")
Back to Journals » OncoTargets and Therapy » Volume 13
Olaparib and Pembrolizumab Treatment for BRCA1-Mutated and PD-L1-Positive Intrahepatic Cholangiocarcinoma Recurrence and Metastasis: A Case Report
Authors Xiong F, Gong J, Wang Q
Received 19 February 2020
Accepted for publication 7 June 2020
Published 1 July 2020 Volume 2020:13 Pages 6385—6391
DOI https://doi.org/10.2147/OTT.S250454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Fan Xiong, Jing Gong, Qi Wang
Department of Integrative Traditional Chinese and Western Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, People’s Republic of China
Correspondence: Qi Wang
Department of Integrative Traditional Chinese and Western Medicine Tongji Hospital, Tongji Medical College,Huazhong University of Science and Technology, Wuhan 430030, People’s Republic of China
Email [email protected]
Abstract: Olaparib has been applied as monotherapy to treat ovarian and breast cancer patients with malignant or suspected malignant BRCA1/2 mutations. Pembrolizumab has been approved to treat unresectable or metastatic tumors in patients who exhibited progression after previous treatment, regardless of histology. However, there are no reports on the use of olaparib and pembrolizumab for the treatment of BRCA1/2-mutated and PD-L1-positive intrahepatic cholangiocarcinoma (iCCA). This case report aimed to observe the safety and efficacy of olaparib and pembrolizumab in treating BRCA1-mutated and PD-L1-positive iCCA recurrence and metastasis. This case report describes a patient with BRCA1-mutated and PD-L1-positive iCCA recurrence and metastases who received olaparib and pembrolizumab. Olaparib (400 mg orally twice daily) and pembrolizumab (100 mg iv every 3 weeks) were administered to the patient for 9 months. The patient achieved complete response (CR) confirmed by liver magnetic resonance imaging (MRI)+ perfusion-weighted imaging (PWI)+ diffusion-weighted imaging (DWI), and the carcinoembryonic antigen (CEA), alpha fetoprotein (AFP), carbohydrate antigen 125 (CA-125), and carbohydrate antigen 199 (CA19-9) tumor marker levels were normal after treatment. There were no significant adverse events, and routine blood counts, coagulation function, and liver and kidney function were normal. The Eastern Cooperative Oncology Group (ECOG) performance status decreased from a score of 1 to a score of 0. Olaparib and pembrolizumab can effectively treat BRCA1-mutated and PD-L1-positive iCCA patients, and adverse effects were largely unobserved. More studies should be performed to promote the development of tumor genomics because the findings from these studies may help clinicians select suitable biomarkers to treat iCCA patients. As the use of immunotherapy alone to treat tumors may not achieve the expected effect, targeted therapy combined with immunotherapy has become a new approach in cancer treatment strategies.
Keywords: intrahepatic cholangiocarcinoma, olaparib, pembrolizumab, BRCA1/2 mutations, PD-L1 positive
Introduction
CCAs are a heterogeneous group of cancers originated from the bile duct epithelium.1 CCAs comprise an estimated 3% of all gastrointestinal system cancers and are divided into 3 groups according to the anatomical site: intrahepatic cholangiocarcinoma (iCCA), perihilar cholangiocarcinoma (pCCA) and distal cholangiocarcinoma (dCCA).2,3 ICCA is the second most common liver cancer, and its incidence is rising worldwide widely reported,4 but this trend might not be entirely true because there were some misclassifications in the past that might interfere with prevalence and incidence.5 Epidemiological studies show that although there are multiple risk factors for CCA, including biliary diseases, biliary malformations, cholelithiasis, cholecystitis, liver flukes, cirrhosis, and alcoholic liver disease, the main risk factor for iCCA is chronic viral hepatitis.6 Because of the lack of effective methods to screen and the hysteresis of clinical manifestations, the diagnosis of early-stage iCCA is difficult, and most patients miss the opportunity to undergo surgery. The majority of patients with painless jaundice, itchy skin and emaciation are already in advanced-stage iCCA, so the therapeutic effect is not satisfactory, and the prognosis is poor. Traditional therapies have reached a bottleneck in advanced iCCA, and no targeted drugs and immunotherapy agents for iCCA have been approved at present. Therefore, we describe a case in which olaparib and pembrolizumab were used to treat a patient with BRCA1-mutated and PD-L1-positive iCCA recurrence and metastases at our hospital. This study was approved by the Clinical Trial Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Case Report
A 43-year-old male patient was found to have liver-occupying lesions by color Doppler ultrasound, with no symptoms of abdominal pain, diarrhea, nausea or vomiting at the time of physical examination on August 27, 2015. The patient had a history of chronic viral hepatitis B and had been taking lamivudine for a long time. Upper abdominal computed tomography (CT) suggested that the lesion in the anterior upper segment of the right lobe of the liver was considered a tumor and that cancer should not be excluded. Later, the patient came to our hospital for treatment on September 1, 2015. The tumor biomarkers CEA, AFP, CA-125, and CA19-9 were normal, and routine blood counts, coagulation function, and liver and kidney function were also normal. Then, the patient underwent segment V hepatectomy + segment IV partial hepatectomy + cholecystectomy under general anesthesia in the department of hepatobiliary surgery of our hospital on September 8, 2015. The postoperative pathological examination suggested that the liver lesion was moderately/poorly differentiated CCA. Immunohistochemical (IHC) staining showed EMA (+), CK19 (+), hepatocyte (-), arginase (-), CD34 (-), and a Ki-67 index of 30%. After surgery, the patient underwent adoptive immunotherapy for 3 years.
The liver magnetic resonance imaging (MRI)+ perfusion-weighted imaging (PWI)+ diffusion-weighted imaging (DWI) re-examination on September 28, 2018 showed that the hepatic portal and retroperitoneal lymph nodes were enlarged, and tumor metastasis was considered (Figure 1). A positron emission tomography-computed tomography scan (PET-CT) performed on October 11, 2018, suggested that multiple lymph nodes of the hepatic portal and retroperitoneum were enlarged and had high metabolism (SUVmax: 12.3); these findings indicated metastatic lesions. On October 13, 2018, the CA19-9 level was 41.92 U/mL (normal value: <34 U/mL), and the CEA, AFP and CA-125 levels were normal. The patient was hospitalized again in the department of hepatobiliary surgery of our hospital on October 12, 2018, and bile duct lesion resection + portal lymph node dissection (palliative) + choledochojejunostomy were performed under general anesthesia on October 19, 2018. Postoperative pathology suggested moderately/poorly differentiated adenocarcinoma (CCA) (Figure 2) that invaded the nerves, with 1/1 lymph node metastasis in 13 groups. On November 16 and December 4, 2018, the CEA, AFP, CA-125 and CA19-9 levels were normal. On December 19, 2018, chest enhanced CT showed that the bronchial wall of the posterior segment of the upper lobe of the right lung was slightly thickened, and the lumen was inhomogeneous. Liver MRI+PWI+DWI examinations were performed on December 20, 2018; the liver and gallbladder showed postoperative changes, a hemangioma was observed in the lower segment of the right posterior lobe of the liver, multiple cysts were observed in the liver, and long T2-weighted signals, limited hepatic portal diffusion and heterogeneous enhancement was observed (0.7×0.6 cm), indicating metastatic lesions (Figure 3). The recurrence site was in the liver, additionally, increased and enlarged hepatic portal and retroperitoneal lymph nodes were seen. The patient did not receive radiotherapy, chemotherapy or other locoregional therapies.
 |
Figure 1 Preoperative radiological examination of the patient. Liver MRI (A) +PWI (B) +DWI (C) showed that the hepatic portal and retroperitoneal lymph nodes were enlarged. Abbreviations: MRI, magnetic resonance imaging; PWI, perfusion-weighted imaging; DWI, diffusion-weighted imaging. |
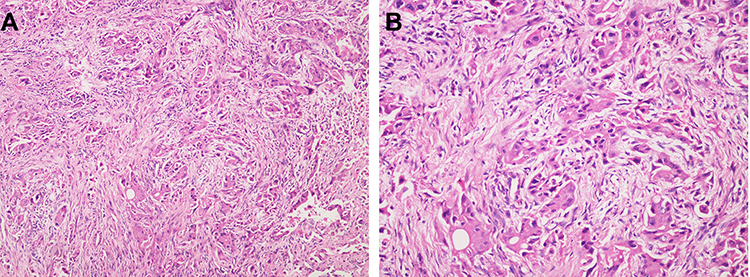 |
Figure 2 Postoperative pathological examination of the patient. (A) stain: hematoxylin and eosin (H&E), original magnification×100; (B) stain: H&E, original magnification×200. |
 |
Figure 3 Postoperative radiological examination of the patient. Liver MRI (A) +PWI (B) +PWI (C) showed long T2-weighted signals indicating limited hepatic portal diffusion and heterogeneous enhancement. Abbreviations: MRI, magnetic resonance imaging; PWI, perfusion-weighted imaging. |
Genomic profiling was performed on December 29, 2018. The genomic profiling results were as follows: gene variation: TP53 p. R273H, mutation frequency: 7.91%; and gene variation: BRCA1 p. K654fs, mutation frequency: 5.89%. NTRK2-RTP1 gene fusion was detected. The BRCA1 p. K654fs point mutation suggested that the patient might be sensitive to olaparib. The NTRK2-RTP1 gene fusion suggested that the patient might be sensitive to larotrectinib. Additionally, the PD-L1 expression level of patient tumor tissue was detected, and IHC staining results of tissue sections revealed a tumor proportion score (TPS) of 5% for PD-L1, indicating low expression (TPS < 1%: negative/no expression, TPS 1–49%: low expression, TPS ≥ 50%: high expression). On January 11, 2019, the CEA, AFP, CA-125 and CA19-9 levels were normal, and the routine blood counts, coagulation function, and liver and kidney function were normal. Then, the patient began to receive targeted therapy and immunotherapy on January 11, 2019. The measurements of the target lesions were evaluated by liver MR+DWI+PWI and chest enhanced CT, which were basically reexamined every 2 months.
Up to October 2019, the patient was treated with olaparib orally at a dose of 400 mg, bid, and with pembrolizumab 15 times. On October 9, 2019, the CEA, AFP, CA-125 and CA19-9 levels were normal, and the routine blood counts, coagulation function, and liver and kidney function were normal. The Eastern Cooperative Oncology Group (ECOG) score declined from 1 to 0. The repeat chest enhanced CT on October 9, 2019 showed chronic inflammatory changes in the posterior segment of the right upper lobe; micronodules in the lower lobe of the left lung; stripe foci in the lower lobe of the left lung; increased and enlarged bilateral axillary, mediastinal and right diaphragmatic angle lymph nodes; and right pleural hypertrophy and adhesions. The liver MRI+DWI+PWI re-examinations on October 15, 2019 showed postoperative changes in the liver and gallbladder; a hemangioma at the lower end of the right posterior lobe of the liver; and multiple small cysts in the liver. The long T2-weighted signals in the hepatic portal disappeared, and hepatic portal and retroperitoneal lymph node enlargement was not observed (Figure 4). At that point, olaparib was combined with pembrolizumab to treat this iCCA patient, and the CR duration was up to 9 months.
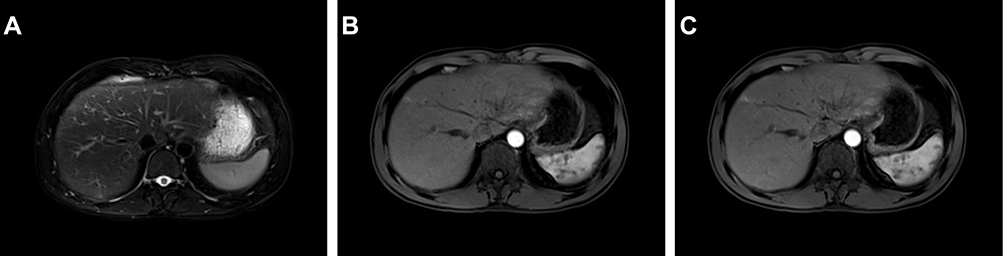 |
Figure 4 Radiological examination after combination therapy in the patient. Liver MRI (A) +PWI (B) +PWI (C) showed that the long T2-weighted signals in the hepatic portal disappeared, and hepatic portal and retroperitoneal lymph node enlargement were not observed. Abbreviations: MRI, magnetic resonance imaging; PWI, perfusion-weighted imaging. |
Discussion
Currently, surgery is still the main curative approach for iCCA patients, and surgical resection has been revealed to improve the short-term survival outcomes of these patients, but the long-term prognosis after surgery still remains unsatisfactory.7 It has been reported that the overall survival (OS) rate at 5 years after curative-intent resection remains only 20–30%.4 Even after R0 resection, some studies have reported disease recurrence rates of 60% after 21 months of follow-up and rates as high as 80% after 5 years of follow-up.8,9 If no other treatments was considered, the survival for unresectable advanced CCA is a median of 3.9 months;10 therefore, a large number of unresectable advanced CCA patients are willing to undergo all kinds of chemotherapy and radiotherapy. At present, the first-line treatment for unresectable advanced and metastatic CCA patients is the combination of gemcitabine and cisplatin chemotherapy.11,12 In addition, although some studies have suggested certain therapeutic effects of various forms of radiation and locoregional therapies to improve prognosis, more studies are needed before these treatments can be added to the current CCA guidelines.
With a greater understanding of tumor pathophysiology, molecular biology and genomics, the diagnosis and therapy of tumors have gradually entered a more precise, targeted therapy phase. FGFR1-3 fusions, BRAF substitutions, IDH1/2 mutations, BAP1 mutations, MET amplifications and a low KRAS mutation expression are more common in iCCA,13 whereas extrahepatic CCAs and distal CCAs feature ERBB2 amplifications, ARID1B, ELF3 and PRKACA/B mutations;14 the results of these studies have also revealed different types of mutations in tumors with different etiologies and anatomical locations. Because of the limited benefit of conventional treatments in advanced iCCA, an increasing number of patients wish to receive molecular targeted treatments. Recently, the emergence of molecular targeted treatments, including VEGF receptor inhibitors, EGFR inhibitors, FGFR2 inhibitors, IDH inhibitors, HGF/MET signaling pathway inhibitors, and JAK/STAT cytokine pathway inhibitors,15 have offered new ideas for further investigations into iCCA. However, the results of clinical trials on targeted treatments such as anti-EGFR drugs have been discouraging.16,17 The lack of iCCA-specific data from clinical trials is due to the relatively low incidence and high heterogeneity of iCCA.15 Therefore, investigations into the molecular pathology of iCCA are warranted, as the results of these studies may help us better select suitable targets to further enhance the therapeutic effect.
The “Basket Trial” was a clinical trial designed according to the principles of cancer genomics and essentially explores the use of the same drug to treat different types of tumors that possess similar genomic characteristics. At this point, genetic background and molecular profiling studies have been added to cancer treatment strategies, which are no longer limited by the pathologic type of tumors.18 BRCA1 is a tumor suppressor gene that can encode a nucleic acid protein that keeps the genome stable and plays an important role in transcription, double-stranded DNA repair and DNA recombination. BRCA1/2 mutations are commonly associated with ovarian and breast cancer, and abnormalities in the function of this protein can also increase the risk for pancreatic and prostate cancer. Olaparib is a PARP inhibitor that has been applied as monotherapy to treat terminal ovarian cancer patients with malignant or suspected malignant BRCA1/2 mutations who received 3 or more front-line chemotherapy agents in the past. A total of 298 patients with BRCA1/2 mutations were enrolled in a multicenter Phase II study including advanced breast cancer patients with metastasis; ovarian cancer patients resistant to platinum therapy; pancreatic cancer patients after gemcitabine treatment; and prostate cancer patients with progression after systemic treatment.19 The results of the clinical trial revealed the following: the overall response rate was 26.2%, and the response rate was 12.9% in the breast cancer patients, 31.1% in the ovarian cancer patients, 21.7% in the pancreatic cancer patients, and 50.0% in the prostate cancer patients, respectively.19 The different types of cancer with BRCA1/2 mutations and the response to olaparib were observed through this clinical trial. Although tumors with BRCA1/2 mutations have been detected in CCA patients14,20 and BRCA1/2-mutated tumors are often sensitive to PARP inhibitors, these drugs have not yet been prospectively evaluated in CCA patients.
Immunotherapy is a type of treatment that exerts its effects by activating specific T lymphocytes and enhancing the anti-tumor immune response to target attack and eliminate tumor cells. PD-1 is a co-inhibitory cell surface receptor that induces immunosuppression and enables tumor cells to escape the response of cytotoxic T cells during carcinogenesis;21 therefore, the ability to block the binding between PD-1 and its ligand PD-L1 to reduce tumor immune escape effectively is a promising approach.22 It has been reported that the expression of PD-L1 in CCA specimens ranged from 9–72%.23 In addition, high expression of PD-L1 was found to be associated with poor survival.24 These findings indicate that PD-1/PD-L1 inhibitors could be used as adjuvant therapy for CCA. PD-1/PD-L1 antibodies including nivolumab, pembrolizumab, atezolizumab, durvalumab and avelumab have been approved worldwide. Pembrolizumab is a high-affinity, highly selective, humanized IgG4a that is mainly used to treat non-small cell lung cancer, gastric cancer, Hodgkin’s lymphoma and other malignant tumors in clinical settings. The KEYNOTE-028 (NCT02054806) trial investigated the results of treatment with pembrolizumab monotherapy for 24 biliary tract cancer patients, and proved that pembrolizumab was effective and safe. This clinical trial also found that the overall response rate (ORR) was 17% and that the median progression-free survival (PFS) was 1.9 months.15 Pembrolizumab has been approved for the treatment with unresectable or metastatic tumors, independent of histology.3 However, the follow-up of PD-1/PD-L1 expression after tumor treatment found that long-term persistent anti-PD-1 or anti-PD-L1 therapy did not achieve the desired survival rate.25 The main reason may be because tumor immunotherapy covers multiple signaling pathways that have complex interactions. The use of a PD-1 antibody or PD-L1 antibody alone to treat tumors may not achieve the expected effect, so combined therapy has become the new approach for tumor therapy.
Conclusion
In this report, our patient was diagnosed with resectable iCCA, and then adoptive immunotherapy was administered to the patient for 3 years after surgery. However, disease recurrence was detected, and new lesions were found in the liver, so surgical resection was performed again. Lesion recurrence again occurred, and intrahepatic metastases were observed after surgery. After genomic profiling, BRCA1 mutations and low PD-L1 expression were found, and combination therapy with olaparib and pembrolizumab was subsequently administered. Multiple lesions in the liver and hilar and retroperitoneal lymph nodes disappeared gradually after 9 months of this combination treatment. This report is the first to describe a case of iCCA treated with olaparib and pembrolizumab. The safety and efficacy of this combination treatment have also been demonstrated. In addition, the results of this report suggest that the same treatment can be used for different types of tumors with the same gene mutation. Moreover, this report again confirmed that treating tumors with a PD-1/PD-L1 antibody alone may not achieve the expected effect and that combined therapy, which has become the new trend for tumor therapy, should be considered. Traditional therapies have reached a bottleneck for advanced iCCA, but attempts to treat new targets and use of immunotherapy have provided a glimmer of hope. However, most of the clinical research is still in the early stage. Whether the treatment of these new targets and the use of immunotherapy can truly offer clinical benefit requires further exploration with a large sample size in future prospective studies.
Informed Consent
Written informed consent was provided by the patient for publication of the report.
Acknowledgments
The authors thank the National Natural Science Foundation of China (No. 81904022) and Hubei Provincial Science and Technology Project (No. ZY2019M040) for their support.
Disclosure
The authors declare that they have no conflicts of interest related to this report.
References
1. Bragazzi MC, Ridola L, Safarikia S, et al. New insights into cholangiocarcinoma: multiple stems and related cell lineages of origin. Ann Gastroenterol. 2018;31:42–55. doi:10.20524/aog.2017.0209
2. Messina C, Merz V, Frisinghelli M, et al. Adjuvant chemotherapy in resected bile duct cancer: a systematic review and meta-analysis of randomized trials. Crit Rev Oncol Hematol. 2019;143:124–129. doi:10.1016/j.critrevonc.2019.09.002
3. Rizvi S, Khan SA, Hallemeier CL, et al. Cholangiocarcinoma — evolving concepts and therapeutic strategies. Nat Rev Clin Oncol. 2018;15(2):95–111. doi:10.1038/nrclinonc.2017.157
4. Razumilava N, Gores GJ. Cholangiocarcinoma. Lancet. 2014;383(9935):2168–2179. doi:10.1016/S0140-6736(13)61903-0
5. Khan SA, Tavolari S, Brandi G. Cholangiocarcinoma: epidemiology and risk factors. Liver Int. 2019;39(suppl1):19–31. doi:10.1111/liv.14095
6. Krasinskas AM
7. Choi SB, Kim KS, Choi JY, et al. The prognosis and survival outcome of intrahepatic cholangiocarcinoma following surgical resection: association of lymph node metastasis and lymph node dissection with survival. Ann Surg Oncol. 2009;16:3048–3056. doi:10.1245/s10434-009-0631-1
8. Hyder O, Hatzaras I, Sotiropoulos GC, et al. Recurrence after operative management of intrahepatic cholangiocarcinoma. Surgery. 2013;153(6):811–818. doi:10.1016/j.surg.2012.12.005
9. Tabrizian P, Jibara G, Hechtman JF, et al. Outcomes following resection of intrahepatic cholangiocarcinoma. HPB (Oxford). 2015;17(4):344–351. doi:10.1111/hpb.12359
10. Park J, Kim MH, Kim KP, et al. Natural history and prognostic factors of advanced cholangiocarcinoma without surgery, chemotherapy, or radiotherapy: a large-scale observational study. Gut Liver. 2009;3(4):298–305. doi:10.5009/gnl.2009.3.4.298
11. Valle JW, Furuse J, Jitlal M, et al. Cisplatin and gemcitabine for advanced biliary tract cancer: a metaanalysis of two randomised trials. Ann Oncol. 2014;25(2):391–398. doi:10.1093/annonc/mdt540
12. Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N Engl J Med. 2010;362(14):1273–1281. doi:10.1056/NEJMoa0908721
13. Simbolo M, Fassan M, Ruzzenente A, et al. Multigene mutational profiling of cholangiocarcinomas identifies actionable molecular subgroups. Oncotarget. 2014;5:2839–2852. doi:10.18632/oncotarget.1943
14. Nakamura H, Arai Y, Totoki Y, et al. Genomic spectra of biliary tract cancer. Nat Genet. 2015;47(9):1003–1010. doi:10.1038/ng.3375
15. Rahnemai-Azar AA, Weisbrod AB, Dillhoff M, et al. Intrahepatic cholangiocarcinoma: current management and emerging therapies. Expert Rev Gastroenterol Hepatol. 2017;11(5):439–449. doi:10.1080/17474124.2017.1309290
16. Ole Larsen F, Taksony Solyom Hoegdall D, Hoegdall E, et al. Gemcitabine, capecitabine and oxaliplatin with or without cetuximab in advanced biliary tract carcinoma. Acta Oncol. 2016;55(3):382–385. doi:10.3109/0284186X.2015.1080858
17. Leone F, Marino D, Cereda S, et al. Panitumumab in combination with gemcitabine and oxaliplatin does not prolong survival in wildtype KRAS advanced biliary tract cancer: a randomized Phase 2 trial (Vecti-BIL study). Cancer. 2016;122(4):574–581. doi:10.1002/cncr.29778
18. Cheng Y, Zhang J, Qin SK, et al. Treatment with olaparib monotherapy for BRCA2-mutated refractory intrahepatic cholangiocarcinoma: a case report. Onco Targets Ther. 2018;18(11):5957–5962. doi:10.2147/OTT.S176914
19. Kaufman B, Shapira-Frommer R, Schmutzler RK, et al. Olaparib monotherapy in patients with advanced cancer and a germline BRCA1/2 mutation. J Clin Oncol. 2015;33(3):244–250. doi:10.1200/JCO.2014.56.2728
20. Churi CR, Shroff R, Wang Y, et al. Mutation profiling in cholangiocarcinoma: prognostic and therapeutic implications. PLoS One. 2014;9(12):e115383. doi:10.1371/journal.pone.0115383
21. Dai S, Jia R, Zhang X, et al. The PD-1/PD-Ls pathway and autoimmune diseases. Cell Immunol. 2014;290:72–79. doi:10.1016/j.cellimm.2014.05.006
22. Chen W, Li G, Hu Z, et al. Significant response to anti-PD-1 based immunotherapy plus lenvatinib for recurrent intrahepatic cholangiocarcinoma with bone metastasis. Medicine. 2019;98:
23. Gani F, Nagarajan N, Kim Y, et al. Program death 1 immune checkpoint and tumor microenvironment: implications for patients with intrahepatic cholangiocarcinoma. Ann Surg Oncol. 2016;23:2610–2617. doi:10.1245/s10434-016-5101-y
24. Ye Y, Zhou L, Xie X, et al. Interaction of B7-H1 on intrahepatic cholangiocarcinoma cells with PD-1 on tumor-infiltrating T cells as a mechanism of immune evasion. J Surg Oncol. 2009;100(6):500–504. doi:10.1002/jso.21376
25. Homet Moreno B, Mok S, Comin-Anduix B, et al. Combined treatment with dabrafenib and trametinib with immunestimulating antibodies for BRAF mutant melanoma. Oncoimmunology. 2016;5:e1052212. doi:10.1080/2162402X.2015.1052212
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.