")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
Nurses’ Experiences with Disclosure of Patient Safety Incidents: A Qualitative Study
Received 11 March 2020
Accepted for publication 2 May 2020
Published 21 May 2020 Volume 2020:13 Pages 453—464
DOI https://doi.org/10.2147/RMHP.S253399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Yujeong Kim,1 Haeyoung Lee2
1College of Nursing, Research Institute of Nursing Science, Kyungpook National University, Daegu 41944, Republic of Korea; 2Red Cross College of Nursing, Chung-Ang University, Seoul 06974, Republic of Korea
Correspondence: Haeyoung Lee 84 Heukseok-ro, Dongjak-gu, Seoul 06974, Republic of Korea
Tel +82-10-3117-6381
Email [email protected]
Background: Patient safety incidents trigger conflict between healthcare providers and patients. Patients and families want to hear detailed explanations and apologies from medical staff, but nurses may face difficulties with disclosure of patient safety incidents.
Purpose: To identify nurses’ experiences with disclosure of patient safety incidents.
Methods: Data were collected through in-depth interviews with nine clinical and five head nurses and were analyzed using Colaizzi’s phenomenological method.
Findings: After formulating 18 themes representing nurses’ experiences with disclosure of patient safety incidents, we clustered them into four theme clusters: “mixed responses from patients and families,” “caught in a swirl of negative emotions,” “facing the reality that hinders disclosure,” and “waiting for a breakthrough that would enable disclosure”.
Conclusion: Policies, systems, and culture that help both patients and healthcare professionals should be developed.
Keywords: disclosure, medical errors, nurses, patient safety, qualitative research
Introduction
The US Institute of Medicine’s (IOM, 2000) report “To Err is Human” estimated that 44,000–98,000 Americans die every year from preventable accidents in hospitals. One out of ten inpatients suffer an unintentional injury, of which 50% are reported to have been preventable.1 Unintentional patient safety incidents [PSIs] trigger tension and conflict between healthcare providers and patients.2 Patients and families wish to receive a detailed explanation, such as the details of the incident and subsequent progress, along with a sincere apology from the hospital.3 However, as some patients demand compensation for the harm and pain caused by a PSI and punishment of the healthcare professionals involved,4 healthcare institutions and professionals have grave concerns with and feel burdened by the risks related to the disclosure of PSI [DPSI].5
DPSI refers to hospitals’ or healthcare professionals’ actions of expressing regret about the incident and providing an explanation about the incident, along with an analysis of it and measures to prevent similar cases, to patients and their caregivers, regardless of accepting the responsibility and fault.6 Apologies are a particularly important aspect in resolving adverse events, and an honest explanation and apology about an adverse event by a healthcare professional help maintain a trust relationship with patients following the event.7 The effects of DPSI are known to reduce the number of medical malpractice disputes, litigation costs, and compensation payouts,8,9 and is also a major factor that lowers healthcare professionals’ guilt and turnover.2
Despite evidence supporting that DPSI lowers the number of medical dispute cases and relevant cost, reduces patients’ intent of punishing healthcare professionals, strengthens relationships with patients, and promotes ethical patient-centered medicine, healthcare professionals are still hesitant to practice DPSI. Prior studies reported that only about 30% of medical errors are disclosed.10,11 Although healthcare professionals generally agree on the need to report and disclose PSIs to prevent them and promote patient safety, they are reported to be reluctant to do so due to reasons such as punitive organizational culture, legal responsibility, and destruction of their trust relationship with patients.12 In particular, nurses experience various PSIs, such as medication errors, falls, and pressure ulcers, so they are more likely to be exposed to situations in which DPSI is required.13 In addition, among healthcare professionals, nurses have the closest relationship with patients, so they worry about how to explain the PSIs to the patient or caregiver.14 Due to the nature of medicine, it is difficult for non-medical personnel, such as patients and families, to confirm and prove medical errors unless healthcare professionals report them and provide explanations. Failure to appropriately disclose PSIs deprives healthcare professionals of their opportunity for improvement from their experience with error and hinders the prevention of similar PSIs in the future. Therefore, surveying and understanding the fundamentals of nurses’ experiences with DPSI is crucial to help nurses to honestly disclose PSIs while preserving their trust relationship with patients and caregivers.
Most prior studies on DPSI examined the experiences of physicians,15–17 with only a handful of studies surveying nurses’ experiences. In one study that investigated American nurses’ experiences with DPSI, nurses from institutions with PSI disclosure policies were enrolled, and the results showed that, except in serious cases, nurses are the ones to disclose nursing PSIs.18 In a study of Swiss nurses, most were aware of the need to disclose PSIs but found that relevant policies were lacking in healthcare institutions.19 However, Korea has not enacted an apology act, which typically protects the expression of regret by the healthcare provider but not the accompanying information related to causality/fault regarding the PSIs.20 In addition, there are not yet guidelines for DPSI in Korea, so whether or not to disclose depends on the judgement of nurses. It is important to establish guidelines for DPSI by identifying the factors that hinder and support DPSI by healthcare professionals. There may be structural and cultural differences in nurses’ experiences because nursing staffing structures and PSI-related organizational cultures differ across countries. Therefore, studies need to present foundational data to positively and successfully introduce and establish DPSI in the healthcare culture.
In this context, we aim to gain a broad understanding of the meanings and essence of Korean nurses’ experiences with DPSI through a phenomenological method.
Methods
Study Design
This study is a qualitative study utilizing the phenomenological method to comprehensively understand and explore nurses’ experiences with DPSI. The phenomenological method aims to understand the meanings and fundamental structures of human experiences and focuses on identifying the common properties shared by an entire study population as opposed to examining individual characteristics. Moreover, it enables an undistorted analysis of participants’ language. Thus, we determined that it is an appropriate methodology for understanding nurses’ experiences with DPSI.
Selection of Study Participants and Investigator Preparations
Nurses working in a general or tertiary hospital who had experienced DPSI within the past two years and were capable of adequately expressing their experiences were recruited. New nurses currently undergoing orientation were excluded. The hospitals the nurses were recruited from were not the same as the hospitals employing the researchers. Nurses from one general hospital were recommended, and after informing them of the purpose and method of the study over the phone, we allowed them to volunteer as participants. Snowball sampling was used, wherein participants who completed an interview were asked to recommend other participants. The reason for applying snowball sampling in this study was to find participants willing to discuss their experience with DPSI frankly and sufficiently explain their DPSI situation.
For qualitative studies, the recommended sample size is 10, which is an adequate number even after deleting other perspectives during analysis.21 In this study, we conducted the interviews until reaching theoretical saturation, where no novel fundamental meanings are discovered from participants’ statements, and a total of 14 participants were enrolled. No one refused or dropped out.
As researchers are the primary instrument in qualitative studies, we underwent courses and attended special lectures on qualitative research in graduate school to ensure that the study was reliable and to ensure accurate examination of outcomes. The researchers have conducted qualitative studies in the past as well. We all worked in a care quality management unit in which PSIs were analyzed and quality improvement activities were performed for five years or longer. Through our work, we became interested in nurses’ experiences with PSIs and accumulated empirical experience of understanding healthcare professionals, patients, and caregivers through interviews during the process of analyzing the causes of incidents and administering interventions. Furthermore, to prevent our experiences with DPSI from influencing the interviews or outcome analysis and establish a neutral stance, we tried to eliminate our own opinions or bias while reflecting primarily on the participants’ experiences and opinions.
Data Collection
Data were collected through individual in-depth interviews with each participant from April 18, 2018 to May 30, 2018. The interviews were conducted in a comfortable environment near the participants’ hospitals or homes. Non-participants were not present alongside the participants and researchers. One to two rounds of interviews were conducted for each participant, with each interview lasting for 50 minutes to two hours. The interview questions were asked by two female nursing PhD professors who had been in charge of PSIs at a healthcare institution and thus had ample experience interviewing healthcare professionals. Before the interviews, they explained the study’s purpose and procedure and defined DPSI.
The major questions for the in-depth interviews were: “What was your experience like when you communicated with patients or caregivers about a patient safety incident?,” “Is disclosure of patient safety incidents necessary?,” “What do you think is important in the disclosure of a patient safety incident?,” “What are the challenges of disclosure of a patient safety incident?,” and “Which areas should be improved for healthcare professionals to disclose patient safety incidents?” We asked the questions in this order according to the flow of conversation with the participant so that the participants continued to talk throughout the interview. The interviews were voice-recorded upon obtaining consent from the participants and were transcribed verbatim by the researcher immediately afterward.
Data Analysis
The collected data were analyzed per the process suggested by Colaizzi.22 We repeatedly read the interview transcriptions (verbatim) to comprehensively understand and develop insight into the participants’ experiences. Next, we marked significant words and sentences directly related to the phenomenon to extract meaningful statements and described the meanings as general statements in our own words. Then, similar meanings were clustered into themes, and similar themes were grouped into theme clusters. We continuously checked them against the transcriptions to ensure that the identified theme clusters were consistent with the meanings expressed by the participants. In the final stage, we wrote comprehensive statements that captured the essential structure of the phenomenon under study.
Rigor
To maintain the rigor of qualitative research, we assessed this study per the assessment criteria for scientific studies by Guba and Lincoln.23 First, in terms of credibility, we voice-recorded the interviews and transcribed the contents verbatim based on which concepts were extracted. We conducted interviews and analyses with a neutral attitude to eliminate the influence of researchers’ bias and presuppositions. Second, in terms of fittingness, we checked our descriptions and analyses with three participants to ensure that they were in line with their expressed experiences. Additionally, we consulted with two nurses and one head nurse, who were not among our participants but had with experience with DPSI, to confirm that our results were meaningful. We also received feedback on whether the results drawn from the collected data were appropriate from one nursing professor who had conducted several qualitative studies. Third, to ensure auditability, we presented a detailed description of the process of analysis in the methods section and directly cited participants’ statements in the results section so that readers can verify our analyses. Fourth, confirmability was established by complying with the credibility, fittingness, and auditability criteria.
Ethics Approval and Consent to Participate
This study was approved by Institutional Review Board of the Hoseo University in Korea (IRB No. 1041234–170822-HR-061-01). Ethical issues regarding plagiarism, informed consent, misconduct, data fabrication and/or falsification, double publication and/or submission, and redundancy have been observed completely by the author. Only those who voluntarily agreed to participate could fill out the written informed consent. The participation agreement included a statement about protecting the participants’ anonymity and confidentiality and explained that participating in this research would have no impact on their work.
Findings
Participants were recruited from nurses working in six general or tertiary hospitals in South Korea, and 14 participants were enrolled. There were 13 women and one man, with a mean age of 35.86 years and a mean clinical career of 12.55 years. Ten were college graduates, while four had a master’s degree. Six were married, and there were five head nurses and nine staff nurses. Eight nurses worked inwards, five in an intensive care unit, and one in the operating room (Table 1).
 |
Table 1 Participants (N=14) |
We analyzed the interview data using the Colaizzi22 method to understand the essence of nurses’ experiences with DPSI. There were 659 key statements, which were clustered into 129 meanings. Based on these, 18 themes that represented nurses’ experiences with DPSI were formulated, which were then clustered into four theme clusters (Table 2).
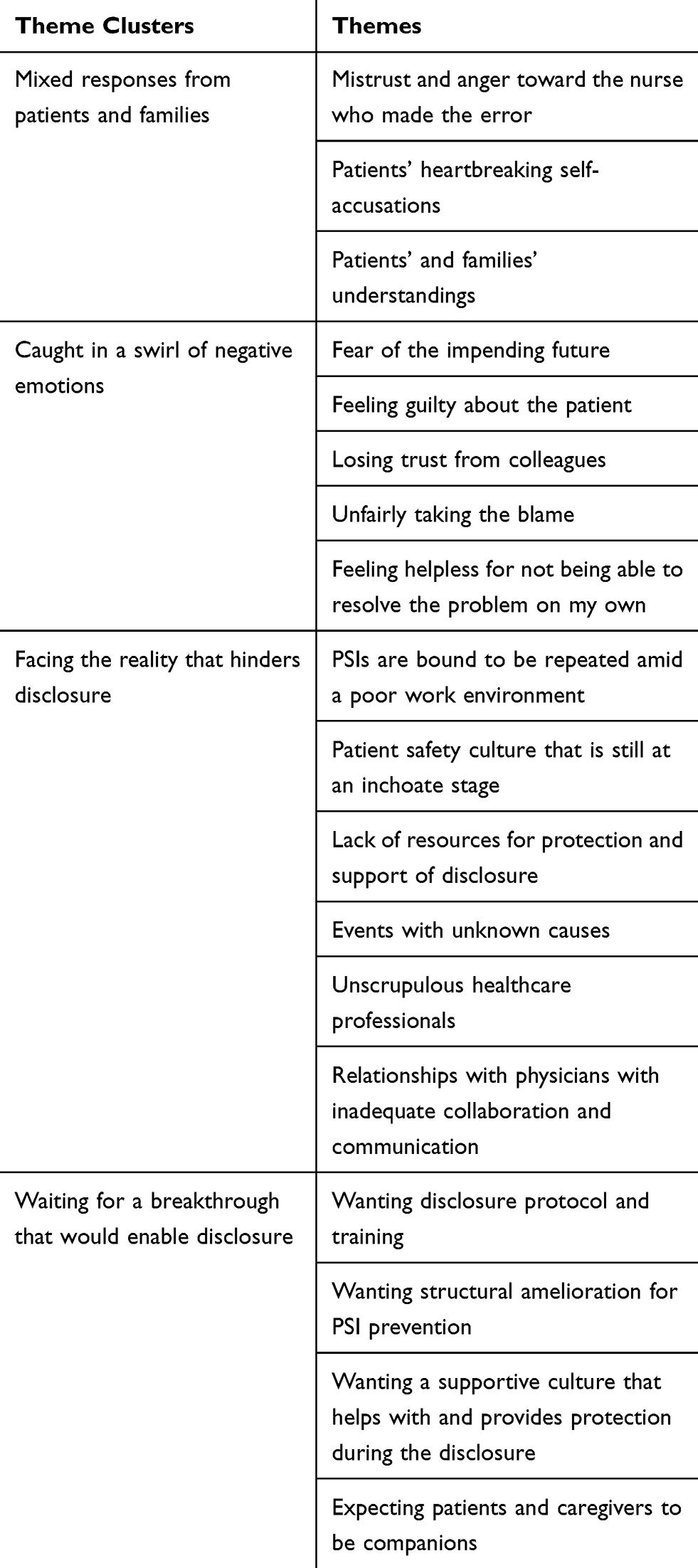 |
Table 2 Nurses’ Experiences with the Disclosure of Patient Safety Incidents |
Mixed Responses from Patients and Families
Mistrust and anger toward the nurse who made the error. The participants gave an explanation and apology to the patients and their families regarding a PSI, but the patients and families violently expressed their anger against them and hold them responsible. Further, nurses also experienced that patients and families mistrusted them for making an error and monitored their behaviors to keep record.
I apologized and said I’m really sorry, but the caregiver got really upset and began to curse at me, demanded to see the CCTV, and said he’ll call the cops. Nurses from previous shifts were also called and we explained to him over and over and kept apologizing. The caregiver was really mad, saying things like wouldn’t this kill the patient and what are you going to do if anything happens to the patient. (Participant 7)
Some patients or caregivers would just raise their voices and make a big deal even if we politely apologized. Young caregivers react more fiercely than patients do. They scream and give nurses hell. They watch every move we make with untrusting eyes, tape-record everything, and even take pictures and videos. (Participant 9)
Patients’ heartbreaking self-accusations. The participants felt sorry as they explained an error regarding PSI to the patients, but sometimes they encountered patients who would say that it was their fault for not being careful. The participants felt even sorrier for patients who consoled them for making an error even when they were sick.
My eyes teared up when I was explaining about a medication error to a patient. The patient told me that it was his drug, so he should’ve been more careful. He would keep console me and say that it’s okay even when he was not in good condition. (Participant 3)
Patients’ and families’ understandings. The participants experienced that patients would accept and understand when the nurses explained about a PSI and expressed regret. Patients asked the nurses to ensure that no more accidents would occur in the future, but they did not persistently challenge the nurses about it or express negative emotions.
The anticancer agent was infused too quickly, but the patient was a DNR and had a good relationship with nurses. I thought that it’s just his character. When I explained to him that there was a medication error, he just said, “Please be careful next time” and that was it. We told him that we will compensate for it, but he refused and thanked us for being honest. Sometimes, we had a better rapport with the patient after the incident. (Participant 1)
Caught in a Swirl of Negative Emotions
Fear of the impending future. The participants experienced a fear of the PSI seriously harming the patient. Furthermore, they felt afraid of the criticism and disciplinary measures that would ensue after the incident.
One of the reasons that we do not want to disclose the incident is the fear of disadvantages, criticism, disciplinary action, and lawsuits. The first question people ask when an incident occurs is “who did this?” The person responsible is first identified, and criticism and disciplinary action follow. That is our greatest fear and concern. You know, because we deal with human lives. (Participant 12)
Feeling guilty about the patient. The participants felt guilty for making a mistake that harmed or might have harmed a patient. Also, they still felt sorry for failing to honestly tell the patient about the incident even after some time since the incident. Nurses who had good relationships with the patient felt more sorry and guilty.
I accidentally administered 1/10 of the prescribed dose of insulin. Thankfully, nothing happened. The head nurse told me that we shouldn’t make a big deal because nothing happened in the ward, so we didn’t do anything. We didn’t go to the patient or caregiver to explain the incident. But I still feel sorry for that. If I had apologized, it would’ve helped me feel less guilty. At the time, I had felt fortunate because nothing happened to the patient, but now I just feel sorry. Nothing happened, so if I had just apologized at the time, it wouldn’t keep bothering me now … (Participant 8)
Losing trust from colleagues. The participants experienced losing trust from their coworkers and being stigmatized as a nurse who had caused a problem as a result of the incident. They were not empathized by fellow healthcare professionals, overheard coworkers talking behind their backs, and felt as if they are not recognized as a colleague. They also felt that fellow nurses were coldhearted for talking about the worst-case scenario despite the intimidated and nervous state of the nurse who made an error.
A new nurse accidentally removed the central line and was frightened to death, but other senior nurses told her, “Hey, you might be reported” when she was already shaking like a dog because she was new … Some nurses don’t consider new nurses as a colleague in those situations. (Participant 6)
Unfairly taking the blame. The participants experienced that as nurses, they are especially the targets of patients’ and families’ criticism and blame regarding PSIs. They feel unfairly blamed by patients and families who especially chastise the nurses even though the incident was not solely due to the nurse’s error. Also, they feel they are unfairly taking the blame for more senior nurses who were also at fault in the incident.
Of course, it is the hospital’s fault. But sometimes, when the healthcare professionals unconditionally take the blame, the caregivers suddenly become the more powerful party and we are the subjugated. They can’t say anything to the doctors, but they blame and project all kinds of feelings on the nurses. I felt so unfairly treated in those situations. (Participant 12)
Feeling helpless for not being able to resolve the problem on my own. The participants lacked knowledge and skills about how to explain the PSI to the patients and caregivers and handle the situation and felt that they cannot do anything on their own. Even in PSIs that did not cause any harm to the patient, nurses experienced that they cannot resolve the problem on their own. Even if nurses explained the situation to patients and caregivers, they wanted a doctor to explain the same as they had more trust in the doctor, which made nurses feel helpless.
I heard about how to deal with customers with complaints during nurse job training. But I have never been trained about how to handle these incidents, so I don’t know what to do. When the caregivers make complaints to me, I just freeze and can’t handle the situation on my own. (Participant 10)
Facing the Reality That Hinders Disclosure
PSIs are bound to be repeated amid a poor work environment. The participants felt that the inadequate nursing staffing compared to the severity of patients’ conditions is the structural culprit for the repeated PSIs. They stated that they sense their limitations when swamped with an overload of work and miss something in an instant in such a hectic environment. They felt that PSIs are bound to be repeated in such an extremely poor and hectic work environment where they cannot adhere to principles and rules.
The environment is so poor. The government, which has been abetting this healthcare system, is busy blaming the healthcare professionals and pulling their feet out when something big happens. There are just too many situations where nurses can’t work in their right minds …. Minor incidents happen so many times every day. How can we possibly tell patients all of this? (Participant 9)
You know, even if you try to focus, an error happens in an instant. It is inevitable. You can’t check 5 rights, not because you don’t know them but because something happened at that moment that hindered you from doing so. This will sound like an excuse for patients. With inadequate staffing, nurses are always pressed for time and these incidents cannot be prevented. Disclosure is not the ultimate solution. (Participant 14)
A patient safety culture that is still at an inchoate stage. The participants felt that they should try to hide a PSI and not report it due to criticism of patient safety culture. Although they thought that reporting the incident and explaining to the patient were the right things to do, their manager criticized them for making a big deal out of it and tarnishing the team’s reputation. The manager publicly announced to give the nurse a disadvantage and rejected any opinions for improvement. The participants experienced that the patient safety culture promoted in campaigns and patient safety education is yet to be established.
The nursing director chastised me and blamed me, saying, “Why did you apologize first? … If you hadn’t apologized, we could’ve just let it pass like it was nothing, and if we did, this wouldn’t have happened. We could’ve not made a big deal out of it.” In patient safety education, I learned to quickly detect errors and correct them. In the hospital, they tell you to shut your mouth if an accident occurs instead of correcting it, and they’re busy covering it up. They say that these accidents happened out of bad luck. I quit my job after the incident. (Participant 11)
There was this one drug that would make kids cry because it’s too stimulating when shot through IV. When I researched the drug, the manual says to mix the drug in the fluid to dilute it when giving it to patients. I printed out the information and handed it over to the head nurse, and it went straight into her drawer. It’s way more convenient for nurses to work if we just shoot it through IV. I didn’t make any suggestions since then. (Participant 14)
Lack of resources for protection and support of disclosure. The participants felt that there were no protective systems to enable DPSI. They perceived that healthcare professionals may not be protected regarding numerous PSIs that would occur and could be hurt from the disclosure of PSIs. They do not know how to handle PSIs and feel that there is no one available to provide professional help regarding disclosure. They experienced that although head nurses tried to resolve the issues, they failed to properly handle the situations due to a lack of professional knowledge and skills regarding disclosures.
I’m afraid that the hospital would bring the disclosure policies in foreign countries to Korea without adjustment. They give healthcare professionals no protection after disclosure. If we cannot disclose because of this, people decry that we have no ethics. The healthcare scene is a minefield, but even when problems blow up, hospitals don’t cover for us, the country doesn’t cover for us … only healthcare professionals are brutally sacrificed. (Participant 11)
Events with unknown causes. The participants experienced that they could not disclose an event because they did not know whether the nurse was at fault. They believed that pinpointing the exact cause of an incident is difficult and nurses are not at fault. Further, patients and families perceive that nurses are at fault when nurses disclose an incident without clearly knowing the cause, so they had to remain silent in such cases.
The patient underwent a second surgery due to a problem with their aorta, but the aorta ruptured during suction and the patient had to undergo an emergency operation. The caregivers blamed everything on the nurse. In these situations, we’re not sure if we should apologize or not because we don’t know whether it is our fault or not. (Participant 2)
Unscrupulous healthcare professionals. The participants witnessed nurses who reacted casually to their errors as if they are nothing serious or avoid taking responsibility and felt that these nurses lacked ethics. They also felt immoral for thinking that disclosure seems unnecessary because it only makes the patient anxious and is not helpful for their work. They sensed that they were unscrupulous in situations in which the patient passed away from an accident and the entire case was determined to be an exacerbation of conditions and concluded without giving the family any details or consolation.
A few days ago, one nurse gave her patient a double dose of a drug. But she claimed that it wasn’t her fault. She argued that the nurse on the previous shift mixed the drug wrong and so it wasn’t her fault. I asked her if she confirmed the drug dosage during handover, but she just said that she had to give the drug as prepared by the other nurse. Some nurses blame others for their errors and don’t even know that they did something wrong. (Participant 1)
Relationships with physicians with inadequate collaboration and communication. The participants experienced conflicts with physicians regarding the person at fault in a PSI. They felt that they have little understanding of each other’s perspectives and that information about the details of the event and subsequent treatment plan for the patient is not shared with nurses. While patients and families complain and express their anger about the event to the nurse, nurses could not tell them anything or give them consolation because they did not know anything.
There was an older patient who persistently had abnormally high cardiac enzyme levels, and I forgot to notify the physician on duty about the follow-up test done over the weekend. The patient went to hemodialysis on Monday, and his doctor came to work on that morning and found out that the patient had high cardiac enzyme levels. The doctor said that he wouldn’t have ordered hemodialysis if he knew the test results. The patient underwent CPR that night and was transferred to the ICU, but later passed away. His state was already bad and that the nurse’s failure to notify was not the direct cause of the incident. But the doctor was busy blaming the nurse. I cannot forget that “evening shift nurse *** didn’t notify” was written on the progress record. (Participant 8)
Waiting for a Breakthrough That Would Enable Disclosure
Wanting disclosure protocol and training. The participants wanted a disclosure protocol, education, and training. They wanted to be educated and trained to be able to give heartfelt disclosures to patients and families. They hoped that performing disclosure according to a set protocol would be helpful for patients and would be safe for nurses as well.
We need experience and a role model for disclosing a PSI to patients. If there are senior nurses or head nurses who are good at them, we can learn a lot from them. But it’s really difficult for head nurses, too. They’re not educated with that or anything. Having sincerity is, of course, a must, but you also need skills to apologize and resolve the situation while understanding how patients and caregivers feel. New nurses just stand there and cry in front of patients. (Participant 1)
Wanting structural amelioration for PSI prevention. The participants felt that adequate staffing and system improvements to prevent PSIs are needed before apologizing to patients for accidents. They felt that the priorities are developing practice guidelines, recruiting more nursing staff to prevent PSIs, and establishing a structural environment that enables nurses to adequately care for patients and explain situations to them.
There are policies related to patient safety and the hospital tells us to comply with them, but the gap between the ideal and reality is too big. Can we do all these … Maybe we can but can small hospitals do this? … Is this the answer … ? They stepped up everything and told us to just follow them, but it’s practically impossible. I think before DPSI, practical measures and government support that protect patients from accidents are needed even more. (Participant 2)
To run DPSI in Korea, I think it’s important to have the proper healthcare system and provide support before discussing safety culture or educating healthcare professionals. There are way fewer nurses for all the work we do. I even think that nurses are lucky not to make errors in such situations. (Participant 9)
Wanting a supportive culture that helps with and provides protection during disclosure. The participants felt the need for a supportive culture that enables them to disclose their errors to patients and families and report them without fear. They desperately wanted managers and a positive patient safety culture that would protect, not criticize, them. They needed help from experts who can stand by them through the difficult process of disclosure as well as programs that promote recovery of nurses who have been hurt by accidents.
We need to settle a patient safety culture that gives nurses confidence that they would not be held responsible and be punished for the incident. Nurses must be able to trust that the purpose is to improve these problems for the better and not to criticize individual nurses. (Participant 4)
One of the greatest complaints that nurses have is that the head nurse offers absolutely no protection at all because when a PSI occurs, the head nurse is not there. She’s not there when patients complain, and although we hope that the head nurse will do something in those situations, she’s just gone and not there. I’m not saying that the head nurse should take the fall, but I think she should protect the nurses to some degree. (Participant 12)
Expecting patients and caregivers to be companions. The participants hoped that patients and families might develop an increased awareness of DPSI. They wanted patients and families to make constructive suggestions for preventing accidents to healthcare professionals and rationally resolve the incident together. They hoped that patients would be more actively involved with and understand their treatment so that they could become the final line of defense for patient safety.
If the patients are well aware of their treatment process, healthcare professionals would be more careful. I think these unfair things happen to them because of the large gap in knowledge. Korean hospitals completely block out patients and caregivers in treatment and just push forward with healthcare professionals’ plans. I think patients need to be well aware of the drugs or treatments they’re going through to protect themselves. (Participant 14)
After the incident, I thanked the child’s caregiver for understanding and apologized and told him not to hesitate to ask us when he has doubts about the drugs that we give the patient. But doing that does filter things. I think educating patients and caregivers to sufficiently know about their treatment and actively participate in it is important, especially for pediatric patients. (Participant 6)
Discussion and Recommendations
In this study, we explored nurses’ experiences with DPSI, and four theme clusters emerged: “Mixed responses from patients and families,” “Caught in a swirl of negative emotions,” “Facing the reality that hinders disclosure,” and “Waiting for a breakthrough that would enable disclosure.”
In the first theme cluster, the participants experienced “mixed responses from patients and families” after disclosing a PSI. While some patients and families expressed anger and mistrust in the nurse who made an error and held her responsible for it, some patients demonstrated an understanding attitude toward the nurse, accepted the current situation, or even blame themselves for playing a part in the incident. Negative reactions, such as mistrust and anger, by patients following an explanation about a PSI are similar to the findings of another study, where these reactions were attributed to patients’ loss of trust in healthcare professionals as a result of their attitude changes.24 Kim, Lee, Choi, and Sohn25 reported that 95% of patients involved in a medical malpractice case suffer from post-traumatic stress disorder. Also, inadequate explanations given by healthcare professionals and their failure to offer emotional consolation exacerbate patients’ psychological shock following the incident.26 Multiple studies have found that patients can understand the situation better, accept it, and develop a greater trust in healthcare professionals when these healthcare professionals make a full apology and acknowledge their responsibility.7,27 As DPSI is directly related to patients’ right to know, it is necessary to inform patients of the situation affecting them. The Medical Error Disclosure Guideline by the Canadian Patient Safety Institute28 recommends healthcare professionals to meet with patients, provide emotional and practical support for them, express regret, and accept their questions. To implement DPSI, legal protection, such as an apology law that excludes the expression of regret from the evidence of liability for compensation, is required. Based on such systems, hospitals should promote patient safety and improve relations with patients through open conversation and transparent disclosure of information with patients.
In the second theme cluster, the participants experienced being “caught in a swirl of negative emotions.” They experienced a fear of criticism, disciplinary action, lawsuits, and worsening of the patient’s condition, feeling guilty about patients, and diminished trust from fellow healthcare professionals. This is similar to another study’s findings that immediately after PSI, nurses are afraid that a patient’s conditions will worsen and feel guilty for their carelessness, which may cause harm to patients.29 Nurses were reported to develop greater fear, anxiety, frustration, and depression with greater harm to a patient as a result of the PSI.30 The National Quality Forum31 stressed the need for support and protection of healthcare professionals, who become a second victim after committing a medical error. The participants also felt powerless as nurses who cannot independently provide explanations for an incident contrary to physicians, and they also felt unfairly treated when the responsibility was shifted to them. These results are similar to previous findings that nurses undergo potentially more problematic experiences following medical errors compared to physicians and pharmacists.32 Nurse managers must pay close attention to the signs of suffering among nurse who experienced a PSI, and hospitals should provide a support system for recovery. Scott et al33 suggested that rapid response teams should be instituted for second victims and that they should be given a referral for professional counseling. The US and Australia implemented an employee assistance program to minimize employees’ emotional and occupational damage following a PSI.34 Some healthcare institutes in Korea provide continuous counseling and interventions for the psychological and emotional injury caused by a PSI among healthcare professionals through mental health clinics.
In the third and fourth theme clusters, the participants “faced the reality that hinders disclosure” and “waited for a breakthrough that would enable disclosure.” The participants experienced healthcare professionals’ unscrupulous attitudes regarding DPSI. Myung35 stated that the most common dilemma healthcare professionals experience when a PSI occurs is whether to disclose the incident or remain silent. Although abiding by one’s conscience and code of ethics is the most important for patient safety, increasing awareness and enforcing patient safety would be difficult without sufficient resources, education, and a positive environment.13,36 In this study, the participants perceived the current Korean environment to be hindering DPSI due to the poor work environment, negative patient safety culture, lack of protection and supporting resources for disclosure, and lack of cooperation among healthcare professionals. In particular, in this study, nurses wanted collaboration and communication with physicians. It was reported that nurses found it difficult to ask for help from physicians when communicating about a PSI that caused severe harm to the patient, so when individual nurses are held responsible for DPSI, the chance of a timely DPSI is reduced.13 In addition, Shannon et al18 reported that nurses were excluded from the disclosure plan and process, which was reported as a problem when providing patient care. In other words, nurses do not know what to say in response to the patient’s questions about a care plan following a PSI, and as a result, inaccurate or unsafe information may be provided to the patient. Further study of DPSI results is needed of situations in which nurses are involved in the disclosure plan and process, and detailed DPSI guidelines as a team approach are necessary.
The participants hoped to have a disclosure protocol and training to make a breakthrough in the current poor environment and desired structural improvement for PSI prevention and a supportive environment that helps them engage in disclosure and protects them from the consequences of disclosure. These results are similar to previous findings that healthcare professionals lack communication skills due to a lack of official education or training is an obstacle to disclosure.2 Korea newly added an item about disclosure of sentinel events to patients and caregivers in the accreditation criteria for acute care hospitals.37 However, a national guideline is still lacking, and a disclosure protocol appropriate to the Korean environment needs to be established. Foreign countries educate healthcare professionals with disclosure through lectures, video case-based studies, and simulations,35 and Korea administers disclosure education as a part of its education for new patient safety personnel in some healthcare institutes. The effects of disclosure education programs have been confirmed and reported in foreign countries, and additional studies are needed to examine whether similar effects are found in the Korean medical culture.
In addition to education for healthcare professionals, the participants also pointed to the need for experts or an exclusive unit dedicated to helping healthcare professionals who have little experience or skills with DPSI. Some Korean hospitals hire risk managers, independent from patient safety personnel, but professional education and training related to medical error disclosure for risk managers are lacking. According to Gallagher,15 risk managers perceive their roles to follow-up with patients and families concerning error disclosure, be involved in the compensation process, and provide timely coaching and education for healthcare professionals. Governmental and hospital support are needed so that risk managers are equipped with the knowledge and competence required to actively intervene in times of crises to facilitate a systematic disclosure between patients and healthcare professionals.
The participants experienced the need for structural improvements, such as hiring additional nursing staff, to prevent PSIs in the first place before having to disclose PSIs. Several studies have reported the correlation between nursing staffing and patient safety.38–40 Korea has a serious nursing shortage problem, where the number of nurses on a per capita basis in Korea is extremely low: 4.6 nurses per 1000 population, compared to the OECD average of 9.3 per 1000 population.41 Therefore, structural improvement by ensuring adequate nursing staffing is a priority to help nurses deliver safe care, which would then contribute to preventing PSIs before having to disclose PSIs.
The participants experienced the dire need to foster a patient safety culture to help, protect, and support them with disclosure. This is similar to other previous findings, which state that medical error disclosure is significantly positively correlated with patient safety culture.42,43 A study on Korean nurses’ perception of DPSI reported that nurses are reluctant to disclose medical errors because it only has benefits for the patients while having negative outcomes for themselves.44 The ultimate goal of DPSI is to promote patient safety, and it is important for all members of a healthcare institution be aware of this and to establish honesty, transparency, and integrity as the culture of healthcare institutions.45 A culture in which patients and healthcare professionals mutually collaborate and voluntarily promote DPSI is needed, as opposed to a culture that forces DPSI onto individual healthcare professionals with an ethical justification and only directs criticism and accusation toward them. Healthcare institutions must cultivate a just and fair safety culture that prioritizes patient safety and resolves problems with systematic approaches.
Finally, the participants experienced “expecting patients and caregivers to be companions.” Patients’ understanding and involvement in their treatment is a core value in patient safety. Although patients have better access to medical information and higher levels of overall medical knowledge than they did in the past, the number of cases in which they define unexpected outcomes as medical errors and violently react or file lawsuits is rising.46 On the other hand, approaches to actively involve patients and their families and encourage them to speak up in their treatment process are lacking.47,48 The US Joint Commission launched a campaign titled “Speak-up Initiatives” in 2002 and has been continuing with the campaign to promote patients to ensure their safety during the process of care.49 Korean healthcare institutes have also launched speak-up campaigns for patients and caregivers as a part of patient safety activity, through which they promote patients’ active participation in their treatment process, such as patient identification and surgical site identification. In addition to providing DPSI education for healthcare professionals, healthcare institutions should promote and provide systematic education so that patients and families serve as the final line of defense in patient safety by speaking up in their treatment.
One limitation of this study is that it examined the experiences of DPSI only from the perspective of nurses; therefore, additional studies should conduct an in-depth analysis of patients’ and families’ experiences to promote patient safety. Further, the interviews, which were conducted in Korean, were translated to English and thus may fail to sufficiently capture the original intentions.
Conclusions
This study conducted an in-depth exploration of nurses’ experiences of DPSI using a phenomenological research method. The results showed that nurses experience mixed responses from patients and families, are caught in a swirl of emotions, face the reality that hinders disclosure, and wait for a breakthrough that would enable disclosure. The significance of this study lies in its presentation of an in-depth understanding of various obstacles that hinder nurses’ disclosure and offered suggestions about the policies as well as structural, cultural, environmental, and social changes needed for nurses to confidently disclose PSIs in clinical practice. Further, the in-depth understanding of nurses’ experiences of DPSI presents evidence supporting policies, systems, and culture that help both patients and healthcare professionals who may become victims of medical errors.
Based on these results, we present the following suggestions. First, in-depth studies on patients’ and families’ experiences with DPSI are needed. Second, studies should develop a DPSI protocol and guidelines appropriate to the Korean environment. Finally, studies should develop and assess the effects of education and training programs for DPSI for healthcare professionals.
Acknowledgments
We would like to thank all of the participants who attended the interview. We would also like to thank the National Research Foundation of Korea (NRF).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Baker GR, Norton PG, Flintoft V, et al. The Canadian adverse events study: the incidence of adverse events among hospital patients in Canada. Can Med Assoc J. 2004;170(11):1678–1686. doi:10.1503/cmaj.1040498
2. O’Connor E, Coates HM, Yardley IE, Wu AW. Disclosure of patient safety incidents: a comprehensive review. Int J Qual Health Care. 2010;22(5):371–379. doi:10.1093/intqhc/mzq042
3. Ock M, Kim HJ, Jo MW, Lee SI. Perceptions of the general public and physicians regarding open disclosure in Korea: a qualitative study. BMC Med Ethics. 2016;17(1):50. doi:10.1186/s12910-016-0134-0
4. Mazor KM, Simon SR, Yood RA, et al. Health plan members’ views about disclosure of medical errors. Ann Intern Med. 2004;140(6):409–418. doi:10.7326/0003-4819-140-6-200403160-00006
5. Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA. 2003;289(8):1001–1007. doi:10.1001/jama.289.8.1001
6. Pace WD, Staton EW. Improving the disclosure of medical incidents: a genuine apology is only the first step in the process. BMJ. 2011;343(jul25 1):d4340. doi:10.1136/bmj.d4340
7. Wu AW, Huang IC, Stokes S, Pronovost PJ. Disclosing medical errors to patients: it’s not what you say, it’s what they hear. J Gen Intern Med. 2009;24(9):1012. doi:10.1007/s11606-009-1044-3
8. Blendon RJ, Schoen C, DesRoches C, Osborn R, Zapert K. Common concerns amid diverse systems: health care experiences in five countries. Health Aff. 2003;22(3):106–121. doi:10.1377/hlthaff.22.3.106
9. Iedema R, Sorensen R, Manias E, et al. Patients’ and family members’ experiences of open disclosure following adverse events. Int J Qual Health Care. 2008;20(6):421–432. doi:10.1093/intqhc/mzn043
10. Blendon RJ, DesRoches CM, Brodie M, et al. Views of practicing physicians and the public on medical errors. N Engl J Med. 2002;347(24):1933–1940. doi:10.1056/NEJMsa022151
11. Lamb RM, Studdert DM, Bohmer RM, Berwick DM, Brennan TA. Hospital disclosure practices: results of a national survey. Health Aff. 2003;22(2):73–83. doi:10.1377/hlthaff.22.2.73
12. Kang MA, Kim JE, An KE, Kim Y, Kim SW. Physicians’ perception of and attitudes towards patient safety culture and medical error reporting. Health Policy Manage. 2005;15(4):110–135. doi:10.4332/KJHPA.2005.15.4.110
13. Choi EY, Pyo J, Ock M, Lee SI. Nurses’ perceptions regarding disclosure of patient safety incidents in Korea: a qualitative study. Asian Nurs Res. 2019;13(3):200–208. doi:10.1016/j.anr.2019.05.002
14. Delbanco T, Bell SK. Guilty, afraid, and alone—struggling with medical error. N Engl J Med. 2007;357(17):1682–1683. doi:10.1056/NEJMp078104
15. Gallagher TH, Waterman AD, Garbutt JM, et al. US and Canadian physicians’ attitudes and experiences regarding disclosing errors to patients. Arch Intern Med. 2006;166(15):1605–1611. doi:10.1001/archinte.166.15.1605
16. Garbutt J, Brownstein DR, Klein EJ, et al. Reporting and disclosing medical errors: pediatricians’ attitudes and behaviors. Arch Pediatr Adolesc Med. 2007;161(2):179–185. doi:10.1001/archpedi.161.2.179
17. Hobgood C, Hevia A, Tamayo-Sarver JH, Weiner B, Riviello R. The influence of the causes and contexts of medical errors on emergency medicine residents’ responses to their errors: an exploration. Acad Med. 2005;80(8):758–764. doi:10.1097/00001888-200508000-00012
18. Shannon SE, Foglia MB, Hardy M, Gallagher TH. Disclosing errors to patients: perspectives of registered nurses. Jt Comm J Qual Saf. 2009;35(1):5–12. doi:10.1016/S1553-7250(09)35002-3
19. McLennan SR, Diebold M, Rich LE, Elger BS. Nurses’ perspectives regarding the disclosure of errors to patients: a qualitative study. Int J Nurs Stud. 2016;54:16–22. doi:10.1016/j.ijnurstu.2014.10.001
20. Phillips-Bute B. Transparency and disclosure of medical errors: it’s the right thing to do, so why the reluctance. Campbell L Rev. 2013;35:333–354.
21. Freeman T. ‘Best practice’ in focus group research: making sense of different views. J Adv Nurs. 2006;56(5):491–497. doi:10.1111/j.1365-2648.2006.04043.x
22. Colaizzi PF. Psychological Research as the Phenomenologist Views It. New York, NY: Oxford University Press; 1978.
23. Guba EG, Lincoln YS. Fourth Generation Evaluation. Newbury Park, CA: Sage; 1989.
24. Rhee HS, Lee JH, Rhim KH, Choi MK. The thoughts of patients on medical accidents and disputes in Korea. Korea J Hosp Manage. 2006;11(1):1–30.
25. Kim NY, Lee SR, Choi YE, Sohn YW. Post-traumatic stress disorder (PTSD) in medical accident patients: the interaction effect of clinicians’ explanation and attitude and social support. Korean J Cult Social Issues. 2017;23(2):215–237. doi:10.20406/kjcs.2017.05.23.2.215
26. Vincent CA. Understanding and responding to adverse events. N Engl J Med. 2003;348(11):1051–1056. doi:10.1056/NEJMhpr020760
27. Kaldjian LC, Jones EW, Wu BJ, Forman-Hoffman VL, Levi BH, Rosenthal GE. Disclosing medical errors to patients: attitudes and practices of physicians and trainees. J Gen Intern Med. 2007;22(7):988–996. doi:10.1007/s11606-007-0227-z
28. Canadian Patient Safety Institute. Canadian disclosure guidelines. Being open with patients and families; 2011. Accessed from http://www.patientsafetyinstitute.ca/English/toolsResources/disclosure/Documents/CPSI%20Canadian%20Disclosure%20Guidelines.pdf.
29. Kim YJ. Nurses’ experience of inpatients’ falls. J Korean Acad Fundam Nurs. 2017;24(2):106–117. doi:10.7739/jkafn.2017.24.2.106
30. Maiden J, Georges JM, Connelly CD. Moral distress, compassion fatigue, and perceptions about medication errors in certified critical care nurses. Dimens Crit Care Nurs. 2011;30(6):339–345. doi:10.1097/DCC.0b013e31822fab2a
31. National Quality Forum. Safe Practices for Better Healthcare—2010 Update. Washington, DC: National Quality Forum; 2010.
32. Lewis EJ, Baernholdt M, Hamric AB. Nurses’ experience of medical errors: an integrative literature review. J Nurs Care Qual. 2013;28(2):153–161. doi:10.1097/NCQ.0b013e31827e05d1
33. Scott SD, Hirschinger LE, Cox KR, et al. Caring for our own: deploying a systemwide second victim rapid response team. Jt Comm J Qual Saf. 2010;36(5):233–240. doi:10.1016/S1553-7250(10)36038-7
34. Clinical Excellence Commission. Open Disclosure Handbook. Sydney, Australia: Clinical Excellence Commission; 2014.
35. Myung SJ. Medical error disclosure: ‘Sorry’ works and education works! Korean Med Educ Rev. 2019;21(1):13–21. doi:10.17496/kmer.2019.21.1.13
36. Ock M, Lim SY, Jo MW, Lee SI. Frequency, expected effects, obstacles, and facilitators of disclosure of patient safety incidents: a systematic review. J Prev Med Public Health. 2017;50(2):68–82. doi:10.3961/jpmph.16.105
37. Korea Institute for Healthcare Accreditation. Accreditation Standards 3.0. Seoul, South Korea: Department of Health and Human Services; 2018.
38. Cho E, Lee NJ, Kim EY, et al. Nurse staffing level and overtime associated with patient safety, quality of care, and care left undone in hospitals: a cross-sectional study. Int J Nurs Stud. 2016;60:263–271. doi:10.1016/j.ijnurstu.2016.05.009
39. Stone PW, Mooney-Kane C, Larson EL, et al. Nurse working conditions and patient safety outcomes. Med Care. 2007;45(6):571–578. doi:10.1097/MLR.0b013e3180383667
40. Schubert M, Glass TR, Clarke SP, et al. Rationing of nursing care and its relationship to patient outcomes: the Swiss extension of the International Hospital Outcomes Study. Int J Qual Health Care. 2008;20(4):227–237. doi:10.1093/intqhc/mzn017
41. Yoo SJ, Choi KS, Kim HY. A study of improvement plan for workforce standards law system. KHIDI. 2013;27–28.
42. Elwy AR, Bokhour BG, Maguire EM, et al. Improving healthcare systems’ disclosures of large-scale adverse events: a department of veterans affairs leadership, policymaker, research and stakeholder partnership. J Gen Intern Med. 2014;29(S4):895–903. doi:10.1007/s11606-014-3034-3
43. Renkema E, Broekhuis M, Ahaus K. Conditions that influence the impact of malpractice litigation risk on physicians’ behavior regarding patient safety. BMC Health Serv Res. 2014;14(1):38. doi:10.1186/1472-6963-14-38
44. Kim SJ. The Impact of General Hospital Nurses’ Perception of Medical Error Report and Medical Error Disclosure on Their Patient Safety Culture (Unpublished Master’s Thesis). Seoul: Korea University; 2017.
45. Nieva VF, Sorra JS. Safety culture assessment: a tool for improving patient safety in healthcare organization. Qual Saf Health Care. 2013;12(2):17–19.
46. Park JS. A study of major issues in the act (draft) on remedy for damage from medical accident and medical dispute mediation, etc. KJ-HSM. 2010;4(2):107–117.
47. Ginsburg L. ‘Speaking up’ climate: a new domain of culture to measure and explore. BMJ Qual Saf. 2015;24(11):661–663. doi:10.1136/bmjqs-2015-004598
48. Institute of Medicine. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
49. The Joint Commission. Speak up initiatives; 2016. Accessed from: http://www.jointcommission.org/speakup.aspx.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.