and 14.6% of galcanezumab-treated patients (120 mg and 240 mg, respectively) and was greater than placebo (6.3%).88
The subgroup of patients treated with both doses of galcanezumab who previously failed two or more preventive therapies (n=172 with EM, n=323 with CM) experienced a statistically significant reduction in the average monthly MHD from baseline vs those treated with placebo (3.45 days for 120 mg and 3.85 days for 240 mg vs 0.81 days for placebo in EM, 5.91 days for 120 mg and 3.30 days for 240 mg vs 1.44 days for placebo in CM), and at least a 50% reduction in monthly MHD compared to the placebo arm (54.6% for 120 mg and 61.2% for 240 mg vs 26.2% for placebo in EM, 30.4% for 120 mg and 18.3% for 240 mg vs 9.7% for placebo in CM).89
Interestingly, galcanezumab-treated patients who did not achieve early satisfactory improvement appear to have a reasonable likelihood of continued improvement in the months following the initial treatment. For example, of 155 EM patients whose answer was 30%–50% fewer MHD after 1 month of dosing, 62% achieved “good” (≥50% reduction in baseline MHD) and 20% “better” (≥75% reduction in baseline MHD) responses with continued treatment. Similarly, of 116 CM patients having 10%–30% fewer MHD after 1 month of dosing, 38% achieved “good” and 13% “better” responses with continued treatment.90 Importantly, available data do not offer any evidence of differential responses from patients affected by migraine with aura vs patients affected by migraine without aura.
Additional clinical trials on galcanezumab for different clinical indications are summarized in Table 3. Interestingly, a trial that aims to investigate galcanezumab in adults with treatment-resistant migraine, the CONQUER study (NCT03559257),91 began at the end of July 2018. Although the present review is focused on the use of galcanezumab for the prevention of migraine in adults, it is noteworthy that galcanezumab has been also studied in the pediatric population; the Phase III REBUILD study (NCT03432286)92 has been enrolling participants 6–17 years of age affected by EM, since March 2018. In addition, galcanezumab is being widely studied for the prophylaxis of episodic and chronic cluster headache in Phase III randomized clinical trials (NCT02397473,93 NCT02438826,94 NCT02797951).95
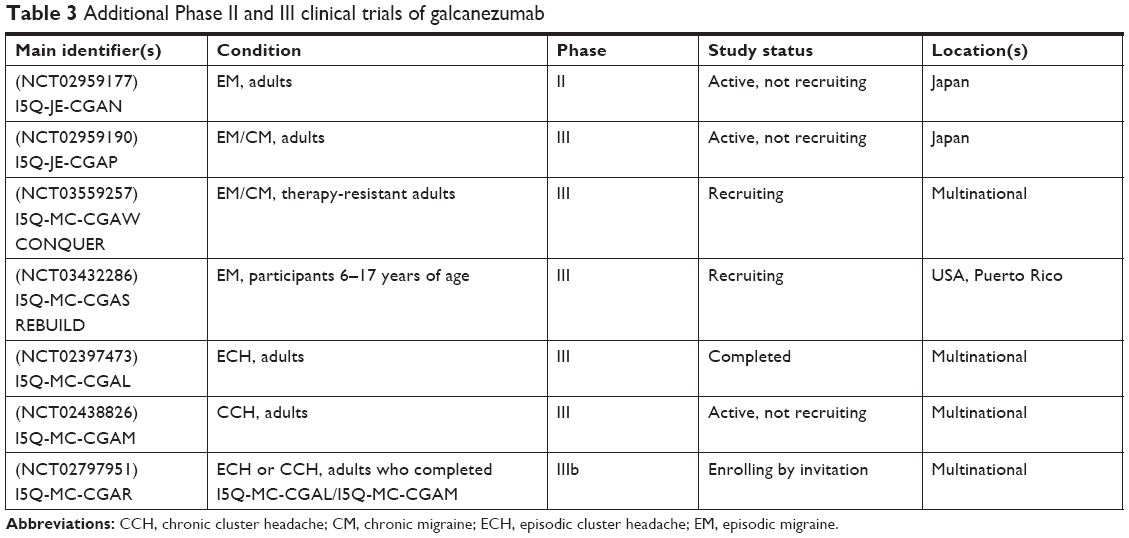 | Table 3 Additional Phase II and III clinical trials of galcanezumab |
Safety and tolerability
In a small number of healthy male subjects, galcanezumab was well tolerated when administered as a single subcutaneous dose ranging from 1 to 600 mg and after four consecutive doses of 150 mg administered over 6 weeks. The most common treatment-emergent adverse events (TEAEs) were headache, nasopharyngitis, hematuria, and contact dermatitis; they were transient, with no apparent relationship with the prolonged systemic drug exposure, due to the long half-life of the MAb. There were no apparent differences between galcanezumab dose groups or between galcanezumab dose groups and placebo in terms of frequency and type of any TEAEs (with the exception of hematuria that was absent in the placebo arm) or changes from baseline in vital signs (ie, pulse rate, systolic and diastolic blood pressure, and body temperature), laboratory values, or electrocardiogram (ECG) parameters. The administration of galcanezumab was not associated with time or dose-related cardiovascular or hepatotoxic effects.72
The safety and the tolerability of monthly galcanezumab in migraine patients have been further demonstrated in both randomized double-blind Phase II studies62,74 and Phase III studies.64,65,85 A similar profile of TEAEs was reported in both the placebo group and active arm/s, except for EVOLVE-2 where the proportion of patients who referred at least one TEAE was significantly greater in the galcanezumab 240 mg group than in the placebo group (71.5% vs 62.3%) (Table 4). Across all trials, most TEAEs were of mild to moderate intensity and transient. The profile of TEAEs was consistent with a peripheral site of action for galcanezumab. TEAEs related to the injection site, such as injection-site pain, injection-site erythema, and injection-site pruritus, urinary tract infections, upper respiratory tract infections, and nasopharyngitis were frequently reported. In particular, in Phase III trials, injection-site pain was the most common TEAE in all three treatment groups without statistically significant differences (Table 5). Furthermore, no clinically significant differences were found in mean change from baseline for vital signs, body weight,64,65,85 laboratory values, and ECGs85 between the active groups and the placebo arm.
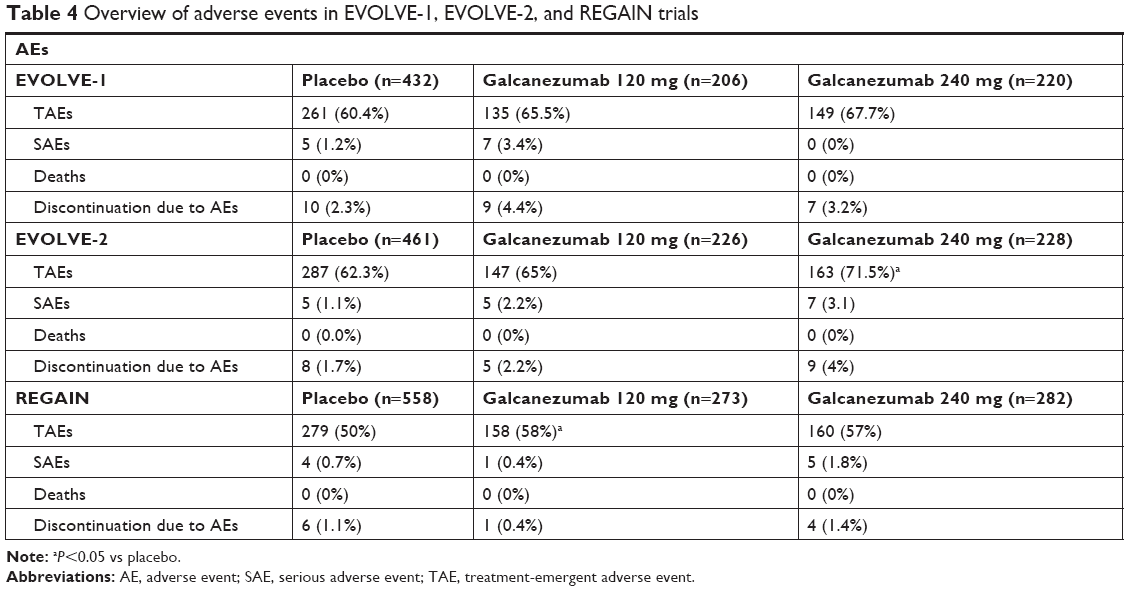 | Table 4 Overview of adverse events in EVOLVE-1, EVOLVE-2, and REGAIN trials |
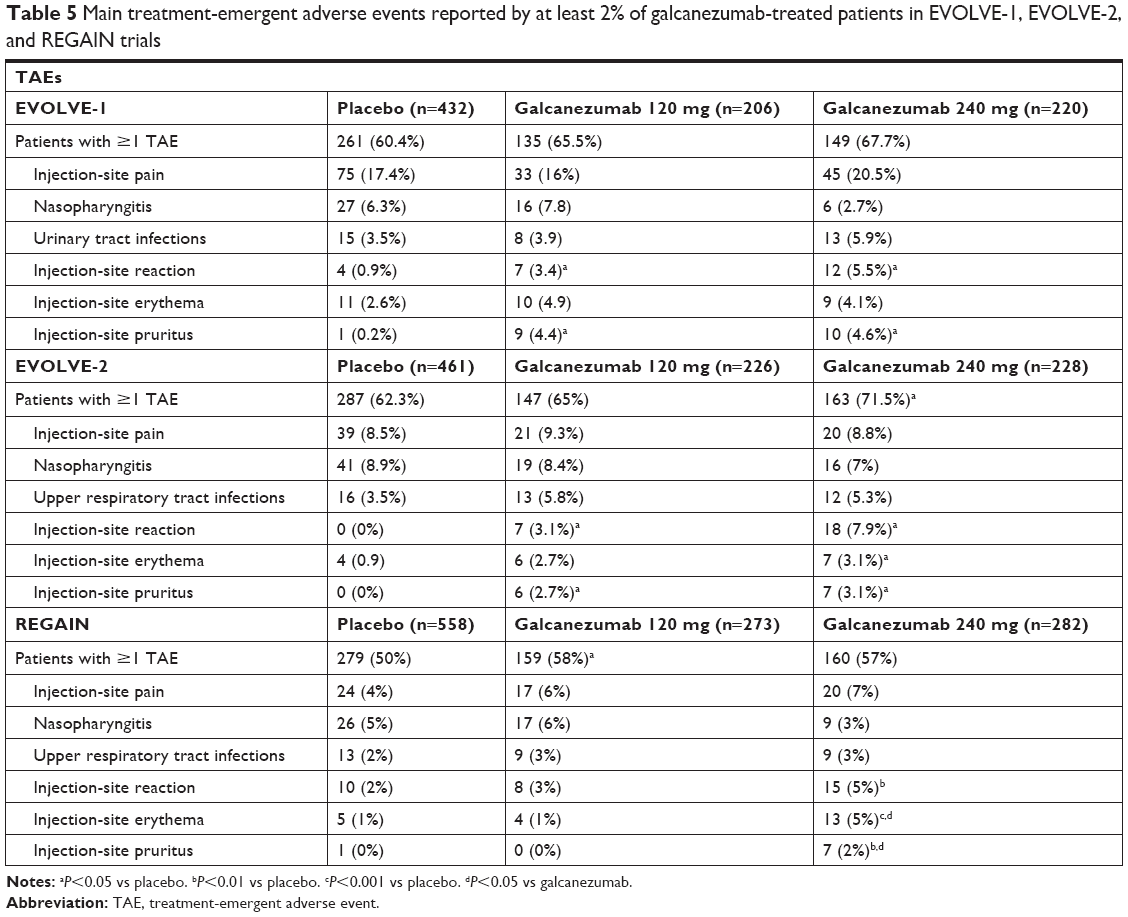 | Table 5 Main treatment-emergent adverse events reported by at least 2% of galcanezumab-treated patients in EVOLVE-1, EVOLVE-2, and REGAIN trials |
In REGAIN, treatment-emergent suicidal ideation, assessed by the Columbia-Suicide Severity Scale (C-SSRS), was reported by the 1% of patients in the three arms of the study (four patients on placebo, three patients in the galcanezumab 120-mg group, and two patients in the galcanezumab 240-mg group), with no suicidal behavior.85
Similar to placebo, galcanezumab was associated with low discontinuation rates owing to TEAEs (<1% in Phase IIb study for all galcanezumab doses, 3.8% and 3.1% for the two galcanezumab doses in EVOLVE-1 and EVOLVE-2, respectively, and 0.9% for the two galcanezumab doses in REGAIN). In the same way, the percentage of serious adverse events (SAEs), none of which was considered to be related to galcanezumab, was low and no deaths were reported (Table 3).
In Phase II studies,62,74 the development of treatment-emergent antidrug antibodies (ADAs) following galcanezumab administration did not appear to have any clinically meaningful effect on safety profile, pharmacokinetics, or mechanism of action. These results were confirmed in larger populations where treatment-emergent ADAs and neutralizing ADAs, antibodies that recognize the target-binding sites on galcanezumab and compete with its binding to CGRP in vitro, showed no impact on either safety or efficacy.64,65,85
The safety and tolerability profile of galcanezumab has been furtherly characterized in a Phase III, long-term, open-label safety study, in which galcanezumab 120 or 240 mg was administered subcutaneously once monthly for a year, in adult patients with EM and CM.86 The completion rate was high, with 77.8% of patients completing all 12 months of treatment, 3.7% of patients experienced an SAE, and 4.8% discontinued due to AEs. TEAEs with a frequency ≥10% of patients in either dose group were injection-site pain, nasopharyngitis, upper respiratory tract infection, injection-site reaction, back pain, and sinusitis. As shown in previous studies, laboratory values, vital signs, ECGs, and treatment-emergent ADAs did not show any clinically meaningful differences between galcanezumab doses. Although nearly 17% of the patients had comorbid depression and four patients reported suicidal ideation on the C-SSRS, no treatment-emergent suicidal behavior was registered.86
Patient-focused perspectives
The relevance given to patient-reported outcome measures (PROMs) has been growing in recent years and is especially important in pain conditions, such as migraine. Accordingly, some PROMs have been assessed in trials aimed at establishing galcanezumab efficacy.
In ART-01, patients treated with galcanezumab showed a greater improvement in quality of life than did those who were administered placebo, as highlighted by the Migraine Specific Quality of Life (MSQL) and the Headache Impact Text (HIT-6) scores at week 12; however, no formal statistical analyses were performed on these data.62 In the dose-ranging trial, a post hoc secondary analysis showed that, in comparison with placebo, galcanezumab 120 mg was associated with significant functional improvements as reflected by changes in MSQL scores, at 12 weeks post treatment. Reduction in MHD was associated with improvements in MSQL and reductions in HIT-6 scores, suggesting that galcanezumab may have a benefit on headache frequency, as well as on disease-specific health-related quality of life and disease burden.96 In the EVOLVE-1 and EVOLVE-2 trials, treatment with both 120 mg and 240 mg dosages of galcanezumab was associated with statistically significant reduced functional impairment due to migraine as measured in the MSQ role-function restrictive domain at month 6 vs placebo. Similarly, significant improvement in patients’ global impression of severity of their disease estimated by the Patient Global Impression of Severity (PGI-S) rating and in total Migraine Disability Assessment (MIDAS) scores was detected in comparison with placebo at the end of the 6-month treatment period.64,65 In the REGAIN study, a statistically significant improvement in the MS role-function restrictive domain and in PGI-S rating was identified at month 3 in the group treated with galcanezumab 240 mg compared to the placebo arm.85 In the Phase III, long-term, open-label safety study, at least 69% of patients treated with galcanezumab responded with high levels of overall satisfaction, preference, and less impact from side effects over previous treatments at months 1, 6, and 12. In this trial, there were within-group reductions from baseline in migraine-specific healthcare resource utilization (per 100 patient-years) with galcanezumab for healthcare professional visits (from 173.4 to 59.6, statistically significant for both arms), emergency room visits (from 20.2 to 4.7, statistically significant for the galcanezumab 240 mg arm), and hospital admissions (from 3.7 to 0.4) during the treatment period.87 Of the 270 patients who participated in the study, 179 used both the prefilled syringe and the autoinjector at least once. Patient-rated ease of usability was assessed with the Subcutaneous Administration Assessment Questionnaire (SQAAQ) and compared between devices. Over 90% of the patients (combined dose groups) reported positive experiences with the first use of the autoinjector, and these ratings remained very positive with subsequent use. A higher proportion of “agree/strongly agree” responses on the SQAAQ items were reported with the autoinjector than the prefilled syringe.76
Conclusion and place in therapy
According to available data, galcanezumab is safe and efficacious in preventing migraine in EM patients, also reducing disability and functional impairment due to the disorder. The high tolerability of this drug, as shown by the low percentages of discontinuations during the clinical trials, creates a significant premise for good adherence to treatment in real-life patients. Hopefully, and similar to results obtained with other MAbs,32 efficacy and safety will be proved also for CM. The placement of galcanezumab in the current therapeutic scenario will be a revolution for migraine patients, and probably in a less near future for patients affected by other primary headaches (eg, cluster headache). After years from the launch of triptans and for the first time after methysergide has been withdrawn from the market, migraine patients may have access to a mechanism-driven therapy. Importantly, the treatment schedule will save patients from daily intake of drugs, favoring their adherence97 and, consequently, the effectiveness of the treatment. The real value of galcanezumab, together with that of other MAbs, should be calculated considering not only direct costs due to the treatment (ie, drug costs), but also indirect costs prevented, such as visits to the emergency room and absenteeism. To this aim, the precise definition of the cardiovascular safety of galcanezumab and similar drugs will be fundamental. In addition to the abovementioned results emerging from clinical trials, available data collected for erenumab, which did not impair exercise time in patients with high cardiovascular risk,98 support that inhibition of the CGRP receptor does not favor myocardial ischemia occurrence. Finally, according to the distribution of the clinical response observed in the trials, with some patients showing excellent responses and others not responding at all, it is likely that in the future a differential place in therapy may be considered for diverse migraine endophenotypes, hopefully identifiable through a reliable biomarker – that, however, still has to be found. Additional data are needed to draw a complete profile, in terms of both efficacy and safety, of this new drug class, including galcanezumab, and to optimally place it in therapy. The recent release of marketing authorization from both the US Food and Drug Administration (erenumab, galcanezumab) and the European Medicines Agency (erenumab) for different antibodies blocking the CGRP pathway, allowing their use in real practice, will be fundamental to this aim.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Dr Guerzoni participated as coinvestigator in the I5Q-MC-CGAI trial (NCT02614261) and in the I5Q-MC-CGAW trial (NCT03559257). Dr Lupi participated as coinvestigator in the I5Q-MC-CGAI trial (NCT02614261), in the I5Q-MC-CGAL trial (NCT02397473), and in the I5Q-MC-CGAM trial (NCT02438826). Dr Benemei and Dr Negro report no conflicts of interest in this work.
References
Stovner L, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193–210. | ||
GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. | ||
Linde M, Gustavsson A, Stovner LJ, et al. The cost of headache disorders in Europe: the Eurolight project. Eur J Neurol. 2012;19(5):703–711. | ||
Antonaci F, Ghiotto N, Wu S, Pucci E, Costa A. Recent advances in migraine therapy. Springerplus. 2016;5(1):637. | ||
Lipton RB. Tracing transformation: chronic migraine classification, progression, and epidemiology. Neurology. 2009;72(5 Suppl):S3–S7. | ||
Negro A, Rocchietti-March M, Fiorillo M, Martelletti P. Chronic migraine: current concepts and ongoing treatments. Eur Rev Med Pharmacol Sci. 2011;15(12):1401–1420. | ||
Negro A, Curto M, Lionetto L, Guerzoni S, Pini LA, Martelletti P. A critical evaluation on MOH current treatments. Curr Treat Options Neurol. 2017;19(9):32. | ||
Kashipazha D, Ghadikolaei HS, Siavashi M. Levetiracetam in compare to sodium valproate for prophylaxis in chronic migraine headache: a randomized double-blind clinical trial. Curr Clin Pharmacol. 2017;12(1):55–59. | ||
Assarzadegan F, Tabesh H, Hosseini-Zijoud SM, et al. Comparing zonisamide with sodium valproate in the management of migraine headaches: double-blind randomized clinical trial of efficacy and safety. Iran Red Crescent Med J. 2016;18(9):e23768. | ||
Diener HC, Gendolla A, Feuersenger A, et al. Telmisartan in migraine prophylaxis: a randomized, placebo-controlled trial. Cephalalgia. 2009;29(9):921–927. | ||
Stovner LJ, Linde M, Gravdahl GB, et al. A comparative study of candesartan versus propranolol for migraine prophylaxis: a randomised, triple-blind, placebo-controlled, double cross-over study. Cephalalgia. 2014;34(7):523–532. | ||
Hesami O, Sistanizad M, Asadollahzade E, Johari MS, Beladi-Moghadam N, Mazhabdar-Ghashghai H. Comparing the effects of atorvastatin with sodium valproate (divalproex) on frequency and intensity of frequent migraine headaches: a double-blind randomized controlled study. Clin Neuropharmacol. 2018;41(3):94–97. | ||
Ebrahimi-Monfared M, Sharafkhah M, Abdolrazaghnejad A, Mohammadbeigi A, Faraji F. Use of melatonin versus valproic acid in prophylaxis of migraine patients: a double-blind randomized clinical trial. Restor Neurol Neurosci. 2017;35(4):385–393. | ||
Cho SJ, Song TJ, Chu MK. Treatment update of chronic migraine. Curr Pain Headache Rep. 2017;21(6):26. | ||
Negro A, D’Alonzo L, Martelletti P. Chronic migraine: comorbidities, risk factors, and rehabilitation. Intern Emerg Med. 2010;5(Suppl 1):S13–S19. | ||
Lionetto L, Borro M, Curto M, et al. Choosing the safest acute therapy during chronic migraine prophylactic treatment: pharmacokinetic and pharmacodynamic considerations. Expert Opin Drug Metab Toxicol. 2016;12(4):399–406. | ||
Lipton RB, Bigal ME, Diamond M, et al; AMPP Advisory Group. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343–349. | ||
Hepp Z, Dodick DW, Varon SF, Gillard P, Hansen RN, Devine EB. Adherence to oral migraine-preventive medications among patients with chronic migraine. Cephalalgia. 2015;35(6):478–488. | ||
Bigal ME, Serrano D, Reed M, Lipton RB. Chronic migraine in the population: burden, diagnosis, and satisfaction with treatment. Neurology. 2008;71(8):559–566. | ||
Blumenfeld AM, Bloudek LM, Becker WJ, et al. Patterns of use and reasons for discontinuation of prophylactic medications for episodic migraine and chronic migraine: results from the second International burden of migraine study (IBMS-II). Headache. 2013;53(4):644–655. | ||
Hepp Z, Bloudek LM, Varon SF. Systematic review of migraine prophylaxis adherence and persistence. J Manag Care Pharm. 2014;20(1):22–33. | ||
Ramsey RR, Ryan JL, Hershey AD, Powers SW, Aylward BS, Hommel KA. Treatment adherence in patients with headache: a systematic review. Headache. 2014;54(5):795–816. | ||
Dekker F, Knuistingh Neven A, Andriesse B, et al. Prophylactic treatment of migraine; the patient’s view, a qualitative study. BMC Fam Pract. 2012;13(1):13. | ||
Rozen TD. Migraine prevention: what patients want from medication and their Physicians (a headache specialty clinic perspective). Headache. 2006;46(5):750–753. | ||
Peres MFP, Silberstein S, Moreira F, et al. Patients’ preference for migraine preventive therapy. Headache. 2007;47(4):540–545. | ||
Kowacs PA, Piovesan EJ, Tepper SJ. Rejection and acceptance of possible side effects of migraine prophylactic drugs. Headache. 2009;49(7):1022–1027. | ||
Smelt AFH, Eijsenga SJ, Assendelft WJJ, Blom JW. Acceptance of preventive treatment in migraine patients: results of a survey. Eur J Gen Pract. 2012;18(3):143–148. | ||
Goadsby PJ. The vascular theory of migraine – a great story wrecked by the facts. Brain. 2009;132(Pt 1):6–7. | ||
Pietrobon D, Moskowitz MA. Pathophysiology of migraine. Annu Rev Physiol. 2013;75(1):365–391. | ||
Messlinger K. Migraine: where and how does the pain originate? Exp Brain Res. 2009;196(1):179–193. | ||
Raddant AC, Russo AF. Calcitonin gene-related peptide in migraine: intersection of peripheral inflammation and central modulation. Expert Rev Mol Med. 2011;13:e36. | ||
Edvinsson L, Haanes KA, Warfvinge K, Krause DN. CGRP as the target of new migraine therapies – successful translation from bench to clinic. Nat Rev Neurol. 2018;14(6):338–350. | ||
Russell FA, King R, Smillie SJ, Kodji X, Brain SD. Calcitonin gene-related peptide: physiology and pathophysiology. Physiol Rev. 2014;94(4):1099–1142. | ||
Mulderry PK, Ghatei MA, Bishop AE, Allen YS, Polak JM, Bloom SR. Distribution and chromatographic characterisation of CGRP-like immunoreactivity in the brain and gut of the rat. Regul Pept. 1985;12(2):133–143. | ||
Eftekhari S, Salvatore CA, Calamari A, Kane SA, Tajti J, Edvinsson L. Differential distribution of calcitonin gene-related peptide and its receptor components in the human trigeminal ganglion. Neuroscience. 2010;169(2):683–696. | ||
Eftekhari S, Salvatore CA, Johansson S, Chen TB, Zeng Z, Edvinsson L. Localization of CGRP, CGRP receptor, PACAP and glutamate in trigeminal ganglion. Relation to the blood-brain barrier. Brain Res. 2015;1600:93–109. | ||
Walker CS, Hay DL. CGRP in the trigeminovascular system: a role for CGRP, adrenomedullin and amylin receptors? Br J Pharmacol. 2013;170(7):1293–1307. | ||
Gallai V, Sarchielli P, Floridi A, et al. Vasoactive peptide levels in the plasma of young migraine patients with and without aura assessed both interictally and ictally. Cephalalgia. 1995;15(5):384–390. | ||
Cernuda-Morollón E, Larrosa D, Ramón C, Vega J, Martínez-Camblor P, Pascual J. Interictal increase of CGRP levels in peripheral blood as a biomarker for chronic migraine. Neurology. 2013;81(14):1191–1196. | ||
Goadsby PJ, Edvinsson L, Ekman R. Vasoactive peptide release in the extracerebral circulation of humans during migraine headache. Ann Neurol. 1990;28(2):183–187. | ||
Goadsby PJ, Edvinsson L. The trigeminovascular system and migraine: studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Ann Neurol. 1993;33(1):48–56. | ||
Sarchielli P, Alberti A, Codini M, Floridi A, Gallai V. Nitric oxide metabolites, prostaglandins and trigeminal vasoactive peptides in internal jugular vein blood during spontaneous migraine attacks. Cephalalgia. 2000;20(10):907–918. | ||
Juhasz G, Zsombok T, Jakab B, Nemeth J, Szolcsanyi J, Bagdy G. Sumatriptan causes parallel decrease in plasma calcitonin gene-related peptide (CGRP) concentration and migraine headache during nitroglycerin induced migraine attack. Cephalalgia. 2005;25(3):179–183. | ||
Lassen LH, Jacobsen VB, Haderslev PA, et al. Involvement of calcitonin gene-related peptide in migraine: regional cerebral blood flow and blood flow velocity in migraine patients. J Headache Pain. 2008;9(3):151–157. | ||
Hansen JM, Hauge AW, Olesen J, Ashina M. Calcitonin gene-related peptide triggers migraine-like attacks in patients with migraine with aura. Cephalalgia. 2010;30(10):1179–1186. | ||
Asghar MS, Hansen AE, Amin FM, et al. Evidence for a vascular factor in migraine. Ann Neurol. 2011;69(4):635–645. | ||
Recober A, Kuburas A, Zhang Z, Wemmie JA, Anderson MG, Russo AF. Role of calcitonin gene-related peptide in light-aversive behavior: implications for migraine. J Neurosci. 2009;29(27):8798–8804. | ||
Olesen J, Diener HC, Husstedt IW, et al; BIBN 4096 BS Clinical Proof of Concept Study Group. Calcitonin gene-related peptide receptor antagonist BIBN 4096 BS for the acute treatment of migraine. N Engl J Med. 2004;350(11):1104–1110. | ||
Ho TW, Ferrari MD, Dodick DW, et al. Efficacy and tolerability of MK-0974 (telcagepant), a new oral antagonist of calcitonin gene-related peptide receptor, compared with zolmitriptan for acute migraine: a randomised, placebo-controlled, parallel-treatment trial. Lancet. 2008;372(9656):2115–2123. | ||
Connor KM, Shapiro RE, Diener HC, et al. Randomized, controlled trial of telcagepant for the acute treatment of migraine. Neurology. 2009;73(12):970–977. | ||
Voss T, Lipton RB, Dodick DW, et al. A phase IIb randomized, double-blind, placebo-controlled trial of ubrogepant for the acute treatment of migraine. Cephalalgia. 2016;36(9):887–898. | ||
Hewitt DJ, Aurora SK, Dodick DW, et al. Randomized controlled trial of the CGRP receptor antagonist MK-3207 in the acute treatment of migraine. Cephalalgia. 2011;31(6):712–722. | ||
Marcus R, Goadsby PJ, Dodick D, Stock D, Manos G, Fischer TZ. BMS-927711 for the acute treatment of migraine: a double-blind, randomized, placebo controlled, dose-ranging trial. Cephalalgia. 2014;34(2):114–125. | ||
Sun H, Dodick DW, Silberstein S, et al. Safety and efficacy of AMG 334 for prevention of episodic migraine: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. 2016;15(4):382–390. | ||
Tepper S, Ashina M, Reuter U, et al. Safety and efficacy of erenumab for preventive treatment of chronic migraine: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017;16(6):425–434. | ||
Goadsby PJ, Reuter U, Hallström Y, et al. A controlled trial of Erenumab for episodic migraine. N Engl J Med. 2017;377(22):2123–2132. | ||
Dodick DW, Goadsby PJ, Silberstein SD, et al; ALD403 study investigators. Safety and efficacy of ALD403, an antibody to calcitonin gene-related peptide, for the prevention of frequent episodic migraine: a randomised, double-blind, placebo-controlled, exploratory phase 2 trial. Lancet Neurol. 2014;13(11):1100–1107. | ||
Bigal ME, Dodick DW, Rapoport AM, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of high-frequency episodic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2B study. Lancet Neurol. 2015;14(11):1081–1090. | ||
Bigal ME, Dodick DW, Krymchantowski AV, et al. TEV-48125 for the preventive treatment of chronic migraine: Efficacy at early time points. Neurology. 2016;87(1):41–48. | ||
Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. 2017;377(22):2113–2122. | ||
Dodick DW, Silberstein SD, Bigal ME, et al. Effect of Fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. 2018;319(19):1999–2008. | ||
Dodick DW, Goadsby PJ, Spierings ELH, Scherer JC, Sweeney SP, Grayzel DS. Safety and efficacy of LY2951742, a monoclonal antibody to calcitonin gene-related peptide, for the prevention of migraine: a phase 2, randomised, double-blind, placebo-controlled study. Lancet Neurol. 2014;13(9):885–892. | ||
Skljarevski V, Oakes TM, Zhang Q, et al. Effect of different doses of Galcanezumab vs placebo for episodic migraine prevention: a randomized clinical trial. JAMA Neurol. 2018;75(2):187–193. | ||
Stauffer VL, Dodick D, Zhang M, Carter JN, Ailani J, Conley RR. Evaluation of Galcanezumab for the prevention of episodic migraine: The EVOLVE-1 randomized clinical trial. JAMA Neurol. 2018;75(9):1080–1088. | ||
Skljarevski V, Matharu M, Millen BA, Ossipov MH, Kim BK, Yang JY. Efficacy and safety of galcanezumab for the prevention of episodic migraine: results of the EVOLVE-2 phase 3 randomized controlled clinical trial. Cephalalgia. 2018;38(8):1442–1454. | ||
Benschop RJ, Collins EC, Darling RJ, et al. Development of a novel antibody to calcitonin gene-related peptide for the treatment of osteoarthritis-related pain. Osteoarthritis Cartilage. 2014;22(4):578–585. | ||
Buntinx L, Vermeersch S, de Hoon J. Development of anti-migraine therapeutics using the capsaicin-induced dermal blood flow model. Br J Clin Pharmacol. 2015;80(5):992–1000. | ||
Van der Schueren BJ, Rogiers A, Vanmolkot FH, et al. Calcitonin gene-related peptide 8–37 antagonizes capsaicin-induced vasodilation in the skin: evaluation of a human in vivo pharmacodynamic model. J Pharmacol Exp Ther. 2008;325(1):248–255. | ||
Holzer P. Local effector functions of capsaicin-sensitive sensory nerve endings: involvement of tachykinins, calcitonin gene-related peptide and other neuropeptides. Neuroscience. 1988;24(3):739–768. | ||
Van der Schueren BJ, de Hoon JN, Vanmolkot FH, et al. Reproducibility of the capsaicin-induced dermal blood flow response as assessed by laser Doppler perfusion imaging. Br J Clin Pharmacol. 2007;64(5):580–590. | ||
Vermeersch S, Benschop RJ, Van Hecken A, et al. Translational pharmacodynamics of calcitonin gene-related peptide monoclonal antibody LY2951742 in a capsaicin-induced dermal blood flow model. J Pharmacol Exp Ther. 2015;354(3):350–357. | ||
Monteith D, Collins EC, Vandermeulen C, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of the CGRP binding monoclonal antibody LY2951742 (galcanezumab) in healthy volunteers. Front Pharmacol. 2017;8:740. | ||
Galcanezumab; 2006. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30372007. Accessed November 9, 2018. | ||
Oakes TMM, Skljarevski V, Zhang Q, et al. Safety of galcanezumab in patients with episodic migraine: a randomized placebo-controlled dose-ranging phase 2B study. Cephalalgia. 2018;38(6):1015–1025. | ||
Zhou H, Mascelli MA. Mechanisms of monoclonal antibody-drug interactions. Annu Rev Pharmacol Toxicol. 2011;51(1):359–372. | ||
Stauffer VL, Sides R, Lanteri-Minet M, et al. Comparison between prefilled syringe and autoinjector devices on patient-reported experiences and pharmacokinetics in galcanezumab studies. Patient Prefer Adherence. 2018;12:1785–1795. | ||
Tfelt-Hansen P. Site of effect of LY2951742 for migraine prophylaxis. Lancet Neurol. 2015;14(1):31–32. | ||
Dodick DW, Goadsby PJ, Spierings EL, Scherer JC, Sweeney SP, Grayzel DS. Site of effect of LY2951742 for migraine prophylaxis – authors’ reply. Lancet Neurol. 2015;14(1):32–33. | ||
Schankin CJ, Maniyar FH, Seo Y, et al. Ictal lack of binding to brain parenchyma suggests integrity of the blood-brain barrier for 11C-dihydroergotamine during glyceryl trinitrate-induced migraine. Brain. 2016;139(7):1994–2001. | ||
Preston JE, Joan Abbott N, Begley DJ. Transcytosis of macromolecules at the blood-brain barrier. Adv Pharmacol. 2014;71:147–163. | ||
Karasek C, Ojala E, Allison D, et al. Characterization of the intrinsic binding features of three anti-CGRP therapeutic antibodies effective in preventing migraine: a comparative pre-clinical case study of ALD403, LY-2951742, TEV-48125. In: 58th Annual Scientific Meeting of the American Headache Society. San Diego, CA; 2016:251. | ||
Khan S, Olesen A, Ashina M, Cgrp AM. CGRP, a target for preventive therapy in migraine and cluster headache: systematic review of clinical data. Cephalalgia. 2017;20:0333102417741297. | ||
Mitsikostas DD, Reuter U. Calcitonin gene-related peptide monoclonal antibodies for migraine prevention: comparisons across randomized controlled studies. Curr Opin Neurol. 2017;30(3):272–280. | ||
Rosen N, Pearlman E, Ruff D, Day K, Jim Nagy A. 100% response rate to galcanezumab in patients with episodic migraine: a post hoc analysis of the results from phase 3, randomized, double-blind, placebo-controlled EVOLVE-1 and EVOLVE-2 studies. Headache: J Head Face Pain. 2018;58(9):1347–1357. | ||
Detke HC, Goadsby PJ, Wang S, Friedman DI, Selzler KJ, Aurora SK. Galcanezumab in chronic migraine: The randomized, double-blind, placebo-controlled REGAIN study. Neurology. 2018;91(24):e2211–e2221. | ||
Camporeale A, Kudrow D, Sides R, et al. A phase 3, long-term, open-label safety study of Galcanezumab in patients with migraine. BMC Neurol. 2018;18(1):188. | ||
Ford JH, Foster SA, Stauffer VL, Aurora SK, Versijpt J, Satisfaction P. Patient satisfaction, health care resource utilization, and acute headache medication use with galcanezumab: results from a 12-month open-label study in patients with migraine. 2018;2018:2413–2424. | ||
Förderreuther S, Zhang Q, Stauffer VL, Aurora SK, Láinez MJA. Preventive effects of galcanezumab in adult patients with episodic or chronic migraine are persistent: data from the phase 3, randomized, double-blind, placebo-controlled EVOLVE-1, EVOLVE-2, and regain studies. J Headache Pain. 2018;19(1):121. | ||
Eli Lilly and Company. AAN 2018: Lilly’s galcanezumab significantly reduced monthly migraine headache days in patients with migraine who previously failed to respond to multiple preventive therapies. 2018;2:85–87. Available from: https://www.prnewswire.com/news-releases/aan-2018-lillys-galcanezumab-significantly-reduced-monthly-migraine-headache-days-in-patients-with-migraine-who-previously-failed-to-respond-to-multiple-preventive-therapies-300634848.html. Accessed February 22, 2019. | ||
Nichols R, Doty E, Sacco S, Ruff D, Pearlman E, Aurora SK. Analysis of initial nonresponders to Galcanezumab in patients with episodic or chronic migraine: results from the EVOLVE-1, EVOLVE-2, and regain randomized, double-blind, placebo-controlled studies. Headache. 2019;59(2):192–204. | ||
Eli Lilly and Company. A Study of Galcanezumab (LY2951742) in Adults With Treatment-Resistant Migraine – Full Text View – ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT03559257. Accessed August 25, 2018. | ||
Eli Lilly and Company. A Study of Galcanezumab (LY2951742) in Participants 6 to 17 Years of Age With Episodic Migraine – Full Text View – ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT03432286. Accessed August 25, 2018. | ||
Eli Lilly and Company. A Study of LY2951742 in Participants With Episodic Cluster Headache – Full Text View – ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02397473. Accessed August 25, 2018. | ||
Eli Lilly and Company. A Study of LY2951742 in Participants With Chronic Cluster Headache – Full Text View – ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02438826. Accessed August 25, 2018. | ||
Eli Lilly and Company. A Study of LY2951742 (Galcanezumab) in Participants With Cluster Headache – Full Text View – ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02797951. Accessed August 25, 2018. | ||
Ayer DW, Skljarevski V, Ford JH, Nyhuis AW, Lipton RB, Aurora SK. Measures of functioning in patients with episodic migraine: findings from a double-blind, randomized, placebo-controlled phase 2B trial with Galcanezumab. Headache. 2018;58(8):1225–1235. | ||
Seng EK, Rains JA, Nicholson RA, Lipton RB. Improving medication adherence in migraine treatment. Curr Pain Headache Rep. 2015;19(6):24. | ||
Depre C, Antalik L, Starling A, et al. A randomized, double-blind, placebo-controlled study to evaluate the effect of Erenumab on exercise time during a treadmill test in patients with stable angina. Headache. 2018;58(5):715–723. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.