")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 8
Nutritional self-care among a group of older home-living people in rural Southern Norway
Authors Dale B , Soderhamn U
Received 8 October 2014
Accepted for publication 29 October 2014
Published 23 January 2015 Volume 2015:8 Pages 67—74
DOI https://doi.org/10.2147/JMDH.S75521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bjørg Dale, Ulrika Söderhamn
Centre for Caring Research – Southern Norway, Faculty of Health and Sport Sciences, University of Agder, Grimstad, Norway
Background: Older home-living people are an at-risk group for undernutrition, particularly those who are living alone. Lack of knowledge about healthy dietary habits, altered taste sensation, and declined health status are shown to be some of the factors related to undernutrition. The aims of this study were to explore how a small group of older people in Southern Norway perceived their nutritional self-care.
Methods: An exploratory qualitative approach, combined with a simple self-report questionnaire, was used. Five persons living in rural areas in Southern Norway, who in a former study were screened and found to be at risk for undernutrition, participated. Qualitative data assessed by means of individual self-care talks in the persons' own homes were analyzed using directed content analysis. A simple self-report questionnaire containing demographic variables, two health-related questions, and the Nutritional Form For the Elderly (NUFFE-NO) instrument was filled out at baseline and 6 months after the self-care talks.
Results: The qualitative data showed that the participants had adequate knowledge about healthy and nutritious diets. They were aware of and motivated to adapt their diet to their current state of health and to perform the necessary actions to maintain an optimal nutritional status and nutritional self-care.
Conclusion: Older people living at home are a diverse group. However, this study showed that they may have sufficient knowledge, willingness, and ability to perform nutritional self-care, even if they live alone and have several chronic illnesses and impaired health.
Keywords: adapting, decision-making, knowledge, self-care talks
Introduction
Older people are an at-risk group for undernutrition,1 and a sufficient food intake in older age is necessary in order to prevent undernutrition.2 However, studies among home-living older people have revealed an inadequate food intake as a major health challenge.3,4 Also, older people with a healthy lifestyle, such as being physically active, can have a low intake of key nutrients such as vitamins and calcium. An adequate intake of calcium, for example, is important in reducing the risk for impaired cognitive function.3 Barriers to practicing a healthy diet can be lack of knowledge about healthy dietary habits and the fact that unhealthy food is cheaper, has a pleasant taste, and is easy to prepare.5 In a qualitative study among older persons screened and found to be at risk for undernutrition, it was revealed that the participants considered a varied healthy food intake of fish, meat, vegetables, and fruits to be important.6 However, the findings in that study6 also indicated that taste could guide the choice of food, and that food that was easy to prepare, but assessed as nutritionally sufficient, could be preferred.
Studies among older home-living people have revealed that perceived impaired health,7,8 living alone and being in need of help to manage daily life,2,8,9 and being inactive2,9 are some of the risk factors for undernutrition. Older women living alone are found to be particularly at risk because of simplified cooking and eating.10 Lower social support in older age has also been found to be related to nutritional risk,11 and reduced social activity can predict unintended weight loss12 and social isolation.13
According to Orem,14 a person’s self-care includes knowing capabilities, decision-making capabilities, and doing capabilities that enable him or her to initiate and perform activities on their own behalf to maintain life, health, and well-being. Hence, these self-care capabilities are important for older persons to be able to live independently in their own homes.15 There is an association between self-care ability and nutritional state in older people, ie, higher self-care abilities are found to be associated with lower risk for undernutrition.16,17 Factors found to be closely related to higher self-care ability are not receiving help, being able to prepare food, being active, and being at low risk for undernutrition.17 The perception of having good health in general, and having good mental health in particular, has also been found to be associated with higher self-care ability.18 Moreover, the perception of better health and greater life satisfaction has been found to be associated with daily intake of vegetables and fruit.19
In an intervention study by Wunderlich et al,20 among older people ≥60 years old with home-delivered meals or congregated meals, the results showed a reduced risk for undernutrition after nutrition education and counseling. Since nutritional risk in older age is associated with increased chronic illnesses, dependency on help,2,21 lower self-care ability,17 and perceived ill health,7,8 there is a need for qualitative studies focusing on older individuals’ self-care resources in order to prevent worsening of the nutritional risk or improve the nutritional state.
The aim of this study was to explore how a small group of older people in Southern Norway perceived their nutritional self-care.
Methods
Design
A qualitative, explorative design was used, and individual self-care talks related to nutrition and food intake were carried out during 2012. In addition, a self-reported questionnaire was filled out at baseline and 6 months after the self-care talks.
Recruitment of participants and data collection
Twenty-four older persons living in rural areas in four counties in Southern Norway were invited to participate in the study. In a former study performed in 2010,17 these persons had been found to be at risk for undernutrition, measured by the screening instrument, the Nutritional Form For the Elderly (NUFFE-NO).22 Five persons agreed to participate. The study group filled out a self-report questionnaire containing NUFFE-NO22 at baseline and again after 6 months. Background information about the study group is displayed in Table 1.
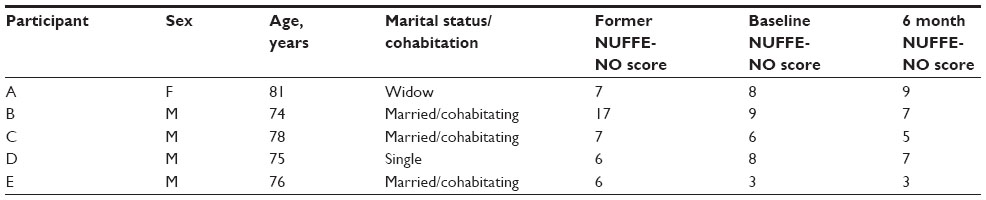 | Table 1 Background variables of the study group and NUFFE-NO scores found in the former study, at baseline, and 6 months after the self-care talks (n=5) |
The participants returned written consent to be visited for a talk by one of the authors in their own home. The purpose of these visits and talks was to gain a deeper insight into the older persons’ self-care related to nutrition and food intake, and to possibly give advice about nutrition if needed. The conversations were audiotaped and subsequently transcribed verbatim by the researcher who conducted the visit.
The questionnaire and screening instrument
The self-report questionnaire consisted of background variables (sex, age, marital status, and type of dwelling), health-related questions (perceived good health or not and presence of chronic diseases or not) that could be answered by “yes” or “no”, and the nutritional screening instrument NUFFE-NO.
The original Nutritional Form For the Elderly is a nutritional screening instrument, at ordinal level, developed in Sweden, for screening older people regarding risk for undernutrition.23,24 It contains 15 three-point items that involve dietary history, dietary assessment, and general assessment. The most favorable option produces a score of 0 and the most unfavorable option a score of 2. The maximum score is 30. Higher screening scores indicate higher risk for undernutrition. The instrument is translated into Norwegian (NUFFE-NO),22 and testing studies have shown satisfactory results regarding reliability and validity,22,25 indicating that the instrument includes adequate psychometric properties for screening older people. Cut-off scores of ≥6 are identified to indicate risk for undernutrition.22
The self-care talks and the qualitative content analysis
Individual face-to-face self-care talks were performed in the informants’ own homes, lasting from 30 to 45 minutes. The first author visited three of the informants, and the second author visited two of them. The authors are both trained nurses and experienced researchers. Initially, the participants were asked to describe freely how they perceived their own situation with regard to meeting appropriate food and nutrition needs. Thereafter, based on data registered in the questionnaire, they were asked to reflect on the answers which were of particular concern. In addition, a thematic guide was prepared to ensure that the content of the self-care talks included the same themes for all participants. Self-care abilities related to knowledge, needs, and resources were the focus, ie, the participants’ abilities to gain, prepare, and eat the food they wanted and needed. The self-care talks also included confirmation of the knowledge the participants had and provision of appropriate advice and suggestions, if needed.
The transcribed texts from the self-care talks were analyzed by both authors. A directed, deductive content analysis approach inspired by Hsieh and Shannon26 was used. Directed content analysis is typically used to validate or extend an existing theory or research, and is normally guided by fairly structured themes or questions.26 This analysis approach was appropriate to use in our study because the themes that were the focus, and the categorizing of the findings, were developed a priori according to Orem’s14 self-care capability domains.
Ethics
The study was approved by the Regional Committee for Medical Research Ethics in Southern Norway (REK sør-øst D 2009/1299 and REK sør-øst B 2012/191). The authors were guided by the intentions of the Declaration of Helsinki (2013)27 and ethical standards28 when designing and performing the study. Written informed consent was obtained from the study group before they were contacted for making appointments regarding the home visits. The participants were guaranteed anonymity and confidentiality.28
Findings
The mean age in the study group was 76.8 years (standard deviation =2.8). The participants were all living in their own homes, and all of them had one or more chronic illnesses. However, only two of the participants perceived bad health at baseline, and one perceived bad health 6 months after the visit. As displayed in Table 1, there were only minor differences found in the study group before and after the self-care talks regarding total scores on the NUFFE-NO instrument. One informant had a great reduction in NUFFE-NO scores between the data collection in the former study in 2010 and the data collection at baseline in the present study. A likely explanation for the marked reduction in NUFFE-NO score for that person is that he had undergone a major operation that had improved his nutritional state and appetite.
The findings from the self-care talks in the participants’ homes were categorized according to Orem’s domains of self-care capabilities, ie, knowing capabilities, decision-making capabilities, and doing capabilities.14 According to Orem,14 sufficient knowledge is fundamental for making appropriate decisions and performing appropriate self-care actions.
Knowing capabilities
The overall impression was that the informants had relevant knowledge and were conscious about their nutritional needs, appropriate food intake, and how to compose meals containing necessary nutrients. Having regular daily meals and eating suitable portions were preferred, and the participants demonstrated great knowledge and awareness regarding the nutritional value of food, for example, the importance of eating vitamins, minerals, proteins, and appropriate amounts of calories. Some of the informants also highlighted the importance of avoiding prefabricated food and making everything from scratch. They acknowledged that their level of activity was decreased due to higher age and chronic diseases and, consequently, that their needs regarding food intake had changed. In addition, they paid attention to their weight to make sure that it was not undesirably high or low. Having a varied diet and regularly eating fish, meat, fruit, vegetables, and wholemeal bread was considered important, and all informants considered their nutritional habits and lifestyle to be healthy or fairly healthy. Knowledge and awareness about having sufficient and appropriate fluid intake was also present, and the informants had knowledge about the consequences of insufficient fluid intake. Some of them had read books or articles to obtain information about nutrition and diets, either general or disease-related information and recommendations. One of the informants had read about and was particularly engaged in a special diet recommended by an American doctor, which was about balancing intake of vitamins and calories, avoiding red meat, eating a lot of fruit and vegetables, and consuming lots of fluids. The informant described what he had read:
[…] he (the American doctor) is very concerned about vitamins and calories. He says that Americans are poisoned by all the processed foods they are eating which are full of all sorts of poisons. He is concerned that Americans live so miserable and unhealthy. So much of what he writes in the book, I have adopted myself. [E]
Another informant explained that he preferred a Mediterranean type of diet, which he had read a lot about. Incidentally, all participants emphasized eating what they described as “ordinary Norwegian usual fare”, and what they had been used to since their childhood.
All participants had several chronic diseases and were dependent on medications which caused unpleasant symptoms and side effects for most of them. However, they had learned to cope with and adjust to their actual health conditions and found different means of managing side effects of medications. For instance, one of the informants had figured out that the use of herbal supplements could be an appropriate way to deal with unwanted side effects such as nausea and obstipation.
Decision-making capabilities
The informants also demonstrated that they had resources for making necessary and appropriate decisions about their diet and food intake. The information and knowledge they obtained constituted the basis for decision-making; for example, if modifying calorie intake, avoiding fat because of indigestion, or avoiding sugar because of diabetes was needed. One of the informants who had recently been diagnosed with diabetes expressed the following:
I read, you know, and I am attentive to follow my diet … one has to change some old habits. If you are fond of chocolate you can avoid having it in the kitchen cupboard. But sometimes I buy an ice cream so I have something good with my coffee … the ones without sugar you know … it is good. [D]
However, skepticism against what they described as “fanatical diet advice” was expressed, and finding one’s own sensible solutions was preferred. One informant (A) put it this way: “you have to use common sense and find everyday cost habits which are suitable and practical to follow.”
Some of the informants made weekly plans for dinner meals to assure a variety of fish, meat, and vegetables. Three informants were married and cohabitants and they expressed how important it was for them to jointly discuss, plan, prepare, and enjoy their meals. One of the widowed informants described that she occasionally felt lonely. However, she enjoyed and was highly motivated about preparing dinner or a hot meal every day, and it was no problem for her to eat alone. Sometimes she invited a friend or a neighbor for dinner. Other times she planned and prepared a large portion, which was divided into smaller portions and stored in the deep freezer. The other alone-living informant said that he occasionally had dinner with a friend or had dinner at the senior center in order to have company during meals.
The activity level varied a lot among the study participants, mainly due to their health conditions. Symptoms like pain, functional disabilities, and unsteadiness caused by osteoarthritis or reduced physical capacity as a result of heart failure were some of the problems they described. However, they were conscious of the importance of regular activity and they were motivated to move as much as they could, not least because they considered it important to balance activity and food intake to keep a suitable weight. For example, one of the informants had figured out that cycling on an exercise bike while watching the news on TV was great.
Doing capabilities
In addition to appropriate knowledge, motivation, and ability to make decisions about their nutritional self-care, the informants gave rich descriptions about how they performed actions to attend to their nutritional needs. Mostly, this was about properly adjusting their diet regarding their actual health condition. They performed necessary actions by, for instance, avoiding food that caused problems and symptoms and by eating certain products that could ease them. One of the informants had previously undergone surgery for bowel cancer and had some problems in the form of nausea and symptoms of dumping syndrome. However, he had experienced and learned that eating small and frequent meals with reduced fat, and lying down for 20 minutes after meals, were ways for him to prevent the symptoms. Most of the participants were engaged in and put a lot of effort into composing and preparing components of a healthy and recommended diet. One of the informants, who was living with his wife, said:
We spend a lot of time in the kitchen preparing food – much more time than people in general at our age. We make everything “from the bottom” – no semi-finished products for us! We are here in the kitchen and enjoying ourselves, having a glass of wine while we make food … vegetables should be peeled and chopped and everything takes a lot of time. Yes, we spend a lot of time in the kitchen, and we enjoy it. [B]
The informants used available knowledge and their creativity to vary the content of their meals, and it appeared that the preparation of food and meals was an important part of their daily lives, even if they lived alone. They planned grocery shopping, and they were all able to shop for all the food they needed. One of the informants took much pleasure in cultivating his own vegetable and herb garden, and these products were a natural part of their daily diet. Another informant explained that she was attending a senior center twice a week, and she enjoyed these gatherings a lot. However, when it was time to eat, she went home, because she usually preferred to prepare her own food and eat it in peace and quiet alone.
Discussion
The aim of this study was to explore how a small group of older people in Southern Norway perceived their nutritional self-care.
According to Orem,14 a person’s self-care includes having necessary knowledge, the ability to make decisions, and the ability to act appropriately in accordance with actual self-care needs. Although all the participants in this study were initially screened and found to be at risk for undernutrition, an overall impression from the dialogues was that they demonstrated having a lot of resources for maintaining their nutritional self-care. They were conscious about their actual health condition and what precautions they had to take the abilities to balance the intake of appropriate food and drinks, balance the need for appropriate activity and rest, balance the need for social interaction and solitude, and protect oneself from unintended harm or risk to make sure they maintained a proper and healthy diet. They were able to make decisions and accept the necessary consequences of nutritional restrictions or adjustments when needed. Although insufficient knowledge is found to be a major reason for poor nutritional status in older adults,29 this seemed not to be the case in our study. However, appropriate knowledge is not sufficient for practicing healthy dietary habits. Another important aspect related to the maintenance of good nutritional status is the older person’s belief in their own ability to complete tasks and reach goals.30 Enjoying healthy and varied food and meals may be goal priorities for older people, and is found to increase their quality of life.31
Having difficulties with meal preparation, caused by general tiredness or declined capacity, is found to be a significant factor related to older persons’ poor nutritional state or risk for undernutrition.30 This was not the case for the participants in the current study. They expressed that they spent quite a lot of time obtaining and preparing appropriate and tasty food, and some of them described that they derived much pleasure from performing these activities. The informants also emphasized the impact of food habits and experiences that they brought with them from earlier phases in life, from their childhood as well as earlier adulthood. Edfors and Westergren32 reported similar findings. Their study showed that norms and values regarding food culture, traditions, and eating habits were founded early and that they changed only to a limited degree later in life.
Studies have also shown that limited economic resources can be a major barrier to possessing healthy dietary habits, because healthy food is often more expensive than unhealthy food.33,34 For example, the study by Turconi et al34 showed that low-income seniors often had high fat and sugar intake instead of protein-rich food, fruits, and vegetables. They suggest that a major reason is that such unhealthy eating patterns cost less. This was not the case for the participants in the present study, and, generally, older people in Norway have a generous enough economy to be able to sustain a healthy lifestyle. This may be another explanation why the individuals in our study managed to put their knowledge about a healthy diet into healthy and varied dietary habits. All the participants reported that they daily or often consumed fruits and vegetables. Daily consumption of fruits and vegetables is found to be strongly associated with better self-rated health and greater life satisfaction in older people,19 which is partly explained by the beneficial effects of appropriate nutrition for preventing diseases and functional decline.
Orem14 also postulates eight universal prerequisites for maintaining human structure and function. Among these self-care requisites are the abilities to balance the intake of appropriate food and drinks, balance the need for appropriate activity and rest, balance the need for social interaction and solitude, and protect oneself from unintended harm or risk. According to nutritional self-care, all these prerequisites are closely interrelated, which was also revealed in the present study. One illustrative example is that the informants were conscious about the benefits and the necessity of being physically active to maintain their weight, to balance the blood sugar, or to prevent obstipation. Being active is found to be associated with decreased risk for undernutrition among older individuals.2,9,35
Another example to illustrate the interrelationship between the prerequisites described by Orem,14 which was also evident in the study group, is the association between the need for appropriate food and drink and the need to balance social interaction and company. Being with other people was valued as very important when meals were prepared and consumed, and corresponding findings are also confirmed in another study.6 On the other hand, one of the participants, who regularly attended a day center for the elderly, explained that she preferred to go home at mealtime and cook and eat on her own. Her explanation was that this gave her a sense of independence and freedom, and that she valued peace and quiet during meals. In general, studies reporting such findings seem to be sparse. One exception is the study by Dale et al.36 A female informant in that study described how she enjoyed preparing and eating a good meal in her own company. It can therefore be concluded that older people’s preferences can vary, and self-care ability in this context may refer to the ability to adjust individual preferences and habits according to actual needs.
Methodological reflections and conclusion
This study included self-care talks in participants’ homes, and, although the differences in scores before and after the talks were small regarding nutritional risk, they were still present.
A limitation of this study is that the sample consisted of only five participants, and it would have been desirable to have had more people who wanted to participate. Hence, it is impossible and meaningless to generalize the findings. Recruiting older people to research studies may be challenging, and a major problem is that the samples tend to consist of those persons with personal, economic, social, and environmental resources.37,38 This may also be the case in the present study. The participants had initially been screened and found to be at risk for undernutrition.17 The screening results on NUFFE-NO at baseline and 6 months after the visits revealed scores quite close to the former17 results. Actually, for some of the informants, the scores improved in the years between the previous and present studies. These results, in addition to the findings in the self-care talks, indicate that the informants were in possession of many resources that they actively used.
The strength of this study is that respondents who, in a former quantitative survey,17 were found to be at risk for undernutrition were, in the present study, followed up with self-care talks to gain a deeper understanding of their daily life experiences regarding nutrition and food intake. There is a paucity of qualitative studies that focus on nutritional self-care and older people’s own thoughts and experiences on how they can maintain their self-care.
Despite the limited study sample, the findings in our study are valuable because they illustrate older people’s motivations and abilities to adjust and find new ways to cope with nutritional changes. The promising findings also show how important it is to encourage and support the elderly’s self-care resources, and that appropriate information given at the right time can prevent undesirable consequences such as undernutrition.
To enhance the trustworthiness of the findings, accuracy was ensured in all phases of the study. Prior to the home visits, the authors thoroughly discussed the content and the implementation of the self-care talks to ensure consistency. Further, the findings from the data analysis and the presentation of the findings were thoroughly reflected on by both authors and discussed. The authors were, initially, prepared to give advice or support during the self-care talks if needed, or if the participants asked for it. Although giving advice was not particularly relevant, providing support and encouragement when participants talked about appropriate ways they had solved their challenges in relation to nutrition and eating habits was part of the self-care talks. Both researchers were also trained nurses with years of experience working with older people. However, being conscious of not mixing the researcher role and therapist role was focused on and discussed.
Older people living at home are as diverse as other groups living in society. However, this study showed that this group may have sufficient knowledge, willingness, and ability to perform nutritional self-care, even if they live alone and have several chronic illnesses and impaired health. More qualitative studies are needed to gain more knowledge of how older people think and act regarding their nutritional needs. A larger sample is needed, and diversity in the sample should be sought to better reflect the variety of perceptions and experiences in the study group.
Acknowledgments
This study was financed by the Norwegian Research Council (project number 18785) and the Faculty of Health and Sport Sciences, University of Agder, Norway.
Disclosure
The authors report no conflicts of interest in this work.
References
Elia M, Zellipour L, Stratton RJ. To screen or not to screen for adult malnutrition? Clin Nutr. 2005;24(6):867–884. | |
Söderhamn U, Dale B, Sundsli K, Söderhamn O. Nutritional screening of older home-dwelling Norwegians: a comparison between two instruments. Clin Interv Aging. 2012;7:383–391. | |
Velho S, Marques-Vidal P, Baptista F, Camilo ME. Dietary intake adequacy and cognitive function in free-living active elderly: a cross-sectional and short-term prospective study. Clin Nutr. 2008;27(1):77–86. | |
Alam I, Larbi A, Pawelec G, Paracha PI. Relationship between anthropometric variables and nutrient intake in apparently healthy male elderly individuals: a study from Pakistan. Nutr J. 2011;10:111. | |
Kwong EW, Kwan AY. Participation in health-promoting behavior: influences on community-dwelling older Chinese people. J Adv Nur. 2007;57(5):522–534. | |
Tomstad ST, Söderhamn U, Espnes GA, Söderhamn O. Lived experiences of self-care among older, home-dwelling individuals identified to be at risk of undernutrition. J Multidiscip Healthc. 2012;5:319–327. | |
Johansson Y, Bachrach-Lindström M, Carstensen J, Ek AC. Malnutrition in a home-living older population: prevalence, incidence and risk factors. A prospective study. J Clin Nurs. 2009;18(9):1354–1364. | |
Söderhamn U, Christensson L, Idvall E, Johansson AK, Bachrach-Lindström M. Factors associated with nutritional risk in 75-year-old community living people. Int J Older People Nurs. 2012;7(1):3–10. | |
Tomstad ST, Söderhamn U, Espnes GA, Söderhamn O. Living alone, receiving help, helplessness, and inactivity are strongly related to risk of undernutrition among older home-dwelling people. Int J Gen Med. 2012;5:231–240. | |
Gustafsson K, Sidenvall B. Food-related health perceptions and food habits among older women. J Adv Nurs. 2002;39(2):164–173. | |
Johnson CS. Psychosocial correlates of nutritional risk in older adults. Can J Diet Pract Res. 2005;66(2):95–97. | |
Sobye LW, Schroll M, Finne Soveri H, et al. Unintended weight loss in the elderly living at home: the aged in Home Care Project (AdHOC). J Nutr Health Aging. 2008;12(1):10–16. | |
Ahmed T, Haboubi N. Assessment and management of nutrition in older people and its importance to health. Clin Interv Aging. 2010;5: 207–216. | |
Orem DE. Nursing: Concepts of Practice. 6th ed. St Louis, MO: Mosby; 2001. | |
Lorensen M. Psychometric properties of self-care management and life-quality amongst elderly. Clin Eff Nurs. 1998;2:78–85. | |
Pearson JM, Schlettwein-Gsell D, Brzozowska A, van Staveren WA, Bjørnsbo K. Life style characteristics associated with nutritional risk in elderly subjects aged 80–85 years. J Nutr Health Aging. 2001;5(4):278–283. | |
Dale B, Söderhamn U, Söderhamn O. Self-care ability among home-dwelling older people in rural areas in southern Norway. Scand J Caring Sci. 2012;26(1):113–122. | |
Sundsli K, Söderhamn U, Espnes GA, Söderhamn O. Ability for self-care in urban living older people in southern Norway. J Multidiscip Healthc. 2012;5:85–95. | |
Lengyel CO, Tate RB, Obirek Blatz AK. The relationships between food group consumption, self-rated health, and life satisfaction of community-dwelling canadian older men: the manitoba follow-up study. J Nutr Elder. 2009;28:158–173. | |
Wunderlich S, Bai Y, Piemonte J. Nutrition risk factors among home delivered and congregate meal participants: need for enhancement of nutrition education and counseling among home delivered meal participants. J Nutr Health Aging. 2011;15(9):768–773. | |
Ülger Z, Halil M, Klan I, et al. Comprehensive assessment of malnutrition risk and related factors in a large group of community-dwelling older adults. Clin Nutr. 2010;29(4):507–511. | |
Söderhamn U, Flateland S, Jessen L, Söderhamn O. Norwegian version of the Nutritional Form for the Elderly: sufficient psychometric properties for performing institutional screening of elderly patients. Nutr Res. 2009;29(11):761–767. | |
Söderhamn U, Söderhamn O. Developing and testing the Nutritional Form For the Elderly. Int J Nurs Pract. 2001;7(5):336–341. | |
Söderhamn U, Söderhamn O. Reliability and validity of the nutritional form for the elderly (NUFFE). J Adv Nurs. 2002;37:28–34. | |
Söderhamn U, Dale B, Sundsli K, Tomstad S, Söderhamn O. Psychometric testing of the Norwegian version of the Nutritional Form For the Elderly among older home-dwelling people. J Multidisc Healthc. 2012;5:121–128. | |
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–1288. | |
WMA Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects [webpage on the Internet]. Fortaleza: World Medical Association; 2008. Available from: http://www.wma.net/en/30publications/10policies/b3/index.html. Accessed May 27, 2014. | |
Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 7th ed. Oxford: Oxford University Press; 2013. | |
Chauhan K, Mahendra A, Mehta P. Study on knowledge and practices of elderly female self care givers: capacity building through nutrition health education (NHE) Intervention. Helpage India–Research & Development Journal. 2009;15(3):7–11. | |
Iizaka S, Tadaka E, Sanada H. Comprehensive assessment of nutritional status and associated factors in the healthy, community-dwelling elderly. Geriatr Gerontol Int. 2008;8:24–31. | |
Dean M, Grunert KG, Raats MM, Nielsen NA, Lumbers M; Food in Later Life Team. The impact of personal resources and their goal relevance on satisfaction with food-related life among the elderly. Appetite. 2008;50:308–315. | |
Edfors E, Westergren A. Home-living elderly people’s view on food and meals. J Aging Res. 2012;761291. | |
Darmon N, Briend A, Drewnowski A. Energy-dense diets are associated with lower diet costs: a community study of French adults. Public Health Nutr. 2004;7:21–27. | |
Turconi G, Rossi M, Roggi C, Maccarini L. Nutritional status, dietary habits, nutritional knowledge and self-care assessment in a group of older adults attending community centres in Pavia, Northern Italy. J Hum Nutr Diet. 2013;26:48–55. | |
Söderhamn U, Bachrach-Lindström M, Ek AC. Nutritional screening and perceived health in a group of geriatric rehabilitation patients. J Clin Nurs. 2007;16:1997–2006. | |
Dale B, Söderhamn U, Söderhamn O. Life situation and identity among single older home-living people: a phenomenological-hermeneutic study. Int J Qual Stud Health Well-being. 2012;7:18456. | |
Buckwalter KC. Recruitment of older adults: an ongoing challenge. Res Gerontol Nurs. 2009;2:265–266. | |
Jacelon CS. Older adults’ participation in research. Nurse Res. 2007;14: 64–73. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.