")
Back to Journals » Clinical Ophthalmology » Volume 16
Novel Inferior Oblique Muscle Y Splitting Procedure to Minimize the Anti-Elevation Syndrome: A Pilot Study
Authors Pujari A , Modaboyina S, Thangavel R, Yadav M, Phuljhele S, Saxena R
Received 8 July 2022
Accepted for publication 15 August 2022
Published 22 August 2022 Volume 2022:16 Pages 2723—2731
DOI https://doi.org/10.2147/OPTH.S381094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Supplementary video of "Y-splitting of the inferior oblique for anti-elevation syndrome" [ID 381094].
Views: 696
Amar Pujari, Sujeeth Modaboyina, Rajeswari Thangavel, Monika Yadav, Swati Phuljhele, Rohit Saxena
Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India
Correspondence: Amar Pujari, Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, Room No. 212, RPC-1, AIIMS, New Delhi, India, Email [email protected]
Purpose: To describe novel Y splitting procedure of inferior oblique muscle to mitigate the anti-elevation syndrome.
Methods: A pilot, prospective interventional study was undertaken to assess the effect of inferior oblique muscle Y-splitting in patients with unilateral 3+ or more overaction. To correct primary gaze hypertropia and the excyclotorsion, a Y-splitting procedure was performed (along with routine horizontal muscle surgery as per the deviation) in 14 subjects. The effect of surgery was assessed at baseline and at 6 months post-intervention.
Results: The mean age of 14 subjects was 25.14± 7.70 years. The mean pre-operative hypertropia, excyclotorsion and inferior oblique muscle over-action was 18.42± 3.50 PD, 14.14± 2.65 degrees, and +3.21± 0.42 respectively. Following surgery, this was reduced to 1.57± 1.74 PD of residual hypertropia (a net correction of 16.85± 2.31 PD, p = 0.005), 3.85± 1.46 degrees of residual excyclotorsion (a net correction of 10.28± 1.72 degrees, p < 0.05), and +0.28± 0.46 of residual inferior oblique over-action (a net correction ∼+3) at the end of 6 months. Amongst fourteen patients, three patients still experienced residual/variable anti-elevation effect, and during the study period none of them experienced any adverse event and none of them required any additional surgeries.
Conclusion: While anteriorizing the inferior oblique muscle to correct primary gaze hypertropia and the excyclotorsion, a novel “Y splitting” procedure can be followed to achieve the desired results with mitigated anti-elevation effect.
Keywords: inferior oblique muscle surgery, anti-elevation syndrome, Y-splitting of the inferior oblique
Introduction
In strabismus surgeries, the inferior oblique muscle procedures are quite unique, as compared to routine recti muscle surgeries, the inferior oblique surgeries follow a distinct pattern.1,2 The most commonly performed surgeries on inferior oblique include its weakening, which are indicated when there is overelevation in adduction. Nevertheless, these procedures are also intended to correct the primary gaze hypertropia as well as excyclotorsion.1–7 In clinics, the inferior oblique muscle overaction is frequently encountered in infantile esotropes, where it can be witnessed in up to 70% of the cases,1 such overactions can also be witnessed in superior oblique palsy, comitant horizontal deviations, dissociated vertical deviation, and others. To treat it, in milder grades (usually 1+), we prefer 8–10 millimeters of inferior oblique recession, and in grade 2+ we prefer 12–14 millimeters of recessions or Elliott and Nankins procedure. In grades 3+ and 4+, we prefer the anteriorization procedure or the antero-nasal transposition procedure, where the primary gaze hypertropia as well as the excyclotorsion are taken care of. Apart from these, myectomy and many other procedures have been described in literature,3,4,6–8 however we rarely prefer them.
All these techniques are able to cure the over-elevation in adduction, and also they are able to collapse the associated “V” pattern strabismus,1,5,7 however, the anteriorization procedures are quite famous for their anti-elevation effect, or the anti-elevation syndrome (as described by Kushner).9,10 Where, due to anatomical changes in the inferior oblique muscle course and its associated neurovascular bundle the vertical rotation is limited, clinically, it can be witnessed as elevation deficit in abduction as well as in primary gazes (Figure 1). Moreover, the associated narrowing of aperture width in up gaze is also equally bothersome in many patients (Figure 1).
 |
Figure 1 Our previously operated patients showing restricted elevation in primary gaze following total anterior positioning in the right eye (A, B two different patients). In straight-ahead up gaze, a significant limitation in elevation with active narrowing of the aperture width can be seen. |
To mitigate this effect, many strategies have been described, including antero-nasal transposition, limited anterior suturing, and modified anterior suturing; however, amongst these only few methods seems address the tension along posterior fibers and the neurovascular bundle.11–15 In anti-elevation effect, the inferior oblique neurofibrovascular bundle (NFVB) is the main culprit, where it mechanically restricts the vertical rotation of globe.1,16,17 Therefore, to minimize this untoward effect we have worked on a novel technique, and it has worked well in our hands. The technique is “Y-splitting” of inferior oblique muscle while anteriorizing it. The indications, surgical steps, and the pre- and post-operative outcomes on over-elevation in adduction, primary gaze hypertropia, excyclotorsion, and the anti-elevation effect are as follows.
Methods
A prospective interventional study was undertaken to explore the effect of inferior oblique “Y splitting” procedure while anteriorizing it. Before initiation, an institution ethical committee clearance (IEC-266/07.05.2021. All India Institute of Medical Sciences, New Delhi. India) was obtained, and as per ethical committee recommendations, it was also registered to the clinical trial registry of India (CTRI/2021/08/035322), even though it was not a comparative trial. During study period, we strictly adhered to the tenants of declaration of Helsinki.
Prospectively, adult patients (more than 18 years) seeking treatment for their ocular misalignment at our strabismus sub-specialty clinic were observed. Patients with horizontal strabismus and primary gaze hypertropia due to unilateral three or four-plus inferior oblique muscle overaction were included. A total of 14 patients (8 patients with horizontal comitant deviation and 6 patients with superior oblique palsy) satisfied these criteria and were considered for surgery (a written informed consent was obtained from each). The demography, complete ocular evaluation, horizontal and vertical deviations using prism bar cover test, pre-operative excyclotorsion (using fundus photographs) and rest of the orthoptic workup (stereopsis, fusional range, and other tests of binocular function depending on the indication and need) was performed at baseline and at the end of 6 months. The surgical dosage for horizontal strabismus was followed as per our existing protocols and for inferior oblique muscle over-action and the associated hypertropia, a “Y-splitting” procedure was opted. All surgeries were performed by the first author, and patients were followed up on day 1, day 7, 1 month, 3 months and 6 months post-operatively. The net correction of inferior oblique overaction, the net effect on vertical deviation, the net change in excyclotorsion (on image J software, ImageJ 1.53k, 2021, USA), and the overall effect on elevation were assessed at 1 month, 3 months and 6 months, but only 6 months results were considered for the final statistical analysis.
Statistical Analysis
The statistical analysis was performed using Stata software version 12.1 (2011, USA). To compare the pre- and post-operative significance paired t-tests were applied, and any p-value of less than 0.05 was considered statistically significant.
Surgical Technique (Video 1)
The eye to be operated was prepared, with the help of a cotton traction suture the inferotemporal quadrant exposed. Forniceal conjunctival peritomy was initiated followed by an opening in the tenons, the lateral rectus was hooked and it was retracted superiorly, with the help of another lens hook the remaining conjunctiva and the tenons were dragged inferiorly. Using two muscle hooks, the inferior oblique muscle was hooked and it was dis-inserted from its insertion. The dis-inserted end was then grasped using serrated forceps and it was divided into two equal halves, each end was sutured using a single arm of 6–0 polyglactin suture and the muscle was secured, following this the half-width dissection was continued posteriorly till about 10–12 millimeters, for any bleed either gentle pressure was applied or limited cautery was performed. Subsequently, the inferior rectus muscle was hooked, and its lateral insertional point was demarcated. The anterior fibers of inferior oblique were sutured anteriorly just 2 millimeters diagonal to the lateral insertional margin of inferior rectus, and the posterior fibers were sutured 6 millimeters behind the inferior rectus insertion (parallel to its lateral muscle border). (Figure 2) After tying final knots, the posterior and the anterior fibers were hooked and checked for tension, when relaxed posterior fibers were confirmed then the peritomy was closed and eye patching was done after placing antibiotic ointment. Post-operatively, the patients were advised topical antibiotic-steroid combination eye drops along with lubricating eye drops for 6 weeks in a tapering manner.
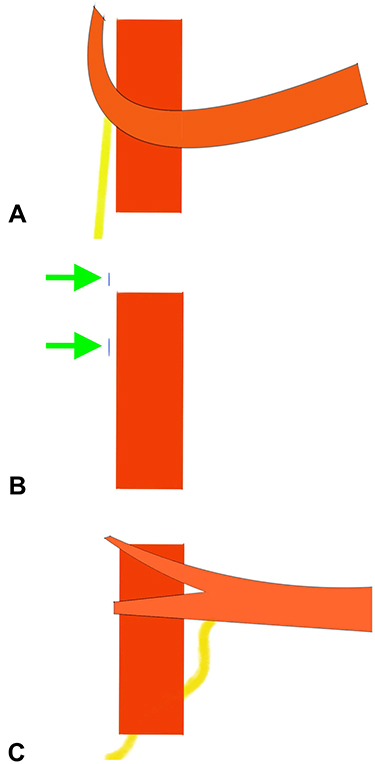 |
Figure 2 The animated diagram shows the Y splitting procedure. While performing the routine total anterior positioning, the whole inferior oblique is sutured just anterior to inferior rectus insertion. During this, the NFVB actively gets stretched, hence it causes the anti-elevation syndrome (A). In our modification, after splitting the inferior oblique muscle, the anterior fibres are sutured just 2 mm diagonal to the lateral margin of the inferior rectus insertion (it should be noted that it is neither simple 2 mm lateral nor simple 2 mm anterior, it’s diagonal 2 mm) (B). The posterior fibres are sutured 6 mm behind the lateral margin of the inferior rectus insertion or 8 mm behind the anterior fibre suturing site (B). Post-suturing, the animation depicts the possible relieving effect on posterior fibres as well as on the NFVB (C). |
Results
The mean age of 14 patients was 25.14±7.70 (19 to 46) years. Seven were male and rest were female. The right eye was operated in 9 and the left in rest. The mean duration of follow-up at final assessment was 196.78±17.38 days (180–240 days or ~6.5 months) (Table 1).
 |
Table 1 The Demographic and the Surgical Parameters in Pre- and Post-Operative Periods |
The mean pre-operative hypertropia was 18.42±3.50 (14–25) prism dioptres (PD), with surgery it was reduced to 1.57±1.74 PD. A net correction of 16.85±2.31 (12–20) PD of hypertropia was achieved per patient, and it was statistically significant (p = 0.005). Similarly, the mean pre-operative excyclotorsion was 14.14±2.65 (10–20) degrees, which was reduced to 3.85±1.46 (2–6) degrees with Y-splitting procedure. Hence, a net correction of 10.28±1.72 degrees of excyclotorsion per patient was achieved, and it was statistically significant (p < 0.05). The mean pre-operative inferior oblique over-action was +3.21±0.42 (+3 to +4) which was reduced to +0.28±0.46 with surgery, and again a net correction ~+3 per patient was achieved (Table 1) (Figures 3–5). Figure 3 (A) In a first patient with an intermittent divergent squint and 3+ inferior oblique overaction in the right eye shows hypertropia (A), restriction-free elevation in up gaze (B), free elevation in abduction (C) and +3 over-elevation in adduction in the right eye (D) (Yellow arrows). (B) The same patient post-surgery at 6 months shows full correction of primary gaze hypertropia (A’), restriction-free (yellow arrow) up gaze (B’) and correction of V pattern. Restriction-free elevation (yellow arrow) in abduction (C’) and correction of +3 over-elevation in adduction (D’).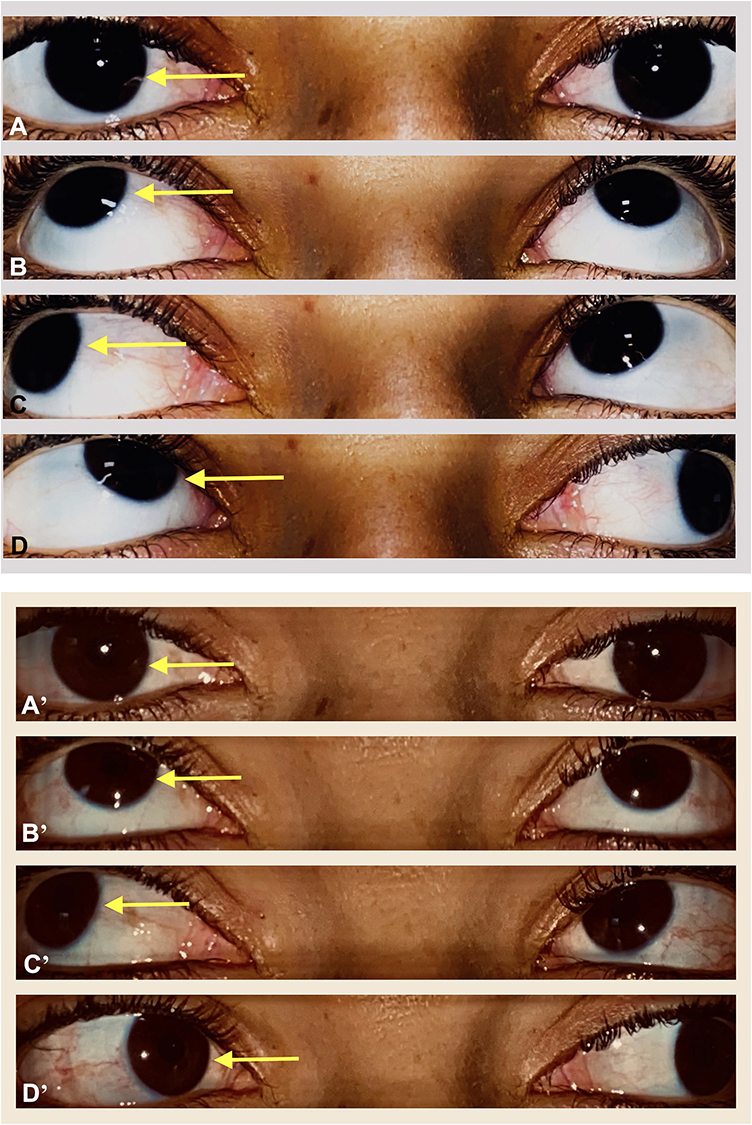
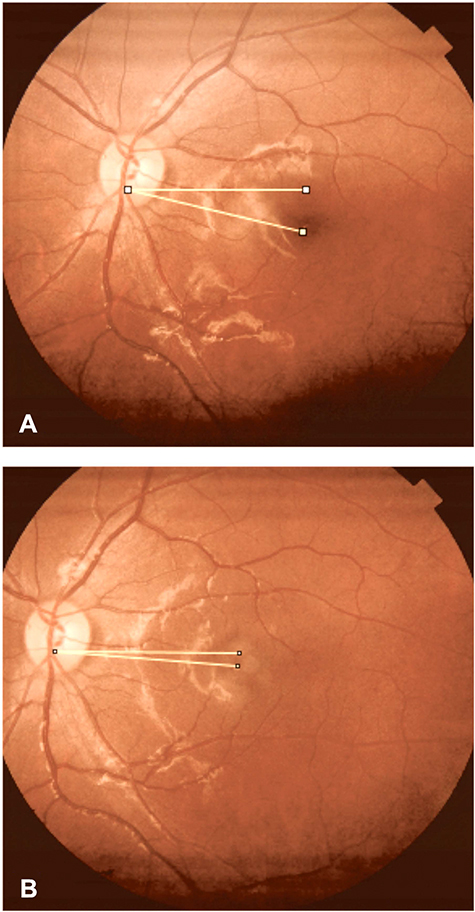 |
Figure 4 Shows the pre-operative excyclotorsion of around 14 degrees (A) and following surgery it was reduced to around 4 degrees (B) (Protractor value). |
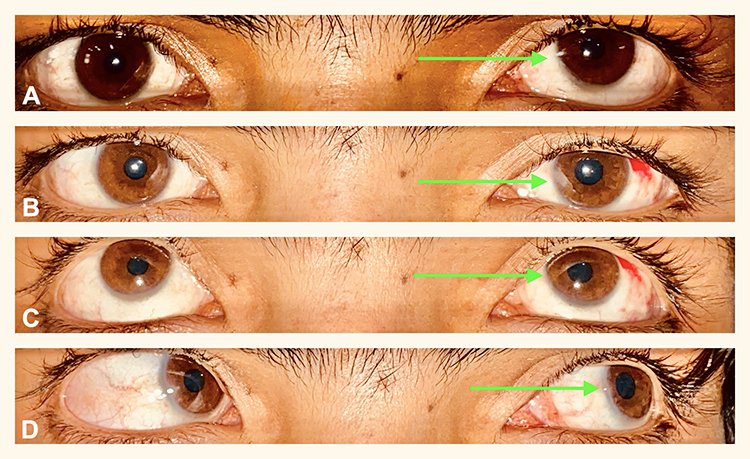 |
Figure 5 In a seventh patient with left-sided superior oblique palsy, pre-operative hypertropia can be seen (Green arrow, (A). Post-surgery, at 1 month, the full correction of primary gaze hypertropia is evident (Green arrow, (B), in up gaze, a very minimal elevation deficit is evident (Green arrow, (C), and in abduction, again a very subtle amount of restriction can be seen (Green arrow, (D). However, this improved further at the end of 6 months with no active complaints. |
Of the 14 patients, all were satisfied with the primary gaze correction; however, three patients (21.4%) complained of minimal anti-elevation effect and/or narrowing of the aperture width in up gaze (usually beyond 20 degrees) (Figures 6 and 7). In two patients, a mild narrowing (1–1.5 mm) of aperture width was noted at 1 month; however, it was less problematic at the end of 6 months (Figure 5). During the study period, none of the patients reported any adverse events and none were dissatisfied with the surgical outcomes, therefore no additional surgery was necessary in any patient.
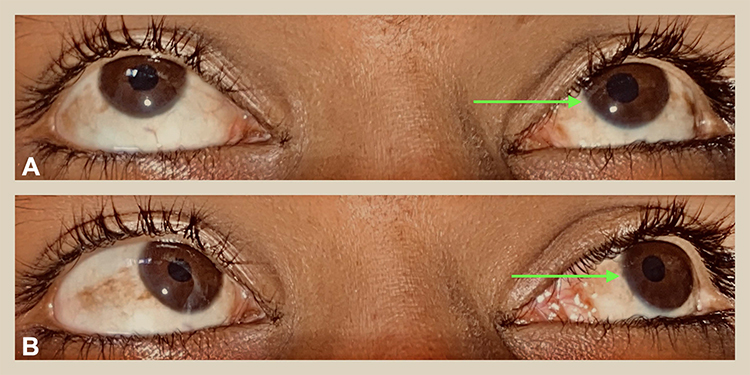 |
Figure 6 In patient 9, post-surgery mild elevation deficit in up gaze (Green arrow, (A), in abduction gaze (Green arrow, (B) can be seen at the end of 3 months. |
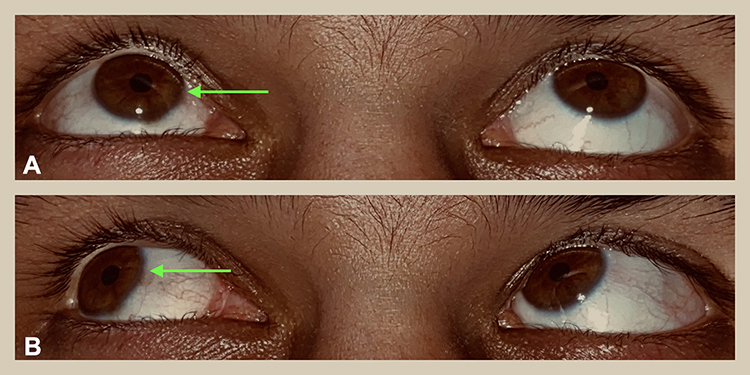 |
Figure 7 Again, in patient 10, post-surgery notable elevation deficit in up gaze (Green arrow, A), and abduction gaze (Green arrow, B) can be seen at the end of 6 months. |
Discussion
The literature has witnessed a steep change in inferior oblique muscle surgeries in recent times.1,2 This is possible due to evolving understandings with respect to oblique muscle anatomy and its functioning.11,16 Till now, many attempts have been made to compare the efficacy of different techniques of weakening procedures, by following any of this procedure, the over-elevation in adduction, the V pattern strabismus and the excyclotorsion can be very well cured. Moreover, with the anteriorization procedure, the vertical deviation can also be cured with reasonable predictability. In an observation by Hatz et al, the anterior positioning cured a mean vertical deviation of 15 PD, and as per authors’ experience for a hypertropia of more than 15 PD a second vertical rectus muscle surgery was recommended.18
These techniques have very few limitations, but as noted by many authors one such unique limitation is the risk of anti-elevation syndrome with the anteriorization procedure (which in our experience happens in many patients of anteriorized muscle). The cause for this can be attributed to the NFVB of inferior oblique muscle. Stager senior has worked extensively on this issue of NFVB and its effect and has defined the mechanism more precisely. According to him, when the inferior oblique muscle was cut from the surrounding inter-muscular septum and when it was kept under 10-gram stress, the possible anterior movement of the dis-inserted inferior oblique was only for about 2 millimeters. Whereas after severing NFVB, under the same stress, the dis-inserted end moved to about 13.8 millimeters (on average).11 Hence, from these anatomical and experimental results, it is quite clear that the NFVB acts as an ancillary origin, and it is the main restrictor for vertical rotation.11
Based on these valuable concepts, we were able to devise a new technique where the NFVB and associated posterior fibers were kept relaxed all the time. After Y splitting of the inferior oblique muscle, the posterior fibers and the NFVB assumed a more recessed position. This is in contrast to the conventional total anterior positioning procedure, where the posterior fibers were actively dragged just anterior to inferior rectus muscle insertion (depending on the site of suture, usually up to a few millimeters). Hence, this active pull was relieved by the current splitting procedure; moreover, it also nullified the possible mechanical pull from the posterior fibers. Therefore, the splitting procedure was able to recess the posterior fibers by an amount of 14 mm (from insertion) and was also able to relax the NFVB in primary, in abduction and in the elevated gazes. This was achieved at no cost to the routine effects of inferior oblique surgery, that is the correction of primary gaze hypertropia, excyclotorsion, over-elevation in adduction and the V pattern strabismus.19
As mentioned in the results section, in 3 patients we noticed a variable amount of elevation restriction. This we explored further using intra-operative details, measurements, and the gross patient features. With these, we noted the following common features which were evident in all three cases. 1) These patients had slightly deep-seated eyes, and 2) intra-operatively these patients’ inferior oblique muscle was quite bulky with increased tension. From these observations, it is possible that the patients with shallow orbits and the muscles with greater tension or due to some other connective tissue reasons, the split may have been less effective in these eyes. Also, as evidenced by Stager junior et al,20 the microscopic features may be equally responsible for this. Out of these three patients, two also complained of minimal fullness under the inferior eyelid until 4–12 weeks; however, after that it resolved gradually probably due to muscle thinning/atrophy (personal experiences) till 6 months. Therefore, in patients with intra-operative tight muscles or with shallow orbital features, caution must be exercised to improve the acceptance of post-operative results.
The index study had some common understandings during surgery which were based on our clinical understandings and our experiences. These include 1) the length of split was maintained between 10 and 12 millimeters. This was because, any separation of less than 10 millimeters were less effective in relieving the tension on posterior fibers, and more than 12 millimeters was avoided just to prevent possible neuro-vascular bundle injuries. 2) By splitting, the chances of inferior oblique palsy were less, during our 6 months observation we did not encounter any patients with features of iatrogenic inferior oblique palsy. 3) After splitting, the anterior fibers were sutured at 2 mm diagonal to the lateral border of inferior rectus insertion, and the posterior fibers at 6 mm posterior to the inferior rectus insertion (or total 8 mm behind the anterior fibers). The recessed anterior fibers cured the hypertropia and the posterior fibers relaxed the NFVB with effective relief of over-elevation in adduction. 4) In our observation 6 months follow-up was sufficient to conclude the possible long-term changes based on our past experiences with inferior oblique surgeries as well as based on current literature evidence.
Our study had few limitations, which include, 1) the study was not a randomized comparative trial (pilot observation) to the traditional total anterior positioning procedure, however, based on our previous encounters with anti-elevation effects, the newer results were convincingly better in relieving the ant-elevation effect; moreover, it was a pilot observation and future comparisons will be undertaken. 2) There is no real-time measure to visualize the relieving effect of Y splitting procedure (apart from intra-operative experiences). 3) The residual anti-elevation effect in 3 cases needs further explanation.
To conclude, while anteriorizing the inferior oblique muscle (due to primary or secondary +3 or more over action), a simple Y splitting procedure can be followed to mitigate the possible anti-elevation syndrome. After splitting, the anterior as well as the posterior fibers do achieve the intended recession effect with added superior cosmetic outcomes.
Data Sharing Statement
All the data related to the study have been extensively mentioned in the text.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stager D Jr, Dao LM, Felius J. Uses of the inferior oblique muscle in strabismus surgery. Middle East Afr J Ophthalmol. 2015;22(3):292–297. doi:10.4103/0974-9233.159723
2. Sato M. Historical review of inferior oblique muscle surgery. Taiwan J Ophthalmol. 2017;7:12–14. doi:10.4103/tjo.tjo_21_17
3. Sanjari MS, Shahraki K, Nekoozadeh S, Tabatabaee SM, Shahraki K, Aghdam KA. Surgical treatments in inferior oblique muscle overaction. J Ophthalmic Vis Res. 2014;9(3):291–295. doi:10.4103/2008-322X.143355
4. Farid MF, Anany M, Abdelshafy M. Surgical outcomes of three different weakening procedures of inferior oblique muscle in the treatment of unilateral superior oblique palsy. BMC Ophthalmol. 2020;20:298. doi:10.1186/s12886-020-01568-w
5. Ozsoy E, Gunduz A, Ozturk E. Inferior oblique muscle overaction: clinical features and surgical management. J Ophthalmol. 2019;2019:9713189. doi:10.1155/2019/9713189
6. Shipman T, Burke J. Unilateral inferior oblique muscle myectomy and recession in the treatment of inferior oblique muscle overaction: a longitudinal study. Eye. 2003;17:1013–1018. doi:10.1038/sj.eye.6700488
7. Coats DK, Olitsky SE. Surgery on the inferior oblique muscle. In: Strabismus Surgery and Its Complications. Berlin, Heidelberg: Springer; 2007. doi:10.1007/978-3-540-32704-2_11.
8. Davis G, McNeer KW, Spencer RF. Myectomy of the inferior oblique muscle. Arch Ophthalmol. 1986;104(6):855–858. doi:10.1001/archopht.1986.01050180089037
9. Kushner BJ. Restriction of elevation in abduction after inferior oblique anteriorization. J AAPOS. 1997;1(1):55–62. doi:10.1016/S1091-8531(97)90024-0
10. Kushner BJ. Torsion as a contributing cause of the anti-elevation syndrome. J AAPOS. 2001;5(3):172–177. doi:10.1067/mpa.2001.115849
11. Stager DR. Costenbader lecture. Anatomy and surgery of the inferior oblique muscle: recent findings. J AAPOS. 2001;5(4):203–208. doi:10.1067/mpa.2001.116273
12. Mims JL 3rd, Wood RC. Antielevation syndrome after bilateral anterior transposition of the inferior oblique muscles: incidence and prevention. J AAPOS. 1999;3(6):333–336. doi:10.1016/S1091-8531(99)70040-6
13. Ziffer AJ, Isenberg SJ, Elliott RL, Apt L. The effect of anterior transposition of the inferior oblique muscle. Am J Ophthalmol. 1993;116(2):224–227. doi:10.1016/S0002-9394(14)71290-5
14. Jeon H, Kwon H, Choi HY. Modified anterior transposition of the inferior oblique muscle. J AAPOS. 2018;22(5):361–365.e1. doi:10.1016/j.jaapos.2018.06.008
15. Cho YA, Kim JH, Kim S. Antielevation syndrome after unilateral anteriorization of the inferior oblique muscle. Korean J Ophthalmol. 2006;20(2):118–123. doi:10.3341/kjo.2006.20.2.118
16. Stager DR. The neurofibrovascular bundle of the inferior oblique muscle as its ancillary origin. Trans Am Ophthalmol Soc. 1996;94:1073–1094.
17. Stager DR, Weakley DR Jr, Stager D. Anterior transposition of the inferior oblique. Anatomic assessment of the neurovascular bundle. Arch Ophthalmol. 1992;110(3):360–362. doi:10.1001/archopht.1992.01080150058028
18. Hatz KB, Brodsky MC, Killer HE. When is isolated inferior oblique muscle surgery an appropriate treatment for superior oblique palsy? Eur J Ophthalmol. 2006;16(1):10–16. doi:10.1177/112067210601600103
19. Min BH, Park JH, Kim SY, Lee SB. Comparison of inferior oblique muscle weakening by anterior transposition or myectomy: a prospective study of 20 cases. Br J Ophthalmol. 1999;83:206–208. doi:10.1136/bjo.83.2.206
20. Stager D
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.