")
Back to Journals » Infection and Drug Resistance » Volume 13
Novel Carbapenem-Resistant Klebsiella pneumoniae ST147 Coharboring blaNDM-1, blaOXA-48 and Extended-Spectrum β-Lactamases from Pakistan
Authors Gondal AJ , Saleem S, Jahan S , Choudhry N, Yasmin N
Received 27 February 2020
Accepted for publication 7 May 2020
Published 2 July 2020 Volume 2020:13 Pages 2105—2115
DOI https://doi.org/10.2147/IDR.S251532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Aamir Jamal Gondal,1,2 Sidrah Saleem,1 Shah Jahan,3 Nakhshab Choudhry,4 Nighat Yasmin2
1Department of Microbiology, University of Health Sciences, Lahore, Pakistan; 2Department of Biomedical Sciences, King Edward Medical University, Lahore, Pakistan; 3Department of Immunology, University of Health Sciences, Lahore, Pakistan; 4Department of Biochemistry, King Edward Medical University, Lahore, Pakistan
Correspondence: Aamir Jamal Gondal
Department of Biomedical Sciences, King Edward Medical University, Nelagumbad Chowk, Anarkali Bazar, Lahore 54000, Pakistan
Tel +92-300-8822055
Email [email protected]
Purpose: The emergence of multidrug-resistant Klebsiella pneumoniae (K. pneumoniae) is associated with the acquisition of multiple carbapenemases. Their clonal spread is a worldwide concern due to their critical role in nosocomial infections. Therefore, the identification of high-risk clones with antibiotic resistance genes is very crucial for controlling its global spread.
Materials and Methods: A total of 227 K. pneumoniae strains collected during April 2018 to November 2019 were confirmed by PCR. Carbapenemases and extended-spectrum β-lactamases (ESBL) were detected phenotypically. Confirmation of carbapenemases was carried out by PCR and Sanger sequencing. The clonal lineages were assigned to selected isolates by multilocus sequence typing (MLST), and the plasmid analysis was done by PCR-based detection of the plasmid replicon typing.
Results: Of the total K. pneumoniae, 117 (51.5%) were carbapenem resistant (CRKP) and 140 (61.7%) were identified as ESBL producers. Intermediate to high resistance was detected in the tested β-lactam drugs while polymyxin-B and tigecycline were found to be susceptible. Among CRKP, 91 (77.8%) isolates were detected as carbapenemase producing, while 55 (47%) were positive for blaNDM-1 23.9% (n=28), blaOXA-48 22.2% (n=26) and blaVIM 0.85% (n=1) while 12.7% (n=7) carried both blaNDM-1 and blaOXA-48 genes. The CRKP coharboring blaNDM-1 and blaOXA-48 genes (n=7) were positive for blaCTX-M blaSHV (n=3), blaSHV (n=1) and blaCTX-M (n=3). The novel CRKP with the coexistence of blaNDM-1, blaOXA-48, blaCTX-M and blaSHV genes were associated with the high-risk clone ST147 (n=5) and ST11 (n=2). The assigned replicon types were IncL/M, IncFII, IncA/C and IncH1.
Conclusion: This is the first report of the coexistence of blaNDM-1, blaOXA-48, blaCTX-M and blaSHV genes on a high-risk lineage ST147 from Pakistan. This study highlights the successful dissemination of carbapenemase resistance genes in the high-risk clones that emphasizes the importance of monitoring and controlling the spread of these diverse clones globally.
Keywords: high-risk clone, New Delhi metallo-β-lactamase, MLST, K. pneumoniae, carbapenem resistance
Introduction
Accelerated emergence and effective propagation of carbapenem-resistant Klebsiella pneumoniae (CRKP) across the world have become a prominent public health challenge due to high mortality rate in healthcare-associated nosocomial infections.1,2 The CRKP has a unique ability to acquire multiple resistance encoding genes through horizontal gene transfer interceded by broad-host-range plasmids, transposons and insertion sequences thereby turning out as one of the most successful nosocomial pathogen.3 Lack of stewardship and irrational use of carbapenems for the infections of ESBL producing K. pneumoniae has led to the evolution of transmissible plasmid-encoding resistance genes that supported the selection of high-risk clones of CRKP involving diverse geographic regions and populations.4 During 2014, the World Health Organization declared CRKP as the third most critical nosocomial pathogen for future concern.5 As carbapenemases and ESBL/AmpC β-lactamases are critical in the acquisition of multidrug resistance, the identification of such broad-spectrum resistance genes is required for the development of new intervention strategies.6
Clinically important carbapenemase genes encompass blaKPC-2, blaVIM, blaIMP, blaNDM-1 and blaOXA-48.7 Global dissemination of such plasmid-encoded carbapenemases has increased alarmingly yet their geographic prevalence varies significantly.8,9 Clinical literature remains expressive about the linkage of NDM-1, most common MBL-type carbapenemase and its transmission to other parts of the world from the endemic areas of Indian subcontinent since the first isolation of blaNDM-1 producing K. pneumoniae ST14 and Escherichia coli (E. coli) in a patient treated in India and later shifted to Sweden in 2009.10 Frequent reports of NDM-1, KPC-2 and OXA-48 type carbapenemase are available from Pakistan during the past decade.11,12 Similarly, the OXA-48 is endemic in several countries since its first identification from Turkey in 2001.13 CRKP co-harboring at least two carbapenemases were reported globally such as KPC-3 and VIM-2 in Italy, NDM-1 and KPC-2 from Brazil9 and Pakistan,12 NDM-1 and OXA-48 in Morocco,14 Switzerland,15 China16 and Sultanate of Oman.17 However, the understanding of molecular and genetic context of the carbapenemases is scarce especially in the developing countries.
Carbapenemases have spread worldwide through evolution of high-risk clones by acquiring, retaining and efficiently transmitting resistance genes. Such globally identified high-risk K. pneumoniae clones for the dissemination of carbapenemases include ST258, ST11 and ST147 co-harboring broad range of plasmids. Several STs were found to be associated with blaNDM-1 producing K. pneumoniae such as ST258, ST340, ST512 and ST147 along with different plasmids IncF, IncA/C and IncL/M.9 Therefore, careful detection and treatment strategies are required especially in developing countries where carbapenemase-producing strains have diverse opportunities.
However, insufficient data are available from Pakistan that describes molecular versatility of resistance genes in relation to genetic analysis and prevalence of high-risk clones. Hence, it is imperative to promptly detect and examine these successful clones to get insights into the global spread of antimicrobial drug resistance. Therefore, the current study aimed to ascertain the prevalence of carbapenemases and to analyze their clonal relatedness.
Materials and Methods
Bacterial Collection and Identification
Clinical strains were collected during the course of routine diagnostic bacterial cultures from tertiary care hospitals of Lahore, Pakistan. A total of 227 clinical strains of K. pneumoniae were included from different sample types from April 2018 to November 2019. The isolates were characterized phenotypically by colony morphology, Gram’s staining and biochemical characteristics by using API-20E according to the manufacturer’s instructions (BioMerieux, France). The study was sanctioned by institutional review board of the University of Health Sciences, Lahore, Pakistan.
Antimicrobial Susceptibility Testing (AST)
AST was carried out by standard disc diffusion method according to the CLSI guidelines using the following antibiotic discs: imipenem (IPM), meropenem (MEM), ertapenem (ETP), ceftazidime (CAZ), ampicillin (AMP), amoxicillin-clavulanic acid (AMC), cefepime (FEP), ceftaroline (CTP), aztreonam (ATM), gentamicin (CN), amikacin (AK), ciprofloxacin (CIP), doxycycline (DO), polymyxin-B (PB), tigecycline (TGC), cefotaxime (CTX), trimethoprim-sulfamethoxazole (SXT) and piperacillin-tazobactam (TZP) (Oxoid, UK). E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as quality control strains.18
Minimal Inhibitory Concentrations (MICs)
MIC of antibiotics was determined by standard broth microdilution method using cation-adjusted Mueller-Hinton broth in accordance with CLSI guidelines with antibiotic concentrations ranging from 0.5 to 1024 μg/mL.18
Phenotypic Characterization
Carbapenemases were identified phenotypically by carbapenem inactivation method (CIM) while the detection of ESBLs was carried out by double-disc synergy test (DDST) using amoxicillin-clavulanic acid alone and in combination with ceftazidime as per the guidelines of CLSI.18
DNA Isolation from Bacterial Strains
Genomic DNA was prepared from pure bacterial culture plates by heat lysis method as reported previously and stored at −20°C for onward processing.19
Molecular Profile Analysis by Polymerase Chain Reaction (PCR)
Klebsiella species, carbapenemase resistance genes (blaNDM-1, blaVIM, blaIMP and blaOXA-48) and ESBL encoding genes (blaTEM, blaCTX-M and blaSHV) were detected through PCR using specific primers as given in Table 1. PCR reaction mixture of 50 μL consisting of 25 μL of 2x PCR Master Mix, 1 μL of each primer, 2 μL of DNA and dH2O upto 50 μL. Amplification was carried out in thermal cycler (Proflex, ABI) with different annealing temperatures given in Table 1. Agarose gel (1–1.5%) was used to resolve and analyze the PCR products. blaNDM-1 genes were further analyzed for allelic discrimination by Sanger’s sequencing method. K. pneumoniae ATCC BAA-2146 was used as NDM positive control.
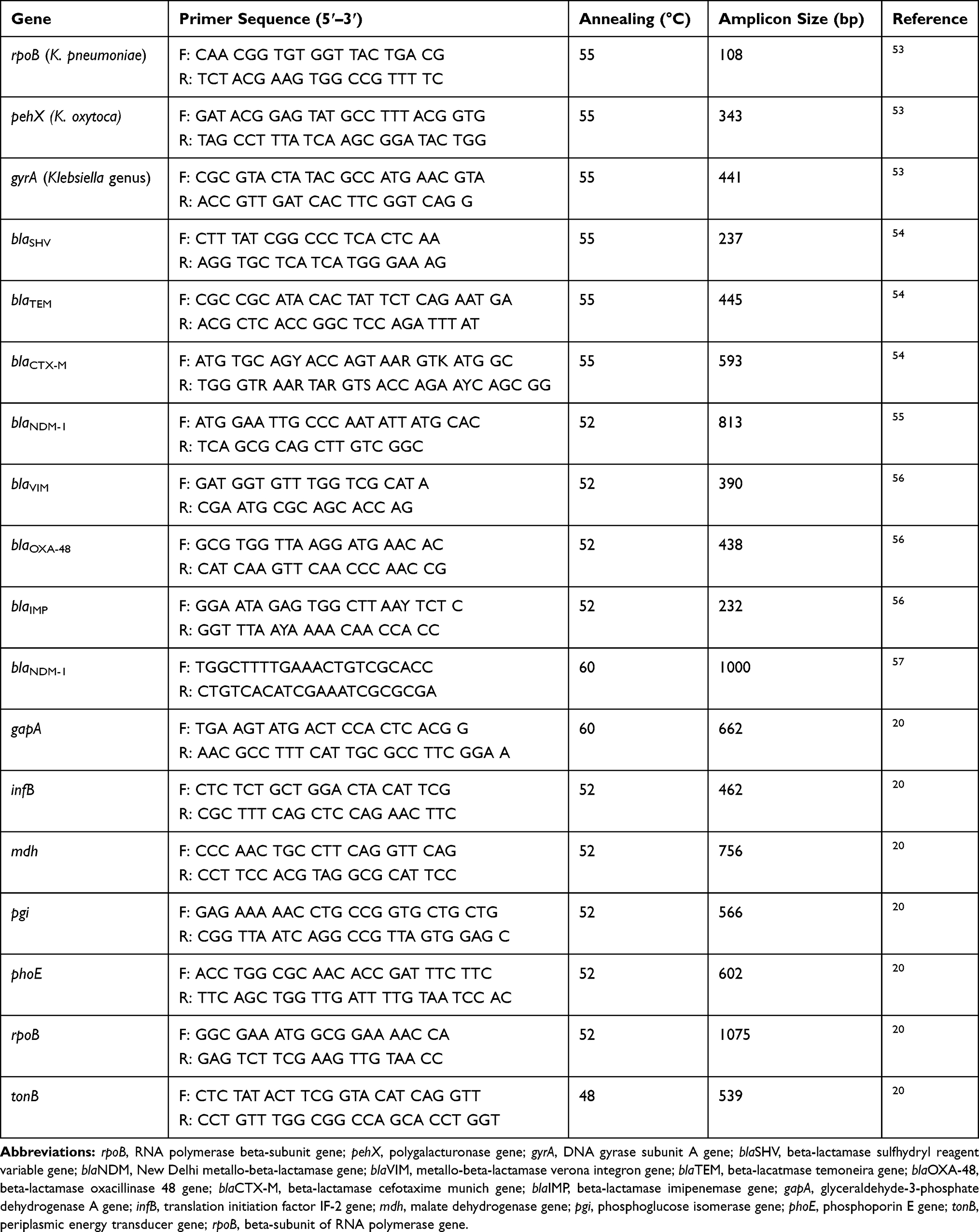 |
Table 1 Primer Sequences Used for PCR |
Multilocus Sequence Typing (MLST) of Klebsiella Species
MLST of CRKP strains coharboring blaNDM-1 and blaOxa-48 was performed using seven housekeeping genes (gapA, infB, mdh, pgi, phoE, rpoB and tonB) as described by K. pneumoniae MLST website.20 The mutation analysis of NDM-1 was carried out by cycle sequencing using specific primers given in Table 1. The cycle sequencing was performed by BigDye terminator v3.1 kit on Proflex thermal cycler while the sequencing products were analyzed through capillary electrophoresis on Genetic Analyzer AB-3500 (Life Technologies by Thermofisher, USA) as per the kit instructions. Data were analyzed by using the sequencing analysis software v6.1 and checked on basic local alignment (BLAST) at NCBI for allele identification. CRKP STs were assigned using the MLST database (http://bigsdb.pasteur.fr/klebsiella/klebsiella.html).
Plasmid Analysis
CRKP coharboring blaNDM-1 and blaOxa-48 were further analyzed for the presence of plasmids. Plasmid DNA was extracted from single colony of CRKP by using the plasmid isolation kit (Thermofisher Scientific) and DNA was stored at −20°C. The samples were run on 0.8% agarose gel for the detection of plasmids. Plasmids were classified according to their incompatibility groups by using the PCR-based replicon typing method as described before.21
Results
During the 19-month study period, 227 clinical strains of Klebsiella were identified by phenotypic and genotypic methods. Of the total, 129 (56.8%) were isolated from males while remaining 98 (43.2%) were from females. These isolates were collected from wound 29.5% (n=67), pus 17.6% (n=40), blood 15.5% (n=35), tracheal secretion 13.2% (n=30), sputum 11% (n=25), urine 7.04% (n=16) and tissue 6.16% (n=14). Isolates originated from different sections of the hospital such as general surgery 26.4% (n=60), SICU 18.5% (n=42), general medicine 15.8% (n=36), dermatology 5.72% (n=13), nephrology 4.40% (n=10), chest medicine 8.37% (n=19), cardiology 3.96% (n=9), pediatric medicine 7.04% (n=16), oncology 5.28% (n=12) and orthopedic surgery 4.40% (n=10).
Antimicrobial Susceptibility Testing and Phenotypic Confirmatory Tests
As high as 51.5% (n=117) clinical strains of K. pneumoniae were carbapenem resistant (CRKP) while remaining 48.5% (n=110) were susceptible (CS). Out of 117 CRKP, 77.7% (n=91) were detected as carbapenemase-producing strains (CPKP). Most of the CRKP exhibited resistant to intermediate resistant profile for the β-lactam combination agents, carbapenems, fluoroquinolones, aminoglycosides and trimethoprim/sulfamethoxazole. Antimicrobial resistance pattern of CRKP strains was as follows: meropenem (96.9%), imipenem (98%), ertapenem (90%), amoxicillin/clavulanic acid (93.5%), ceftazidime (91.2%), ceftriaxone (96%), cefotaxime (95%), aztreonam (90.3%), ciprofloxacin (87%), amikacin (37.1%), tigecycline (21.1%) and polymyxin-B (13.7%). The MIC values of the tested β-lactam antibiotics were as follows: 4 to >1024 mg/L for ertapenem, 8 to >1024 mg/L for meropenem, 8 to >1024 mg/L for imipenem in all tested strains. All of the isolates were recognized as MDR (72%) or XDR (28%). The MIC results of the selected strains are given in Table 2.
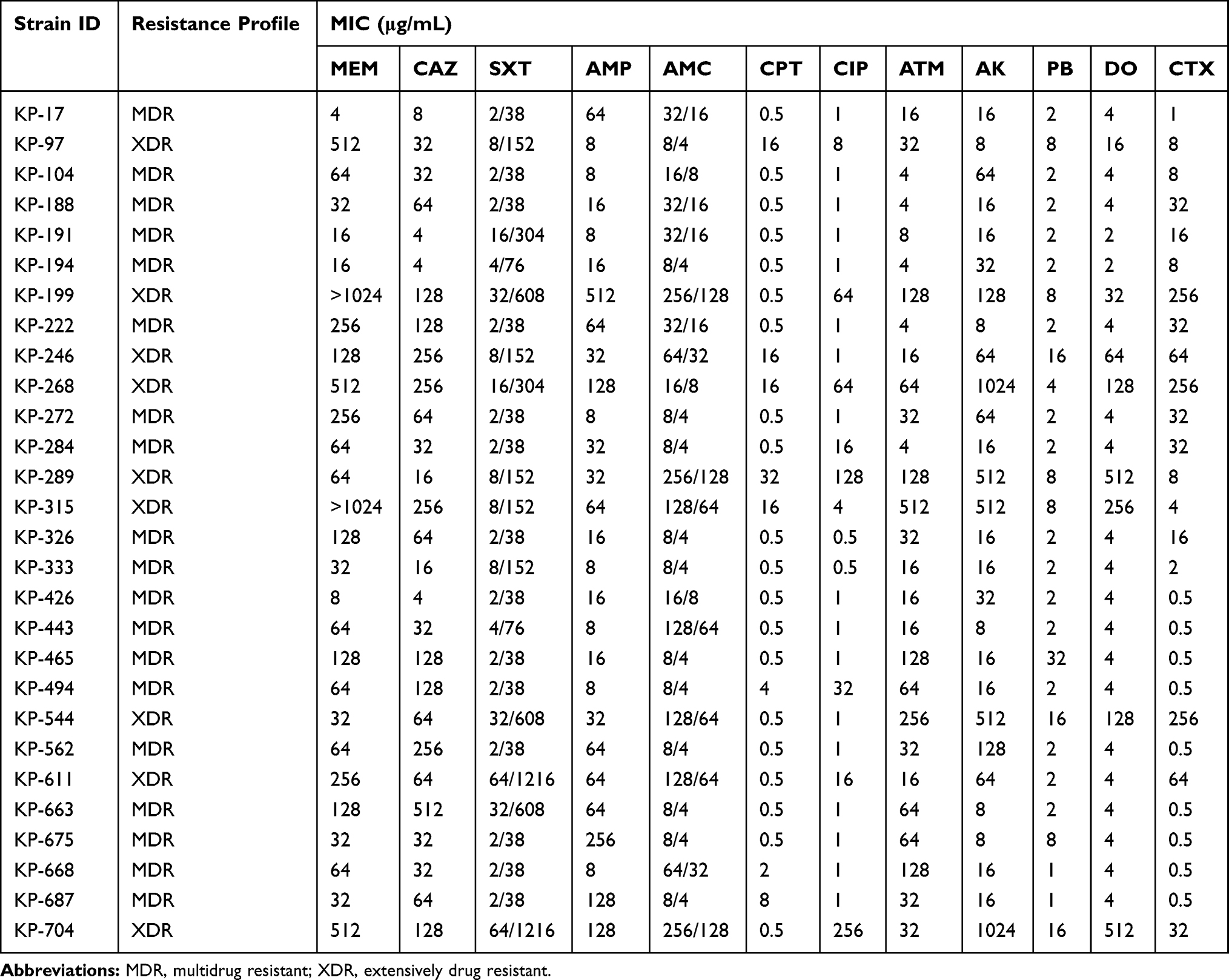 |
Table 2 MIC Values of Selected Carbapenem-Resistant K. pneumoniae Strains |
Significantly higher frequency of CPKP was observed in wound samples 49.4% (n=45; p=0.002), pus samples 27.4% (n=25; p<0.026) and tracheal secretion samples 23.2% (n=21; p=0.029). Clinical strains of CRKP from wound and pus samples were significantly associated with the general surgery (p<0.001) while those from tracheal secretion samples were significantly associated with the SICU (p=0.008) as compared to the other samples obtained from the general surgery and SICU. Out of 227 K. pneumoniae strains, 61.6% (n=140) were ESBL producers and 38.3% (n=87) were non-ESBL producers. Among the 140 strains of ESBL producing K. pneumoniae, 9.28% (n=13) isolates were resistant to one of the third-generation cephalosporins (3GCs), 28.5% (n=40) were resistant against 2 of the 3GCs and 62.1% (n=87) were resistant to all the 3GCs. Association analysis demonstrated that 80% (n=112) ESBL producers were collected from the samples of wound, pus and tracheal secretions (p=0.003).
Antibiotic Resistance Genes
Out of 117 CRKP, 47% (n=55) were positive for the carbapenemase resistance genes by PCR including blaNDM-1 23.9% (n=28), blaOXA-48 22.2% (n=26) and blaVIM 0.85% (n=1); blaIMP was not detected. However, 12.7% (n=7) of CPKP coharbored blaNDM-1 and blaOXA-48 genes. blaNDM-1 positive strains were further confirmed by DNA sequencing. The presence of the β-lactamase-encoding genes blaCTX-M, blaTEM and blaSHV was detected in the ESBL-producing K. pneumoniae strains (n=140). Single ESBL gene was detected in 38.5% (n=54): blaCTX-M 10.7% (n=15), blaSHV 22.8% (n=32), blaTEM 5% (n=7) and double ESBL genes were detected in 61.4% (n=86): blaCTX-M, blaSHV 32.1% (n=45), blaTEM, blaSHV 12.1% (n=17), blaTEM, blaCTX-M 15% (n=21) and blaTEM, blaSHV, blaCTX-M 2.14% (n=3). The CRKP strains coharboring blaNDM-1 and blaOXA-48 genes (n=7) were positive for blaCTX-M, blaSHV (n=3), blaSHV (n=1) and blaCTX-M (n=3). The results are shown in Table 3.
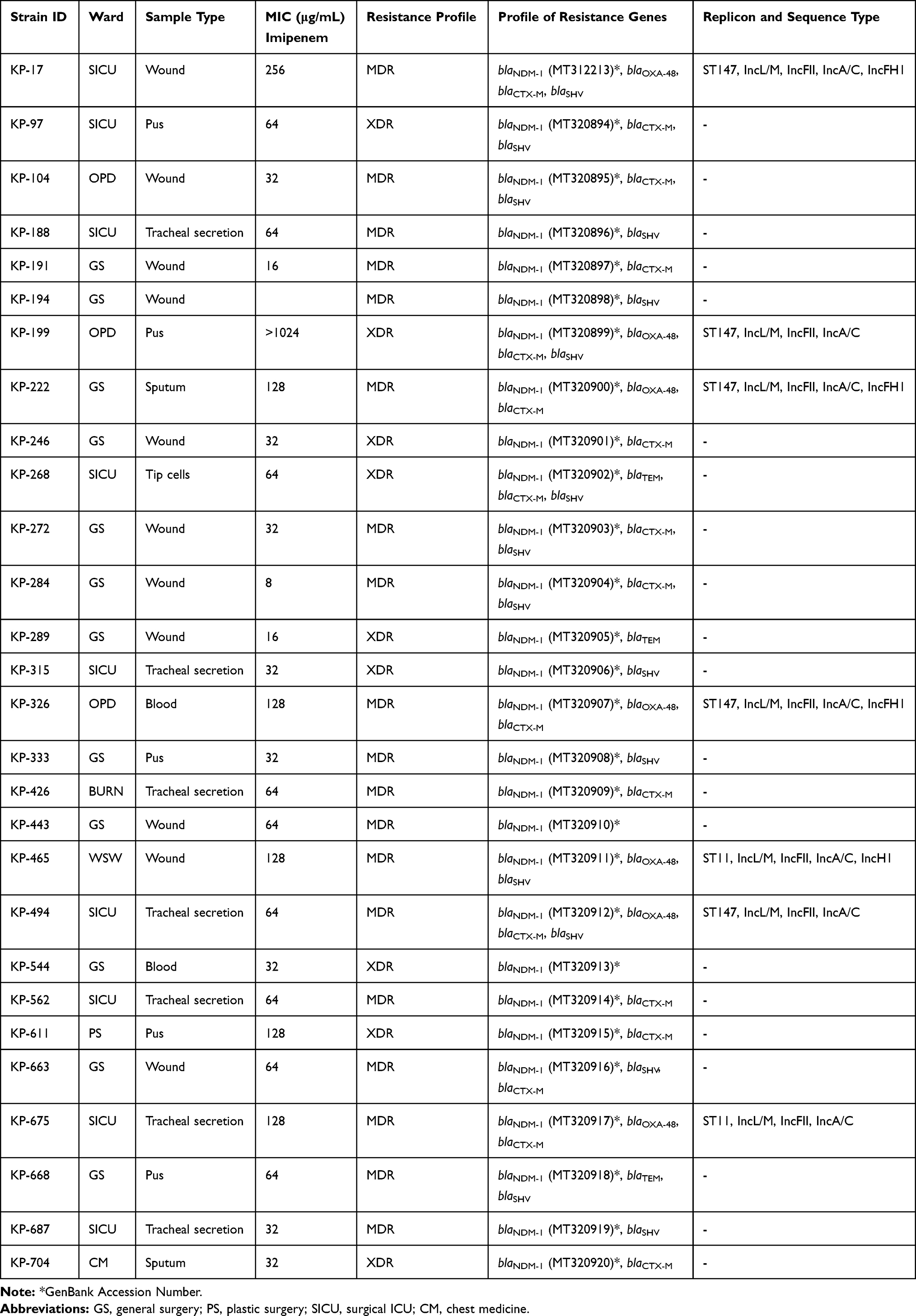 |
Table 3 Resistance Profile of Carbapenem-Resistant K. pneumoniae |
Sequence Type Analysis and Plasmid Detection of NDM-1 Producing Isolates
CRKP coharboring blaNDM-1 and blaOXA-48 (n=7) were further analyzed for sequence typing. High-risk K. pneumoniae clones ST147 coharbored blaNDM-1, blaOXA-48, blaCTX-M, blaSHV (n=3), blaNDM-1, blaOXA-48 blaCTX-M (n=2), while ST11 coharbored blaNDM-1, blaOXA-48, blaSHV (n=1) and blaNDM-1, blaOXA-48, blaCTX-M (n=1). Plasmid analysis of CRKP co-harboring blaNDM-1 and blaOXA-48 identified the following replicon types: IncL/M, IncFII, IncA/C and IncH1.21
Discussion
The emergence of CRKP has resulted in limited effective treatment strategies thus posing a major healthcare threat worldwide.1 Global dissemination of transmissible carbapenemases by virtue of horizontal gene transfer involving certain high-risk clones9 has become alarming especially in developing countries in the backdrop of inconsistent antibiotic policies. K. pneumoniae is among one of the most commonly detected multidrug-resistant member of the Enterobacteriaceae family.22
In the present study, we identified 51.1% CRKP strains that consisted of 77.7% carbapenemase producers. A large-scale study conducted in Turkey has detected only 3.1% (n=45/1452) CRKP isolates,2 while from the European cohort study, 55% (n=944/1717) isolates were carbapenem resistant and 39.84% (n=684/1717) were carbapenemase producers.23 Similarly, 10.69% (n=247/2310) CRKP strains were reported previously.24 However, the highest percentages of carbapenem resistant and carbapenemase producers are reported from Pakistan such as another study identified 88% carbapenemase producers.25 Due to the presence of high carbapenem resistance among K. pneumoniae in Pakistan, it is tempting to speculate that K. pneumoniae strains have the ability to retain diverse resistance determinants especially in a situation of uncontrolled use of high amounts of antibiotics. Wound samples (49.4%) were the major source of the CRKP infection that were significantly associated with the general surgery ward. In line with our study, 40% of wound samples with carbapenemase production were reported recently in association with the emergency department.26 However, blood, urine, sputum, tracheal secretion and pus were the major source of CRKP in other studies.11,24,25,27–29 The identification of CRKP strains from different anatomical sites highlights the importance of diverse set of sampling sites for the surveillance studies.
In consistent with the previous studies,2,11,30–32 the most effective antibiotics against the isolates were polymyxin-B (13.7%) and tigecycline (21.1%). However, intermediate to high resistance levels were observed against carbapenemases (meropenem, imipenem and ertapenem) 90% to 98%, cephalosporins 86% to 92%, aztreonam 90.3%, ciprofloxacin 87% and amikacin 37.1% that counts for 72% MDR and 28% XDR isolates. Sattar et al12 have reported 45% MDR K. pneumoniae strains with 85% to 90% resistance to cephalosporins and 30% resistance to imipenem. Another study from Pakistan reported 22.5% MDR K. pneumoniae strains among the study population in 2013.33 The detailed analysis of antibiotic resistance among the K. pneumoniae from Pakistan suggested that the resistance has been increasing.
The most frequently detected carbapenemases among K. pneumoniae are blaKPC enzymes followed by blaNDM-1, blaOXA-48-like and blaVIM in K. pneumoniae.22 In our study, the detailed resistome analysis revealed the presence of carbapenemase resistance genes in 55 out of 117 CRKP strains. The most commonly detected carbapenemase genes were blaNDM-1 (23.9%; n=28/55) and blaOXA-48 (22.2%; n=26/55) while blaVIM was identified in only 1 isolate and blaIMP was not detected. In consistent with our results, several studies from Pakistan reported that the most prevalent carbapenemase genes in Enterobacteriaceae/K. pneumoniae are blaNDM-1 83.3% (n=30/37),25 70% (n=10),28 14.6% (n=13/82)34 followed by blaOXA-48 86% (n=49/57),35 50% (n=5/10)28 and blaVIM 13.4% (n=11/82),34 3.5% (n=2/57).35 The results of our study are also in line with the observations that India, Bangladesh and Pakistan are the major reservoir countries for the widespread dissemination of carbapenemase genes such as blaNDM-1 and blaOXA-48.36 Since the first report of blaNDM-1 detection in Pakistan in 2010,37 carbapenemase genes have spread significantly. Moreover, in the present study, the blaNDM-1 and blaOXA-48 coproduction was detected in 7 out of 55 CRKP. The co-occurrence of blaNDM-1 and blaOXA-48 has been reported previously in Asian and European countries.16,24,38–40 However, in Pakistan the coexistence of carbapenem-resistant genes is not commonly detected in K. pneumoniae. In clinical isolates of K. pneumoniae, blaKPC-2, blaNDM-1 (n=2/20),12 blaNDM-1, blaOXA-48 (n=2/10)28 and blaVIM, blaNDM-1 (n=4/28) encoding genes in community-based E. coli isolates41 have been identified.
The CRKP strains coharboring blaNDM-1 and blaOXA-48 examined in our study belonged to either ST11; single locus variant of ST25842 or emerging ST147 high-risk CRKP clone with resistance genes located on different plasmids.9 NDM-type carbapenemases have been described associated with ST11, ST14, ST147, ST340, ST149 and ST231.2 The ST11 is typically associated with the acquisition of multidrug resistance due to its ability to capture multiple plasmids42 and K. pneumoniae strains with multiple resistance genes have been reported previously.43 In concurrence with this study, our data also revealed that different antimicrobial resistance and replicon type exist within the identified ST11 isolates. One of the ST11 isolate was polymyxin-B resistant while other was susceptible. Our results are in line with the previously reported study from Pakistan where out of 3 ST11 strains, 2 strains were colistin resistant and 1 strain was colistin susceptible.28 The ST11 isolates identified in our study coharbored blaNDM-1 and blaOXA-48 genes, whereas ST11 isolates positive for blaNDM-1 (n=7), blaNDM-7 (n=2) and blaNDM-5 (n=1) were recently reported from Pakistan.25
Previously, the pandemic lineage ST147 in K. pneumoniae has been correlated with the spread of carbapenemase resistant genes such as blaCTX-M, blaVIM, blaOXA-48, blaKPC and blaNDM-1.44,45 ST147 has also been associated with blaNDM-1, blaCTX-M, blaSHV,30 blaCMY-4, blaOXA-48,46 blaNDM-1, blaOXA-48,38 blaNDM-147 and blaOXA-48.24 Antecedently, two studies are available from Pakistan that reported the existence of ST147 K. pneumoniae with blaOXA181 resistant gene11 and ST147 K. pneumoniae isolate with blaNDM-1, blaNDM-5.25 The coexistence of blaNDM-1, blaOXA-48 has also been detected in ST307 from China16 and blaNDM-1, blaOXA-232 in ST231 from Pakistan.27 However, in our study we have identified the co-emergence of blaNDM-1, blaOXA-48, blaCTX-M, blaSHV among ST147 (n=5), a globally spread high-risk clone. The identification of S147 with blaNDM-1, blaOXA-48, blaCTX-M, blaSHV is alarming as it indicates that strong selection has occurred towards the resistance in these clinical isolates from Pakistan.
Subsequently, four replicon types IncL/M, IncFII, IncA/C and IncH1 were detected in the present study. Previous studies have shown that IncL/M-type plasmid was related to the OXA-48-type carbapenemases and responsible for the blaOXA-48 gene dissemination.48 The molecular studies have reported that the most frequent replicon type identified in K. pneumoniae species is IncFII replicon9 while IncA/C type replicons are responsible for the horizontal spread of NDM-type carbapenemase along with IncFIIK, IncL/M and IncH1.49 Moreover, among the typed resistant plasmids, IncL/M and IncF11 plasmids may be regarded as epidemic as they have been detected in different countries with different origins and sources.50 On the other hand, IncR, IncFIIK-type and IncA/C type replicons have been identified in OXA-48-type carbapenemases and IncR type replicons in NDM-type carbapenemases.51 Previously reported replicon types among the NDM-producing K. pneumoniae from Pakistan include IncN, IncA/C52 and IncFII, IncR.11 In our study, the identified replicon types (IncL/M, IncFII, IncA/C and IncH1) are reported to be responsible for OXA-48-type and NDM-type carbapenemases dissemination.
Conclusion
We reported the first identification of high-risk CRKP clone ST147 coharboring several carbapenem resistance genes blaNDM-1, blaOXA-48, blaCTX-M, blaSHV from Pakistan. Taken into account the presence of highest genetic diversity among K. pneumoniae worldwide, the identification of high-risk clone with multidrug resistance and coexistence of different classes of β-lactamases in the same strain highlight the severity of health challenges posed by K. pneumoniae worldwide. Our findings suggested that the high antimicrobial resistance existed among study isolates that can also be associated with the presence of several β-lactams genes in a high-risk clone. Therefore, the continuous monitoring of carbapenemases is necessary to prevent the national and transnational spread of these powerful isolates especially in case when the healthcare facilities are inadequate.
Acknowledgments
We are thankful to the University of Health Sciences, Lahore, and King Edward Medical University, Lahore for the provision of samples and research facilities.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pitout JD, Nordmann P, Poirel L. Carbapenemase-producing Klebsiella pneumoniae, a key pathogen set for global nosocomial dominance. Antimicrob Agents Chemother. 2015;59(10):5873–5884. doi:10.1128/AAC.01019-15
2. Davarcı İ, Şenbayrak S, Aksaray S, Koçoğlu ME, Kuşkucu MA, Samastı M. Molecular epidemiology of carbapenem-resistant klebsiella pneumoniae isolates. Anatol Clin. 2019;24(1):1–7.
3. Ye Y, Xu L, Han Y, Chen Z, Liu C, Ming L. Mechanism for carbapenem resistance of clinical Enterobacteriaceae isolates. Exp Ther Med. 2018;15(1):1143–1149. doi:10.3892/etm.2017.5485
4. Durdu B, Hakyemez IN, Bolukcu S, Okay G, Gultepe B, Aslan T. Mortality markers in nosocomial Klebsiella pneumoniae bloodstream infection. Springerplus. 2016;5(1):1892. doi:10.1186/s40064-016-3580-8
5. Organization WH. Antimicrobial Resistance: Global Report on Surveillance. World Health Organization; 2014.
6. Jia X, Dai W, Ma W, et al. Carbapenem-resistant E. cloacae in Southwest China: molecular analysis of resistance and risk factors for infections caused by NDM-1-producers. Front Microbiol. 2018;9:658. doi:10.3389/fmicb.2018.00658
7. Aguirre-Quiñonero A, Martínez-Martínez L. Non-molecular detection of carbapenemases in Enterobacteriaceae clinical isolates. J Infect Chemother. 2017;23(1):1–11. doi:10.1016/j.jiac.2016.09.008
8. van Duin D, Doi Y. The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence. 2017;8(4):460–469. doi:10.1080/21505594.2016.1222343
9. Lee C-R, Lee JH, Park KS, Kim YB, Jeong BC, Lee SH. Global dissemination of carbapenemase-producing Klebsiella pneumoniae: epidemiology, genetic context, treatment options, and detection methods. Front Microbiol. 2016;7:895.
10. Bonomo RA, Burd EM, Conly J, et al. Carbapenemase-producing organisms: a global scourge. Clin Infect Dis. 2018;66(8):1290–1297. doi:10.1093/cid/cix893
11. Nahid F, Zahra R, Sandegren L. A blaOXA-181-harbouring multi-resistant ST147 Klebsiella pneumoniae isolate from Pakistan that represent an intermediate stage towards pan-drug resistance. PLoS One. 2017;12(12):e0189438. doi:10.1371/journal.pone.0189438
12. Sattar H, Toleman M, Nahid F, Zahra R. Co-existence of blaNDM-1 and blaKPC-2 in clinical isolates of Klebsiella pneumoniae from Pakistan. J Infect Chemother. 2016;28(4):346–349. doi:10.1179/1973947814Y.0000000223
13. Willemsen I, van Esser J, Kluytmans-van den Bergh M, Kluytmans-van den Bergh M, et al. Retrospective identification of a previously undetected clinical case of OXA-48-producing K. pneumoniae and E. coli: the importance of adequate detection guidelines. Infection. 2016;44(1):107–110. doi:10.1007/s15010-015-0805-7
14. Duman Y, Ersoy Y, Gursoy N, Altunisik Toplu S, Otlu B. A silent outbreak due to Klebsiella pneumoniae that co-produced NDM-1 and OXA-48 carbapenemases, and infection control measures. Iran J Basic Med Sci. 2020;23(1):46–50. doi:10.22038/IJBMS.2019.35269.8400
15. Seiffert SN, Marschall J, Perreten V, Carattoli A, Furrer H, Endimiani A. Emergence of Klebsiella pneumoniae co-producing NDM-1, OXA-48, CTX-M-15, CMY-16, QnrA and ArmA in Switzerland. Int J Antimicrob Agents. 2014;44(3):260–262. doi:10.1016/j.ijantimicag.2014.05.008
16. Xie L, Dou Y, Zhou K, et al. Coexistence of blaOXA-48 and truncated blaNDM-1 on different plasmids in a Klebsiella pneumoniae isolate in China. Front Microbiol. 2017;8:133. doi:10.3389/fmicb.2017.00133
17. Dortet L, Poirel L, Al Yaqoubi F, Nordmann P. NDM-1, OXA-48 and OXA-181 carbapenemase-producing enterobacteriaceae in sultanate of Oman. Clin Microbiol Infect. 2012;18(5):E144–E148. (). doi:10.1111/j.1469-0691.2012.03796.x
18. Wayne P. CLSI. Performance Standards for Antimicrobial Susceptibility Testing. CLSI Supplement M100. Clinical and Laboratory Standards Institute; 2018.
19. Martzy R, Bica-Schröder K, Pálvölgyi ÁM, et al. Simple lysis of bacterial cells for DNA-based diagnostics using hydrophilic ionic liquids. Sci Rep. 2019;9(1):1–10. doi:10.1038/s41598-019-50246-5
20. Brolund A, Rajer F, Giske CG, Melefors Ö, Titelman E, Sandegren L. Dynamics of resistance plasmids in extended-spectrum-β-lactamase-producing Enterobacteriaceae during postinfection colonization. Antimicrob Agents Chemother. 2019;63(4):e02201–e02218. doi:10.1128/AAC.02201-18
21. Carloni E, Andreoni F, Omiccioli E, Villa L, Magnani M, Carattoli A. Comparative analysis of the standard PCR-Based Replicon Typing (PBRT) with the commercial PBRT-KIT. Plasmid. 2017;90:10–14. doi:10.1016/j.plasmid.2017.01.005
22. Grundmann H, Glasner C, Albiger B, et al. Occurrence of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in the European survey of carbapenemase-producing Enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect Dis. 2017;17(2):153–163. doi:10.1016/S1473-3099(16)30257-2
23. David S, Reuter S, Harris SR, et al. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat Microbiol. 2019;4(11):1919–1929. doi:10.1038/s41564-019-0492-8
24. Guo L, An J, Ma Y, et al. Nosocomial outbreak of OXA-48-producing Klebsiella pneumoniae in a Chinese hospital: clonal transmission of ST147 and ST383. PLoS One. 2016;11(8).
25. Qamar MU, Walsh TR, Toleman MA, et al. Dissemination of genetically diverse NDM-1,-5,-7 producing-Gram-negative pathogens isolated from pediatric patients in Pakistan. Future Microbiol. 2019;14(8):691–704. doi:10.2217/fmb-2019-0012
26. Tekeli A, Dolapci İ, Evren E, Oguzman E, Karahan ZC. Characterization of Klebsiella pneumoniae Coproducing KPC and NDM-1 Carbapenemases from Turkey. Microb Drug Resist. 2019;26:118–125.
27. Masseron A, Poirel L, Ali BJ, Syed M, Nordmann P. Molecular characterization of multidrug-resistance in Gram-negative bacteria from the Peshawar teaching hospital, Pakistan. New Microbes New Infect. 2019;32:100605. doi:10.1016/j.nmni.2019.100605
28. Lomonaco S, Crawford MA, Lascols C, et al. Resistome of carbapenem-and colistin-resistant Klebsiella pneumoniae clinical isolates. PLoS One. 2018;13(6):e0198526. doi:10.1371/journal.pone.0198526
29. Ejaz H, Wang N, Wilksch JJ, et al. Phylogenetic analysis of Klebsiella pneumoniae from hospitalized children, Pakistan. Emerg Infect Dis. 2017;23(11):1872. doi:10.3201/eid2311.170833
30. Kiaei S, Moradi M, Hosseini-Nave H, Ziasistani M, Kalantar-Neyestanaki D. Endemic dissemination of different sequence types of carbapenem-resistant Klebsiella pneumoniae strains harboring blaNDM and 16S rRNA methylase genes in Kerman hospitals, Iran, from 2015 to 2017. Infect Drug Resist. 2019;12:45. doi:10.2147/IDR.S186994
31. Gamal D, Fernández-Martínez M, Salem D, et al. Carbapenem-resistant Klebsiella pneumoniae isolates from Egypt containing blaNDM-1 on IncR plasmids and its association with rmtF. Int J Infect Dis. 2016;43:17–20. doi:10.1016/j.ijid.2015.12.003
32. Samonis G, Maraki S, Karageorgopoulos D, Vouloumanou E, Falagas M. Synergy of fosfomycin with carbapenems, colistin, netilmicin, and tigecycline against multidrug-resistant Klebsiella pneumoniae, Escherichia coli, and Pseudomonas aeruginosa clinical isolates. Eur J Clin Microbiol Infect Dis. 2012;31(5):695–701. doi:10.1007/s10096-011-1360-5
33. Sabir R, Alvi SFD, Fawwad A. Antimicrobial susceptibility pattern of aerobic microbial isolates in a clinical laboratory in Karachi-Pakistan. Pak J Med Sci. 2013;29(3):851. doi:10.12669/pjms.293.3187
34. Nahid F, Khan AA, Rehman S, Zahra R. Prevalence of metallo-β-lactamase NDM-1-producing multi-drug resistant bacteria at two Pakistani hospitals and implications for public health. J Infect Public Health. 2013;6(6):487–493. doi:10.1016/j.jiph.2013.06.006
35. Demir Y, Zer Y, Karaoglan I. Investigation of VIM, IMP, NDM-1, KPC AND OXA-48 enzymes in Enterobacteriaceae strains. Pak J Pharm Sci. 2015;28.
36. Wailan A, Paterson D. The spread and acquisition of NDM-1: a multifactorial problem. Expert Rev Anti Infect Ther. 2014;12(1):91–115. doi:10.1586/14787210.2014.856756
37. Kumarasamy KK, Toleman MA, Walsh TR, et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: a molecular, biological, and epidemiological study. Lancet Infect Dis. 2010;10(9):597–602. doi:10.1016/S1473-3099(10)70143-2
38. Solgi H, Badmasti F, Giske CG, Aghamohammad S, Shahcheraghi F. Molecular epidemiology of NDM-1-and OXA-48-producing Klebsiella pneumoniae in an Iranian hospital: clonal dissemination of ST11 and ST893. J Antimicrob Chemother. 2018;73(6):1517–1524. doi:10.1093/jac/dky081
39. Lixandru BE, Cotar AI, Straut M, et al. Carbapenemase-producing Klebsiella pneumoniae in Romania: a six-month survey. PLoS One. 2015;10(11):e0143214. doi:10.1371/journal.pone.0143214
40. Jamal WY, Albert MJ, Khodakhast F, Poirel L, Rotimi VO. Emergence of new sequence type OXA-48 carbapenemase-producing Enterobacteriaceae in Kuwait. Microb Drug Resist. 2015;21(3):329–334. doi:10.1089/mdr.2014.0123
41. Rahman S, Hussain MA, Murtaza A, et al. How ESBL-and carbapenemase-producing genes are mobilized-analysis of escherichia coli isolates recovered from poultry retail meat in district mardan KPK Pakistan.
42. Navon-Venezia S, Kondratyeva K, Carattoli A. Klebsiella pneumoniae: a major worldwide source and shuttle for antibiotic resistance. FEMS Microbiol Rev. 2017;41(3):252–275. doi:10.1093/femsre/fux013
43. Souza RD, Pinto NA, Hwang I, et al. Molecular Epidemiology and Resistome Analysis of Multidrug-Resistant ST11 Klebsiella Pneumoniae Strain Containing Multiple Copies of Extended-Spectrum Β-Lactamase Genes Using Whole-Genome Sequencing. 2017.
44. Damjanova I, Toth A, Paszti J, et al. Expansion and countrywide dissemination of ST11, ST15 and ST147 ciprofloxacin-resistant CTX-M-15-type β-lactamase-producing Klebsiella pneumoniae epidemic clones in Hungary in 2005—the new ‘MRSAs’? J Antimicrob Chemother. 2008;62(5):978–985. doi:10.1093/jac/dkn287
45. Samuelsen Ø, Toleman M, Hasseltvedt V, et al. Molecular characterization of VIM-producing Klebsiella pneumoniae from Scandinavia reveals genetic relatedness with international clonal complexes encoding transferable multidrug resistance. Clin Microbiol Infect. 2011;17(12):1811–1816. doi:10.1111/j.1469-0691.2011.03532.x
46. Grami R, Mansour W, Ben Haj Khalifa A, et al. Emergence of ST147 Klebsiella pneumoniae producing OXA-204 carbapenemase in a University Hospital, Tunisia. Microb Drug Resist. 2016;22(2):137–140. doi:10.1089/mdr.2014.0278
47. Wang X, Xu X, Li Z, et al. An outbreak of a nosocomial NDM-1-producing Klebsiella pneumoniae ST147 at a teaching hospital in mainland China. Microb Drug Resist. 2014;20(2):144–149. doi:10.1089/mdr.2013.0100
48. Poirel L, Bonnin RA, Nordmann P. Genetic features of the widespread plasmid coding for the carbapenemase OXA-48. Antimicrob Agents Chemother. 2012;56(1):559–562. doi:10.1128/AAC.05289-11
49. Bonnin RA, Poirel L, Carattoli A, Nordmann P. Characterization of an IncFII plasmid encoding NDM-1 from Escherichia coli ST131. PLoS One. 2012;7(4):e34752. doi:10.1371/journal.pone.0034752
50. Carattoli A. Resistance plasmid families in Enterobacteriaceae. Antimicrob Agents Chemother. 2009;53(6):2227–2238. doi:10.1128/AAC.01707-08
51. Erdem F, Oncul O, Aktas Z. Characterization of resistance genes and polymerase chain reaction-based replicon typing in carbapenem-resistant klebsiella pneumoniae. Microb Drug Resist. 2019;25(4):551–557. doi:10.1089/mdr.2018.0231
52. Sartor AL, Raza MW, Abbasi SA, et al. Molecular epidemiology of NDM-1-producing Enterobacteriaceae and Acinetobacter baumannii isolates from Pakistan. Antimicrob Agents Chemother. 2014;58(9):5589–5593. doi:10.1128/AAC.02425-14
53. Chander Y, Ramakrishnan M, Jindal N, Hanson K, Goyal SM. Differentiation of Klebsiella pneumoniae and K. oxytoca by multiplex polymerase chain reaction. Int J Appl Res Vet M. 2011;9(2):138.
54. Rajivgandhi G, Maruthupandy M, Ramachandran G, Priyanga M, Manoharan N. Detection of ESBL genes from ciprofloxacin resistant Gram negative bacteria isolated from urinary tract infections (UTIs). Front Lab Med. 2018;2(1):5–13. doi:10.1016/j.flm.2018.01.001
55. Tada T, Shrestha B, Miyoshi-Akiyama T, et al. NDM-12, a novel New Delhi metallo-β-lactamase variant from a carbapenem-resistant Escherichia coli clinical isolate in Nepal. Antimicrob Agents Chemother. 2014;58(10):6302–6305. doi:10.1128/AAC.03355-14
56. Candan ED, Aksöz N. Escherichia coli: characteristics of carbapenem resistance and virulence factors. Braz Arch Biol Technol. 2017;60.
57. Toleman MA, Bugert JJ, Nizam SA. Extensively drug-resistant New Delhi metallo-β-lactamase–encoding bacteria in the environment, Dhaka, Bangladesh, 2012. Emerg Infect Dis. 2015;21(6):1027. doi:10.3201/eid2106.141578
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.