")
Back to Journals » Journal of Blood Medicine » Volume 6
Occurrence of anti-D alloantibodies among pregnant women in Kasese District, Western Uganda
Authors Mbalibulha Y, Muwanguzi E , Mugyenyi G, Natukunda B
Received 15 January 2015
Accepted for publication 17 February 2015
Published 17 April 2015 Volume 2015:6 Pages 125—129
DOI https://doi.org/10.2147/JBM.S80977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin Bluth
Video abstract presented by Yona Mbalibulha.
Views: 3474
Yona Mbalibulha,1 Enoch Muwanguzi,1 Godfrey R Mugyenyi,2 Bernard Natukunda1
1Department of Medical Laboratory Sciences, 2Department of Obstetrics and Gynecology, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda
Objectives: This study was undertaken to determine the distribution of ABO/RhD (rhesus D antigen) blood phenotypes, prevalence of anti-D alloantibodies, and the risk factors for alloimmunization among pregnant women in Kasese District, Western Uganda.
Materials and methods: Ethylenediamine tetraacetic acid-containing plasma samples and serum samples were taken from pregnant women attending the antenatal clinic. The blood groups were identified using the microplate grouping method, while the presence of anti-D alloantibodies was detected by the indirect antiglobulin test (IAT). Data were also collected from the pregnant women on the risk factors associated with anti-D alloantibody formation.
Results: Among the 726 participants, the blood group distribution was as follows: O: 356 (49.%); A: 190 (26.%); B: 152 (21%); and AB: 28 (4%). A total of 28 (3.86%) pregnant women were RhD negative. Anti-D alloantibodies were detected in 88 (12.1%) of the participants; and of these, 13 (14.8%) were RhD negative. Statistically significant risk factors for anti-D alloimmunization included miscarriage, stillbirth, and postpartum hemorrhage.
Conclusion: Blood group O was the most common among the pregnant women in this study and the prevalence of Rh negativity was 3.8%. The frequency of anti-D alloimmunization among pregnant women in Kasese District was 12.12%, with 85.5% of these being RhD positive. Risk factors such as a history of stillbirths, miscarriages, and incidence of postpartum hemorrhage were significantly associated with anti-D alloimmunization. There is a need to routinely carry out antenatal blood grouping and IAT screening on pregnant women in Uganda to detect anti-D alloimmunization. Given the high prevalence of anti-D alloantibody formation among RhD-positive women, we recommend additional research studies on the role of autoimmunity among antigen-positive women, as well as the occurrence of RhD variants plus their implications on hemolytic disease of the fetus and newborn, in Uganda.
Keywords: ABO/RhD blood groups, anti-D alloimmunization, indirect antiglobulin test, pregnant women, Western Uganda
Introduction
There are approximately 400 red blood cell antigens in 33 blood group systems.1 Of these, >50 different antigens are capable of causing maternal alloimmunization and fetal hemolytic disease. Rhesus D antigen (RhD) alloimmunization has been a focus of concern for obstetricians and hematologists for centuries because of the occurrence of Rh hemolytic disease. The prevalence of RhD negative group varies in different ethnic populations, with approximately 15.8% of Caucasians, 8% of Blacks, and 1% of Asians being RhD negative.2 Exposure to the D antigen is vital in obstetrics because if the maternal anti-D is immunoglobulin G (IgG), it is capable of crossing the placenta and causing complications such as hemolytic disease of the fetus and the newborn (HDFN). HDFN can present in three forms based on the red cell antigens to which maternal immunization has occurred; these include the following: 1) HDFN due to ABO antigens, 2) HDFN due to Rh, either due to anti-D alone or due to anti-D accompanied by other Rh antibodies such as anti-C, anti-c, anti-E, or anti-e, and 3) HDFN caused by “Other” factors – unexpected immune antibodies other than anti-D, which may be Jk, K, Fy, and S. The HDFN toward or due to Rh is the most common and severe.3
Although most people are either D+ or D−, there is a plethora of D variants, often categorized as either weak D or partial D. DVI is the D variant most commonly associated with anti-D production. Weak D types 1, 2, and 3 are rarely associated with alloanti-D production, so a policy recommendation would be to treat patients with those D variants as D+, patients with all other D variants would be treated as D−.4 These variants can lead to alloimmunization in RhD-positive pregnant women and the proportion of these variants is not established in Uganda.
Routine antenatal RhD and alloanti-D screening among women is a tool used in identifying significant maternal risk factors putting the neonate at risk of HDFN. This should then be followed by the administration of anti-D prophylaxis dose antepartum at the 28th week of gestation and a postpartum injection of anti-D within 72 hours of delivering an RhD-positive infant.5,6 However, in Uganda, there is no routine screening for maternal alloimmunization. Hence, we carried out this study to assess the level of alloimmunization within pregnant women in western Uganda.
Materials and methods
Study participants
A total of 726 pregnant women attending the antenatal clinic at the Kagando Hospital, Bwera Hospital, and Nyabirongo Health Centre IV in Kasese District, Western Uganda, were recruited into the study. Participants consented and the study was approved by the research and ethics committee of Mbarara University and by the Uganda National Council of Science and Technology.
Sample collection and analysis
Whole blood (4 mL) was drawn by venipuncture of the antecubital vein into plain and ethylenediaminetetraacetic acid-containing vacutainer tubes. Samples were analyzed for ABO and RhD blood groups using the microplate method after dilution of red blood cells to a 5% suspension with 0.9% (w/v) saline and adding the grouping antisera appropriately. These were then vortexed, and the presence or absence of agglutination was checked for. The indirect antiglobulin test (IAT) was performed, which involved the incubation of standard cells with the test serum at 37°C for 30 minutes and then reacting with anti-human globulin to bring about agglutination of the red cells in positive samples.
Statistical analysis
The information was recorded using data collection forms. Data were then entered using the statistical software package EXCEL 5.0 (Microsoft, Redmond, WA, USA) and transferred to STATA 12 (StataCorp, College Station, TX, USA) for analysis. Descriptive statistics (mean, median, interquartile range, and standard deviation) were used and the proportions calculated for categorical variables. Categorical data were analyzed using bivariate and multivariate comparisons. The P-value was set at ≤0.05 to be considered statistically significant.
Results
Demographic characteristics of the participants
The participants had an age range of 15–42 (median: 24, IQR: 20, 30) years and there were 160 (22%) prime gravid women. Complications reported in the present pregnancy included malaria, bleeding, and HIV. A total of 170 women (23.4%) had a previous obstetric history of abortion (14%), cesarian section (2.75%), stillbirths (5.65%), and postpartum hemorrhage (PPH) (0.96%). Nine women (1.24%) had a history of blood transfusion.
Blood group distribution and maternal alloimmunization
Most of the participants had blood group O (356; 49.04%), with women of other blood groups as follows: A: 190 (26%), B: 152 (21%), and AB: 28 (3.86%). A total of 28 (3.86%) participants were RhD negative. There were 88 (12.1%) IAT-positive participants, and of these, 13 (14.8%) were of RhD-negative status and 75 (85.2%) were RhD positive.
Risk factors for anti-D alloimmunization
There was an association of obstetric history, parity, and gravidity with alloimmunization. Thus, 43% had a parity of two to four children, while 37.5% had a parity of more than four children; the remaining participants were prime gravid women. A bivariate analysis of risk factors closely associated with RhD alloimmunization showed that obstetric history, age, and parity/gravidity had P-values of 0.001, 0.025, and 0.114, respectively, thus being significantly associated with alloimmunization. In all the pregnant women, a positive association was common with obstetric history (P-value: 0.0001) and transfusion history (P-value: 0.2966). There was no association with factors such as HIV and cesarian section generally. Factors such as abortion/miscarriage, stillbirth, and PPH in obstetric history had a close association. Age category (>30 years) showed a significant association with anti-D alloimmunization (P-value: 0.004) (Tables 1 and 2).
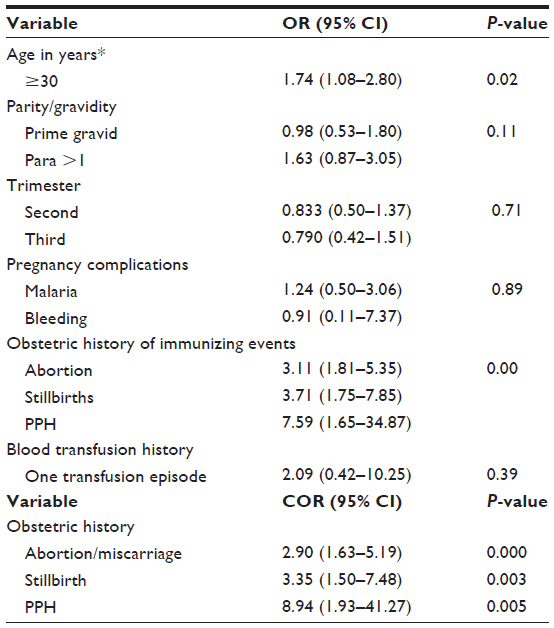 | Table 1 Risk factors for maternal anti-D alloimmunization |
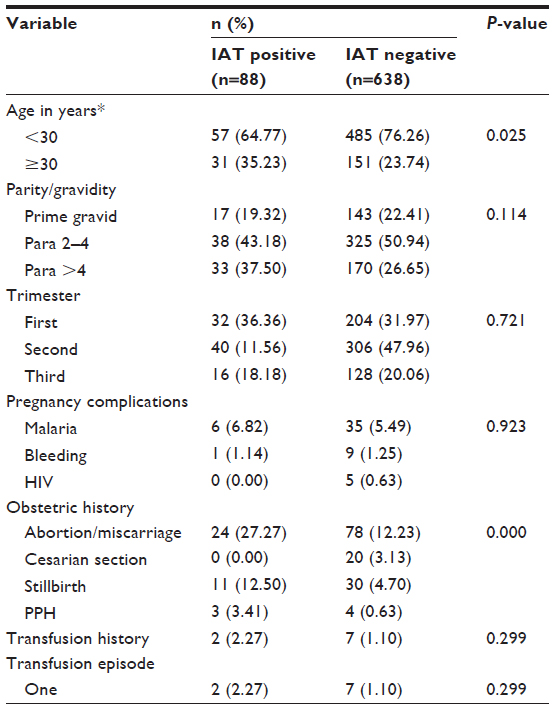 | Table 2 Risk factors of alloimmunization in sensitized and nonsensitized pregnant women (N=726) |
Discussion
RhD alloimmunization has been a focus of concern for obstetricians and hematologists for centuries in their quest to try and eliminate HDFN as a common obstetric problem. The alloanti-D antibodies arise following sensitizing factors such as pregnancy when a RhD-negative woman conceives a RhD-positive fetus, transfusion of RhD-positive blood to RhD-negative woman, and obstetric sensitizing factors such as abortion, ectopic pregnancy, and hemorrhagic episodes in RhD-positive women, and this phenomenon has remained a problem leading to HDFN.7 In this study, the focus was on both RhD-positive and RhD-negative pregnant women; we wanted to determine the ABO blood group distribution, test for the presence of alloantibodies, and establish the associated risks.
Our study established a distribution of the ABO blood group, with group O (49%) having the highest percentage, followed by A (26%), B (20.9%), and AB (3.9%). This is similar to the result of the study carried out in Kampala, Uganda, where the blood group distribution was 48.9%, 26.4%, 21.0%, and 3.8% for the blood groups O, A, B, and AB, respectively,8 but differing greatly from the distribution among the Loe population of the Lao Republic, with distributions as follows: O 37.7%, B 35.6%, A 19.9%, and AB 6.0%. This is because of the ethnic variation.
In this study, Rh group distribution was 3.86%; which is similar to a study that was carried out in southwestern Uganda and which showed 3.6%.9 But the Rh distribution is lower than the 7.1% found in Black blood donor populations in the USA and 7.5% found in Saudi Arabia.10 We observed a lower prevalence of RhD-negative status (4.0%) among the pregnant women studied herein compared to that among Caucasians (≥14%). Our findings are consistent with several previous studies among Africans and Asians, reporting RhD prevalence of ≤7.2%.11
A total of 88 (12.12%) participants tested positive, indicating the presence of the antibodies. This indicated a higher prevalence of these antibodies in relation to the results of a similar study8 conducted in Kampala, wherein a prevalence of 5.5% was obtained. Among the 88 participants who were IAT positive, 75 (85.2%) were RhD-positive pregnant women, indicating the development of alloantibodies within the RhD-positive women, which could mainly be due to RhD variants within the population or, to some extent, due to autoimmunity triggered by anti-RhD antibody coating the erythrocytes, and this need to be verified further.
It is possible that not all the women in the study could recall being transfused in early childhood, which may explain the presence of alloantibodies in the prime gravid women and the absence of previous transfusion as a risk factor for maternal alloimmunization. However, the alloimmunization frequency in our teenage pregnant women was comparable to the frequency, albeit greater, in older women. It is possible to speculate that persistence of an antibody formed after an unrecognized transfusion during childhood explains antibody prevalence in the young women, while high parity is responsible for antibody prevalence in the older women. This trend was also observed in other Ugandan studies.8,9
Age was significantly associated with the rate of alloimmunization (P=0.0007) in RhD-negative pregnant women. Because parity rises with age, the rate of alloimmunization might rise with maternal age; this is because the association was found in those aged ≥30 years because these women are continuously exposed to risk factors during every pregnancy. The alloimmunization in the young women could be explained by other sensitizing factors, such as childhood blood transfusion, which could not be remembered. This is comparable to a study in southwestern Uganda, where several sensitizing factors such as parity, age, and other obstetric factors were found to be associated with alloimmunization.9
In the RhD-positive pregnant women, a strong association was obtained with the obstetric history (P=0.0001). It is therefore indicative that risk factors such as miscarriage, stillbirth, and PPH (P=0.001, 0.002, and 0.012, respectively) play a key role in RhD alloimmunization in RhD-positive pregnant women as in the RhD-negative women. Other factors such as transfusion history and having blood group O had a mild association, but this was not strong enough to be strongly linked. This could be that few pregnant women report having been transfused or could not remember.
Conclusion
Blood group O-positive is the most prevalent blood group among pregnant women attending antenatal clinics in Kasese District and the prevalence of Rh negativity was 3.8%. The prevalence of Rh alloimmunization in pregnant women was found at 12.12%, with 85% of these women being RhD positive, which is higher than that reported in similar studies in Kampala. Risk factors such as stillbirth, miscarriage/abortion, and PPH had a close association with alloimmunization.
The implications of our findings are limited given the deidentified nature of the specimens tested and lack of follow-up data on the newborns of these women. Consequently, this study only showed the presence of demonstrable alloantibody, but it would be necessary to establish the frequency and specificities of demonstrable clinically significant antibodies that may cause HDFN or require compatible blood for transfusion among pregnant women and their neonates in Kasese. It demonstrates the feasibility of establishing the blood group type and screen testing for RhD alloantibody in a health care setting.
Acknowledgments
The authors wish to thank the study participants. We are grateful to the Medical Education Partnership Initiative–Medical Education Services for All Ugandans (MEPI–MESAU) consortium.
Funding
This work was supported by grant number 5R24TW008886, supported by Office of the US Global Aids Coordinator, National Institutes of Health, and Health Resources and Services Administration. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the supporting offices.
Author contributions
YM participated in study conception and design, data acquisition, analysis and interpretation, manuscript drafting and revising. EM participated in data collection, analysis and interpretation, manuscript drafting and revising. GM participated in study design, data analysis and interpretation, manuscript drafting and revising. BN participated in study conception, design, data analysis and interpretation, manuscript drafting and revising.
Disclosure
The authors report no conflicts of interest in this work.
References
John G. Wintrobe’s Clinical Haematology. Vol 1. 11th ed. Netherlands: Wolters Kluwer; 2008:804–805. | |
Avent ND, Reid ME. The Rhesus blood group system. J Am Soc Haematol. 2000;95(2):375–387. | |
Catrina FR. Hemolytic disease of of the new born. REX Lab Bulletin. 2007;126:1–4 | |
Daniels G. Variants of RhD current testing and clinical consequences. Br J Haematol. 2013;161(4):461–470. | |
Gajjar K, Spencer C. Diagnosis and management of non anti-D red cell antibodies in pregnancy. Obstetr Gynaecol. 2009;11:89–95. | |
Kumar S, Regan F. Management of pregnancies with RhD alloimmunisation. Br Med J. 2005;330:1255–1258. | |
Marek L. Prevention of alloimmunisation in RhD negative women. Biomed Pap MeFac Univ Palacky Olomouc Czech Repub. 2010;1(154):3–8. | |
Eipl K. Seroprevalence of unexpected red cell antibodies among pregnant women in Uganda. Immunohematology. 2012;4(28):115–117. | |
Natukunda B, Mugenyi G, Brand A, Schonewille H. Maternal red blood cells alloimmunisation in south western Uganda. Transfus Med. 2011;21(4):262–266. | |
Bondagji NS. Rhesus alloimmunization in pregnancy. A tertiary care center experience in the Western region of Saudi Arabia. Saudi Med J. 2012;33(6):688. | |
Erhabor O, TC A. Rh alloimmunization in Sub Saharan Africa. Int J Womens Health. 2010;2:429–437. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.