")
Back to Archived Journals » Robotic Surgery: Research and Reviews » Volume 7
Novel Energy Devices in Head and Neck Robotic Surgery – A Narrative Review
Authors Ross T , Tolley NS, Awad Z
Received 28 January 2020
Accepted for publication 6 April 2020
Published 23 April 2020 Volume 2020:7 Pages 25—39
DOI https://doi.org/10.2147/RSRR.S247455
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Masoud Azodi
Talisa Ross,1,2 Neil S Tolley,2,3 Zaid Awad2,3
1Department of Ear, Nose and Throat Surgery, London North West University Healthcare NHS Trust, London, UK; 2Faculty of Medicine, Imperial College London, London, UK; 3Department of Ear, Nose and Throat Surgery, Imperial College Healthcare NHS Foundation Trust, London, UK
Correspondence: Talisa Ross
Tel +44 7825 637 913
Email [email protected]
Abstract: The advent of trans-oral robotic surgery (TORS) has facilitated removal of tumors previously deemed unresectable, by providing access to the deep structures of the head and neck. Despite this, the wider dissemination of TORS has been restricted due to issues with line of access, as the da Vinci robot was never designed with head and neck surgery in mind. Flexible instruments and novel energy delivery devices offer great potential in overcoming some of the existing challenges surrounding TORS. This review aimed to summarize the existing literature surrounding energy delivery in TORS and highlight areas of future innovation. MEDLINE was searched for studies relating to energy delivery in TORS in November 2019. The existing literature surrounding monopolar and bipolar electrocautery, LASER (CO2, Tm:YAG and blue LASER), Ligasure and Harmonic was reviewed. Additionally, the latest iteration of the da Vinci; the SP, and the FLEX robot were evaluated as novel methods of energy delivery in TORS. Overall, these novel energy devices and robotic systems are predicted to further improve energy delivery to the head and neck. The use of flexible LASER in particular is well substantiated in the literature. This has the potential to achieve treatment de-escalation, based on the excellent outcomes demonstrated for disease-free margins and post-operative morbidity.
Keywords: robot, head and neck, LASER, TORS
Introduction
The dawn of robotics in Ear, Nose and Throat Surgery (ENT) within the last 15 years has revolutionized treatment for head and neck malignancy. Trans-oral robotic surgery (TORS) thus far has provided surgeons with access to the deep structures of the head and neck through the natural orifice of the mouth to facilitate tumor resection using the most widely disseminated da Vinci robotic system (Intuitive Surgical®, Sunnyvale, California). TORS has armored the surgeon with a tool which can offer both improved functional preservation and reduced morbidity, compared to conventional treatment.
Since the patent on the da Vinci recently expired, this has paved the way for new systems to enter the market. In addition to its substantial cost, wider diffusion of TORS has been restricted by the lack of flexibility and limited instrumentation offered by the da Vinci. The system was never designed with the head and neck in mind, giving rise to a number of criticisms surrounding its ergonomics. Newer systems, in addition to later iterations of the da Vinci, have set out to provide a more fit-for-purpose machine for use in head and neck surgery, through the use of single-port access, flexible instruments and novel energy delivery devices. This dissertation intends to review the existing literature surrounding energy delivery in existing and novel robotic systems and highlight potential areas for future innovation.
A Brief History of Robotic Surgery in ENT
Prior to the 1990s, open surgery was the mainstay of treatment for head and neck malignancies.1 Due to the poor results of such radical open surgery, this was later replaced by chemoradiotherapy, which appeared to achieve equivalent locoregional disease control and survival outcomes, with less associated morbidity. Despite its advantages, concerns began to arise about chemoradiotherapy-related toxicities and the vast functional implications on speech and swallowing.
This era of head and neck cancer treatment coincided with a dramatic increase in the incidence of HPV-related head and neck malignancy. Prognostically, being HPV positive appears to offer patients an advantage over their HPV negative counterparts.2 The notion, however, of the typically younger non-smoking and non-drinking cohort of patients affected by HPV being afflicted with the drastic functional implications of existing treatment gave rise to the concept of treatment de-escalation. The aim of treatment de-escalation was to minimize treatment intensity and hence reduce the rate of treatment-related toxicities, with their ensuing impact of speech and swallowing.1 Interest in surgery as first-line treatment was thereby reinvigorated, which corresponded with the advent of TORS.
TORS was first introduced in 2005, when O’Malley and Weinstein at the University of Pennsylvania completed the first trans-oral resection of a tongue base tumor using the da Vinci robot,3 after demonstrating proof-of-concept with a supraglottic laryngectomy in a canine model.4 The use of TORS subsequently expanded to laryngeal, oropharyngeal, hypopharyngeal and parapharyngeal sites. Using the mouth as a natural orifice has pioneered natural orifice trans-luminal endoscopic surgery (NOTES) in ENT, thereby obviating the need for lip and jaw splitting. Over time, TORS has also been incorporated into NICE guidance for the management of carcinoma of unknown primary (CUP) tumors,5 in addition to its use in benign disease such as obstructive sleep apnea (OSA), for those intolerant to continuous positive airway pressure (CPAP).6
TORS has proven advantageous over its open predecessor for a number of reasons. Firstly, it removes the need for a mandibular split to provide access to the operative site. TORS using the da Vinci also provides the surgeon with a three-dimensional view and endo-wristed instruments with seven degrees of freedom, thereby ameliorating surgical dexterity.7 In contrast to trans-oral LASER microsurgery (TLM), where line-of-sight can be a significant issue, tumors can be resected en-bloc using TORS, maintaining the essential surgical oncology principle not to remove the tumor piecemeal. This also permits better histopathological assessment of the tumor; of great importance when considering treatment de-escalation.8
TORS has opened up the possibility of surgery for many patients whose malignant disease may have been previously unresectable.9 The advent of TORS for both malignant and benign disease is therefore expanding surgery to a new cohort of patients, and its uptake is predicted to continue, replacing trans-oral LASER microsurgery as the mainstay of treatment for selected patients.1,10 Its uptake will further increase, however, if some of the limitations of existing tools and instruments can be overcome. Work has already begun in this area, which is proving to be an exciting field of technological innovation in surgical robotics.
Current Physical Challenges in TORS
There are a number of salient physical challenges that the TORS surgeon will face when operating using the da Vinci. Despite a number of tools being available with the da Vinci, the variety of instruments offered are somewhat more limited than in open surgery. Additionally, changing tools intra-operatively can prove disruptive and slow, as this involves the assistant de-mounting the first tool from the robotic arm, and exchanging it (and re-aligning it) with a new one. Naturally, this leads to intra-operative stagnation, thereby increasing operating time and temporarily diverting the operating surgeon’s attention away from the operative site.
In addition, historically, directing a carbon dioxide (CO2) light amplification by stimulated emission of radiation (LASER) through a metal endoscope has demonstrated extremely limited access to the head and neck, due to the rigid axis the LASER follows when used in this way.11,12 As a result of the greater flexibility offered with TORS, resection of previously inaccessible tumors has now become possible, albeit however with associated challenges. Principally, TORS instruments must be small enough, flexible enough, and precise enough to achieve accurate tissue dissection. Only two of the three arms can be used with the standard da Vinci, however, due to the space restrictions via trans-oral approach. Not only this, but tissue must be kept cool, to avoid thermal injury to critical structures in surrounding areas in a limited space with narrow safety margins.
Tissue preservation is essential in oropharyngeal cancer, so it is imperative that this is considered during instrument selection. The “ideal” instrument for TORS would allow dissection of the tumor en-bloc, permitting clear histopathological analysis. Both lymphovascular invasion and invasion front can be more easily evaluated in a cleanly dissected specimen, as can resection margins.
Achieving disease-free margins whilst minimizing damage to healthy tissue is therefore an essential balance needed to treat malignant disease, whilst preserving function. Additionally, achieving good surgical margins without requiring extra tissue dissection due to thermal artifact is essential in terms of functional preservation. Current instruments used in TORS offer a compromise between these factors, in addition to speed of operating, reducing primary and secondary bleeding, cost, and local availability. Therefore, the innovation of an “ideal” energy device that can feasibly be implemented into everyday practice remains theoretical.
Research Question
Given the limitations of currently used robotic energy delivery devices, novel innovations have plenty of scope to ameliorate existing technology. As such, the following research question was generated:
How do new robotic systems and instruments aim to improve access and energy delivery to target tissues?
Aims
- To review existing literature to evaluate existing energy delivery methods in robotic head and neck surgery.
- To identify key areas of development in energy delivery, through new energy devices and new robotic systems.
- To discuss potential future innovations in “the ideal robotic energy delivery device”.
Search Strategy
MEDLINE was searched in November 2019 and two separate searches were carried out. From preliminary literature scoping, LASER was cited as a key energy device to review; therefore, a search was performed focusing on this. Similarly, a separate search was carried out to obtain literature surrounding next-generation robots used in TORS.
For the LASER search, keywords used were:
- Transoral* or TORS or trans-oral*
- Head adj2 neck
- Head and neck surgery
- Robotic surgical procedures
- Robot*
- 1 or 2 or 3
- 4 or 5
- Laser
- 6 and 7 and 8
For the next-generation robots search, keywords used were:
- Transoral* or TORS or trans-oral*
- Head adj2 neck
- Head and neck surgery
- Robotic surgical procedures
- Robot*
- Flex or Versius or Verb or Sport or da Vinci SP
- (((Cambridge medical or Johnson) adj1 Johnson) or Titan or Intuitive or Medrobotics) and robot*
- 1 or 2 or 3
- 4 or 5
- 6 and 9
- 8 and 10
- 7 and 8 and 9
- 11 or 12
MeSH terms were trialed in initial design of the search strategy; however, due to the relative novelty of the subject area, MeSH terms available were generating inferior search results compared to keywords alone. A decision to search using keywords only was therefore made, to maximize search quality and inclusion of relevant studies.
Results were restricted to English-language studies only. Covidence was used for screening, removal of duplicate studies, and subsequent exclusion of papers by abstract screening. Studies were excluded from both searches if they included pediatric patients, did not pertain to head and neck surgery, did not discuss energy devices, or did not include TORS patients. Full-text articles were screened after short-listing, prior to commencing the review.
Figures 1 and 2 show results breakdowns of both searches.
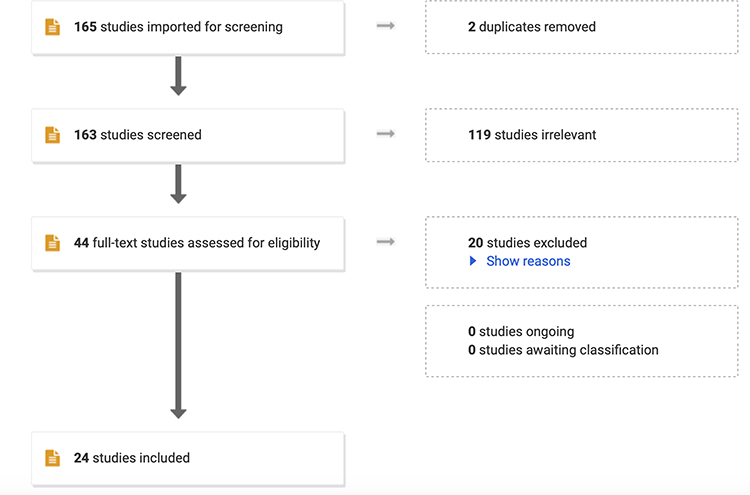 |
Figure 1 LASER search. |
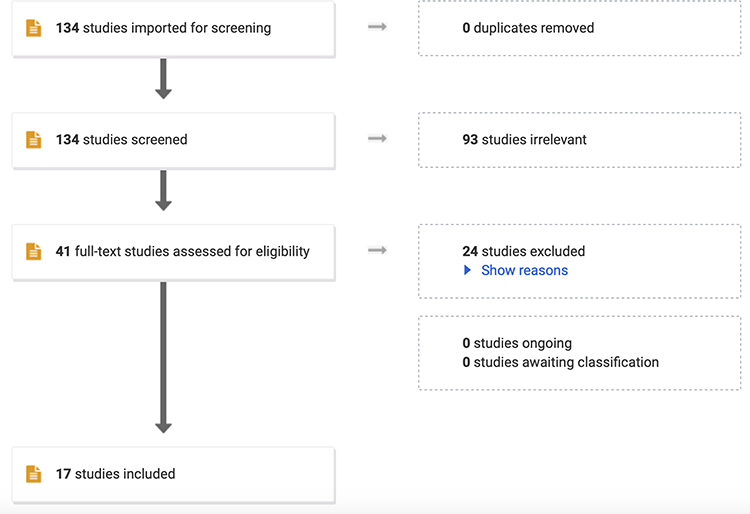 |
Figure 2 Next-generation robots search. |
Additional literature was identified by evaluating the references in included papers through snowballing. Finally, a search of gray literature was carried out to ensure that the latest available data concerning TORS were included that may not have been previously published in peer-reviewed journals.
Importance of Disease-Free Margins
There is great emphasis on the importance of negative margins in patients undergoing TORS for head and neck cancer. Over one-third of surgical cases have positive margins due to tumor infiltration or due to anatomical restrictions on the resection secondary to nearby critical structures.13 If positive margins are seen, residual disease may lead to locoregional recurrence, and therefore subsequently directs decisions regarding treatment escalation. As a result, there has been abundant interest in the impact of surgical approach on margin status.
A systematic review and meta-analysis by Gorphe and Simon was published in November 2019, which assessed the incidence of positive surgical margins in TORS for oropharyngeal cancer and attempted to identify the factors associated with positive margins.14 Amongst a rather heterogeneous 42 articles included, the total rate of positive margins in conventional trans-oral surgery, TLM, and TORS was 7.8%; however, there was a broad range of what defined a positive margin. Four articles reported specific margins of disease-free tissue around the tumor of between 10 and 15 mm, another 14 papers classified margins as “positive”, “close”, or “negative”. Definitions of even these terms varied, however, or were even absent, and the final 28 studies reported margins as just “positive” or “negative”. Positive margins were associated with poorer locoregional control (OR 3.651 [1.691, 7.882]), although the five included studies which provided data on this were heterogenous, with an I2 value = 93.4%. The use of intra-operative frozen sections reduced the risk of positive margins. Conversely, T4 disease was related to an increased risk of positive margins. Due to the short-term follow-up periods in most studies included in the review, the impact of margins on disease-free survival and overall survival was not available for analysis. An evaluation of the energy device used for tumor dissection was not performed in terms of effect on margins and the review regrettably did not directly compare the difference in margin status between different surgical approaches (trans-oral versus TLM versus TORS).
A further evaluation was subsequently carried out by Hanna et al to compare negative margins and overall survival rates between patients undergoing TORS, TLM, and conventional trans-oral surgery.15 This retrospective analysis of 1780 patients in the US National Cancer Database with T1 and 2 laryngeal squamous cell carcinoma found that TORS patients had a lower rate of positive margins than open surgery (when compared to open surgery [TORS: HR 1.56, p = 0.05], [TLM: HR 1.52, p = 0.05]). The highest 5-year overall survival was in the TORS cohort. The authors therefore concluded that the impact of TORS on negative margins was similar to that of TLM, demonstrating both feasibility and an impact on overall survival.
A further recent retrospective analysis of the US National Cancer Database (2010–2014) by Li et al also aimed to compare oncological outcomes for patients who underwent TORS with those having conventional trans-oral surgery or TLM.16 Of the 2224 patients with oropharyngeal squamous cell carcinoma, TORS patients were less likely to have positive margins than conventional trans-oral surgery, however still more likely than TLM patients ([conventional trans-oral surgery: HR 1.51, p<0.001], [TLM: HR 1.13, p = 0.582]). Furthermore, TORS patients were less likely to require post-operative chemoradiotherapy than TLM and conventional trans-oral surgery ([conventional trans-oral surgery: HR 2.07, p<0.001], [TLM: HR 1.65, p<0.001]). As a consequence, the authors concluded that TORS patients are less likely to require adjuvant treatment, resulting from their lower rate of positive margins.
An instrument used in TORS that can minimize the rate of positive margins would therefore be highly desirable, for its impact on treatment de-escalation, and ensuing impact on survival rates. Due to the properties of different energy devices, this review will go on to discuss the impact on margins of the various instruments compatible with TORS.
Energy Delivery in Trans-Oral Surgery
Monopolar Energy
Monopolar energy remains the most widely used dissection tool in TORS.3 It is widely recognized, however, to cause significant collateral tissue damage, which can in turn affect nearby structures and resultant clinical outcomes.11 Secondary to energy transmission to tissue, pain and tongue swelling can be a significant challenge. Additionally, tissue sticking to the spatula tip can prove problematic, as frequent cleaning of debris every few cuts substantially increases operating time.17 Monopolar can be incorporated into the existing da Vinci through either monopolar scissors or spatula, both of which are widely used in TORS.
Bipolar Energy
Bipolar electrocautery has also proven a useful tool in TORS. It facilitates good hemostasis; however, this can be limited by the relative size of the instrument in relation to space confines of the deep tissues of the head and neck. On the other hand, less energy is transmitted through the body of the instrument, enabling more precision when bipolar forceps are utilized.
Radiofrequency Energy
Radiofrequency is cited as an alternative modality for facilitating dissection and hemostasis in trans-oral surgery. Due to the reduced tissue resistance compared to CO2 LASER and monopolar, a narrower coagulation zone is produced.11 It can be used in volume-reduction surgery, where tissue bulk is of importance; obstructive sleep apnea surgery is a prime example of this. Radiofrequency uvulopalatoplasty and/or tongue base reduction have been well described.18
Radiofrequency has been further demonstrated in a 25 patient case series, with both benign and malignant lesions.19 In this study, intra-operative bleeding and tissue sticking were minimal, and the area of collateral coagulation was negligible. The authors also reported that specimens could be better assessed by their blinded histopathologist than their LASER counterparts (p<0.001). A significant limitation of this study, however, was that the operating surgeon self-reported their results, leading to an element of reporting bias.
LASERs
LASER is a widely utilized tool in surgery, harnessed for its cutting precision. Before discussing the use of LASERs in TORS, it is imperative to hold a basic understanding of how they work. Via stimulated emission, excited electrons release energy inside a chamber with mirrors at each end.20 To prevent energy decay as light bounces between the two mirrors, a gain medium is required to add energy back into the system. Eventually, some light escapes as a focused beam, which provides the action of the LASER.
Gain media are typically solids or gases. Solid crystal structures are heat resistant and stable, such as YAG.20 Gases do not distort the LASER beam in the same manner as solids do and can be easier to create. CO2 is a widely used gas LASER in ENT.
As a LASER operates at incredibly high power, naturally an element of energy is lost as heat, reducing the efficiency of the LASER. This also has the potential to heat up surrounding tissue causing collateral thermal injury.
Prior to the introduction of hollow wave guides, CO2 LASER could not be used in TORS, as a microscope was required for attachment to the delivery system. Now, LASER can be easily used in TORS and has been harnessed for its ability to dissect tissue without direct contact. Feasibility with the da Vinci was first demonstrated in 2007, in cadaver and animal models by Solares et al,21 followed by human use in 2012.22 It is thought to be easy to use, has a good hemostasis profile, and causes less tissue injury compared to cold steel or electrocautery.23,24 It is, however, relatively more costly than traditional electrocautery, due to the expense of LASER fiber maintenance and calibration. Furthermore, there is no aiming beam when used with the da Vinci and no coherence, greatly impacting on LASER precision.
Thulium: yttrium, aluminum, and garnet (Tm:YAG) LASER was first reported in endolaryngeal surgery in 2006.25 This continuous flexible LASER generated a 50% more collateral heat damage than the CO2 LASER, but importantly, less than electrocautery. Zeitels et al found that Tm:YAG was superior to CO2 in inducing hemostasis. Tm:YAG therefore offers an excellent compromise by being superior to other cutting and ablating LASERs for hemostasis, whilst minimizing the excessive collateral heat damage seen with electrocautery. It works similarly to the CO2 LASER, where the chromophore is water.26 This results in rapid absorption by target tissue, thereby limiting thermal damage to surrounding tissue. Feasibility has since been demonstrated in TORS patients.27 The presence of an aiming beam is thought to be a major advantage compared to CO2 LASER. The fiber needs to be very close to target tissue, however, and burns frequently, requiring refreshing of the cutting tip. Precision is also reduced compared to CO2 LASER.
Ligasure
In comparison to the aforementioned energy delivery devices used for a combination of dissection and hemostasis, Ligasure is primarily a vessel sealant device. Its mechanism of action is through applying pressure and lower bipolar energy over a vessel to achieve vessel fusion. Its manufacturer states that it can be used in vessels up to 7 mm in diameter.28
Although direct comparison studies of Ligasure versus other energy devices in robotic surgery are somewhat limited in the head and neck, other specialties have evaluated its use. In their in vitro study evaluating lateral heat spread using Ligasure versus monopolar, Ligasure was found to have less critical thermal spread compared to monopolar.29 The study also found that the use of a Maryland clamp as a means of containing heat spread was effective; however, the application of this to TORS is somewhat limited, due to the space confines when operating in the head and neck and requirement for a thicker arm.
Similarly, although there are no known studies comparing the effect of Ligasure to other energy devices used in the head and neck on tissue margins, a small non-randomized study of 30 patients compared Ligasure to cold steel, monopolar, and bipolar dissection for breast malignancies.30 Ligasure was found to be non-inferior to the other instruments used in terms of thermal damage. The need for a well-designed study in a cohort of patients undergoing TORS is therefore highlighted, given the huge importance of protecting surrounding delicate structures in the head and neck, and the relationship between this and the consequential impact on post-operative function. Currently, Ligasure is only compatible with the da Vinci X and XI, but not the latest SP model. It is also difficult to use as a cutting tool, especially for mucosa, given that its tip is short and thick.
Harmonic Scalpel
The Harmonic scalpel is another novel device that has proved popular as a vessel sealant, whose properties have been harnessed for use in TORS. Unlike previously discussed devices, it works using ultrasound. Ultrasound waves cause tissue friction at a cellular level, giving rise to changes in protein structure, denaturation, and eventually causing coagulation. Similarly to the Ligasure, it can be used in vessels up to 5 mm.31
When compared to other vessel sealing devices, the Harmonic achieves faster sealant.32 In thyroidectomy, this has been shown to lead to a reduction in operating time, compared to the Ligasure.33,34 In a cadaver study on tongue tissue, however, Hanby et al showed increased thermal damage using the Harmonic, compared to CO2 LASER (p = 0.003),24 indicating that perhaps shorter operating time sacrifices improved tissue resection margins and less collateral thermal damage.
Currently, there is a Harmonic attachment that is compatible with the da Vinci X and XI, but not the latest SP model.
Novel Developments in LASERs
CO2 LASER has proved to be a predictable and precise instrument to use in the head and neck, achieving good hemostasis with minimal collateral heat damage. A previously recognized significant limitation of the use of CO2 LASER in TORS lay in delivering it outside the line of sight. In its conventional design, a CO2 LASER could only travel in a straight line, in contrast to Tm:YAG LASER.
As CO2 LASER lies in the (non-visible) infra-red part of the electromagnetic spectrum, directing the beam requires a small joystick attached to a microscope joined with a visible guidance beam, to represent the desired point of LASER contact.35 Should the target site be out of direct sight due to anatomical confines (eg, large tongue, obesity, spinal immobility), the CO2 LASER becomes an unsuitable instrument to use. Tm:YAG LASER offers an alternative energy source, through the use of a flexible fiber to direct its beam around a corner, however, proves more costly and less precise when compared to CO2. Due to the heat generated and loss of energy to surrounding regions, it was previously not possible to incorporate CO2 LASER delivery into a fiber.
A photonic bandgap fiber was therefore developed by OmniGuide (OmniGuide, Cambridge, MA, USA) in 1998 to circumvent this difficulty.12 It works by delivering LASER energy through a reflective tube with a hollow core. This tube is lined by a dielectric mirror, made of a combination of high and low refractive index substances, which directs light along the hollow core of the fiber.35 A metal sheath protects the end of the fiber from debris. Helium also runs through it, to further minimize debris and smoke, in addition to cooling both the fiber and target tissue. OmniGuide permits LASER use in both pulse and continuous modes. CO2 LASER energy is then taken up by water inside the tissue, leading to vaporization of surface cells.
The FlexGuide ULTRA (OmniGuide, Cambridge, MA, USA) is a later iteration of the tube used specifically in TORS. It offers articulation with robotic instrument arms and is suitable for multiple usage. A BeamPath fiber lies inside the FlexGuide ULTRA to deliver CO2 to the target tissue. In a small case series of six patients, Mattheis et al evaluated the feasibility of this flexible CO2 LASER for treatment of head and neck malignancy.36 They compared cutting properties, duration of surgery and hemostasis to retrospective data on 17 patients who had undergone resection with electrocautery or Tm:YAG LASER. The authors demonstrated feasibility of the flexible CO2 LASER and showed a smaller zone of coagulation, thereby facilitating clear resection margins without compromising healthy tissue.
Similarly, Durmus et al further demonstrated the feasibility of the flexible CO2 LASER (OmniGuide, Cambridge, MA, USA) with TORS for hypopharyngeal cancer in a group of five patients in 2015,37 following a previous case report by Kucur et al using CO2 LASER with TORS for hypopharyngeal cancer in 2014.38 Durmus et al reported that all of their TORS resections using a flexible CO2 LASER were completed en bloc, with no positive margins and minimal-associated peri-operative morbidity. On closer inspection of the paper, however, only two of the five patients included actually underwent LASER resection of their tumor; the other three had their tumors dissected with electrocautery. The rationale for choosing LASER versus electrocautery for tumor dissection and the difference in their subsequent functional outcomes was unclear.
The integration of improved CO2 LASER technology into TORS has great potential. In a previously performed direct comparison study between TLM and TORS using electrocautery, TLM proved superior in terms of margin evaluability, post-operative pain, and length of feeding tube placement.39 This study, however, used electrocautery for TORS dissection and reported significant issues with resection margins due to collateral thermal damage. One can postulate the effect of electrocautery also impacted substantially on the amount of post-operative pain, and preservation of swallow, as previously discussed. With the advent of flexible CO2 LASER fibers that can be integrated into the da Vinci, it is therefore likely that these differences between TLM and TORS will be minimized. Overall survival and disease-free survival have already been shown to be equivocal amongst TLM and TORS patients with supraglottic cancer in a non-randomized study.40 Similarly, non-inferiority in terms of survival has been demonstrated in a meta-analysis for hypopharyngeal squamous cell carcinoma, comparing TORS to TLM.41 Further randomized studies to assess this are certainly required; however, lack of precision in flexible CO2 LASER remains a problem.
Finally, new wavelength LASERs are undergoing clinical feasibility studies to assess their use in head and neck surgery. One particularly promising LASER is the so-called “blue LASER”. At 445nm wavelength, it has been well recognized for its dual photoangiolytic and cutting properties; the first of its kind.42 It can also carry high energy up to 15 Watts. This could therefore usurp the current use for the CO2 LASER for vascular tissue, by offering a superior device for not only cutting but also for hemostasis. Although it is yet to be TORS compatible, this would undoubtedly be a useful tool to incorporate into new robotic systems. Beam divergence, however, has been cited as a problem with the blue LASER, leading to the LASER defocusing the further away it was from target tissue. Similarly, a small coagulation zone was only seen when the LASER was in close or direct contact with tissue, akin to Tm:YAG LASER. This suggests the need for integration with a flexible waveguide (should this be feasible) to enable its use in TORS for cancer, by permitting close contact with the deep tissues of the head and neck.
Comparison of Current Energy Devices Used with the da Vinci
Surprisingly, there is a paucity of literature comparing existing TORS instruments that can be used for dissection, perhaps due to the relative novelty of TORS in relation to other approaches in head and neck surgery. The most well-conducted study is from 2014 by Hoffmann et al which aimed to compare dissection methods in an animal model, looking at CO2 LASER versus Tm:YAG LASER versus monopolar blade versus radiofrequency, commenting on their advantages and disadvantages.11 The authors evaluated the width of incision, in addition to the area of tissue coagulated. Furthermore, performance (split into bleeding, tissue sticking, coagulation, user-friendliness, and speed) was assessed. Overall, they found that the radiofrequency needle showed the best cutting profile, with a smaller collateral heat dispersal, and was therefore superior in preserving adjacent structures. The performance was best using CO2 LASER and radiofrequency. The most bleeding was seen when monopolar was used, and monopolar was also the greatest culprit for tissue sticking to it, echoing previously referenced studies. Conversely, radiofrequency only required instrument activation to gently release stuck tissue, although the frequency of stuck tissue was higher than in other energy devices. More extensive collateral coagulation was seen using radiofrequency, Tm:YAG LASER and the monopolar blade, compared to minimal coagulation using the CO2 LASER. Similarly, CO2 LASER and radiofrequency were the most time-efficient. Financially, monopolar and radiofrequency were the cheapest modalities. An important criticism of this paper lies in its evaluation of performance. Two head and neck surgeons evaluated the five measured domains on a visual analog scale; however, there was no mention of the assessment of inter-rater reliability in the article.11 There is therefore risk of disparity between scores given, potentially leading to heterogenous results.
In comparison to the previous paper which focused on malignant resections, a non-randomized prospective study by Karaman et al compared flexible CO2 LASER to monopolar energy in tongue base surgery for obstructive sleep apnea.17 In their small cohort of 20 patients who underwent surgery using the da Vinci, intra-operative bleeding, operating time, length of stay, duration until oral intake, post-operative pain, post-operative airway complications, Apnea–Hypopnea index scores (AHI), and Epworth Sleepiness Scale scores (ESS) were assessed. Follow-up was not standardized but had a mean of 12 months. CO2 LASER resulted in less bleeding (p<0.001), shorter duration of surgery (p<0.001), shorter length of stay (p<0.001), faster resumption of oral intake (p<0.001), and less post-operative pain (p<0.001), with a greater improvement in AHI (p<0.001). There was no significant difference, however, between ESS in the CO2 LASER and monopolar groups. The study was non-randomized and allocated treatment arms based on patient preference; the first 10 patients who accepted the higher cost of the CO2 LASER were placed in that arm, introducing a large element of allocation bias.
A further study conducted by Van Abel et al compared the outcomes of Tm:YAG LASER used in TORS for patients with head and neck malignancy against electrocautery.43 This prospective cohort study evaluated 15 patients having a TORS resection using Tm:YAG LASER (Revolix Jr, LISA Laser, Katlenburg-Lindau, Germany) with 30 control patients who had electrocautery TORS. The study demonstrated feasibility for Tm:YAG in achieving negative margins. Additionally, blood loss was <150 mL for 87% of Tm:YAG patients versus in 63% of electrocautery patients. Intra-operative pharyngotomy occurred in 8% of Tm:YAG patients versus 42% electrocautery patients. Post-operative pain was also reported to be significantly worse in the electrocautery group (p = 0.02). No significant difference in hemostasis was found. Due to the reduced (albeit non-statistically significant) collateral thermal damage seen in the Tm:YAG cohort (p = 0.06), the authors hypothesized that this was the rationale behind reduced post-operative pain in the Tm:YAG cohort.
Increased collateral thermal damage when using electrocautery compared to LASER is also cited as the justification behind the superior outcomes seen for LASER TORS in another recent paper.44 In 2019, Benazzo et al published a non-randomized retrospective study which compared monopolar electrocautery against Tm:YAG (Revolix Jr, LISA Laser, Katlenburg-Lindau, Germany) and flexible CO2 LASER (OmniGuide, Cambridge, MA, USA) for all 20 patients with T1 or T2 oropharyngeal and supraglottic squamous cell carcinoma treated with TORS in their unit between 2010 and 2019. Nine patients had LASER-TORS (Tm:YAG n = 8, CO2 n = 1) and 11 underwent monopolar TORS, both using the da Vinci, but were not randomized to each arm. Positive or close margins were more common in electrocautery patients (p = 0.028). Moreover, length of stay, duration of nasogastric feeding, and tracheostomy removal were prolonged in the monopolar cohort (p = 0.04, p = 0.04, and p = 0.05, respectively). Given that only one patient underwent LASER TORS using CO2, no comparison was made between outcomes in this patient and others undergoing Tm:YAG LASER TORS, which is a limitation of this paper. In summary, this paper provides strong evidence further endorsing LASER use in TORS, to minimize the rate of positive margins and improve functional outcomes, however it does not offer conclusive evidence regarding choice of gain medium. Well-powered randomized controlled trials are needed to generate higher-quality evidence to further corroborate these conclusions.
Energy Delivery via the FLEX Robotic System
Undoubtedly, the development of flexible LASER technology has helped to overcome some pre-existing challenges of acquiring surgical access to the deep structures of the head and neck using the da Vinci robotic system. Since the recent patent expiration of the da Vinci, newer robotic systems have been released onto the market, showing great promise in further overcoming the ongoing challenges seen with energy delivery in TORS.
One such system is the FLEX robotic system (Medrobotics Inc, Raynham, MA), which has received the most attention in recent literature. It is the first machine developed specifically with TORS in mind, and through a single port, it uses a rigid endoscope and two flexible instruments, thereby improving surgical access. Adjustment can be made to transition from semi-rigid to flexible, through manipulating tension of the cables within it.45 The system can be steered by the operating surgeon by enabling the outer parts to protrude by further changes in cable tension. This enhances the maneuverability of the compatible instruments, facilitating access to the larynx and hypopharynx.46 Both electrocautery and LASER can be incorporated, permitting a choice of energy device.
Its use in the larynx was first demonstrated in 2012 when Rivera-Serrano et al demonstrated trans-oral visualization of the larynx without laryngeal suspension.47 The FLEX robotic system has since received validation in cadavers.48–50 After receiving a CE mark in Europe in 2014, the first human procedures were performed using the FLEX robotic system,45,51 after which it subsequently received FDA approval in 2015.
A case report by Schuler et al reported the successful use of the FLEX robotic system for the treatment of a T2 squamous cell carcinoma of the lateral wall of the oropharynx in a 54-year-old male.52 Monopolar was used for dissection, achieving a margin of 5–10 mm. The authors reported an episode of arterial bleeding in the bed of the tumor, which was successfully controlled with further monopolar. The tumor was successfully removed en bloc and histopathological analysis revealed negative margins. Given that this was one of the first case reports using the FLEX, evaluation of coagulation zone, operating time, and other such factors were not recorded, nor compared to the effect of monopolar energy used with the da Vinci. The authors astutely mentioned this in their discussion and highlighted it as an area of future research.
In 2014–2015, a further study by Mattheis et al recruited 40 patients and evaluated the feasibility and performance of the FLEX in both benign and malignant diseases in a prospective non-randomized study.53 Of the 40 patients, 11 underwent endoscopy and biopsy, and the remaining 29 had a resection. Either monopolar or a flexible CO2 LASER (Lumenis AcuPulse DUO, Lumenis, Yokneam) was used for cutting; however, the individual difference in outcomes between instruments was not evaluated. One patient undergoing a resection did have positive margins, and underwent subsequent secondary TLM; again, the method of dissection was not specified.
Lang et al have also published results of a multi-center, prospective study evaluating the safety and efficacy of the FLEX in 80 patients.54 Forty-one patients underwent complete tumor resection, 31 patients had a biopsy only and the remainder were converted to TLM primarily due to inadequate access. For cutting, monopolar needle knife, monopolar cautery, or a flexible CO2 LASER (Lumenis AcuPulse DUO, Lumenis, Yokneam) were used with the FLEX system. One patient with a lateral oropharyngeal wall tumor experienced moderate intra-operative bleeding, requiring abandonment of the FLEX system and hemostasis with alternative rigid instruments. Otherwise, hemostasis was achieved in all other patients using flexible monopolar (either via monopolar spatula or Maryland dissector) ± trans-oral rigid monopolar suction cautery or endoscopic clips. No further detail was provided regarding which patients required rigid instrumentation or clips to achieve hemostasis, which would have been valuable. The authors, however, did suggest future development of integrated flexible bipolar tools and a clip applicator to minimize the requirement of this (something also of potential benefit to the da Vinci). Exploring the factors which led the surgeons to switch to rigid monopolar or clips would be beneficial scope for further research. The use of flexible instruments was cited as being more ergonomic and seamless for intra-operative instrument exchange, compared to the da Vinci. Furthermore, the flexible CO2 LASER and monopolar knife permitted resections at varying angles; not just limited to the line of sight. The flexible LASER also facilitated guiding the tip close and parallel to the target tissue, allowing the spot size of the LASER to be as small as possible.
An additional retrospective, multi-center study in the United States similarly evaluated outcomes in patients undergoing surgery using the FLEX system between 2015 and 2017.55 Thirty-one out of 68 patients had a resection, as opposed to biopsy. The authors demonstrated superior results in terms of hemostasis in comparison to previous TORS studies. Hemostasis was achieved in all patients using primarily bipolar and monopolar suction cautery, which albeit were not integrated FLEX instruments but none required removal of the robot to permit usage. Some larger vessels needed surgical clips, but again, robot removal was not required. Length of stay in cancer patients was 2.45 days (inclusive of resections requiring neck dissection and/or tracheotomy, in addition to biopsies) and for benign disease, 0.64 days. Six patients were readmitted in the first month after surgery, due to dysphagia (n = 1) or post-operative bleeding (n = 5). Overall, this large case series demonstrated that bipolar cautery and endoscopic clips are feasible for insertion alongside the FLEX system for hemostasis. Similar to the aforementioned studies on the FLEX system, this highlights an area for ongoing research to investigate whether improved agents for hemostasis can be incorporated into the robot, thus alleviating the requirement for insertion of rigid instrumentation when bleeding occurs.
In terms of impact on surgical margins, there are few studies thus far using the FLEX that have commented on this. Twenty patients who underwent surgery using the FLEX have been evaluated in a case series performed by an experienced robotic center in Adelaide, Australia.56 Eleven patients had surgery for cancer, and of these, nine had oropharyngeal squamous cell carcinoma. Monopolar was used for dissection in all cases. This resulted in a subjectively clear operative field and cleanly dissected specimens for histopathological evaluation. Eight out of nine patients had disease-free margins, and four out of these nine did not require any adjuvant treatment, demonstrating the importance of negative margins on treatment de-escalation. In the future, direct comparison of margins achieved with the FLEX system versus the more well-established da Vinci technology would be helpful to demonstrate equivalence or superiority. Likewise, comparison between margins achieved with monopolar and CO2 LASER FLEX instruments would be of interest, and additionally, the consequent impact of these treatment escalation/de-escalation.
Overall, the FLEX system is showing great promise in overcoming some of the previous physical challenges in energy delivery to the head and neck via TORS. Initial studies have demonstrated encouraging results; however, a number of important outcomes are yet to be adequately measured. These include the impact of the FLEX system on tissue margins in malignant disease and the effect of different FLEX compatible instruments (namely monopolar cautery versus CO2 LASER) on both zone of coagulation and hemostasis.
Energy Delivery via the da Vinci SP
The original iterations of the da Vinci robot have thus far proved a useful tool in head and neck surgery. The ratio of the large instruments to the anatomical confines of the head and neck, however, make for difficult ergonomics, as the machine was never designed with the head and neck in mind. A novel flexible single-port robot has now been developed by Intuitive Surgical Inc. known as the da Vinci SP (Intuitive Surgical®, Sunnyvale, California), which was first tested in urological surgery in 201057 and has since been further tested in pre-clinical studies in the head and neck.58–60 These studies have demonstrated that the da Vinci SP could be deployed with minimal instrument collision or restriction of arm movement; a promising feature for energy delivery to target tissues. Currently, electrocautery using monopolar and bipolar is permissible, but to our knowledge, LASER attachments are yet to be developed for the da Vinci SP.
The surgeon console matches the standard da Vinci system, except for an additional pedal for control of the instrument arm. Similarly, the patient side cart is the same, except the instrument arms have been modified to permit single port access. The da Vinci SP’s instruments are longer, have an extra joint to form an “elbow” and incorporate a serpentine configuration.
A non-randomized trial assessing 21 patients with laryngeal and pharyngeal lesions undergoing TORS with the da Vinci SP was carried out in Hong Kong, published in 2019.61 Eight of these patients had malignant disease, seven of which were in the oropharynx. Of this cohort, six out of seven patients had HPV positive squamous cell carcinoma. They all achieved negative margins using monopolar for dissection. Pain post-operatively was typically most intense after two weeks but subsided by 30 days post-operatively. Swallowing outcomes evaluated using the MDADI score were comparable to other studies using the standard da Vinci.
A similar study encompassing the previous Hong Kong cohort, in addition to three US centers, evaluated 47 patients undergoing TORS with the da Vinci SP.62 40 of these patients had cancer. There were no intra-operative complications and intra-operative blood loss was minimal. Two patients had a post-operative bleed, requiring a return to theatre; however, both of these were on antiplatelet therapy so were at higher risk of bleeding. As high as 96% of patients were feeding orally within 30 days. Only one patient had a positive margin (3%). The authors cited that a significant limitation of the da Vinci SP was that the instruments required further refinement to adapt to TORS. They recommended improvement of instrumentation for cutting soft tissue and hemostasis and suggested this could be achieved through a finer monopolar needle. Furthermore, they endorsed the development of a compatible CO2 LASER to assist with cutting mucosa and hemostasis; a principle well supported by the previously discussed literature concerning the standard da Vinci and FLEX.
Thus far, the da Vinci SP has demonstrated feasibility and non-inferiority to the previously released da Vinci robot; however, further development is required to adapt the machine for cutting soft tissue in the head and neck. Ongoing modifications might facilitate improved hemostasis, which could be achieved through integration of a compatible CO2 LASER.
Energy Delivery via Other Robots in Development
There are number of other new robots in development that offer potential to improve energy delivery to the head and neck during TORS. These innovations are still at early stages in their development but already show great promise in overcoming existing challenges in energy delivery.
Johnson and Johnson have made multiple announcements surrounding the launch of its new surgical robot, the Verb.63 They claim to have miniaturized existing robotic technology to a machine 20% of the size of current platforms, allowing the surgeon to get closer to the target tissue. Exactly what this will entail for head and neck surgery remains unclear, but a smaller machine with compatibility for a variety of energy devices would be an area of interest to further overcome ongoing physical challenges in energy delivery.
The Versius (Cambridge Medical Robotics, Cambridge) is now entering early clinical testing in India, including head and neck surgery.64 Although not specifically developed with the head and neck in mind, it offers a smaller, more portable machine for a significantly lower cost than the da Vinci. An array of compatible energy devices will be available; therefore, the Versius may offer improved methods of delivering energy to tissue in the head and neck. Although there is yet to be any published literature surrounding the Versius, this will be of great interest once preliminary data are available.
A final robotic system in development is the SPORT robot (Titan Medical Inc., Toronto, Ontario).65 Similar to the da Vinci SP and FLEX, the SPORT is a single-port robot which offers small diameter flexible instrumentation that could prove successful in the head and neck. Both monopolar and bipolar electrocautery are available for dissection and hemostasis. It has thus far undergone pre-clinical evaluation and is currently proceeding into next stages of testing.66
In general, although peer-reviewed literature is yet to become available on the above robotic systems, they offer some promise in advancing the field of TORS. If feasibility can be been demonstrated using these machines, further evaluation of their individual assets in energy delivery should be achievable.
Comparison of Energy Delivery by Platform
Table 1 compares energy devices compatible with the currently available trans-oral surgery platforms.
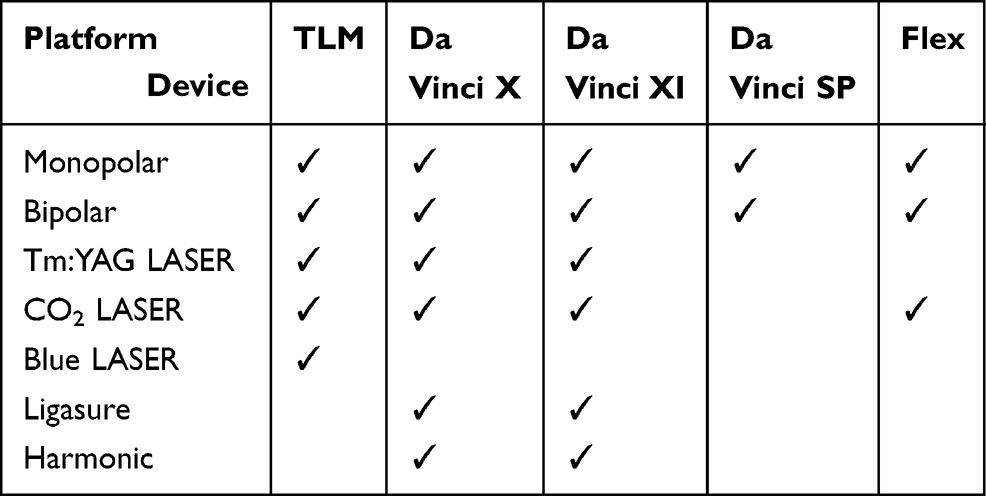 |
Table 1 Comparison of Energy Devices for Different Trans-Oral Surgery Platforms |
Table 2 reports the advantages and disadvantages of energy devices compatible with trans-oral surgery platforms.
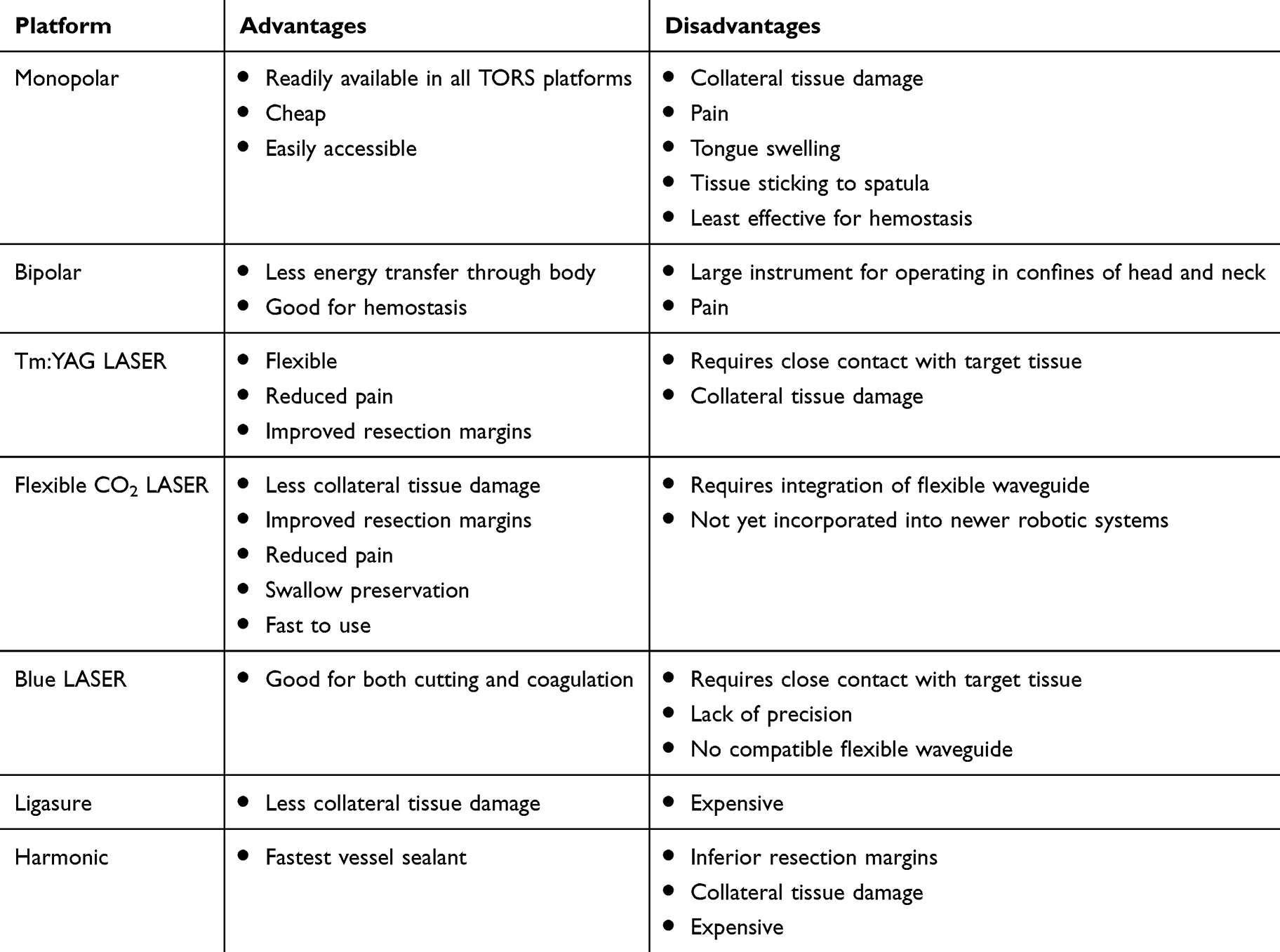 |
Table 2 Advantages and Disadvantages of Energy Devices Used in TORS |
Conclusion
Since the advent of TORS in the early 2000s, there is now a plethora of literature to support the use of various energy devices in the head and neck in both benign and malignant disease. The ability to improve the line of access for novel energy devices has revolutionized robotic surgery in the head and neck, demonstrating a significant impact on both mortality and function. Optimizing energy delivery to the head and neck offers great potential in identifying patients with malignancy who are amenable to treatment de-escalation, given the good outcomes demonstrated for margins, post-operative swallow, length of stay, etc., when appropriate energy delivery methods are selected.
There is a particularly strong body of evidence to support the use of LASER in TORS. There is no conclusive data, however, to endorse the use of CO2 over Tm:YAG LASER, with both gain media showing superior hemostatic properties, reduced post-operative pain, minimized collateral thermal damage, and most importantly, lower rates of positive margins when compared to electrocautery. Furthermore, early literature suggests that newer LASERs in development, such as the blue LASER, have the potential to be integrated into existing robotic technology, by providing an energy device that not only cuts precisely but also delivers excellent hemostasis.
Next-generation robotic systems are also offering significant potential in overcoming some of the previous challenges in energy delivery to the head and neck. The FLEX robot is now offering unparalleled access to the target tissue, and early studies have demonstrated feasibility for its use. As the FLEX is a less well-established system compared to its da Vinci counterpart, there are no comparison studies yet to demonstrate the superiority of FLEX LASER over electrocautery or other methods of energy delivery. The existing literature does support the future development of miniaturized energy devices, particularly LASER, to be incorporated into the arms of the FLEX, to alleviate the current requirement for using external instrumentation alongside the robot to provide additional hemostasis. Similarly, literature regarding the da Vinci SP also corroborates the need for integration of LASER technology into its existing design (which currently only offers electrocautery) to facilitate less collateral thermal damage, reduced rates of positive margins, and improved hemostasis. Finally, the integration of a clip applicator into existing and novel systems would also be of great benefit to enhance hemostasis.
Funding
No funding was required.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Golusinski W, Golusinska-Kardach E. Current role of surgery in the management of oropharyngeal cancer. Front Oncol. 2019;9:388. doi:10.3389/fonc.2019.00388
2. Ang KK, Harris J, Wheeler R, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363(1):24–35. doi:10.1056/NEJMoa0912217
3. O’Malley BW
4. Weinstein GS, O’Malley BW
5. NICE. Cancer of the Upper Aerodigestive Tract: Assessment and Management in People Aged 16 and Ove. London; 2016.
6. Arora A, Chaidas K, Garas G, et al. Outcome of TORS to tongue base and epiglottis in patients with OSA intolerant of conventional treatment. Sleep Breath. 2016;20(2):739–747. doi:10.1007/s11325-015-1293-9
7. Garas G, Arora A. Robotic head and neck surgery: history, technical evolution and the future. ORL. 2018;80(3–4):117–124.
8. Golusinski W. Functional organ preservation surgery in head and neck cancer: transoral robotic surgery and beyond. Front Oncol. 2019;9:293. doi:10.3389/fonc.2019.00293
9. Ibrahim AS, Civantos FJ, Leibowitz JM, et al. Meta-analysis comparing outcomes of different transoral surgical modalities in management of oropharyngeal carcinoma. Head Neck. 2019;41(6):1656–1666. doi:10.1002/hed.25647
10. von Scotti F, Kapsreiter M, Scherl C, Iro H, Bohr C. A 9-year analysis of transoral laser microsurgery (TLM) of head and neck cancer on their potential suitability for transoral robotic surgery (TORS) for estimation of future TORS-specific caseload. Eur Rev Med Pharmacol Sci. 2018;22(10):2949–2953.
11. Hoffmann TK, Schuler PJ, Bankfalvi A, et al. Comparative analysis of resection tools suited for transoral robot-assisted surgery. Eur Arch Oto-Rhino-Laryngology. 2014;271(5):1207–1213. doi:10.1007/s00405-013-2615-9
12. O’Flynn P, Awad Z, Kothari P, Vaz FM. The first UK report of the applications of flexible CO2 laser in head and neck surgery: how we do it. Clin Otolaryngology. 2010;35(2):139–142. doi:10.1111/j.1749-4486.2010.02082.x
13. Hinni ML, Ferlito A, Brandwein-Gensler MS, et al. Surgical margins in head and neck cancer: a contemporary review. Head Neck. 2013;35(9):1362–1370. doi:10.1002/hed.23110
14. Gorphe P, Simon C. A systematic review and meta-analysis of margins in transoral surgery for oropharyngeal carcinoma. Oral Oncol. 2019;98:69–77. doi:10.1016/j.oraloncology.2019.09.017
15. Hanna J, Brauer PR, Morse E, Judson B, Mehra S. Is robotic surgery an option for early T-stage laryngeal cancer? Early nationwide results. Laryngoscope. 2019;24:24.
16. Li H, Torabi SJ, Park HS, et al. Clinical value of transoral robotic surgery: nationwide results from the first 5 years of adoption. Laryngoscope. 2019;129(8):1844–1855. doi:10.1002/lary.27740
17. Karaman M, Gun T, Temelkuran B, Aynaci E, Kaya C, Tekin AM. Comparison of fiber delivered CO2 laser and electrocautery in transoral robot assisted tongue base surgery. Eur Arch Oto-Rhino-Laryngology. 2017;274(5):2273–2279. doi:10.1007/s00405-017-4449-3
18. Lim DJ, Kang SH, Kim BH, et al. Treatment of obstructive sleep apnea syndrome using radiofrequency-assisted uvulopalatoplasty with tonsillectomy. Eur Arch Otorhinolaryngol. 2013;270(2):585–593. doi:10.1007/s00405-012-2082-8
19. Hofauer B, Knopf A, Strassen U, et al. Radiofrequency resection in oral and oropharyngeal tumor surgery. Auris Nasus Larynx. 2019;47(1):148–153.
20. Rollin M. The Physics of Lasers. London: Imperial College London; July 2019.
21. Solares CA, Strome M. Transoral robot-assisted CO2 laser supraglottic laryngectomy: experimental and clinical data. Laryngoscope. 2007;117(5):817–820. doi:10.1097/MLG.0b013e31803330b7
22. Remacle M, Matar N, Lawson G, Bachy V, Delos M, Nollevaux MC. Combining a new CO2 laser wave guide with transoral robotic surgery: a feasibility study on four patients with malignant tumors. Eur Arch Oto-Rhino-Laryngology. 2012;269(7):1833–1837. doi:10.1007/s00405-011-1838-x
23. Matsumoto K, Suzuki H, Usami Y, Hattori M, Komoro T. Histological evaluation of artifacts in tongue tissue produced by the CO2 laser and the electrotome. Photomed Laser Surg. 2008;26(6):573–577. doi:10.1089/pho.2007.2217
24. Hanby DF, Gremillion G, Zieske AW, et al. Harmonic scalpel versus flexible CO2 laser for tongue resection: a histopathological analysis of thermal damage in human cadavers. World J Surg Oncol. 2011;9(1):83. doi:10.1186/1477-7819-9-83
25. Zeitels SM, Burns JA, Akst LM, Hillman RE, Broadhurst MS, Anderson RR. Office-based and microlaryngeal applications of a fiber-based thulium laser. Ann Otol Rhinol Laryngol. 2006;115(12):891–896. doi:10.1177/000348940611501206
26. Pothen AJ, Evenboer J, Swartz JE, et al. Use of the 2-μm continuous wave thulium laser for the resection of oral squamous cell carcinomas does not impair pathological assessment. Lasers Surg Med. 2014;46(8):608–613. doi:10.1002/lsm.22270
27. Benazzo M, Canzi P, Occhini A. Transoral robotic surgery with laser for head and neck cancers: a feasibility study. Orl J Oto-Rhino-Laryngology Related Specialties. 2012;74(3):124–128. doi:10.1159/000337092
28. Medtronic. LIGASURE TECHNOLOGY. https://www.medtronic.com/covidien/en-us/products/vessel-sealing/ligasure-technology.html. Published 2019.
29. Hefermehl LJ, Largo RA, Hermanns T, Poyet C, Sulser T, Eberli D. Lateral temperature spread of monopolar, bipolar and ultrasonic instruments for robot-assisted laparoscopic surgery. BJU Int. 2014;114(2):245–252. doi:10.1111/bju.12498
30. Turkan A, Akkurt G, Yalaza M, et al. Effect of ligasure, monopolar cautery, and bipolar cautery on surgical margins in breast-conserving surgery. Breast Care (Basel). 2019;14(4):194–199. doi:10.1159/000493985
31. Timm RW, Asher RM, Tellio KR, Welling AL, Clymer JW, Amaral JF. Sealing vessels up to 7 mm in diameter solely with ultrasonic technology. Med Devices (Auckl). 2014;7:263–271. doi:10.2147/MDER.S66848
32. Person B, Vivas DA, Ruiz D, Talcott M, Coad JE, Wexner SD. Comparison of four energy-based vascular sealing and cutting instruments: a porcine model. Surg Endosc. 2008;22(2):534–538. doi:10.1007/s00464-007-9619-8
33. Luo Y, Li X, Dong J, Sun W. A comparison of surgical outcomes and complications between hemostatic devices for thyroid surgery: a network meta-analysis. Eur Arch Otorhinolaryngol. 2017;274(3):1269–1278. doi:10.1007/s00405-016-4190-3
34. Garas G, Okabayashi K, Ashrafian H, et al. Which hemostatic device in thyroid surgery? A network meta-analysis of surgical technologies. Thyroid. 2013;23(9):1138–1150. doi:10.1089/thy.2012.0588
35. Holsinger FC, Prichard CN, Shapira G, et al. Use of the photonic band gap fiber assembly CO2 laser system in head and neck surgical oncology. Laryngoscope. 2006;116(7):1288–1290. doi:10.1097/01.mlg.0000227557.61978.18
36. Mattheis S, Hoffmann TK, Schuler PJ, Dominas N, Bankfalvi A, Lang S. The use of a flexible CO2-laser fiber in transoral robotic surgery (TORS). Laryngorhinootologie. 2014;93(2):95–99. doi:10.1055/s-0033-1343413
37. Durmus K, Kucur C, Uysal IO, Dziegielewski PT, Ozer E. Feasibility and clinical outcomes of transoral robotic surgery and transoral robot-assisted carbon dioxide laser for hypopharyngeal carcinoma. J Craniofacial Surg. 2015;26(1):235–237. doi:10.1097/SCS.0000000000001185
38. Kucur C, Durmus K, Dziegielewski PT, Ozer E. Transoral robot-assisted carbon dioxide laser surgery for hypopharyngeal cancer. Head Neck. 2015;37(5):743–745. doi:10.1002/hed.23860
39. Ansarin M, Zorzi S, Massaro MA, et al. Transoral robotic surgery vs transoral laser microsurgery for resection of supraglottic cancer: a pilot surgery. Int J Med Rob Comput Assisted Surg. 2014;10(1):107–112. doi:10.1002/rcs.1546
40. Asik MB, Satar B, Serdar M. Meta-analytic comparison of robotic and transoral laser surgical procedures in supraglottic carcinoma. J Laryngology Otology. 2019;133(5):404–412. doi:10.1017/S0022215119000707
41. De Virgilio A, Iocca O, Malvezzi L, et al. The emerging role of robotic surgery among minimally invasive surgical approaches in the treatment of hypopharyngeal carcinoma: systematic review and meta-analysis. J Clin Med. 2019;8(2):18. doi:10.3390/jcm8020256
42. Hess MM, Fleischer S, Ernstberger M. New 445 nm blue laser for laryngeal surgery combines photoangiolytic and cutting properties. Eur Arch Oto-Rhino-Laryngology. 2018;275(6):1557–1567. doi:10.1007/s00405-018-4974-8
43. Van Abel KM, Moore EJ, Carlson ML, et al. Transoral robotic surgery using the thulium: YAG laser: a prospective study. Arch Otolaryngology Head Neck Surg. 2012;138(2):158–166. doi:10.1001/archoto.2011.1199
44. Benazzo M, Canzi P, Mauramati S, et al. Transoral robot-assisted surgery in supraglottic and oropharyngeal squamous cell carcinoma: laser versus monopolar electrocautery. J Clin Med. 2019;8(12):2166. doi:10.3390/jcm8122166
45. Remacle M, Prasad VMN, Lawson G, Plisson L, Bachy V, Van der Vorst S. Transoral robotic surgery (TORS) with the Medrobotics Flex™ System: first surgical application on humans. Eur Arch Oto-Rhino-Laryngology. 2015;272(6):1451–1455. doi:10.1007/s00405-015-3532-x
46. Poon H, Li C, Gao W, Ren H, Lim CM. Evolution of robotic systems for transoral head and neck surgery. Oral Oncol. 2018;87:82–88. doi:10.1016/j.oraloncology.2018.10.020
47. Rivera-Serrano CM, Johnson P, Zubiate B, et al. A transoral highly flexible robot: novel technology and application. Laryngoscope. 2012;122(5):1067–1071. doi:10.1002/lary.23237
48. Johnson PJ, Rivera Serrano CM, Castro M, et al. Demonstration of transoral surgery in cadaveric specimens with the medrobotics flex system. Laryngoscope. 2013;123(5):1168–1172. doi:10.1002/lary.23512
49. Mandapathil M, Greene B, Wilhelm T. Transoral surgery using a novel single-port flexible endoscope system. Eur Arch Oto-Rhino-Laryngology. 2015;272(9):2451–2456. doi:10.1007/s00405-014-3177-1
50. Friedrich DT, Scheithauer MO, Greve J, et al. Potential advantages of a single-port, operator-controlled flexible endoscope system for transoral surgery of the larynx. Ann Otology Rhinology Laryngology. 2015;124(8):655–662. doi:10.1177/0003489415575548
51. Mattheis S, Lang S. A new flexible endoscopy-system for the transoral resection of head and neck tumors. Laryngorhinootologie. 2015;94(1):25–28. doi:10.1055/s-0034-1377008
52. Schuler PJ, Duvvuri U, Friedrich DT, Rotter N, Scheithauer MO, Hoffmann TK. First use of a computer-assisted operator-controlled flexible endoscope for transoral surgery. Laryngoscope. 2015;125(3):645–648. doi:10.1002/lary.24957
53. Mattheis S, Hasskamp P, Holtmann L, et al. Flex robotic system in transoral robotic surgery: the first 40 patients. Head Neck. 2017;39(3):471–475. doi:10.1002/hed.24611
54. Lang S, Mattheis S, Hasskamp P, et al. A european multicenter study evaluating the flex robotic system in transoral robotic surgery. Laryngoscope. 2017;127(2):391–395. doi:10.1002/lary.26358
55. Persky MJ, Issa M, Bonfili JR, Goyal N, Goldenberg D, Duvvuri U. Transoral surgery using the Flex robotic system: initial experience in the United States. Head Neck. 2018;40(11):2482–2486. doi:10.1002/hed.25375
56. Sethi N, Gouzos M, Padhye V, et al. Transoral robotic surgery using the medrobotic flex system: the adelaide experience. J Robot Surg. 2019;05:05.
57. Kaouk JH, Haber G-P, Autorino R, et al. A novel robotic system for single-port urologic surgery: first clinical investigation. Eur Urol. 2014;66(6):1033–1043. doi:10.1016/j.eururo.2014.06.039
58. Holsinger FC. A flexible, single-arm robotic surgical system for transoral resection of the tonsil and lateral pharyngeal wall: next-generation robotic head and neck surgery. Laryngoscope. 2016;126(4):864–869. doi:10.1002/lary.25724
59. Tateya I, Koh YW, Tsang RK, et al. Flexible next-generation robotic surgical system for transoral endoscopic hypopharyngectomy: a comparative preclinical study. Head Neck. 2018;40(1):16–23. doi:10.1002/hed.24868
60. Orosco RK, Tam K, Nakayama M, Holsinger FC, Spriano G. Transoral supraglottic laryngectomy using a next-generation single-port robotic surgical system. Head Neck. 2019;41(7):2143–2147. doi:10.1002/hed.25676
61. Chan JYK, Tsang RK, Holsinger FC, et al. Prospective clinical trial to evaluate safety and feasibility of using a single port flexible robotic system for transoral head and neck surgery. Oral Oncol. 2019;94:101–105. doi:10.1016/j.oraloncology.2019.05.018
62. Holsinger FC, Magnuson JS, Weinstein GS, et al. A next-generation single-port robotic surgical system for transoral robotic surgery: results from prospective nonrandomized clinical trials. JAMA Otolaryngology Head Neck Surg. 2019;19:19.
63. Johnson and Johnson. Verb Surgical. https://www.verbsurgical.com. Published 2019.
64. Cambridge Medical Robotics. 1Versius. https://cmrsurgical.com. Published 2019.
65. Titan Medical Inc. SPORT Robot. https://titanmedicalinc.com. Published 2019.
66. Seeliger B, Diana M, Ruurda JP, Konstantinidis KM, Marescaux J, Swanstrom LL. Enabling single-site laparoscopy: the SPORT platform. Surg Endosc. 2019;33(11):3696–3703. doi:10.1007/s00464-018-06658-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.