")
Back to Journals » Patient Preference and Adherence » Volume 10
Obstructive sleep apnea affects the clinical outcomes of patients undergoing percutaneous coronary intervention
Authors Zhang J , Gao X, Ge Z, Jiang X , Xiao P, Tian N, Kan J , Lee C, Chen S
Received 12 January 2016
Accepted for publication 22 March 2016
Published 20 May 2016 Volume 2016:10 Pages 871—878
DOI https://doi.org/10.2147/PPA.S104100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Jun-jie Zhang,1,2,* Xiao-fei Gao,1,* Zhen Ge,1,2 Xiao-Min Jiang,1 Ping-xi Xiao,1,2 Nai-liang Tian,1,2 Jing Kan,2 Chi-Hang Lee,3 Shao-Liang Chen1,2
1Department of Cardiology, Nanjing First Hospital, Nanjing Medical University, 2Department of Cardiology, Nanjing Heart Center, Nanjing, People’s Republic of China; 3Department of Cardiology, National University Heart Center, Singapore
*These authors contributed equally to this work
Background: There is a paucity of evidence regarding the association between obstructive sleep apnea (OSA) and patients undergoing percutaneous coronary intervention (PCI) for coronary artery disease. We sought to investigate whether OSA affects the clinical outcomes of patients undergoing PCI.
Patients and methods: All enrolled individuals treated with PCI were evaluated for OSA by polysomnography. The primary end point was defined as major adverse cardiac events (MACEs) at 2 years, including cardiac death, myocardial infarction (MI), and/or target vessel revascularization.
Results: A total of 340 consecutive patients undergoing PCI were assigned to the OSA (n=152, apnea–hypopnea index ≥15) and non-OSA (n=188, apnea–hypopnea index <15) groups. The incidence of OSA in patients with coronary artery disease undergoing PCI was 44.7%. Patients in the OSA group had more three-vessel disease (34.9%), increased number of total implanted stents (3.3±2.0), and longer total stent length (83.8±53.1 mm) when compared to the non-OSA group (23.4%, P=0.020; 2.8±1.9, P=0.007; 68.7±48.4, P=0.010). After a median follow-up of 2 years, the incidence of MACEs was significantly higher in patients with OSA (25.0% vs 16.0%, P=0.038), mainly driven by the increased periprocedural MI (19.2% vs 11.2%, P=0.038) in the OSA group. By Cox regression multivariable analysis, the independent predictor of MACEs was OSA (hazard ratio: 1.962, 95% confidence interval: 1.036–3.717, P=0.039).
Conclusion: There was a high prevalence of moderate-to-severe OSA in patients undergoing PCI, and OSA was associated with significantly increased MACE rate, mainly due to the increase in periprocedural MI rate.
Keywords: coronary artery disease, percutaneous coronary intervention, myocardial infarction, obstructive sleep apnea
Corrigendum for this paper has been published
Introduction
Obstructive sleep apnea (OSA), which presents in ~9% of females and 24% of males, is characterized by repetitive upper airway obstruction in breathing during sleep and is usually associated with hypertension, arrhythmia, heart failure, insulin resistance, and cerebrovascular accident.1,2 It has also been shown that the prevalence of OSA in patients with coronary artery disease (CAD) was two times more than that in those without CAD, with increased risk of mortality and myocardial infarction (MI), which was believed to be caused by hypoxia, enhanced inflammation, oxidative stress, and endothelial dysfunction.1,3,4 So far, percutaneous coronary intervention (PCI) has been the crucial treatment for symptomatic CAD; however, there is a paucity of evidence regarding the association between OSA and patients undergoing PCI. In 89 consecutive patients with acute coronary syndrome (ACS) treated with PCI, the incidence of cardiac death, reinfarction, and target vessel revascularization (TVR) at 8-month follow-up was 23.5% in the OSA group, which was significantly higher than 5.3% in patients without OSA.5 However, the advanced devices, especially the new generation of drug-eluting stent (DES), were not used in the small-scale study with short follow-up. Therefore, this prospective study is designed to address the long-term clinical impact of OSA in patients undergoing PCI.
Patients and methods
Study population
From October 2012 to April 2014, a total of 1,130 consecutive real-world patients who were treated with DES implantation at our center were considered as candidates for this study. Finally, 340 patients were included in the study according to the inclusion and exclusion criteria. Inclusion criteria were as follows: age >18 years and successful PCI in at least one major epicardial coronary artery. Exclusion criteria are shown in Figure 1. Of note, patients with OSA receiving any relevant treatments were excluded. The protocol was approved by the Institutional Ethics Committee of Nanjing First Hospital, and written informed consent was obtained from all patients.
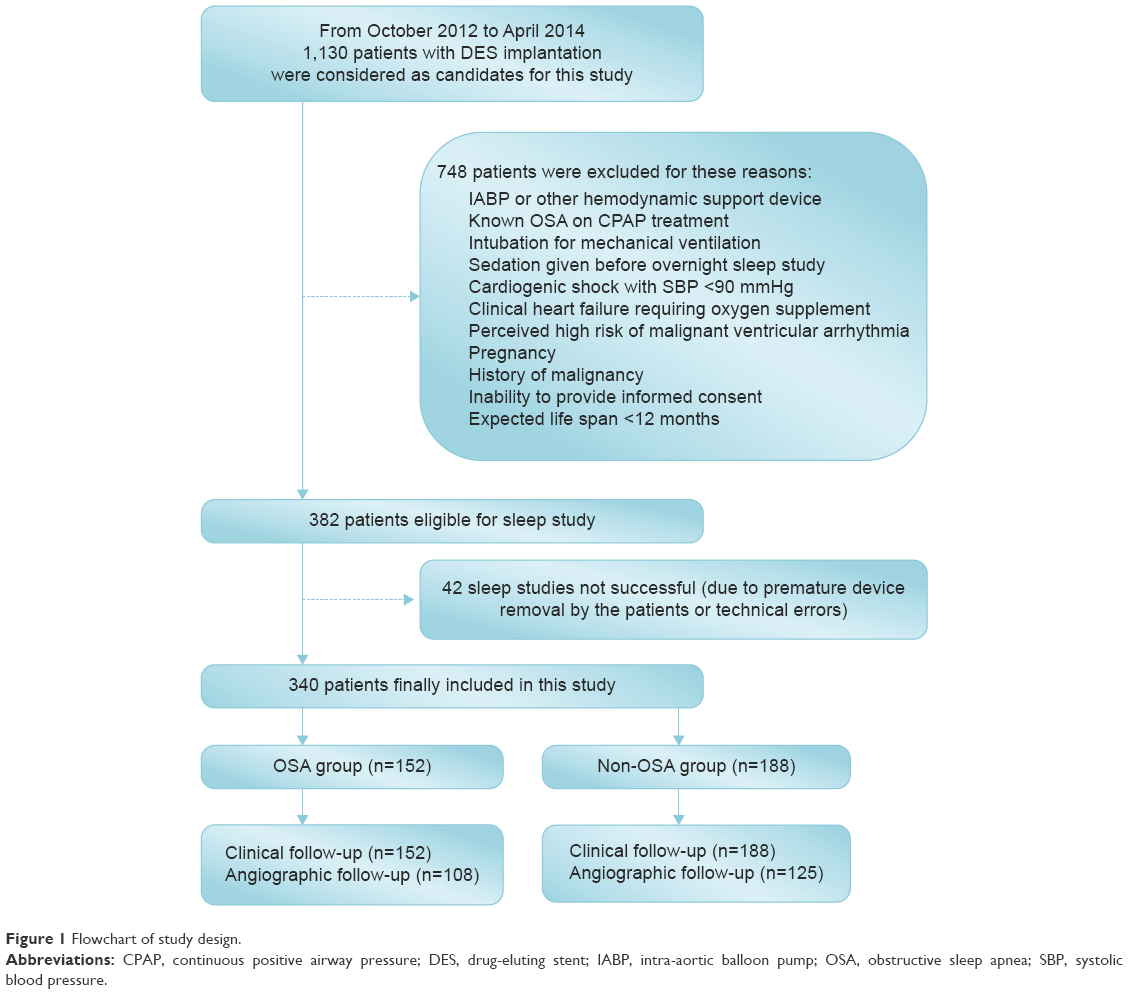 | Figure 1 Flowchart of study design. |
Percutaneous coronary intervention
All interventional procedures were performed in accordance with the current guidelines. Use of the type of DES, glycoprotein IIb/IIIa inhibitors, intravascular ultrasound, fractional flow reserve, and optical coherence tomography was at the operator’s discretion. A loading dose of clopidogrel (300 mg) or ticagrelor (180 mg) was administered before the index procedure. Total creatine kinase, creatine kinase-myocardial band, and troponin were dynamically measured until 72 hours postprocedure. After the intervention, all patients received 100 mg/d aspirin indefinitely and clopidogrel (75 mg/d) or ticagrelor (90 mg/d bid) for at least 12 months.
Sleep study
All overnight sleep studies for eligible patients were conducted using the Embletta Gold standardized level-3 portable diagnostic system (Natus Medical Inc., Ontario, Canada) 7–10 days after the index PCI procedure,6,7 which included nasal airflow, thoracoabdominal movements, arterial oxygen saturation, snoring episodes, limb movement, electrocardiogram, and body position. All sleep studies were reviewed by an independent sleep specialist according to the guidelines,8 and the poor quality of sleep tracings were excluded from the final analysis of the sleep data. Two independent sleep technologists with registered polysomnographic technologist credentials manually analyzed all studies. The respiratory events of sleep study were performed in accordance with the American Association of Sleep Medicine Guidelines.8 The primary measurement of the sleep study was the apnea–hypopnea index (AHI), which “was used to stratify patients” into the OSA (AHI ≥15) and non-OSA groups (AHI <15).9
Study end points and definitions
The primary end point was the rate of major adverse cardiac events (MACEs) at 2 years, including cardiac death, MI, and/or TVR. The safety end point was the occurrence of stent thrombosis (ST). All deaths were considered cardiac in origin unless a noncardiac cause was confirmed clinically or at autopsy. MI was diagnosed in accordance with the Society for Cardiovascular Angiography and Interventions definition.10 Target lesion revascularization, TVR, and ST were defined according to the Academic Research Consortium definition.11
Follow-up
Clinical follow-up was performed either by telephone or through a clinical office visit at 1 month, 6 months, and 12 months, and every year thereafter. Repeat coronary angiography was scheduled at 12 months after the indexed procedure unless clinical reasons indicated earlier. An independent committee that was blinded to the study assessed all clinical events.
Quantitative coronary angiography
Quantitative coronary angiographic analysis (QCA) at baseline, post-stenting, and at follow-up was performed offline using edge detection techniques (CAAS II, Version 5.0; Pie Medical, Maastricht, the Netherlands) by an independent core laboratory (China Cardiovascular Research Foundation, Beijing, People’s Republic of China). QCA variables included reference vessel diameter, minimal lumen diameter, acute gain, late lumen loss, and net gain, which were defined in our previous study.12
Statistical analysis
The distribution of continuous variables was assessed by the Kolmogorov–Smirnov test. Categorical variables were expressed as frequencies or percentages and compared using chi-square statistics or Fisher’s exact test. Continuous variables were summarized as mean ± SD or median and compared using Student’s t-test (for normal data) and Mann–Whitney U-test (for non-normally distributed variables). Survival curves were generated by the Kaplan–Meier method and compared using the log-rank test. Hazard ratios (HR) are presented along their 95% confidence interval (CI). Univariable and multivariable Cox proportional hazard models were applied to identify potential factors that correlated with MACEs. The variables showing statistical significance or a trend (P<0.1) in univariable Cox model were subjected to multivariable analysis with a forced-entry method. A P-value <0.05 was considered statistically significant, except for P-value <0.01 in univariable analysis to minimize the probability of type I error. All analyses were performed using the statistical program SPSS 16.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline clinical and sleep characteristics
A total of 340 patients (average age: 64.69±10.38 years) with DES implantation were finally enrolled and assigned to the OSA (n=152, 44.7%) and non-OSA (n=188, 55.3%) groups stratified by the AHI. Baseline clinical and sleep characteristics are shown in Table 1. None of the 340 study patients had received treatments for OSA. Ten percent of the individuals were admitted with stable angina and the remaining with ACS. Patients in the OSA group were more likely to be males (78.9%) and had greater body mass index (BMI; 25.4±2.9 kg/mm2) and larger left ventricular end diastolic diameter (LVDd; 50.6±6.8 mm), when compared to the non-OSA group (68.6%, P=0.032; 24.5±3.1 kg/mm2, P=0.007; 48.2±4.6 mm, P=0.003). The median AHI of 340 enrolled patients was 13.8, and the median time for SpO2 level <90% was 16.3 minutes in the OSA group, which was significantly higher than the >5.1 minutes in the non-OSA group (P<0.001).
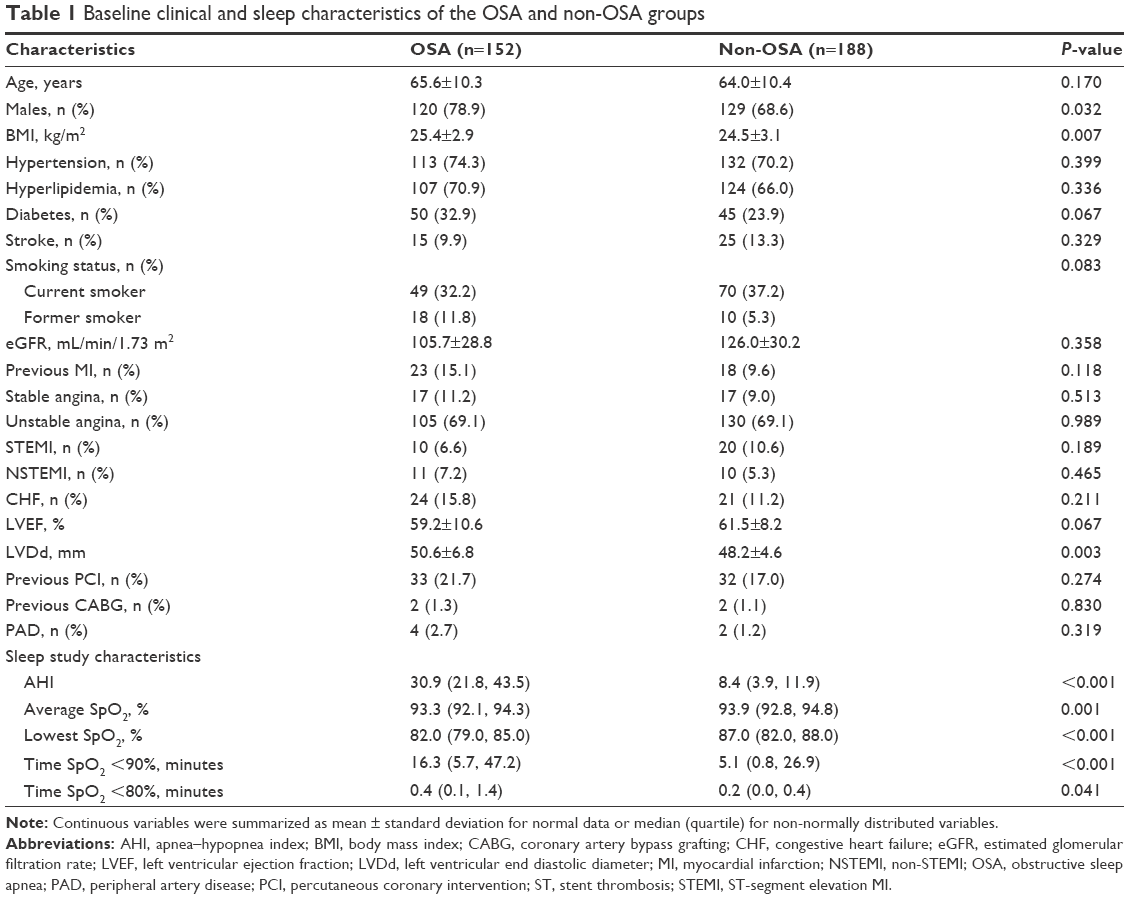 | Table 1 Baseline clinical and sleep characteristics of the OSA and non-OSA groups |
Lesions and procedural characteristics
Table 2 shows that patients in the OSA group had more three-vessel disease (34.9%), increased number of total implanted stents (3.3±2.0), and larger total stent length (83.8±53.1 mm) when compared to the non-OSA group (23.4%, P=0.020; 2.8±1.9, P=0.007; 68.7±48.4, P=0.010). As a result, the OSA group had higher procedural time (64.0±49.7 minutes vs 52.8±39.6 minutes, P=0.026).
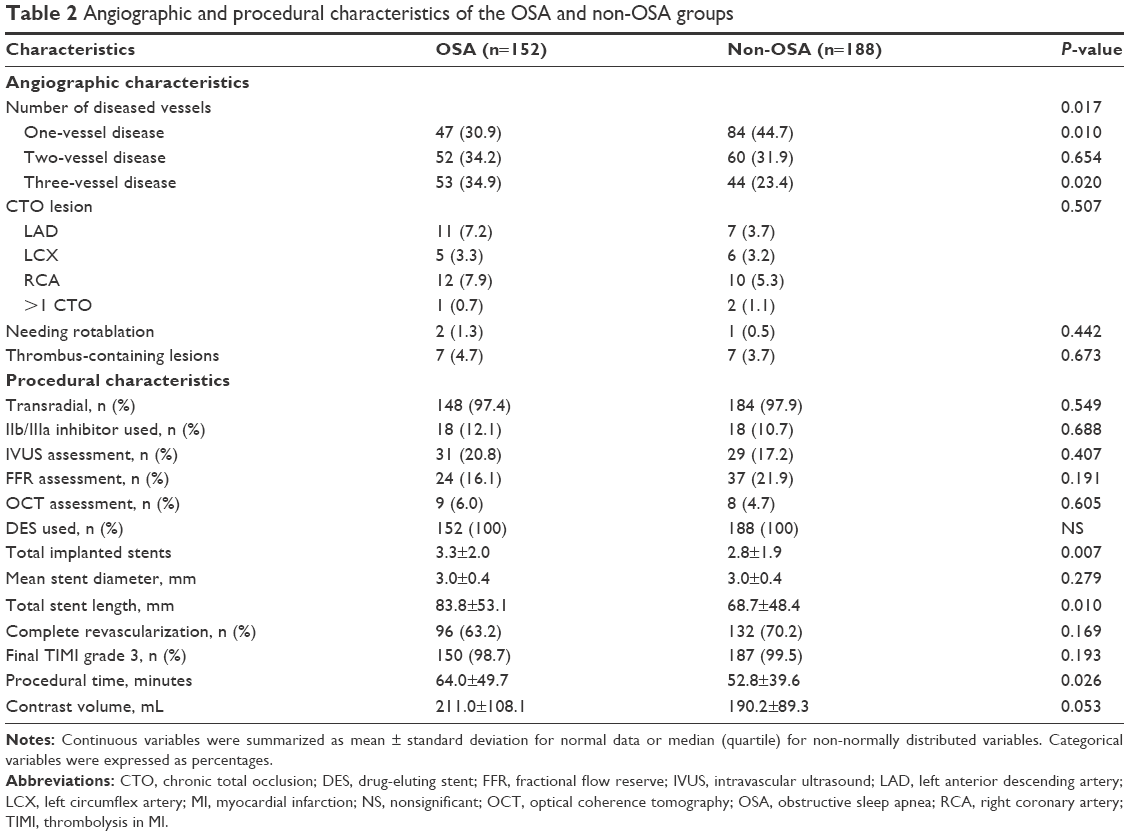 | Table 2 Angiographic and procedural characteristics of the OSA and non-OSA groups |
OSA and cardiovascular events
After a median follow-up of 2 years, there were 38 (25.0%) composite MACEs in the OSA group and 30 (16.0%) in the non-OSA group (P=0.038), which were mainly driven by the more periprocedural MI (19.2%) in the OSA group compared to the non-OSA group (11.2%, P=0.038; Table 3, Figure 2). By Cox regression multivariable analysis, the independent predictor of MACEs was OSA (HR: 1.962, 95% CI: 1.036–3.717, P=0.039; Table 4). There were no significant differences in QCA between the OSA and non-OSA groups (Table 5).
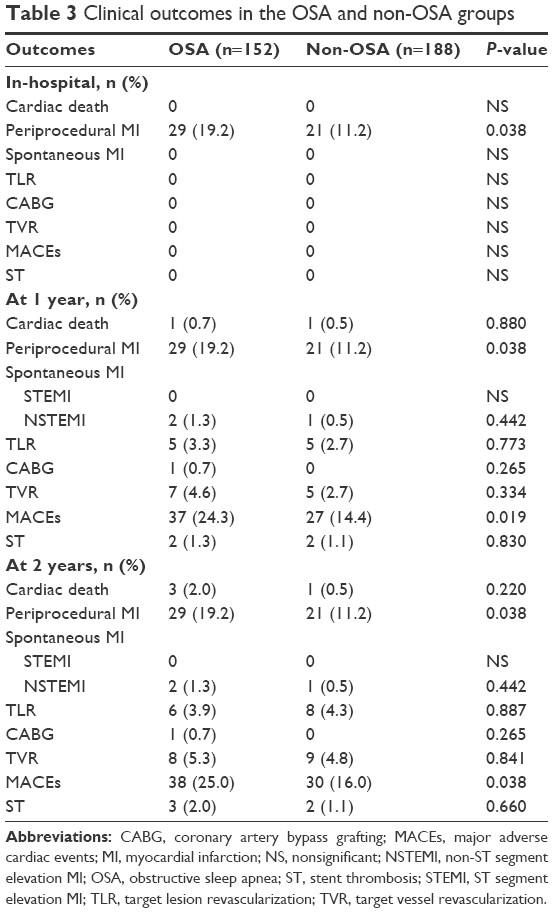 | Table 3 Clinical outcomes in the OSA and non-OSA groups |
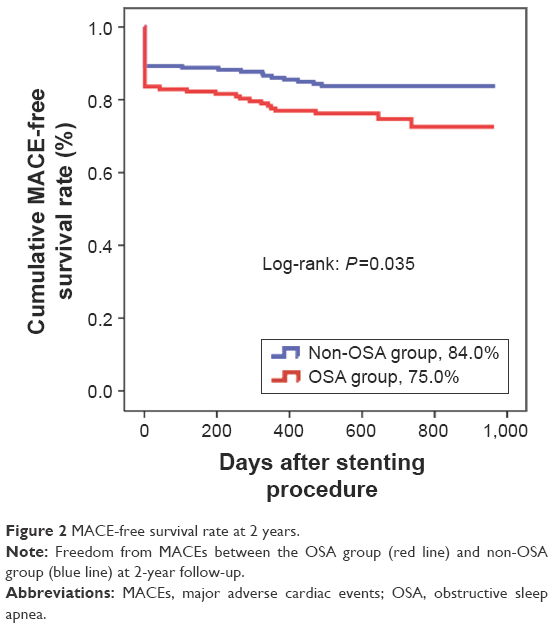 | Figure 2 MACE-free survival rate at 2 years. |
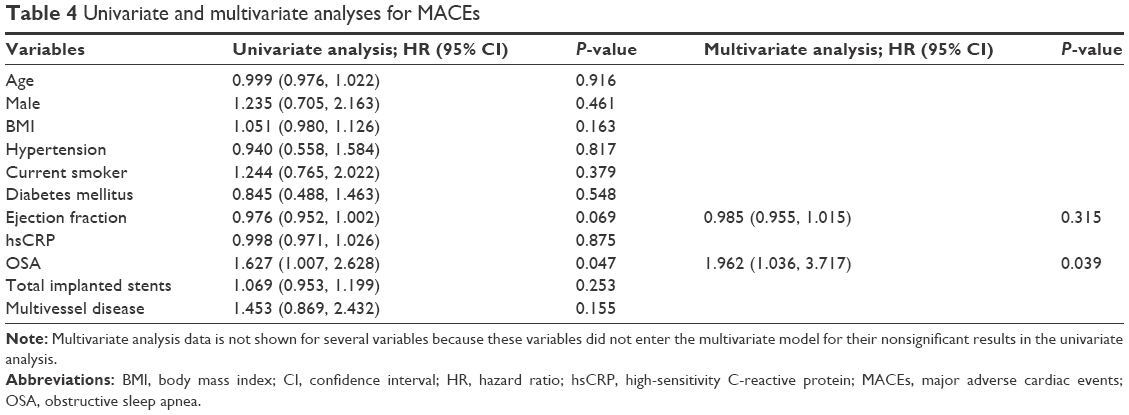 | Table 4 Univariate and multivariate analyses for MACEs |
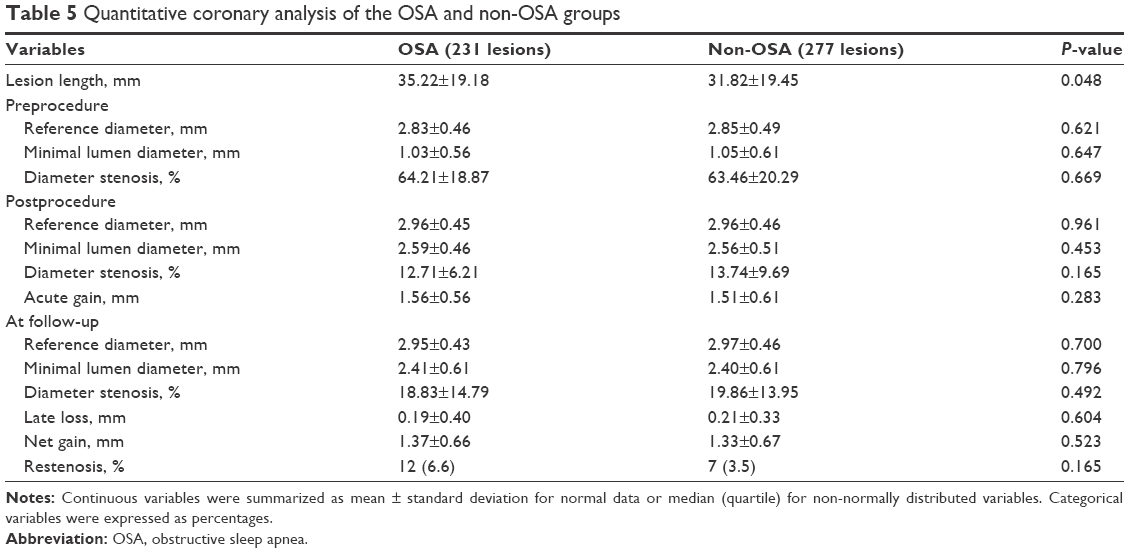 | Table 5 Quantitative coronary analysis of the OSA and non-OSA groups |
Subgroup analysis
Figure 3 shows the results of subgroup analysis for the associations between OSA and risk of MACEs in patients with DES implantation at 2 years. The incidence of composite MACEs in the OSA group was more remarkable among male patients aged ≤75 years, with BMI >25 kg/m2, hyperlipidemia, and ACS.
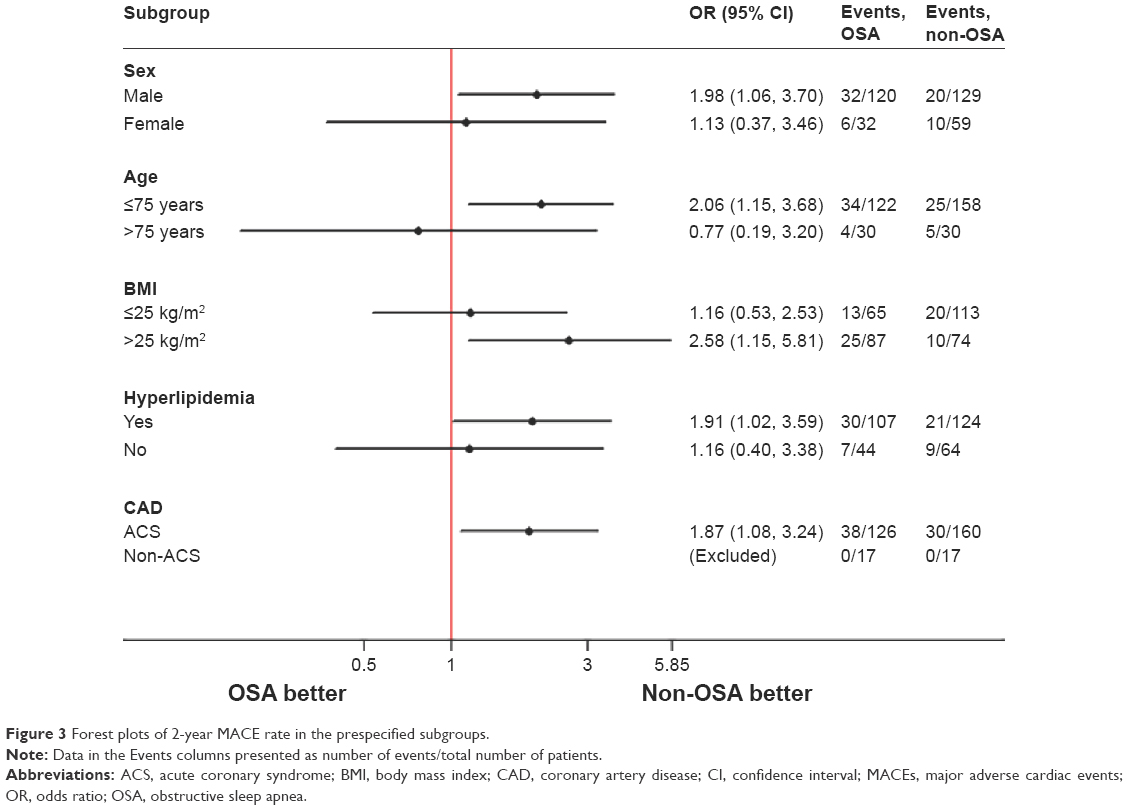 | Figure 3 Forest plots of 2-year MACE rate in the prespecified subgroups. |
Discussion
The major finding of the current study was that the high prevalence of moderate-to-severe OSA was found in patients with DES implantation, and OSA was associated with significantly increased 2-year composite MACE rate, mainly due to the increment of periprocedural MI rate.
In the current study, we found that 44.7% of patients with CAD undergoing PCI had moderate-to-severe OSA, which was similar to 48.3% and 57% in the current literature.5,13 With chronic intermittent hypoxemia, reoxygenation, and hypercapnia in patients with OSA, there is increased sympathetic activation, induction of oxidative stress, vasoconstriction, and provocation of inflammation leading to endothelial dysfunction and atherosclerosis.1,14,15 Therefore, it is not surprising that the high prevalence of OSA was found in these patients with CAD undergoing PCI. In addition, the current study showed that patients with OSA were more likely to be males and had a significantly greater BMI, which was consistent with published data in the Randomized Intervention With Continuous Positive Airway Pressure in Coronary Artery Disease and Sleep Apnea trial,16 suggesting that age, male, and BMI were predictors of OSA. Moreover, compared to patients without OSA, patients with OSA were more likely to undergo multivessel PCI and had an increased number of DESs implanted during PCI, which might be explained by chronic hypoxia, enhanced inflammation, oxidative stress, and endothelial dysfunction.1,3
The association between OSA and adverse cardiac events has been explored in general population in several studies.3,4,17 The Sleep Heart Health Study enrolling 1,927 men and 2,495 women free of CAD showed that OSA was a significant predictor of incident CAD, MI, revascularization procedure, or cardiovascular death after a median of 8.7-year follow-up.4 In another long-term study including 1,436 patients, OSA increased the risk of coronary events or cardiovascular death, and OSA was an independent risk factor for cardiovascular events, including MI.3 Similar negative effects of OSA could be found in patients with ACS.11,18,19 In 168 consecutive patients with unstable angina or non-ST elevation acute MI, OSA had higher risk of cardiovascular complications during the acute phase of ACS.11 Overall, the current data indicated that OSA has been associated with increased risk of adverse cardiac events in general population or patients with ACS.
Whether OSA adversely affected the prognosis of patients with stent placement for CAD has not been established, and there is a deficiency of evidence regarding the association between OSA and patients undergoing PCI. In 105 patients admitted with ST-segment elevation MI undergoing stent placement, severe OSA carried a negative prognostic impact for these patients after 18-month follow-up.20 Another study which enrolled 89 consecutive patients with ACS treated with PCI showed that the incidence of cardiac death, reinfarction, and TVR at 8-month follow-up was 23.5% in the OSA group, significantly higher than 5.3% in patients without OSA.5 However, the new generation of DES was not used in this small-scale study with short follow-up. Our data confirm this previous evidence and add some novel findings. First, to the best of our knowledge, this is the first study to demonstrate increased periprocedural MI rate of OSA after DES implantation in patients with CAD. Second, a great many angiographic and procedural variables, indicating anatomic severity for coronary disease and the potentially important confounding factors, were included and adjusted in this study. Third, subgroup analysis was conducted to identify a subset of patients undergoing PCI for whom an unfavorable effect of OSA was remarkable. Finally, the differences in techniques, lesion complexity, and DES types used may be impact factors attributed to the discrepancy in several results. However, results from a previous study5 and ours demonstrated a negative effect of OSA on composite MACE rate in patients undergoing PCI for CAD.
Study limitations
The current study has several limitations. First, none of the 340 study patients had received treatments for OSA, and it was not possible to evaluate the effects of continuous positive airway pressure treatment on cardiovascular outcome. Second, there were 42 sleep studies that were not successful due to premature device removal by the patients or technical errors, and it might not be possible to conduct a repeat sleep study in consideration of the short hospitalization period in patients after PCI. Third, patients were not tested for sleep data again in the follow-up. Thus, there was lack of information regarding post-discharge sleep data and the timing of cardiac events during the follow-up.
Conclusion
The current study showed a high prevalence of moderate-to-severe OSA in patients with DES implantation for CAD, and OSA was associated with significantly increased 2-year composite MACE rate, mainly due to the increment of periprocedural MI rate.
Acknowledgment
The study is supported by the Jiangsu Provincial Special Program of Medical Science (BL2013001).
Disclosure
The authors report no conflicts of interest in this work.
References
Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. J Am Coll Cardiol. 2008;52(8):686–717. | ||
Perk J, De Backer G, Gohlke H, et al; European Association for Cardiovascular Prevention & Rehabilitation (EACPR); ESC Committee for Practice Guidelines (CPG). European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J. 2012;33(13):1635–1701. | ||
Shah NA, Yaggi HK, Concato J, Mohsenin V. Obstructive sleep apnea as a risk factor for coronary events or cardiovascular death. Sleep Breath. 2010;14(2):131–136. | ||
Gottlieb DJ, Yenokyan G, Newman AB, et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: the sleep heart health study. Circulation. 2010;122(4):352–360. | ||
Yumino D, Tsurumi Y, Takagi A, Suzuki K, Kasanuki H. Impact of obstructive sleep apnea on clinical and angiographic outcomes following percutaneous coronary intervention in patients with acute coronary syndrome. Am J Cardiol. 2007;99(1):26–30. | ||
Tiihonen P, Hukkanen T, Tuomilehto H, Mervaala E, Töyräs J. Evaluation of a novel ambulatory device for screening of sleep apnea. Telemed J E Health. 2009;15(3):283–289. | ||
Tonelli de Oliveira AC, Martinez D, Vasconcelos LF, et al. Diagnosis of obstructive sleep apnea syndrome and its outcomes with home portable monitoring. Chest. 2009;135(2):330–336. | ||
Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. | ||
Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136–143. | ||
Moussa ID, Klein LW, Shah B, et al. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J Am Coll Cardiol. 2013;62(17):1563–1570. | ||
Mauri L, Hsieh WH, Massaro JM, Ho KK, D’Agostino R, Cutlip DE. Stent thrombosis in randomized clinical trials of drug-eluting stents. N Engl J Med. 2007;356(10):1020–1029. | ||
Chen SL, Ye F, Zhang JJ, et al. Distal left main coronary bifurcation lesions predict worse outcome in patients undergoing percutaneous implantation of drug-eluting stents: results from the Drug-Eluting Stent for the Treatment of Left Main Disease (DISTAL) Study. Cardiology. 2009;113(4):264–273. | ||
Loo G, Koo CY, Zhang J, et al. Impact of obstructive sleep apnea on cardiovascular outcomes in patients treated with percutaneous coronary intervention: rationale and design of the sleep and stent study. Clin Cardiol. 2014;37(10):261–269. | ||
Carlson JT, Rangemark C, Hedner JA. Attenuated endothelium-dependent vascular relaxation in patients with sleep apnoea. J Hypertens. 1996;14(5):577–584. | ||
Cepeda-Valery B, Acharjee S, Romero-Corral A, Pressman GS, Gami AS. Obstructive sleep apnea and acute coronary syndromes: etiology, risk, and management. Curr Cardiol Rep. 2014;16(10):535. | ||
Glantz H, Thunstrom E, Herlitz J, et al. Occurrence and predictors of obstructive sleep apnea in a revascularized coronary artery disease cohort. Ann Am Thorac Soc. 2013;10(4):350–356. | ||
Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053. | ||
Szymanski FM, Filipiak KJ, Hrynkiewicz-Szymanska A, Karpinski G, Opolski G. Clinical characteristics of patients with acute coronary syndrome at high clinical suspicion for obstructive sleep apnea syndrome. Hellenic J Cardiol. 2013;54(5):348–354. | ||
Konecny T, Kuniyoshi FH, Orban M, et al. Under-diagnosis of sleep apnea in patients after acute myocardial infarction. J Am Coll Cardiol. 2010;56(9):742–743. | ||
Lee CH, Khoo SM, Chan MY, et al. Severe obstructive sleep apnea and outcomes following myocardial infarction. J Clin Sleep Med. 2011;7(6):616–621. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.