")
Back to Journals » Advances in Medical Education and Practice » Volume 6
Nurse educators' perceptions of critical thinking in developing countries: Ghana as a case study
Received 20 May 2015
Accepted for publication 9 July 2015
Published 4 September 2015 Volume 2015:6 Pages 555—560
DOI https://doi.org/10.2147/AMEP.S88942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Christian Makafui Boso,1 Janet J Gross2,3
1School of Nursing and Midwifery, College of Health Science and Allied Sciences, University of Cape Coast, Cape Coast, Ghana; 2Morehead State University, Morehead, KY, USA; 3School of Nursing and Midwifery, University of Cape Coast, Cape Coast, Ghana
Abstract: The ability to critically evaluate information for the purpose of rendering health care is a prerequisite for modern nurses in a complex and ever-changing health care environment. The nurse educators’ perceptions influence the utilization of critical thinking strategies in the classroom. The purpose of this study was to assess nursing faculty’s perceptions of critical thinking. Using a questionnaire 106 nurse educators from two types of nursing educational program self-reported their perceptions. Data were collected from November 2013 to March 2014. Results were presented using frequencies, percentages, and t-test. The findings revealed that majority (95.3%) of nurse educators could not provide definitions that captured both affective and cognitive aspects of critical thinking. However, the majority of nurse educators had positive perceptions of critical thinking. Nurse educators in universities had more positive perceptions of critical thinking than those in the nurses’ training colleges (P=0.007). The results suggested that the current nursing programs are not preparing nurses with the necessary critical thinking skills for the complex health care environment. Professional development programs in critical thinking should be instituted for nurse educators to assist them in developing appropriate teaching strategies to foster students' acquisition of critical thinking skills.
Keywords: nurse educators, critical thinking, perceptions, Ghana, developing countries
Introduction
Critical thinking (CT) is a prerequisite for contemporary nursing in the dynamic health care environment.1 The National League for Nursing recognized CT as a vital skill for practicing nurses.2 Nurses are expected to draw on a holistic nursing knowledge base in consideration of each individual patient’s needs in order to render safe, high-quality nursing care rather than merely relying on tradition. Nurses need to utilize their intellectual ability, and theoretical and experiential knowledge in applying CT in health care situations.3
Globally, some graduates of nursing programs may not be prepared to meet entry-level requirements for making clinical decisions.4 Historically, programs have focused on mastering content instead of relating CT to circumstances.4–6 Nurse educators need to utilize educational strategies that foster the development of CT to address students’ learning needs.7
CT in nursing is defined in a variety of ways. As a result of a Delphi study, Scheffer and Rubenfeld8 defined CT as “habits of mind” and “cognitive skills”. Elements of habits of mind included “confidence, contextual perspective, creativity, flexibility, inquisitiveness, intellectual integrity, intuition, open-mindedness, perseverance, and reflection”.8 The cognitive skill elements were identified as “analyzing, applying standards, discriminating, information seeking, logical reasoning, predicting, and transforming knowledge”.8
In Ghana, it has been identified that CT is not being exhibited by nurses in caring for their patients.9,10 The emphasis of nursing on tasks is partly to blame for the lack of CT skills. Students are still taught to follow the functional model of nursing care which is used in the majority of health care facilities.11 This model perpetuates task-orientation and is a major obstacle to the development of CT skills. Similarly, Wilmot et al12 reported serious deficiencies in nursing education in Ghana that impeded effective learning in the classroom. Some of these deficiencies included inappropriate pedagogical methods in teaching, large class sizes, and absenteeism.12
The Nursing and Midwifery Council of Ghana (NMC)13 has incorporated CT into its recommended curricula. However, the perceptions of nurse educators about CT may impede the attempt to develop CT skills of nursing students in Ghana. Nurse educators’ perceptions influence the utilization of CT strategies in the classroom. The authors are not aware of any published study that assessed the Ghanaian nurse educators’ perception of CT. Therefore, this research sought to identify nurse educators’ perceptions of CT.
Research questions
The following research questions guided the study:
- What are the perceptions of nurse educators about CT?
- Are perceptions of CT significantly different between nurse educators of Nurses’ Training Colleges (NTCs) and public universities?
Research design
This study was conducted using a cross-sectional survey design and data were analyzed using univariate descriptive statistics.
Research setting
Surveys were distributed at eleven publically funded nursing educational institutions from November 2013 to March 2014. Two of the study sites were public universities and nine were NTCs.
Study population and sampling
The target population for this study consisted of nurse educators with a full-time appointment to public nursing schools in Ghana offering general nursing programs. A sample size of 163 through a cluster sampling technique was considered sufficient for this study based on Slovin’s formula.14 A proportionate ratio resulted in 151 nurse educators from NTCs and 12 from universities. Nurse educators were few at the universities; therefore all educators from the universities were included at the expense of those from NTCs. This resulted in a ratio of 20 nurse educators from universities to 143 from NTCs. Proportionate sampling was also used to select participants at various NTCs. In order to eliminate any possible bias, the University in which the researchers were staff was excluded.
Ethical considerations
Ethical approval for the study was received from University of Cape Coast (UCC) Institutional Review Board. All principles of research ethics were applied. Written informed consent was received from all participants before data were collected.
Instrumentation
Data for this study were collected using a self-administered questionnaire composed of five Likert-type scales. The questionnaire included three sections: demographic information; participants’ definition of CT; and perceptions of CT.
Two nursing education experts reviewed the questionnaire to establish face and content validity. A pretest study was conducted at an NTC in Kumasi. The scale of perceptions yielded a Cronbach’s alpha of 0.682, which was adequate for reliability of the instrument. Additionally, the perceptions of CT scale used both positive and negative items in order to eliminate or reduce acquiescent and extreme response biases. However at the analysis stage, the negative statements were reversed (scored opposite to the positive statement) to remove the error of miscoding.
Data collection procedure and analysis
The main data were collected from November 2013 to March 2014. An introductory letter from Department of Nursing, UCC was submitted to the schools included in the study. Lists of educators were obtained, and participants randomly sampled. Hard copies of the surveys were personally delivered and received by the principle investigator. The respondents were requested to return the surveys within a week. No returned survey was rejected. Data entry and statistical analysis were done using Statistical Package for the Social Sciences (SPSS) software, version 16 (SPSS Inc., Chicago, IL, USA). Results were presented using frequencies, percentages, and t-test.
Results
Demographic data
Table 1 demonstrates the background characteristics of the respondents.
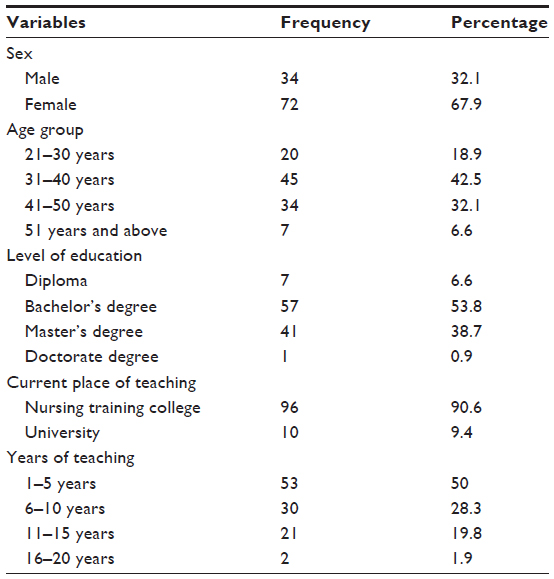 | Table 1 Demographic characteristics of respondents (N=106) |
One hundred and six (65% response rate) responded to the survey. Almost two-thirds of the participants were 40 years or younger, with only 6.6% being above 50 years. More than half (53.8%) of the respondents were bachelor’s degree holders while only one (0.9%) held a doctorate degree at the time of the study. A few (6.6%) of the nurse educators held a diploma as their highest educational achievement.
Definition of critical thinking
Respondents were asked the question, “What is your definition of CT?” The responses included words ranging from 2 to 62. Scheffer and Rubenfeld’s8 attributes of CT were used to assess the respondents’ definitions of CT. The attributes were used without modifications. Using Scheffer and Rubenfeld’s8 definition of CT, the results were categorized as habits of mind (affective) and cognitive skills. Table 2 shows participants’ definition of CT.
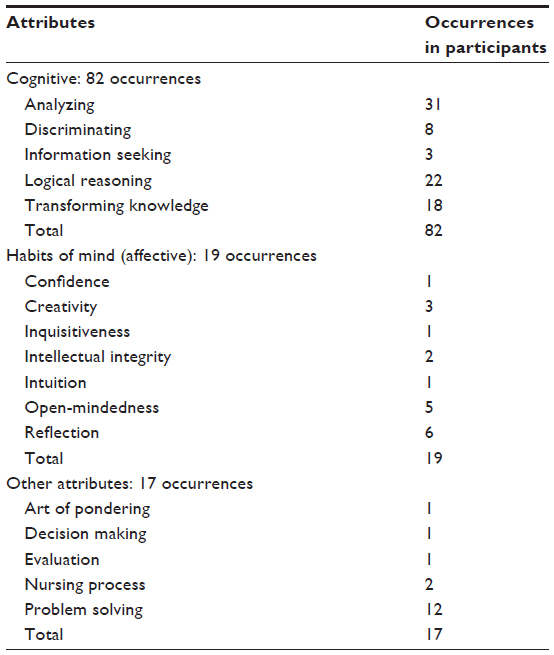 | Table 2 Definition of critical thinking |
None of the educators gave a clear, concise definition that captured all aspects of CT as provided by Scheffer and Rubenfeld.8 Most did provide some characteristics of CT. Only 4.7% (five respondents) educators cited attributes that cut across both cognitive and affective domains of CT as defined by Scheffer and Rubenfeld.8 A few educators (8.5%) did not respond to the question.
The data in Table 2 indicates that the cognitive domain was most frequently referred to (82 occurrences), with analysis (31 occurrences) referred to most often. Information seeking was cited the least (three occurrences).
The most frequently cited attribute in habits of mind domain was reflection (six occurrences). Contextual perspective, flexibility, and perseverance were not referred to at all.
There were some attributes the nurse educators included that did not fall under any of the attributes described in Scheffer and Rubenfeld’s8 definition of CT. The most frequently cited attribute in this category was problem solving, with 12 occurrences.
Table 3 summarizes the perceptions of respondents on CT. The table indicates that 56.6% of the respondents agreed that CT is discipline specific. A majority (69.8%) of the respondents disagreed that CT does not involve the affective domain of learning. Also, most of the participants (66%) disagreed that CT involves only the cognitive domain of learning. More than 95% of the participants agreed that CT was essential in making clinical judgments. A majority of participants (88.6%) believed that CT was needed for daily problem solving.
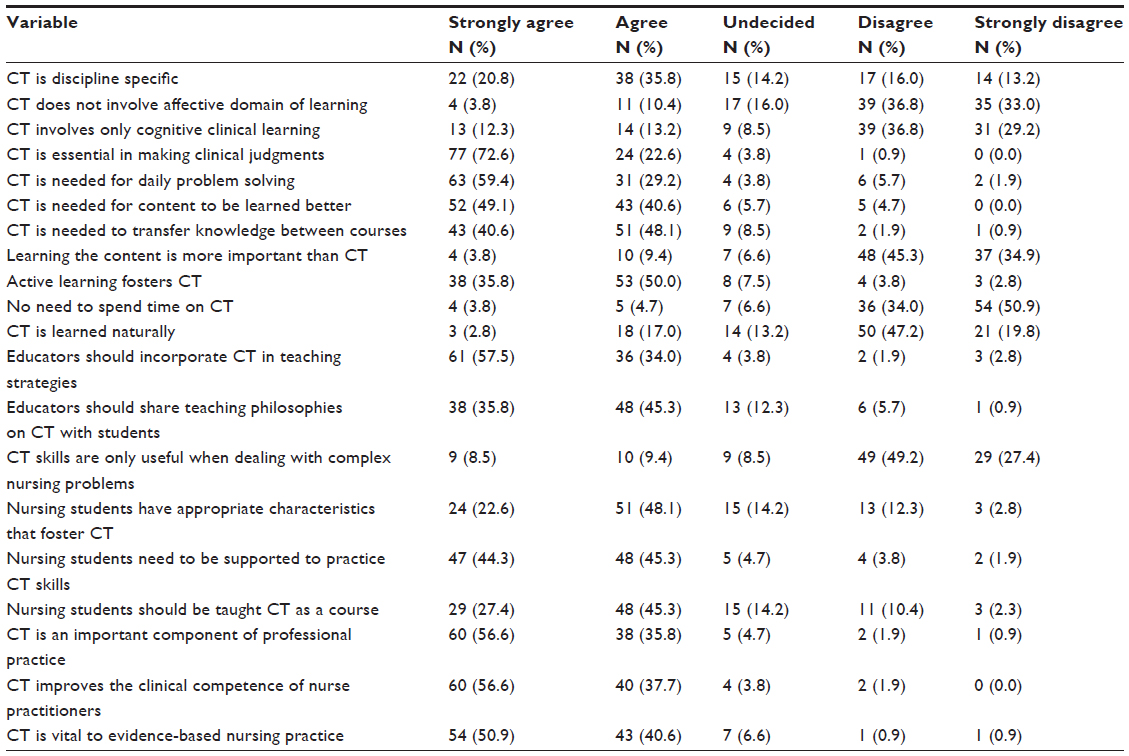 | Table 3 Nurse educators’ perceptions of critical thinking |
Most of the participants (85.8%) perceived that active learning fosters CT, and 92% of the respondents agreed that educators should incorporate CT in teaching strategies. The majority of the respondents (89.6%) agreed that nursing students need to be supported to practice CT skills. More than 70% of the participants believed that nursing students should be taught CT as a separate course. Similarly, 73.6% agreed with the perception that educators are responsible and accountable for the development of CT in students. The majority (91.5%) agreed that CT is vital to evidence-based nursing practice.
To compare the perceptions of the two classes of nurse educators – those in NTCs and those in universities, an independent t-test (Table 4) was used. There was a significant difference between the perception of nurse educators in public universities and nurse educators in NTCs (t-value of 2.74, df =104, P=0.007).
 | Table 4 Comparison of perceptions of nurse educators in universities and NTCs using independent t-test |
Discussion
Though Ghana is known to require a minimum of bachelor’s degree as a requirement to teach in the NTCs, the results revealed that some NTCs had diploma holders (6.6%) on their teaching staff. This raises questions about the adequacy of preparation to assume the role of a nurse educator among those individuals. Some NTCs recruit educators with diploma qualifications to be mentored, including formal education to obtain the minimum qualification to teach. However, these underqualified educators often assume the teaching role. This is perhaps due to the shortage of qualified nurse educators. Despite the argument that formal qualification per se does not reflect competence, Andersson et al15 suggested that some minimum academic qualifications must be satisfied. Similarly, the National Council for State Boards of Nursing recommendations on the qualifications of nurse educators presupposes that the educator’s qualification must be above that of the students they are educating.16 However, National Council for State Boards of Nursing stated that clinical preceptors were allowed to “be educated at or above the level for which the student is preparing”.16
One major finding of this study was that only 4.7% of participants considered CT to have both cognitive and affective aspects per the definition of Scheffer and Rubenfeld;8 therefore only a small number actually regarded CT to have both affective and cognitive domains. This suggests that nurse educators do not truly understand the concept of CT. The majority of nurse educators (81.2%) were above 31 years of age. NMC only introduced CT into the basic nursing curricula in 2007, which is most likely after those nurse educators completed their basic training.13 This could explain why educators do not fully understand CT. These authors have not found any professional development program that specifically helps to develop the CT skills of nurse educators in Ghana. Mangena and Chabeli17 reported that nurse educators themselves were not knowledgeable about CT.
Of importance was the degree of emphasis educators placed on the cognitive domain (82 attributes). This suggested that attention was devoted to the development of skills (cognitive) and knowledge acquisition, neglecting the development of a CT attitude. This contrasted with the opinion of authors who recognized attitude as an essential attribute of CT.18,19 This also supports task-orientation seen in nursing in Ghana, with less emphasis on holistic care.11 Analysis (31 occurrences) was the most frequently referred to attribute in the cognitive aspect. This is consistent with Turner, who reported that from 1992 to 2002 the most frequently referred to attribute of CT in the nursing literature was analysis.20
Educators identified some attributes that were not captured in Scheffer and Rubenfeld’s8 definition of CT. Problem solving was the most frequently identified attribute in this category. CT is often described as problem solving. However, it is not every CT process that is intended to resolve a problem.
The perception that CT was discipline specific and must be taught as a course is an important finding. There are three schools of thought when it comes to how CT should be taught. These include CT taught as a separate course, CT incorporated in all courses, and CT taught as both a separate course as well as incorporated in other courses. This finding is congruent with Ennis21 who argued for CT to be taught as both a separate course and also be incorporated into all courses.
The findings that educators perceived CT as being essential in making clinical judgments and vital to evidence-based nursing practice are not new. The National League for Nursing had cited CT as essential component for good clinical practice.2 Similarly, Ireland also argued that CT is necessary for evidence-based practice.22
The findings that active learning fosters CT, that it should be incorporated in teaching strategies, and philosophies on CT should be shared with students are consistent with other works. It is apparent that educators recognized their significant roles in promoting the development of CT in students. DeYoung23 cited active learning in the promotion of CT in students. Billings and Halstead24 suggested incorporation of CT in teaching strategies. Billings and Halstead24 asserted that educators should share teaching philosophies on CT with students.
One of the major findings of this study was the significant difference in perceptions of CT between nurse educators in public universities and nurse educators in NTCs (P=0.007). This suggested that there is a relationship between educational preparation and perception of CT. The nurse educators working at the universities had more positive perceptions of CT than educators employed in the NTCs. The minimum qualification for teaching in universities in Ghana is a master’s degree. However, individuals with a bachelor’s degree and sometimes a diploma, held teaching appointments in the NTCs, as shown by the demographic characteristics of this study (Table 1). This finding is similar to Kowalczyk et al25 who reported that educators with higher educational qualification were more receptive to CT promotion strategies.
Limitations
The data collection was from one point in time. In addition, self-reporting of perceptions does not directly measure the CT skills and teaching strategies for CT. The response rate (65%) and limited number of respondents from the universities limits the generalization and validity of the results.
Implications for nursing
The large number of nurse educators with undergraduate and diploma qualifications and poor understanding of the concept of CT undermines efforts of enhancing CT in nursing education. The fact that almost 40% of participants had graduate qualifications suggests the likelihood of evolution in nursing education in Ghana.
Nursing requires academically qualified educators to produce nurses who possess the ability to critically evaluate patient data. The findings of this study suggest that attention must be focused on preparation of nurse educators in order to promote CT in students. CT can be exhibited and taught only if the concept is understood. Nursing programs and continuing professional development programs must include CT to reflect its important role in nursing practice.
Conclusion
CT is crucial in shaping health care providers, especially nurses, prepared to respond to the current complex health needs. Yet, Ghana is using a nursing educational system that cannot result in good health outcomes. Nursing programs are not adequately preparing nurses with the necessary CT skills required for a dynamic health care environment. Nurse educators in Ghana do not fully understand CT. Nurse educators in universities are more receptive to integrating the concept of CT into their teaching, yet they do not always have the requisite skills. Professional development programs in CT should be instituted for nurse educators.
Disclosure
The authors report no conflicts of interest in this work.
References
Toofany S. Critical thinking among nurses. Nurs Manag. 2008;14(9):28–31. | |
National League for Nursing. Excellence in Nursing Education Model. New York, NY: National League for Nursing; 2006. | |
Jarvis C. Physical Examination and Health Assessment. 5th ed. St Louis, MO: Elsevier; 2008. | |
del Bueno DA. Crisis in critical thinking. Nurs Educ Perspect. 2005; 26(5):278–282. | |
Walsh CM, Seldomridge LA. Critical thinking: back to square two. J Nurs Educ. 2006;45(6):212–219. | |
Fero LJ, Witsberger CM, Wesmiller SW, Zullo TG, Hoffman LA. Critical thinking ability of new graduate and experienced nurses. J Adv Nurs. 2009;65(1):139–148. | |
Adams BL. Nursing education for critical thinking: an integrative review. J Nurs Educ. 1999;38(3):111–119. | |
Scheffer BK, Rubenfeld MG. A consensus statement on critical thinking in nursing. J Nurs Educ. 2000;39(8):352–360. | |
Adjatey E. Nursing: dispassionate profession in Ghana. Vibe Ghana.com; 2013. Available from: http://vibeghana.com/2013/07/29/nursing-dispassionate-prefession-in-ghana. Accessed July 16, 2015. | |
Adofo R. A Case of Deplorable Attitude of Ghana Nurses: True Story; 2010. Available from: http://www.ghanaweb.com/GhanaHomePage/features/artikel.php?ID=195002. Accessed July 16, 2015. | |
Opare M, Mill JE. The evolution of nursing education in a postindependence context – Ghana from 1957 to 1970. West J Nurs Res. 2000;22(8):936–944. | |
Wilmot EM, Kumfo J, Danso-Mensah D, Antwi-Danso S. An Investigation into the Factors That Contribute to Nurse/Midwife Trainees’ Poor Performance in the Final Licencing Examination in Ghana. Accra, Ghana: Nursing and Midwifery Council of Ghana; 2013. | |
Nursing and Midwifery Council of Ghana. Curriculum for the Registered General Nursing (RGN) Program. Accra, Ghana: Nursing and Midwifery Council of Ghana; 2007. | |
Ellen S. Slovin’s formula sampling techniques. eHow. Available from: http://www.ehow.com/way_5475547_slovins-formula-sampling-techniques.html. Accessed Nov 2014. | |
Andersson P, Köpsén S, Larson A, Milana M. Qualification paths of adult educators in Sweden and Denmark. Stud Cont Educ. 2013;35(1):102–118. | |
National Council for State Board of Nursing. Nursing faculty qualification and roles. Chicago, USA: National Council for State Board of Nursing, Inc.; 2008. | |
Mangena A, Chabeli MM. Strategies to overcome obstacles in the facilitation of critical thinking in nursing education. Nurs Educ Today. 2005;25(4):291–298. | |
Paul RW. Critical thinking: what, why, and how? New Directions Commun Colleges. 1992;77:3–24. | |
Facione PA. The disposition toward critical thinking: its character, measurement, and relation to critical thinking skill. Informal Logic. 2000;20(1):61–84. | |
Turner P. Critical thinking in nursing education and practice as defined in the literature. Nurs Educ Perspect. 2005;26(5):272–277. | |
Ennis RH. Incorporating critical thinking in the curriculum: an introduction to some basic issues. Inquiry Crit Think Across Discipline. 1997;16(3):1–9. | |
Ireland M. Assisting students to use evidence as a part of reflection on practice. Nurs Educ Perspect. 2008;29:90–93. | |
DeYoung S. Teaching Strategies for Nurse Educators. 2nd ed. New Jersey, NJ: Pearson Education Inc.; 2009. | |
Billings DM, Halstead JA. Teaching in Nursing: A Guide for Faculty. 3rd ed. St Louis, MO: Elsevier Saunders; 2009. | |
Kowalczyk N, Hackworth R, Case-Smith J. Perceptions of the use of critical thinking teaching methods. Radiol Technol. 2012;83(3):226–236. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.