")
Back to Journals » Patient Preference and Adherence » Volume 13
Older patients’ preferences and views related to non-face-to-face diabetes chronic care management: a qualitative study from southeast Louisiana
Authors Bazzano AN , Monnette AM, Wharton MK , Price-Haywood EG , Nauman E, Dominick P, Glover C, Hu G, Shi L
Received 10 January 2019
Accepted for publication 14 May 2019
Published 30 May 2019 Volume 2019:13 Pages 901—911
DOI https://doi.org/10.2147/PPA.S201072
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
AN Bazzano,1 AM Monnette,2 MK Wharton,2 EG Price-Haywood,3 E Nauman,4 P Dominick,5 C Glover,5 G Hu,6 L Shi2
1Department of Global Community Health and Behavioral Sciences, Tulane University School of Public Health and Tropical Medicine, New Orleans, LA, USA; 2Department of Health Policy and Management, Tulane University School of Public Health and Tropical Medicine, New Orleans, LA, USA; 3Ochsner Health System Center for Applied Health Services Research, New Orleans, LA, USA; 4Louisiana Public Health Institute, New Orleans, LA, USA; 5LEAD Study Steering Committee, New Orleans, LA, USA; 6Pennington Biomedical Research Center, Baton Rouge, LA, USA
Background: Management of diabetes may be uniquely challenging for older individuals with multiple chronic conditions. Health systems and policymakers have attempted to reduce barriers to chronic care management (CCM) through incentives to provide non-face-to-face care. This qualitative study aimed to investigate and present views on non-face-to-face care management held by elderly patients with diabetes and other chronic conditions in order to contribute to improved programming for this population.
Materials and methods: Semi-structured interviews were conducted with patients over the age of 64 who have been diagnosed with diabetes and at least one other chronic health condition. Interview recordings were transcribed and analyzed by experienced researchers using a thematic analytic approach, and an illustrative case study was developed.
Results: Thirty individuals participated in this study. Participants were drawn from three health systems in south Louisiana, an area with high rates of morbidity and mortality related to chronic diseases. We identified themes related to lived experiences with diabetes and other medical conditions, perception of personal health status, perceived value of non-face-to-face programs, and support needs for future programming. Additionally, we present one case study describing in detail an individual patient’s experience with non-face-to-face CCM.
Conclusion: Health systems should consider intentionally recruiting participants who would benefit most from non-face-to-face care, including higher-need, less self-sufficient patients with resource constraints, while continuing to offer in-person services. Future research should examine whether tailoring non-face-to-face programming and support to address unique barriers can further enhance diabetes care at the population level.
Keywords: diabetes complications, patient care management, aging, patient-centered care
Introduction
Approximately 25% of the United States population over the age of 65 are estimated to have diabetes1 and a third of adults of this age group in the state of Louisiana have a diagnosis of diabetes.2 Diabetes in older adults has been associated with higher mortality, reduced functional status, and increased risk of transfer to institutionalized care. 3 Chronic care management (CCM) efforts have been introduced to mitigate the impact of diabetes and improve health.4 The utility of CCM services amongst patients living with diabetes and other chronic conditions has not been well studied despite evidence that health care providers feel CCM services would be particularly beneficial for elderly patients.5 This may be particularly relevant in the “diabetes belt”, where the geographic region has been linked with different risk factors related to patient outcomes.6 Literature from several interrelated research areas is instructive for understanding relevant information pertaining to this topic.
Patient engagement in understanding how to achieve health care improvement has become a prominent strategy for improving chronic disease management and is often a feature of federally funded health research.7–9 This strategy may be especially important for elderly populations10 and for patients with chronic diseases such as diabetes that require intensive self-management.11,12
Recent qualitative studies presenting patient perspectives have illustrated areas to improve or expand upon diabetes care programming to address community needs and barriers to care, including self-management13 through a patient-centered approach.14 One such study found that particular patient characteristics impacted engagement and success in a program for diabetes and kidney disease—these included socioeconomic status, comorbidities, and patients’ previous negative experiences in health care settings.15 Another recent qualitative study explored the experiences of patients with diabetes in navigating health systems, where most participants perceived the health care system as rushed, impersonal, and fragmented. Patients in that study often faced challenges to build trusting and collaborative relationships with health care professionals in managing diabetes and its complications.16 The improvement of care coordination, appointment follow-up and engagement may be particularly relevant,17 and use of telemedicine holds promise in meeting elderly patient needs.18 A mixed methods study found that the one-on-one relationship model of care was especially beneficial for elderly patients.19 According to other qualitative studies, information sharing with patients through care management programs, or through technology such as electronic health information exchange, is a potential area of opportunity to improve patient satisfaction and outcomes.20,21
While improved patient acceptance and adherence,22 patient empowerment,23 as well as experience and enhanced care coordination from CCM program evaluations24 may be potential positive outcomes, studies also cite challenges in implementing CCM programs, such as both patient and provider education to changes in care delivery.24,25 Developing highly individualized care plans was found to be another important element of CCM implementation.26 Barriers to technology use promoting effective CCM, such as Health Information and Portability Accounting Act compliance of text messages27 and patient need for in-person along with remote technology interventions,28 are also a concern. Lastly, the health care setting and characteristics, such as workplace culture, leadership support, readiness,29 technology infrastructure,30 and patient continuity,31 may also influence provider ability to implement new clinical guidelines such as CCM. Of the available literature, most studies are quantitative and outcomes-focused.32,33
Non-face-to-face chronic care management (NFF CCM) is one potential way to improve the management of diabetes and other chronic conditions in people who are elderly. Recently, this mode of care has been incentivized through billing codes for health systems introduced by the United States Centers for Medicare and Medicaid Services (CMS).34,35 NFF CCM has shown promise as a channel for improving care for diabetes, and previous work by the research team explored patient and health system level factors related to utilization of NFF CCM,36 and a more recent companion paper described the perspectives of physicians and health system staff involved in NFF CCM in Louisiana.37
Thus far, there is scant information on the expectations and experiences of patients with diabetes regarding programs for NFF CCM. Given the key role of patient and community perspectives in improving care management for chronic diseases, this gap in the research has important implications. The current study aimed to collect information from older persons living with diabetes and at least one other chronic condition to understand patients’ views on the CCM and care coordination services they may receive, with a particular focus on any non-face-to-face aspects of those services like phone calls and patient portal messages. The information is provided in the context of the implementation of NFF CCM programs in a region of the United States with high rates of diabetes among adults, and where socioeconomic status is an important factor in access to care. Information that patients provide on programming targeted at improving their health should be used to improve quality of care and make NFF CCM more responsive to identified needs.
Methods
The current study comprises the qualitative research component of the Louisiana Experiment Assessing Diabetes outcomes (LEAD) Study, described elsewhere.36,37 Participants over the age of 64, who had diabetes and at least one other chronic condition, were purposively recruited through primary care practices in Southeast Louisiana which were partnered in the LEAD Study. A total of 30 participants were interviewed through semistructured interviews using a discussion guide. If patients had a primary caregiver such as a spouse or relative, that caregiver was also invited to participate. The sample included patients who had previously received NFF CCM, based on the presence of associated billing codes in their medical records, as well as those who had not. Recruitment channels included patient portal messages, secure emails, or phone calls. Interviews were conducted between October 2017 and February 2018 either in person or by phone, depending on the participant’s preference. Tulane University Institutional Review Board (IRB) approved the research study. The Consolidated Criteria for Reporting Qualitative Research guidelines were used to facilitate reporting of this research.38
The qualitative principal investigator and other researchers involved in the study had extensive previous professional experience conducting qualitative research. No previous relationship was established with the patient participants interviewed in the study before recruitment. Verbal informed consent was obtained (as permitted by the institutional IRB) and recorded from each participant to share their de-identified interview data, which included information on the study and objectives. Interviewers disclosed the goals and objectives of the LEAD Study with participants as well as the study funding source and multiorganization collaboration. Patient participants were also told the individual interviewer’s position as a researcher on the study, such as that they were a student researcher or member of a partner research organization.
Interview guides, the tool used to facilitate topics for discussion during interview, were first drafted in consultation with three patient partners who are active members of the LEAD Study Steering Committee. Researchers also consulted with patient stakeholders to pretest the interview guide, which included obtaining feedback from diabetes advisory groups that were regularly convened to solicit stakeholder perspectives and recommendations on various LEAD Study activities. Interview guide topics centered on how patients experience and deal with their chronic conditions, perceived benefits of NFF CCM in relation to dealing with chronic conditions, support needs for care management, and lived experiences of diabetes patients with NFF CCM.
Researchers utilized audio recordings to collect the interview data for transcription and took detailed field notes before, during, and after the 30-min interviews. Only researchers and participants were present for the interviews to ensure privacy. Transcriptions were not returned to participants for review. Data completeness and trustworthiness was considered an important priority and participants were recruited and consulted in order to ensure diverse perspectives and representation from the different partner organizations.
Thematic analysis and case study design were employed to analyze the patient interviews.39,40 Interview data was used to extract themes. Analysis was conducted by four individual coders using a preliminary list of codes which were based on transcripts of interviews, field notes, and discussion among the interviewers. Groups and preliminary candidate themes were identified after analyzing and coding samples of the total data collected and were then discussed to refine the coding guide. NVivo version 12 was used to manage qualitative data during analysis, including the identification of quotes, case studies, and coding of interview transcripts. Participants did not provide feedback on the analysis; however, patient partners on the LEAD Study Steering Committee and diabetes advisory group members were partners in preliminary analysis and engaged for feedback. Major themes within these diverse perspectives were presented and discussed among the research team and stakeholders.
Patient engagement statement
Patients and other relevant stakeholders as research partners were engaged in the conduct of the study, including planning recruitment approaches, refining and finalizing data collection forms and protocols, and reviewing and interpreting results. Authors worked collaboratively with the LEAD Study Steering Committee, including patient partners, to ensure that the final study protocol was consistent with the relevant CDC, NIDDK, and PCORI methodological standards.
Results
A total of 30 participants were interviewed for this study. The mean self-reported age of participants was 68.3 years and number of years since diagnosis with Type 2 diabetes was 14.5 years prior to the time of the study. Most study participants were women and Medicare-insured, while the remainder of participants were dual eligible for Medicare and Medicaid or privately insured. Participants all had a diagnosis of Type 2 diabetes and at least one comorbid condition, which included but were not limited to hypertension, cardiovascular disease, arthritis, hyperlipidemia, cancer, severe injury or disability, kidney failure, mental health conditions, and sleep apnea. All participants had experience with non-face-to-face care in the course of their interactions with the health system, and approximately 13% had participated in NFF CCM programs reimbursed by Medicare. Demographic characteristics of the sample are presented in Table 1.
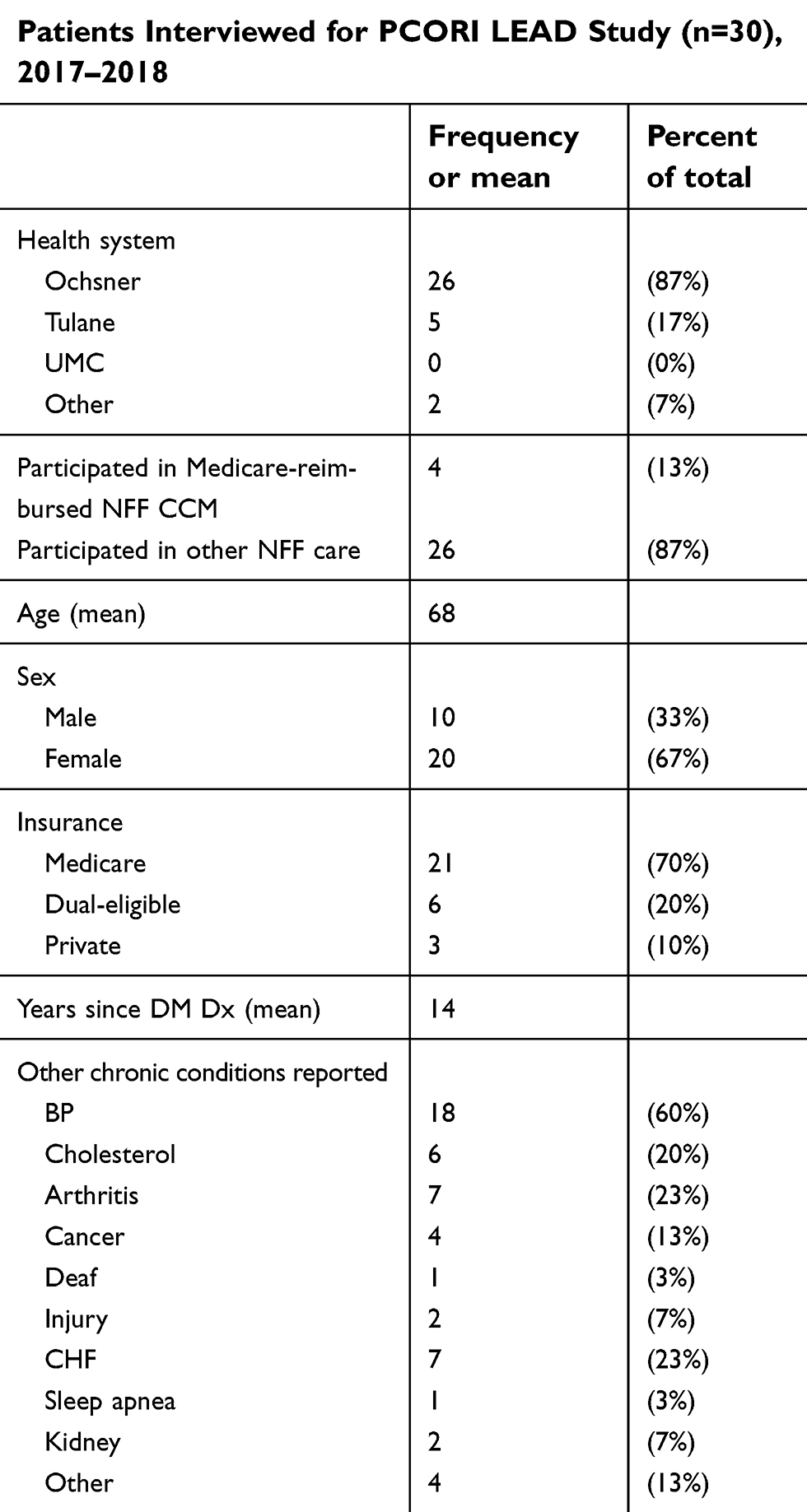 | Table 1 Patient characteristics |
Themes that emerged from the data included dealing with diabetes and chronic conditions in daily life, patient enthusiasm for NFF CCM based on perceived self-efficacy, lived experiences with value of NFF CCM programs, and support needs for management of chronic conditions.
Dealing with diabetes and chronic conditions in daily life
Participants were asked to describe how their chronic conditions impact their lives. Self-reported perceptions of general health and ability to self-manage health conditions varied greatly by the participant. One common theme was self-sufficiency, where patients reported a relatively higher comfort level and ability to use technology, such as patient portals and internet resources for self-education. More self-sufficient patients also reported having greater levels of family support in accessing health care services, such as with transportation, and with understanding and adhering to medication and treatment schedules. Family support with other needs included accessing healthy food and housework.
[My health conditions don’t impact my life] terribly so. I try to get a little bit more exercise than I would normally get, but I’m not very good at that. I’ve got pills I have to take in the morning and evening, and I keep trying to make the diet better … I’ve been successful at controlling the diabetes … There’s not a whole lot more to manage. – 67-year-old male
In many cases, even when the patient reported to have five or more long-term chronic conditions, injuries, or disabilities, these patients tended to also report that they were relatively healthy. One participant who described her health as pretty good reported the following:
[I have] heart disease, high blood pressure, COPD, acid reflux, osteoarthritis, and I have sleep disorder, sleep apnea … I suffer from atrial fibrillation, and I have a pacemaker … . My diabetes- I’ve gotten it under control … There’s a lot of things wrong with me, but I gotta say I get around pretty good.” – 67-year-old female
Some patients reported a recent diagnosis of Type 2 diabetes (within the last 2 years), while others interviewed had been diagnosed for 20 or more years. The patients who had a recent diagnosis expressed interest and engagement in CCM and controlling their diabetes, while people who had been living with the diagnosis longer reported having their self-management methods and routine more established.
Another common theme was having it under control:
I was diagnosed a year ago mid-December with the diabetes, and I had a triple bypass the January 21, 2012. I’ve been going to [Health System Name] here in the North for – well, since I was diagnosed with the diabetes, which was a little over a year ago … I did (go to the doctor more frequently after my diagnosis) there for a while, but it’s lightened off now, because my numbers have all been good. Everything’s under control. – 67-year-old male
Patient enthusiasm for non-face-to-face care varied depending on perceived self-efficacy
Several patients expressed interest in the non-face-to-face CCM program and services, while some patients reported that NFF CCM services would not be helpful to them as they are already able to self-manage their chronic conditions. For the patients who communicated that it would be of benefit to them, they cited a need to have regular check-ins and an individual with whom they could build a rapport and ask questions when needed. A participant expressed it this way:
It would be nice if they would call you to see if you’re feeling better, or if their treatment suggestion is working for you … Or maybe just, “How are you doing with your blood sugar?” But mainly, “How are you doing?” would be nice. – 64-year-old female
For the patients who did not feel NFF CCM would be beneficial to them, they cited that they would not want to pay for the services and that they could identify and utilize needed services without assistance from a care coordinator. One participant described it like this:
I don’t think I’d pay for [NFF CCM]. Typically, stuff like that, I don’t have much confidence in, because I’m generally bigger, better at figuring stuff out than they are. – 67-year-old male
Another participant described that their relationship with their care providers was strong enough that they did not need ancillary NFF services:
I have no problem with my doctors. I can call ‘em if I need ‘em. I get return calls. I have no problem getting appointments set. Even if I’m in distress about something, I can call ‘em and they’ll be wanting to see me the same day. - Female, 67
Another patient affirmed the value in having access to an attentive nurse care coordinator through a NFF CCM program that provided medication assistance, but that his need for NFF CCM was not ongoing once he established a routine that worked for him.
[the NFF CCM] kept me more conscious of what was going on and helped me get back on track … she [the nurse] did, at one point, help me to change – when it wasn’t coming down like we hoped it would, she met with my primary care physician and had them change my injection … she was very conscientious and monitoring what I was doing and offering suggestions on what I could do to get it back in line. Well, he had projected that I would need to use that service for about six months. It’s not something that – once I’m back on track right now, if I keep it up, I don’t see the need to continue working with her. - 68-year-old male
Some patients described not wanting to be contacted by phone, while others would welcome a phone call. Patient comfort level with the technologies used to provide NFF CCM also factored into patient perception of the value of NFF CCM programs. Patients reported a wide range of access to and comfort using technologies such as web-based tools like patient portals and the internet for information versus patients who did not have internet or a computer at home, who may be more advantaged by participation in an over-the-phone NFF CCM program. One participant commented:
I think that I would like both (emails and phone calls), because, when you talk to someone, you can really relay what you are trying to (communicate) better than you can in a text or a voicemail. - Female, 66
… it’s much easier. If I receive the phone calls at home I don’t have to travel 40 minutes to get to the doctor’s office. My health is number one, and the more help I can get with it, the better I feel. Anytime that I don’t – if I forget my blood pressure my health system on my phone will remind me that I did not take my blood pressure that day, and I love that … - 66-year-old male
Further, transportation was a key theme that arose from conversations with patients. The majority of patients noted that accessing their primary care and specialists required some effort. In the more rural communities, patients reported 20-min to 30-min drives to their health care providers, and in more urban areas, public transportation was cited as a means of access. Some patients also discussed reliance on family members, caregivers, and friends for rides to their health care providers, signaling populations who may benefit more from NFF CCM. The transportation needs varied greatly by participant. For example, one patient stated:
No, (getting to the doctor is not that difficult) because I can walk right out of my door and walk right across the street and catch the bus or I can have my daughter pick me up and she’ll bring me. It’s not that difficult – it’s just cold out there but I bundle up. – 68 year-old female
Another patient described driving to appointments as being easy:
I’m pretty self-sufficient. I drive. I take myself pretty much where I want to go. - Female, 66
Some patients who would likely benefit from NFF CCM required intensive care support, including transportation, medication assistance, help with daily tasks, and caregiver co-management of the patients’ conditions. A caregiver for a patient described it this way:
I’ll speak to caregiving for my sister … Well after about [Home Health Management Company], to help manage those daily tasks … Her medicines, she had them distributed through her house in three different main portions and there was no rhyme or reason as to how she took her pills. So, within the first I guess year or two, I discovered that and had to manage her medicines … Along the way with her condition she did some bizarre things driving and some friends reported it to me, her daughter reported it to me and working with the neurologist we sought to actually take the car away from her. So I got the backing from the neurologist although I heard several times that I took the car away, a cross that a care giver has to bear when they’re involved in trying to take care of the loved one. – 68-year-old male on caregiving for his sister with over 6 chronic conditions
Lived experiences with value of NFF CCM programs
Several patients who were enrolled in the NFF CCM programs were able to speak to their experiences in it and the values of the program.
I have one of the nurses from [Health System Name]. She keeps up with me and monitor me and everything, and she calls me like about, oh, once or twice a week. And so if I don’t hear from her, within a week she make sure she get back with me. But we started out with calls once a week – no, twice a week – and then she says things were better; “I feel like I’m more comfortable with the issues, so I’m calling you like every two weeks.” That’s one of the registered nurses … I have her phone number in my phone. – 67-year-old female
[I have a care coordinator]. She’s a nurse, but she works with my doctor, and she’ll call me. We’ll discuss my diabetic … like when I write down my diabetic numbers. And she’ll call me like … she hasn’t called me this month. She called me last month, so she’ll be calling me sometime next week or the week after to find out how my diabetes running … – 68-year-old female
Activities that patients reported were a part of the service included regular phone calls from a nurse or care coordinator to check in on the patient, development, and review of a care management plan and connection to resources when needed.
Oh, I can’t do no damn activities, woman. I can’t walk two floors, no. I’ve been trying though. I see my doctor, my diabetic doctors. I got a whole bunch of them. [The NFF CCM nurse] told me that she was that she was gonna call me, and we was gonna talk about my diabetic plan – you know, how it’s going and how high it is and how low it is and what my medicine was that I was taking … if it’s too high she’s gonna let me know, Well, that’s a little bit too high … once or twice it might be a little high. - 68-year-old female
Patients expressed that they perceived the program and services they had received to be effective and beneficial to them.
(I think my care coordinator helps me) Because she talks to me, and she tells me that if it’s too high she’s gonna let me know, “Well, that’s a little bit too high,” and if it’s too low she’s gonna let me know, but it would never be too low. It always be like … once or twice it might be a little high. And then before you know it, boom it’s gone down to normal. - 68-year-old female
One patient in particular spoke to the value of NFF CCM through her care coordinator and how having a relationship with that coordinator enhanced her care and well-being. The participant’s story is illustrated as a detailed case study in Box S1.
Support needs for management of chronic conditions
Patients were asked to consider what their needs for support were in relation to the management of diabetes and other chronic conditions. Diet and nutrition were the main topics participants mentioned as important for NFF CCM programs.
[The nutritionist’s] recommendation was more low-carb and watching my sugars. But it wasn’t a rigid diet. I have since decided … to put myself on the Mediterranean diet … It seems pretty healthy to me … She told me the last time I met, if I had any questions to please get in contact with her. I just haven’t had the need to. - 66-year-old female
Where participants reported being relatively healthy and with a high degree of self-efficacy, they described the information they were already receiving through diabetes care programs as “common sense” and thus less valuable.
Right after I was diagnosed, they called me and I went in for a class, which was kinda the dumbest thing I’ve ever seen. They’re basically saying, “Don’t eat sugar.” Come on, I picked that up on the internet. – 67-year-old male
One patient expressed being fatigued with the information provided through diabetes education and nutrition counseling and needing more support for implementing behavior change, rather than education through NFF CCM.
I have been to a diabetes education class which they offer, dietary suggestions and things like that. But as far as anybody sitting down with me and telling me, “This is what you need to eat, this is what you don’t need to eat,” I already know that at my age. I just don’t practice it. – 70-year-old female
Frequently participants reported knowing what to eat and that diet and exercise are important, but finding it hard to continuously apply this knowledge in their day-to-day lives. Some patients articulated that there would be value in seeing a dietitian or diabetes educator in-person as well as having the support and community of group classes that would not be afforded by NFF CCM interventions. One participant described how a peer approach would suit them best:
If they could get a group together … and I feel like if the support would have been stronger, or if there would have been … walking clubs and stuff like that. If you had a group that could cheer you on for your diabetes numbers … I think that would be good. −64-year-old female
The perceived value of in-person care management programs, such as group classes or individual appointments with diabetes educators or registered dieticians, was often contrasted with a non-face-to-face approach. Some patients and caregivers spoke to the value of talking to a provider in-person during patient visits.
I felt empowered to just ask them (specialists during his sister’s in-person patient visit) and (the specialists) were so cordial and interactive with me on the different situations that were arising (with my sister’s health) and that – believe it or not – that’s where I really saw the coordination and of course behind the scenes I have no knowledge to know what was going on. – 68-year-old male caregiver
I like sitting down face to face because we can always talk a little bit more about my numbers off of my machines and things like that … we talk about all of that. -Female, 66
Patients expressed the value of having personal, caring relationships with their primary care doctors and some also articulated experiences of these experiences with their providers.
… if the doctor’s not doing what they should for me and I don’t think they’re concerned with my wellbeing, I don’t wanna see that doctor. And that’s the way I’ve always been … So you don’t have time for me, I don’t have time for you either. So bye-bye” – 68-year-old female
Discussion
The clinical relevance of this study centers on recommendations for the improvement of NFF CCM programs. One clear strategy that emerged from this study was the potential for NFF CCM programs to be more effective when intentionally recruiting participants who would benefit most from the program: higher-need, less self-sufficient, and less technology savvy patients with few resources and family support. Also, continuing to offer in-person services in addition to NFF CCM services is likely to be of benefit to patients. One challenge in identifying higher-need patients who are the most appropriate candidates for NFF CCM is the issue of present bias, where a patient’s perception of their own health status may be at odds with clinical presentation. If patients have a different perception of health status, they might not value the potential of the NFF CCM program and thus miss out on health benefits. Identifying a comprehensive recruitment strategy utilizing patient medical record data or other secondary sources may be helpful in selecting the most appropriate population.
Specifically, patients with multiple comorbidities and with complex combinations of physical and mental health conditions might be better suited for NFF CCM programs. Patients in this study who were comfortable using technology (such as patient portals and the internet for education and identification of resources) may experience less need for self-care support and NFF CCM. Also, time from diagnosis of type 2 diabetes may impact patient level of engagement with NFF CCM and services may need to be tailored to recently diagnosed patients versus those diagnosed more than five years ago.
The findings of this qualitative study echo findings of other qualitative research studies related to diabetes care management. Other studies demonstrated the potential value for CCM in elderly populations10 and promise for engagement of older patients17 and telemedicine18 in particular for this population through the one-on-one relationship that can be built between patient and care coordinator.19 Notably, another study pointed to the importance of highly individualized CCM in order for it to be effective.26 Specifically, patients and their caregivers who had higher needs for support with CCM and higher perceived value of NFF CCM programs reported that these services were helpful with referrals to specialists such as the study on optometry and podiatry referrals.41 Patients in this study also discussed how communicating with a care coordinator by phone was helpful for questions regarding their medications and side effects42 as well as barriers to care such as transportation and appointment scheduling.43 Information access and sharing, along with the care coordinator–patient discussion it facilitates for information like lab results, was something that patients in this study found helpful as was reported other studies.44,45 Another perceived benefit of NFF CCM was relationship building; this in addition to the connection to other services such diabetes educators and dietitians for diet and exercise and local resource referrals for gyms and community centers and other services was also found in previous studies.43,46
Previous studies also identified barriers and facilitators to the provision of NFF CCM that were mirrored in this study’s findings. For example, community-level characteristics such as proximity to healthy food and recreation to promote diet and exercise were associated with patient chronic condition self-management and engagement in CCM for people living with type 2 diabetes.6 Organizational structures such as Accountable Care Organizations (ACO), found in one study, were associated with enhanced organizational capacity to implement and conduct NFF CCM programs and services such as information sharing and patient referral, which was a result that patients discussed in one of the larger and more connected partner health systems which a part of an ACO.47
Limitations
Recruitment of patient interview participants and selection of a diverse sample of patients from across different partner health systems was a challenge in the implementation of this study. Another limitation was the small number of patients and caregivers who had direct experience with the CMS reimbursed NFF CCM due to partner health systems either restructuring their programs or not currently using the CMS reimbursement codes, signifying fewer patients enrolled in the CMS code during the study period.
As NFF CCM programs become more individualized based on health system implementation, future studies should include the evaluation of program effectiveness based on program structure (centralized or decentralized, internal to the organization or contracted out to a third party) and rigor of the NFF CCM program to analyze the impact of program design and resources on patient and caregiver experiences.
Conclusion
An essential finding of this study is that there is no “one-size-fits-all” approach to the design, development, and implementation of NFF chronic care management services and programs. The varied backgrounds, experiences, and conditions and levels of need for patients interviewed in this study illustrate that NFF CCM programs will need to be flexible and tailored to individual need, as well as target-specific groups that may benefit more from participation in a program. The current findings provide a strong base to conduct a future, large quantitative study. Patient-level as well as health organization-level and community-level factors will impact the individual patient and family needs, and chronic care management programs will need to be responsive, agile, and adapt accordingly to best serve patients and meet their needs.
Acknowledgments
This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Program Award (NEN-1508-32257). All statements in this poster, including its findings and conclusions, are solely those of the authors and do not necessarily represent the views of PCORI, its Board of Governors or Methodology Committee. The LEAD Study would like to acknowledge the contributions of our partners. The success of this study depended on their ongoing support and expertise. These partners include Ochsner Health System and the Ochsner Patient Research Advisory Board; Tulane Medical Center; Louisiana State University (LSU); Research Action for Health Network (REACHnet, a PCORnet CDRN) and their multi-stakeholder Diabetes Advisory Groups; Pennington Biomedical Research Center; Blue Cross and Blue Shield of Louisiana; and our patient and community partners Patricia Dominick, Cathy Glover, and Peggy Malone. We are grateful to Heather Sandoval for her participation in data collection and analysis and to Jewel Harden-Barrios for her support throughout the study.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1.
2.
3.
4. Schurrer J, O’Malley A, Wilson C, McCall N, Jain N. Evaluation of the Diffusion and Impact of the Chronic Care Management Services: Final Report. Washington, DC: Mathematica Policy Research Institute; 2017.
5. Osman O, Sherifali D, Stolee P, Heckman G. Diabetes management in long-term care: an exploratory study of the current practices and processes to managing frail elderly persons with type 2 diabetes. Can J Diabetes. 2016;40(1):17–30. doi:10.1016/j.jcjd.2015.10.005
6. Myers CA, Slack T, Broyles ST, Heymsfield SB, Church TS, Martin CK. Diabetes prevalence is associated with different community factors in the diabetes belt versus the rest of the United States. Obesity (Silver Spring). 2017;25(2):452–459. doi:10.1002/oby.21959
7. Brett J, Staniszewska S, Mockford C, et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect. 2014;17(5):637–650. doi:10.1111/j.1369-7625.2012.00795.x
8.
9. Maurer M, Dardess P, Carman K, Fraizier K, Smeeding L. Guide to Patient and Family Engagement: Environmental Scan Report. Rockville, MD: Agency for Healthcare Research and Quality; 2012.
10. Iliffe S, McGrath T, Mitchell D. The impact of patient and public involvement in the work of the Dementias & Neurodegenerative Diseases Research Network (DeNDRoN): case studies. Health Expect. 2013;16(4):351–361. doi:10.1111/j.1369-7625.2011.00728.x
11. Chrvala CA, Sherr D, Lipman RD. Diabetes self-management education for adults with type 2 diabetes mellitus: a systematic review of the effect on glycemic control. PubMed - NCBI. Patient Educ Couns. 2016;99(6):926–943. doi:10.1016/j.pec.2016.07.004
12. Fisher L, Polonsky WH, Hessler D, Potter MB. A practical framework for encouraging and supporting positive behaviour change in diabetes. PubMed - NCBI. Diabet Med. 2017;34(12):1658–1666. doi:10.1111/dme.13513
13. Boarini R, Kolev A, McGregor A. Measuring Well-Being and Progress in Countries at Different Stages of Development: Towards a More Universal Conceptual Framework. Paris: Organisation for Economic Cooperation and Development (OECD); 2014.
14. Walters BH, Adams SA, Nieboer AP, Bal R. Disease management projects and the chronic care model in action: baseline qualitative research. BMC Health Serv Res. 2012;12:114. doi:10.1186/1472-6963-12-114
15. Ernecoff NC, Witteman HO, Chon K, et al. Key stakeholders’ perceptions of the acceptability and usefulness of a tablet-based tool to improve communication and shared decision making in ICUs. J Crit Care. 2016;33:19–25. doi:10.1016/j.jcrc.2016.02.002
16. Ciechanowski P, Katon WJ. The interpersonal experience of health care through the eyes of patients with diabetes. Soc Sci Med. 2006;63(12):3067–3079. doi:10.1016/j.socscimed.2006.08.002
17. Wong EL, Woo J, Hui E, Chan C, Chan WL, Cheung AW. Primary care for diabetes mellitus: perspective from older patients. Patient Prefer Adherence. 2011;5:491–498. doi:10.2147/PPA.S18687
18. Trief PM, Sandberg J, Izquierdo R, et al. Diabetes management assisted by telemedicine: patient perspectives. Telemed J E Health. 2008;14(7):647–655. doi:10.1089/tmj.2008.0037
19. Bayliss EA, Edwards AE, Steiner JF, Main DS. Processes of care desired by elderly patients with multimorbidities. Fam Pract. 2008;25(4):287–293. doi:10.1093/fampra/cmn040
20. Ancker JS, Witteman HO, Hafeez B, Provencher T, Van de Graaf M, Wei E. The invisible work of personal health information management among people with multiple chronic conditions: qualitative interview study among patients and providers. J Med Internet Res. 2015;17(6):e137. doi:10.2196/jmir.4381
21. Gammon D, Berntsen GK, Koricho AT, Sygna K, Ruland C. The chronic care model and technological research and innovation: a scoping review at the crossroads. J Med Internet Res. 2015;17(2):e25. doi:10.2196/jmir.3547
22. Davy C, Bleasel J, Liu H, Tchan M, Ponniah S, Brown A. Factors influencing the implementation of chronic care models: a systematic literature review. BMC Fam Pract. 2015;16:102. doi:10.1186/s12875-015-0319-5
23. Small N, Bower P, Chew-Graham CA, Whalley D, Protheroe J. Patient empowerment in long-term conditions: development and preliminary testing of a new measure. BMC Health Serv Res. 2013;13:263. doi:10.1186/1472-6963-13-438
24. Bond GE, Rechholtz L, Bosa C, Impert C, Barker S. Program evaluation of sea mar’s chronic care program for latino and caucasian patients with type 2 diabetes: providers and staff perspectives. J Multidiscip Healthc. 2012;5:241–248. doi:10.2147/JMDH.S35489
25. Del Valle KL, McDonnell ME. Chronic care management services for complex diabetes management: a practical overview. Curr Diab Rep. 2018;18(12):135. doi:10.1007/s11892-018-1107-0
26. Timpel P, Lang C, Wens J, et al. Individualising chronic care management by analysing patients’ needs - a mixed method approach. Int J Integr Care. 2017;17(6):2. doi:10.5334/ijic.3067
27. Garg SK, Lyles CR, Ackerman S, et al. Qualitative analysis of programmatic initiatives to text patients with mobile devices in resource-limited health systems. BMC Med Inform Decis Mak. 2016;16:16. doi:10.1186/s12911-016-0258-7
28. Lie SS, Karlsen B, Oord ER, Graue M, Oftedal B. Dropout from an ehealth intervention for adults with type 2 diabetes: a qualitative study. J Med Internet Res. 2017;19(5):e187. doi:10.2196/jmir.7479
29. Kadu MK, Stolee P. Facilitators and barriers of implementing the chronic care model in primary care: a systematic review. BMC Fam Pract. 2015;16:12. doi:10.1186/s12875-014-0219-0
30. O’Malley AS, Tynan A, Cohen GR, Kemper N, Davis MM. Coordination of care by primary care practices: strategies, lessons and implications. Res Brief. 2009;(12):1–16.
31. Jones JA, Reeve CA. Factors influencing the use of clinical guidelines by general practitioners working in a setting of complex multimorbidity: a case study by interviews. BMC Fam Pract. 2018;19(1):157. doi:10.1186/s12875-018-0787-5
32. Drouin H, Walker J, McNeil H, Elliott J, Stolee P. Measured outcomes of chronic care programs for older adults: a systematic review. BMC Geriatr. 2015;15:139. doi:10.1186/s12877-015-0136-7
33. Stellefson M, Dipnarine K, Stopka C. The chronic care model and diabetes management in US primary care settings: a systematic review. Prev Chronic Dis. 2013;10:E26. doi:10.5888/pcd10.130016
34. Thompson CA. CMS expands Medicare’s chronic care management services. Am J Health Syst Pharm. 2018;75(4):165–166. doi:10.2146/news180011
35. Robeznieks A. ‘The right direction’. Primary-care docs see promise in CMS’ proposed pay for non face-to-face work. Mod Healthc. 2013;43(28):6–7, 1.
36. Yeager VA, Wharton MK, Monnette A, et al. non-face-to-face chronic care management: a qualitative study assessing the implementation of a new CMS reimbursement strategy. Popul Health Manag. 2018. doi:10.1089/pop.2017.0196
37. Bazzano AN, Wharton MK, Monnette A, et al. Barriers and facilitators in implementing non-face-to-face chronic care management in an elderly population with diabetes: a qualitative study of physician and health system perspectives. J Clin Med. 2018;7:11. doi:10.3390/jcm7110451
38. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm018
39. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
40. Seawright J, Gerring J. Case selection techniques in case study research:a menu of qualitative and quantitative options. Polit Res Q. 2008;61(2):294–308. doi:10.1177/1065912907313077
41. Glasson NM, Larkins SL, Crossland LJ. What do patients with diabetes and providers think of an innovative Australian model of remote diabetic retinopathy screening? A qualitative study. BMC Health Serv Res. 2017;17(1):158. doi:10.1186/s12913-017-2045-2
42. Hipwell AE, Sturt J, Lindenmeyer A, et al. Attitudes, access and anguish: a qualitative interview study of staff and patients’ experiences of diabetic retinopathy screening. BMJ Open. 2014;4(12):e005498. doi:10.1136/bmjopen-2014-005498
43. Lewis MA, Williams PA, Fitzgerald TM, et al. Improving the implementation of diabetes self-management: findings from the Alliance to Reduce Disparities in Diabetes. Health Promot Pract. 2014;15(2 Suppl):83S–91S.
44. Valerio MA, Kanjirath PP, Klausner CP, Peters MC. A qualitative examination of patient awareness and understanding of type 2 diabetes and oral health care needs. Diabetes Res Clin Pract. 2011;93(2):159–165. doi:10.1016/j.diabres.2011.03.034
45. Vimalananda VG, Dvorin K, Fincke BG, Tardiff N, Bokhour BG. Patient, primary care provider, and specialist perspectives on specialty care coordination in an integrated health care system. J Ambul Care Manage. 2018;41(1):15–24. doi:10.1097/JAC.0000000000000219
46. Vachon B, Huynh AT, Breton M, et al. Patients’ expectations and solutions for improving primary diabetes care. Int J Health Care Qual Assur. 2017;30(6):554–567. doi:10.1108/IJHCQA-07-2016-0106
47. Shortell SM, Poon BY, Ramsay PP, et al. A multilevel analysis of patient engagement and patient-reported outcomes in primary care practices of accountable care organizations. J Gen Intern Med. 2017;32(6):640–647. doi:10.1007/s11606-016-3934-5
Supplementary material
 | Box S1 Case study |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.