")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Observed Social Support and Willingness for the Treatment of Patients with Schizophrenia
Authors Jameel HT , Panatik SA , Nabeel T, Sarwar F , Yaseen M, Jokerst T, Faiz Z
Received 25 December 2019
Accepted for publication 5 February 2020
Published 25 February 2020 Volume 2020:13 Pages 193—201
DOI https://doi.org/10.2147/PRBM.S243722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Hafiz Tahir Jameel,1 Siti Aisyah Panatik,2 Tanzila Nabeel,1 Farhan Sarwar,3 Muhammad Yaseen,4 Tricia Jokerst,5 Zikra Faiz6
1Department of Special Education, Allama Iqbal Open University, Islamabad, Pakistan; 2School of Human Resource Development and Psychology, Faculty of Social Sciences and Humanities, Universiti Teknologi Malaysia, Johor Bahru, Johor, Malaysia; 3Department of Business Administration and Economics, University of Education, Township Campus, Lahore, Pakistan; 4Department of Mathematics and Statistics, University of Agriculture, Faisalabad, Pakistan; 5Special Education, Huston-Tillotson University, Austin, TX, USA; 6School of Social Sciences and Humanities, University of Management and Technology, Lahore, Pakistan
Correspondence: Hafiz Tahir Jameel
Department of Special Education, Allama Iqbal Open University, Islamabad, Pakistan
Tel +92 30 0769 6802
Email [email protected]
Background: Schizophrenia is a mental disorder that causes the social breakdown of relationships with others. Patients with schizophrenia interpret reality and verbal communication in an abnormal way. They experience great difficulty in building and maintaining of social relationships within society. They also experience barriers in communication and motivation that hinder their readiness for treatment. The willingness of patients with schizophrenia to be treated improves mental illness, social support and other health-related issues. The main purpose of this study was to explore the relationship between social support and willingness for treatment in patients with Schizophrenia.
Methods: The qualitative research approach was used to solicit and capture more in-depth information from participants. The research design was phenomenological in nature. A cross-sectional survey method was employed. The sample consisted of twenty female patients diagnosed with schizophrenia, seven psychiatrists, and seven psychologists. A semi-structured interview guide was developed to collect the data. The interview guide covered three themes. The first theme included four questions for patients with schizophrenia. The second theme consisted of six questions for the psychiatrists and the third theme included two questions for the psychologists. Interview data were analysed through frame workanalysis.
Results: The results of the study showed that social support plays an essential role in the improvement of patients with schizophrenia. Psychiatrists with the help of medication and therapies reduce the negativity and anxiety level of patients and motivate patients to accept treatment. Through counseling, psychologists help patients with schizophrenia build social skills such as the ability to engage in eye contact.
Conclusion: It is revealed that the social support is closely related to the willingness for treatment in patients with schizophrenia. Therefore, social support is recommended in the course of treatment of patients with schizophrenia.
Keywords: schizophrenia, social support, psychiatric disorders; willingness
Introduction
In the 2001 film “A Beautiful Mind” a brilliant, quirky, superior mathematician; gradually develops schizophrenia. The story conveys the character’s subtle descent into psychological disorder. The viewer does not realize that the mathematician has lost touch with reality until his behavior becomes exponentially out of the ordinary. The character was suffering from schizophrenia, which Rosenstock19 defines as a most mystifying disorder. The patients with schizophrenia experience different symptoms such as positive and negative aspects and intellectual aspects. Positive aspects manifest as an absurdity; negative aspects include the absence of emotions and feelings and chaotic speech; Intellectual aspects include lack of attention span, absence of memory in the study and slow learning speed.11 Schizophrenia is a medical term in which the patient is described as very much disturbed, stressed and lacking socialization skills. Patients with schizophrenia have symptoms of absence of encouragement, low explanation of emotions, intellectual problems, cutoff with socialization and uneducated about any disorder. A major cause of schizophrenia is connected to genetic predispositions; other family members generally show signs of schizophrenia too. Schizophrenia is a complicated neurodevelopment disability that has a genetic component. The causes of schizophrenia include biological factors, genetic factors, prenatal and perinatal factors, biochemical factors, and neuroanatomical, psychological or social factors.21
Schizophrenia is the most prevalent mental disease generally associated with hallucinations and fantastic disorganized emotional lives with relative intellectual preservation. It constitutes approximately 1–2% of the general population with serious psychiatric complaints in Pakistan.6 It is a severe mental disorder that affects about seven adult individuals out of one thousand from the whole population; the individuals most commonly affected are ages 15–35 years old. It affects approximately 1% of the population and does not discriminate between gender or age.9 It typically begins during childhood or teen years.3 Females tend to exhibit more symptoms and later mental illness onset than males. Although the official percentage of diagnosed cases of schizophrenia is low, schizophrenia, as the elementary diagnosis, accounts for approximately 40% of patients admitted in mental hospitals in the US. It is also the second major diagnosed disability in patients admitted to psychiatric centers along with other hospitals and institutes.12
Many factors may increase or decrease the likelihood of developing schizophrenia. These factors include an individual’s perception of social support, which greatly affects readiness for treatment.5 It is treated with the help of medication, psychological counseling, and self-help.14 The term social support is defined as the particular assumptions and perceptions of an individual in regards to how much s/he feels adored, esteemed, and admired by others and feels as if s/he belongs to a circle of communication and collective accountability. Many types of social support are perceived, and others are provided. Each type of social support encompasses different qualities. Researchers have discussed the analysis of independently perceived support, and others have proposed to establish social support in a more fair sense. Personality traits are related to receiving support, expectations related to support for specific events, and perceived social support.22 Studies have shown that observed socialization support is the conclusion of an intellectual and mental personality variable like attribution approach, locus of control or relationship arrangement.4 Social support may have different variables that influence the behavior, attitude, and gaining the support of the person that ease with supportive behaviors recalled and the attribution of one person to provide for uncooperative behaviors.23 Socialization support encompasses many different types and definitions as well as all social behaviors and relationships.10 Social support helps fulfill the social needs individuals possess and fosters self-esteem, connection and provides moral support.24 It may be instrumental in helping or it may just provide intimate interactions based on listening, caring, understanding, a show of self- esteem, advice and direction, all of which are contributions of guidance and knowledge and instruction. It may also be explained as counting the proper feedback about an individual’s reactions or behavior, attention or awareness about feelings and positive social communication for the goal of joy and relaxation.13
One-fourth of short and long stay hospitalized schizophrenic patients did not get any help, and the remainder of the test group received support from only a couple of people. Except for the system size, no noteworthy distinction existed among short and long stay hospitalized patients with schizophrenia. There is a critical contrast among short and long stay hospitalized schizophrenic patients, useful properties of social help, and recurrence of contact. The hospitalization was essentially adversely corresponded with absolute practical help properties and recurrence of contact.15 Information, self-esteem, emotional connections, and the benefits of group exercise are the basic foundational dimensions of psychotherapies used during treatment. Certain dimensions help the patient increase social support and build interpersonal skills. Social support is a part of the rehabilitation professional’s duty, which is apparent in this study.22
Family dynamics at work while receiving social help with a member suffering from unremitting schizophrenia. This examination explored and explained the impression of the family, the patients with schizophrenia and their immediate guardians, on receiving social help.20 Having a satisfactory social support system directly correlates with reduced hospitalization and hospital re-admission among patients with schizophrenia. The patients who have a larger network of support people are spending less time in the hospital and are scoring better. Those patients who spent more than 35 hrs a week with their family members were less often readmitted. Focusing on recovery and avoiding readmissions provides patients the chance to spend more time with their families.8
Social help is one of the best strategies to help cope with upsetting life circumstances. The constructive outcome of the relationship is embedded in satisfying an individual’s need for belongingness, acknowledgment and mental stability. A plethora of research has been conducted to explore the relationship between social help and contending with medical problems. The measure of social help an individual received was found to be related to more elevated amounts of mental pain although the nature of social help has been shown to be progressively significant in dissuading mental misery. Receiving social support requires patients with schizophrenia to be willing or ready to accept help. Many studies have been conducted to explore the motivation and social support for patients with schizophrenia.2 Negative communication creates an unhealthy impact on the patient’s mind and creates negative images about other members of society. Ripke et al,17 described a gauge to measure intrinsic motivation (IM) in patients with schizophrenia. The present research aims to explore the relationship between observed social support and willingness for treatment in patients with schizophrenia. A patient’s emotional support system may originate from a few sources including the family, private expert or day program supplier, cover administrators, companions or flatmates, proficient caseworkers, and others. There are various circumstances in which patients with schizophrenia may need assistance from individuals in their family or network. Frequently, an individual with schizophrenia will oppose treatment. He/she accepts that daydreams or mental trips are genuine and that therapist help is not required. Sometimes, family or companions may need to play a vital function by initiating the medical attention necessary for patients with schizophrenia and maintaining on-going treatment after hospitalization. This study also strives to identify the characteristics and symptoms of patients with schizophrenia, which can be difficult due to the resistance to treatment. This study focused on exploring the relationship between observed social support and patient’s willingness for treatment. Based on an increasing sense of perception towards social support and motivational strategies, psychotherapies are explored along with the psychologist’s views about the benefits of counseling for the patients of schizophrenia. The main objectives of the research were:
- To explore the relationship between observed social support and willingness for treatment in patients with schizophrenia.
- To investigate the psychiatrist’s experiences of observed social support and patients with schizophrenia’s’ motivations for treatment.
- To explore the psychologist’s perceptions about the benefits of counseling compared to observed social support and willingness for the treatment of patients in schizophrenia.
Research Methodology
The qualitative research approach was employed in order to solicit more in-depth information from participants. The research design was phenomenological in nature. The present study was conducted through a cross-sectional survey method.
Procedure of the Study
The intention of this research was to explore the relationship between observed social support and willingness for treatment in patients with schizophrenia. The selected sample consisted of three categories of individuals: twenty female patients with schizophrenia along with seven psychiatrists and seven psychologists who also treat the patients with schizophrenia. Only those psychologists and psychiatrists were selected who treat patients with schizophrenia up to 1 year after getting the respective degree in their field. Sample of patients with schizophrenia was taken from the Mayo hospital, Fountain House and Punjab Institute of Mental Health in Lahore that is a provincial capital of Punjab in Pakistan. All the participants including psychologists and psychiatrists and patients with schizophrenia were selected from the same hospitals for better understanding and results. Only seven psychiatrists, seven psychologists and twenty patients with schizophrenia met with the inclusion criteria for the study.
All patients were diagnosed by a psychologist or psychiatrist according to the 5th edition Diagnostic Statistical Manual (DSM-V) and also used Magnetic Resonance Imaging (MRI) and Computerized Axial Tomography (CT) scans. After the completion of the diagnosing process, the treatment began. The psychologist participants were well qualified and experienced in the counseling of patients with schizophrenia. All patient participants had at least a primary education. All the participants were selected using a purposive sampling technique. Patients suffering from any co-morbid disorders were excluded.
A semi-structured interview guide was developed to collect the data. The interview guide was comprised of three sections, and each section was specific to the category of the participants. The first section included four questions for the patients with schizophrenia. The second section consisted of six questions for the psychiatrists, and the third section included two questions for the psychologists. In order to formally initiate the study, Ethical Review Committee, Allama Iqbal Open University, Islamabad, Pakistan approved the study in accordance with the Declaration of Helsinki. In addition, written informed consent was taken from the patients with schizophrenia. After appropriating official legal permission from the administrator of the respective hospital, the data collection process began. The purpose of the current research was explained to all the participants before conducting interviews. The interview duration was approximately 30–40 minutes. The procedure and protocols of the interview has been given in Table 1.
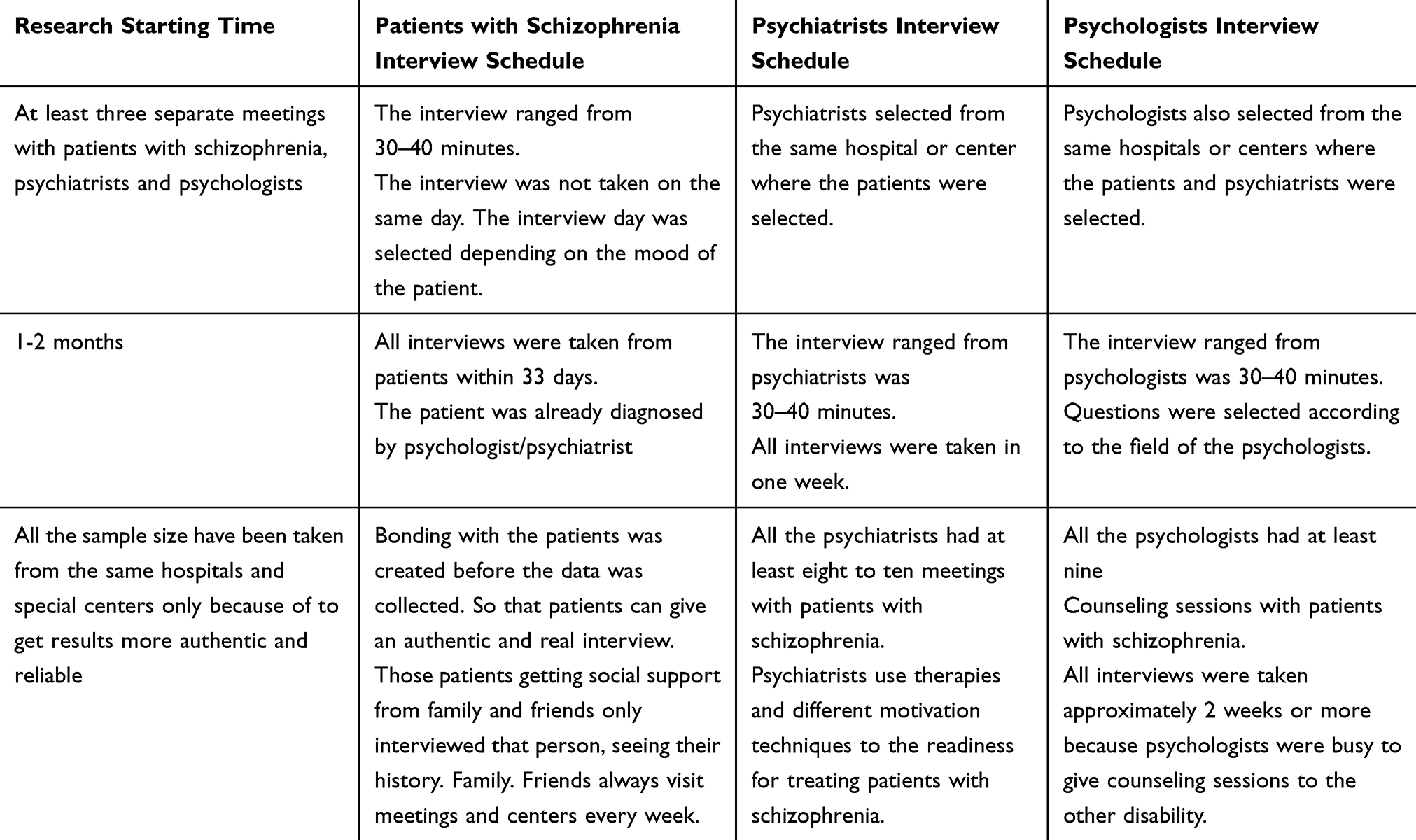 |
Table 1 Schedule and Procedure of the Interview of Participants |
Data Analysis
Framework analysis was used in this study. It included a methodical procedure of filtering, outlining and arranging material as per key issues and themes. Five systematic methods “acclimation, distinguishing a topical structure, ordering, outlining, mapping also, and understanding” was applied to the meeting information in request to comprehend recognition and practices to observed social support and willingness for patients with schizophrenia.1,18 For acquaintance, the specialist tuned into and read through the sound tapes and meeting transcripts material so as to list key thoughts and intermittent subjects. Key issues, ideas and topics recognized through acclimation were then used to set up a topical system, for the most part drawing upon from the earlier issues. The third system, ordering, was utilized by efficiently applying the topical structure to the meeting information in its literary structure. At that point information was “lifted from their unique setting and revised by the proper topical reference” and graphs were contrived with headings and subheadings, a key trait of outlining the strategy. The last method was “mapping and understanding” which included the analysis of the key attributes as spread out in the graphs. Spreading out graphs specifically and contrasting and differentiating every one of the respondents’ observations and practices helped in creating developing topics, which are accounted for in the following section.
Results of the Study
This section has been prepared according to the data collection by researchers and also includes the analysis and interpretation of the collected data. The demographic information has been explained in Table 2.
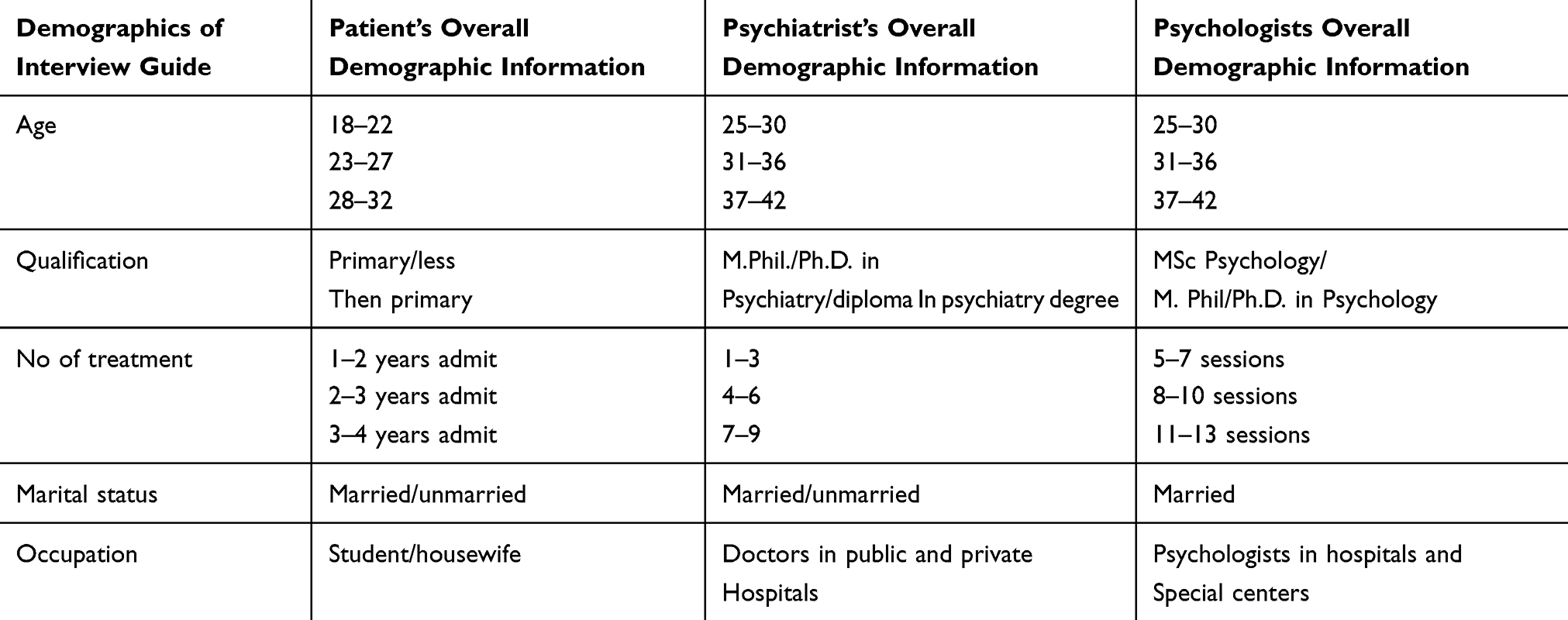 |
Table 2 Demographic Information of the Patients with Schizophrenia, Psychiatrist and Psychologist |
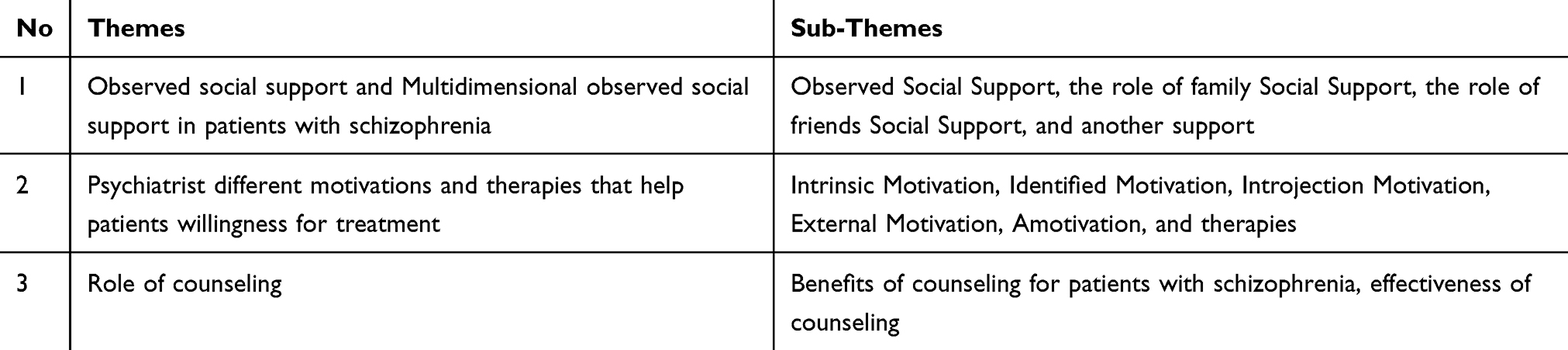 |
Table 3 Themes and Subthemes Developed from the Semi-Structured Interview |
Table 2 contains participants demographic information. Patient participants ranged in age from 18–32 years old. The qualification of all these patients is primary (five class). All patient participants had been admitted to a hospital for 1 to 3 years and have had a great number of treatments from various doctors. Fourteen participants were married and housewives. Fifteen participant’s ages were 31 to 36 years old. The psychiatrist participants possessed qualifications as M.Phi or Ph.D. in psychiatry, and four psychiatrists treated 7–9 patients. All professional participants treat patients with schizophrenia as a doctor in public and private hospitals. The psychiatrists were a combination of married and unmarried. According to the demographics, the psychologists’ ranged in age from 25 to 42 years old and were qualified as MSc psychology or M.Phil psychology. Five psychologist participants had provided eight to ten counseling sessions and worked in various hospitals and special centers. All these participants were married.
The thematic analysis was based on the three themes. Each theme includes four, six and two questions which are is given in Table 3.
Theme 1: Observed Social Support and Multidimensional Observed Social Support in Patients with Schizophrenia
Social support is imperative for patients with schizophrenia. Patients in hospitals or daycare centers need to have at least one person, such as a nurse, available who can take care of them. All female patients with schizophrenia shared their happy and sorrowful feelings with a specific person, whom they trusted. Social support from family, peers, and friends provides positive emotional feelings to the patient. Patients with schizophrenia try to reduce their depression and illness with the help of social support. Lack or absence of social support seems to make patients more aggressive, which leads to negativity and increases the patients’ mental problems. If the patient’s relatives or friends do not contact the patient after admittance to the hospital, the patient becomes more negative, which increases depression. Unmarried patients tend to be depressed and experience more mental health problems than married patients with schizophrenia.
Family attitude and patient’s importance in the family are two factors that greatly influence the patient’s positive emotional state. Having one special person such as a mother, sister or grandmother is a source of comfort. Patients who do not have family immediately present in their lives depend on friends for support. Patients tend to share their problems with their family members before they share with friends. The patients stated that they always need family help and support. Patients with schizophrenia tend to resist treatment because of delusions and/or hallucinations. A psychiatrist cannot easily treat without the patient’s permission and cooperation. Family plays a vital role during treatment and can greatly influence patient decisions. Some families are able to hire psychiatrists, psychologists, or other professionals to treat the patient at home if the patient will not agree to go to the hospital. After a few months of home care, many patients are willing to get admitted to a hospital. With family support, patients feel more positive. Symptoms of depression, illness, and other mental health issues dissipate quickly when family support is present. Twelve participants reported that their family members discuss all matters with them and make decisions that are very supportive of them.
Eight participants expressed that friends provided more social support compared to family members. All the patients reported a happy feeling when family and friends provided social support during treatment. Social support appears to greatly increase the probability of patient improvement. Sometimes, patients never share their problems or issues with their friends. They reported thinking friends are not important in their life. Participants frequently think they are not ready for treatment or talk with a doctor but do not follow through with instructions or recommendations. However, friends’ support eventually convinces the patient to accept treatment.
Thirteen participants identified doctor encouragement and psychiatric counseling as highly effective and helpful in increasing motivation for treatment. The positive behavior and attitude from nurses and doctors tended to develop the patients’ willingness for treatment. The patients reported the hospital environment affects the social support the patient receives. When patients are insulted or treated inappropriately, they are more likely to behave in a negative way such as breaking things and shouting. These patients rarely attend therapies or sessions. One participant pleasantly shouted that “I love my doctor that’s why I am still here and I want to marry my doctor only because of doctor’s support”. One patient professed great affection for her doctor and attributed her success to her doctor. Patients reported regularly taking medications and receiving proper treatment.
Theme 2: Psychiatrist’s Different Motivations and Therapy Help Patient’s Willingness for Treatment
Psychiatrists reported that schizophrenia causes patients to experience a connection deficit in motivation and cognitive abilities. They stated patients tend to live in a life of fantasy and imagination, which greatly hinders motivation to change. Psychiatrists said patients consider motivation differently. Positive motivation, negative motivation, and cognitive motivation help to reduce hallucinations symptoms. Negative thinking creates a major block in changing the patient’s mind and motivation goal. Patients with schizophrenia live in the past and cannot accept the reward. Psychiatrists expressed that the absence of motivation is the primary issue schizophrenia patient’s face. Five psychiatrist participants report that both intrinsic motivation and external motivation are very important during the treatment of the patient with schizophrenia. Intrinsic motivation helps patients to engage themselves in activities and motivates the patient, which can be beneficial even without some external reason. External motivation such as money encourages some patients. Some psychiatrists expressed that identified motivation, introjection motivation and motivation can also be very helpful to increase patients’ willingness for treatment. All these motivations encourage patients and motivate them internally, externally, and mentally and prepare the patient for treatment. All types of motivation increase a patient’s likelihood of improving mental illness and situation. Through intrinsic motivation, psychiatrists engage the patient in different tasks that end with some reward such as an absence of punishment, a gift, or food.
Therapies also proved helpful for increasing a patient’s willingness for treatment. Five psychiatrists agreed that therapy aids in changing a patient’s mind and increases willingness for treatment. Patients do not understand the reality of the situation. Psychiatrists reported family members and other social supports who talk to the patients about the benefits of therapies encourage patients to accept treatment. Therapy allows patients to handle the situation and leads to a more positive state of mind. Therapies help the patients with schizophrenia to have a better understanding of them. Three of the psychiatrist’s participants purposed that some patients with schizophrenia find therapies boring. Speech therapy, cognitive behavior therapy, and behavior modification therapy are most commonly used by psychiatrists during therapy sessions. Medication is also very helpful during treatment. Three psychiatrists discussed psychotherapy as a useful strategy for treating patients with schizophrenia. Psychiatrists reported usually using one to one therapy during treatment. Therapy helps to reduce the symptoms of trauma in the patient. Cognitive remediation therapy (CRT) improves the patient’s cognition level by engaging the patients in various exercises related to sensory activities. One psychiatrist said art therapy is another useful tool in which patients create expressions and feelings through painting. This allows the psychiatrist to easily decrease negative symptoms in the patient.
Theme 3: Role of Counseling
Six psychologists reported that counseling is an essential and compulsory element for patients with schizophrenia. During counseling, psychologists choose different activities and techniques to easily engage patients with schizophrenia. Shaping and chaining, token economy, sports, art and coloring, outdoor and indoor activities are some examples. These techniques and activities are designed to change a person’s mind, beliefs, and clearly confused thinking. Psychologists clarify the concepts of right and wrong. Psychologists reported staying in touch with family and friends improved the patient’s willingness for treatment. Through counseling, psychologists develop social interaction and engagement in the patients. Psychologists conducted three individual counseling sessions with the patients that each lasted approximately 20–30 mins. Psychologists consulted with psychiatrists regarding the counseling session. Medication tends to increase patients’ positive thinking and promotes session attendance. Some activities used during counseling reduce the anxiety and depression levels of patients. Most psychologists agreed that counseling is only beneficial when the patient is mentally ready for change and willing to accept social interaction. Counseling can manage the illness of the mind and emotions of the patients.
Counseling is most effective when medication and therapy are simultaneously combined. Psychologists reported that frequent and consistent use of medication can sometimes be harmful to the patient. Through counseling, psychologists motivate patients and provide support at schools by providing proper guidelines for parents and friends on how to treat patients with schizophrenia at home. Psychologists can change the cognitive and ability level of the patients with schizophrenia. After counseling, patients with schizophrenia may communicate with others and think more effectively. Psychologists never choose one domain; they use all domains like social support of family, friends, therapies, psychiatrists before starting counseling of patients. Psychologists also create a standardized test and assessment of each patient.
Male patients with schizophrenia were not included in the study because the number of patients with schizophrenia was less as compared to female patients with schizophrenia. The clinic visited to conduct the study had about 80% female patients with schizophrenia. However, further studies may be conducted on male patients with the same specifications which would lead to the comparison in dealing with male and female patients with schizophrenia. This study was conducted in Lahore which is one of the provincial capital of Pakistan. the literacy rate of the population and level of awareness among masses is much higher than in other cities. There are established psychiatric clinics at Lahore as the participants prefer to establish their clinics or work at metropolitan cities. People are more open to sharing their experiences and feelings. This could enable them to infer the realistic and genuine feelings of patients as well as the doctors. However, for future studies, the region-wise data may be collected to compare the dynamics and responses of the patients and their families.
Discussion
The present research focused on exploring the relationship between observed social support and willingness for treatment in patients with schizophrenia. Interviews were conducted with patients with schizophrenia diagnosed by both psychiatrists and psychologists. The sample was drawn from various psychiatric departments of hospitals in Lahore such as Punjab Institute of Mental Health, Fountain House and Mayo Hospital. Social support proved to be very important for a person who is suffering from schizophrenia. Social support includes family, friends, doctors and other forms of social support. If all the members of society encouraged patients suffering from schizophrenia, then the patients would not feel so different from other people and would not feel shame. Findings suggested that deficits in observed social support are associated with deriving social phobia, which may be the cause of co-morbid issues and explicate target treatment for social phobia. Low correlations between observed social support and social anxiety measures suggest that observed social support should be specifically evaluated in this population. The meditating roles of observed social support and psychological distress show a relationship between adult attachment and help-seeking intentions. Individuals negatively contributed to their experience of distress and then positively contributed their help-seeking intention. These results are consistent with research conducted by Pandya et al,16 who found that social support of family and friends helps to offset the adverse effects experienced by mothers of critically ill children. Mothers chose between alternative sources of social help from family, companions, and other supportive sources. Family companions and important others were shown to be free independent sources of social support, which affirmed past work. Jindal et al,7 described a clinical profile of back sliding patients with schizophrenia who attended day by day practice. Patients with schizophrenia in short-remain/intense consideration mental units agreed to provide information from the past three years and for a year after their release. No distinctions in the quantity of relapsing patients taking antipsychotic drugs occurred. Over a ten years span, a profile of a relapsing schizophrenia patient was developed, which documented low family support, numerous antipsychotic medication treatments, and poor adherence to treatment. Antipsychotic drug types were not monitored during the patient backslide. However, the long-acting second era antipsychotic medications showed the most noteworthy level of greatest adherence. Psychiatrists and psychologists helped patients to decrease the symptoms of depression, anxiety and mental illness. The psychiatrists used different therapies to engage and motivate the patient to be willing to accept treatment. Psychiatrists’ positive attitude encouraged and motivated the patient. Family, friends and other social supports played a vital role in changing the life of a person who is suffering from schizophrenia. Social support helps patients to see the condition and comply with their psychiatrist’s treatment. Social support encourages the willingness for treatment. Without support, many patients would never agree to treatment and continue to think they were not sick and other people are wrong. Therapies play an important role in communication and reduce the symptoms of depression. Social support develops a relationship with the patients. Cognitive behavior therapy, speech therapy and cognitive enhancement therapy builds the patient’s skills and mind and develops relationship skills. Psychiatrists use medication to reduce side effects in patients with schizophrenia. The most commonly used drugs are Aripiprazole (Abilify), Asenapine (Saphris), Brexpiprazole (Rexulti), Cariprazine (Vraylar) and Clozapine (Clozaril). Through counseling sessions, psychologists are able to reduce the patient’s stress and help them feel relaxed. Sometimes, medication can have side effects. During these times, psychologists only choose the patients’ favorite activities and topics for the counseling sessions. Counseling improves socialization skills, eye contact, and academic and social skills in the patients.
Conclusion
The current study revealed that observed social support is positivity related to the perception of treatment and readiness for treatment. Results showed if the patient with schizophrenia observes their social support in a positive way, they are likely to get treatment, which will reduce the rigidity and facilitate the improvement of their symptoms. Psychotherapy is designed to increase the positive perception of social support and motivation. This research will help psychotherapists as well as psychiatrists to understand how observed social support motivates a person who is suffering from schizophrenia to agree to treatment Social support will increase the patient’s willingness to participate actively in the diagnostic evaluation. Further, it will be beneficial for family members to understand the characteristics of schizophrenia. The current research will be helpful in the development of observed social support and willingness for treatment in patients with schizophrenia.
Recommendations
For further studies it is recommended that tha data may be collected from the hospital in different cities to generalize the data on Pakistan population on large scale. The researcher should use measures that decrease social desirability. Only counseling effects can also be check for patients with schizophrenia.
Funding
The researchers did not receive any financial support for the implementation of the research nor for the authorship of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bryman A, Burgess RG. Analyzing Qualitative Data. Vol. 11. London: Routledge; 1994.
2. De Hert M, Schreurs V, Sweers K, Van Eyck D, Hanssens L, Šinko S. Typical and atypical antipsychotics differentially affect long-term incidence rates of the metabolic syndrome in first-episode patients with schizophrenia: a retrospective chart review. Schizophr Res. 2008;101(1–3):295–303. doi:10.1016/j.schres.2008.01.028
3. Fett A-KJ, Viechtbauer W, Penn DL, van Os J, Krabbendam L. The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: a meta-analysis. Neurosci Biobehav Rev. 2011;35(3):573–588. doi:10.1016/j.neubiorev.2010.07.001
4. Gitlin LN, Rose K. Factors associated with caregiver readiness to use nonpharmacologic strategies to manage dementia‐related behavioral symptoms. Int J Geriatr Psychiatry. 2014;29(1):93–102. doi:10.1002/gps.3979
5. Gross J, Vancampfort D, Stubbs B, Gorczynski P, Soundy A. A narrative synthesis investigating the use and value of social support to promote physical activity among individuals with schizophrenia. Disabil Rehabil. 2016;38(2):123–150. doi:10.3109/09638288.2015.1024343
6. Irfan M, Caldas de Almeida JM, Irfan UM, Raza UA, Farooq S. Schizophrenia diagnosis and treatment by general practitioners: A cross-sectional study in district Peshawar, Pakistan. J Pak Med Assoc. 2015;65(9):937–942.
7. Jindal RD, Pillai AK, Mahadik SP, Eklund K, Montrose DM, Keshavan MS. Decreased BDNF in patients with antipsychotic naive first episode schizophrenia. Schizophr Res. 2010;119(1–3):47–51. doi:10.1016/j.schres.2009.12.035
8. Kasckow J, Felmet K, Zisook S. Managing suicide risk in patients with schizophrenia. CNS Drugs. 2011;25(2):129–143. doi:10.2165/11586450-000000000-00000
9. Kate N, Grover S, Kulhara P, Nehra R. Relationship of caregiver burden with coping strategies, social support, psychological morbidity, and quality of life in the caregivers of schizophrenia. Asian J Psychiatr. 2013;6(5):380–388. doi:10.1016/j.ajp.2013.03.014
10. Meehl PE. Schizotaxia, schizotypy, schizophrenia. Available from: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.462.2509&rep=rep1&type=pdf. Accessed February 17, 2020.
11. Moslem M, Olive J, Falk A. Stem cell models of schizophrenia, what have we learned and what is the potential? Schizophr Res. 2018;210(2019):3–12. doi:10.1016/j.schres.2018.12.023
12. Müller R, Peter C, Cieza A, Geyh S. The role of social support and social skills in people with spinal cord injury—a systematic review of the literature. Spinal Cord. 2012;50(2):94. doi:10.1038/sc.2011.116
13. Nilsen L, Frich JC, Friis S, Røssberg JI. Patients’ and family members’ experiences of a psychoeducational family intervention after a first episode psychosis: a qualitative study. Issues Ment Health Nurs. 2014;35(1):58–68. doi:10.3109/01612840.2013.837992
14. Nordqvist C. Understanding the symptoms of schizophrenia; 2017. Available from: https://www.medicalnewstoday.com/articles/36942.php.
15. Ossman LH, Mahmoud NM. Social support and length of hospital stay among schizophrenic patients. World Appl Sci J. 2012;19(5):625–633.
16. Pandya CD, Kutiyanawalla A, Pillai A. BDNF–TrkB signaling and neuroprotection in schizophrenia. Asian J Psychiatr. 2013;6(1):22–28. doi:10.1016/j.ajp.2012.08.010
17. Ripke S, Neale BM, Corvin A, Walters JT, Farh K-H, Holmans PA. Biological insights from 108 schizophrenia-associated genetic loci. Nature. 2014;511(7510):421–427. doi:10.1038/nature13595
18. Ritchie J, Lewis J, Nicholls CM, Ormston R. Qualitative Research Practice: A Guide for Social Science Students and Researchers. Sage; 2013.
19. Rosenstock J. Beyond a beautiful mind: film choices for teaching schizophrenia. Acad Psychiatry. 2003;27(2):117–122. doi:10.1176/appi.ap.27.2.117
20. Sawant NS, Jethwani KS. Understanding family functioning and social support in unremitting schizophrenia: a study in India. Indian J Psychiatry. 2010;52(2):145–149. doi:10.4103/0019-5545.64593
21. Sibitz I, Amering M, Unger A, Seyringer M, Bachmann A, Schrank B. The impact of the social network, stigma and empowerment on the quality of life in patients with schizophrenia. Eur Psychiatry. 2011;26(1):28–33. doi:10.1016/j.eurpsy.2010.08.010
22. Soundy A, Freeman P, Stubbs B, Probst M, Vancampfort D. The value of social support to encourage people with schizophrenia to engage in physical activity: an international insight from specialist mental health physiotherapists. J Ment Health. 2014;23(5):256–260. doi:10.3109/09638237.2014.951481
23. Vancampfort D, Vansteenkiste M, De Hert M, De Herdt A, Soundy A, Stubbs B. Self-determination and stage of readiness to change physical activity behaviour in schizophrenia. Ment Health Phys Act. 2014;7(3):171–176. doi:10.1016/j.mhpa.2014.06.003
24. Vera-Garcia E, Mayoral-Cleries F, Vancampfort D, Stubbs B, Cuesta-Vargas AI. A systematic review of the benefits of physical therapy within a multidisciplinary care approach for people with schizophrenia: an update. Psychiatry Res. 2015;229(3):828–839. doi:10.1016/j.psychres.2015.07.083
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.