")
Back to Journals » Cancer Management and Research » Volume 8
Novel approaches to target HER2-positive breast cancer: trastuzumab emtansine
Authors Recondo Jr G, de la Vega M, Galanternik F, Díaz-Cantón E, Leone BA , Leone J
Received 17 January 2016
Accepted for publication 10 April 2016
Published 19 May 2016 Volume 2016:8 Pages 57—65
DOI https://doi.org/10.2147/CMAR.S104447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kenan Onel
Gonzalo Recondo Jr,1 Maximo de la Vega,1 Fernando Galanternik,1 Enrique Díaz-Cantón,1 Bernardo Amadeo Leone,2 José Pablo Leone3
1Centro de Educación Médica e Investigaciones Clínicas, Buenos Aires, 2Grupo Oncológico Cooperativo del Sur, Neuquén, Argentina; 3Division of Hematology-Oncology and Blood & Marrow Transplantation, Holden Comprehensive Cancer Center, University of Iowa Hospitals & Clinics, Iowa City, IA, USA
Abstract: The human epidermal growth factor receptor 2 (HER2) is overexpressed in 20% of breast carcinomas. Prior to the development of targeted therapies, HER2-positive breast cancer was associated with more aggressive disease and poor prognosis. Trastuzumab emtansine (T-DM1) is an antibody-drug conjugate that results from the combination of trastuzumab and DM1, a derivative of the antimicrotubule agent maytansine. This molecule has the ability to enhance cytotoxic drug delivery to specifically targeted cells that overexpress HER2, therefore, maximizing efficacy while sparing toxicity. In recent years, T-DM1 has shown to improve outcomes in metastatic HER2-positive breast cancer that is resistant to trastuzumab. In addition, T-DM1 is currently being tested in the neoadjuvant and adjuvant settings to identify patients who may benefit from this therapy. This review focuses on the mechanism of action, early and late-phase clinical trials, and ongoing studies of T-DM1 in HER2-positive breast cancer.
Keywords: T-DM1, trastuzumab emtansine, HER2-positive breast cancer, metastatic breast cancer, targeted therapies
Introduction
Breast cancer is one of the most frequent malignancies worldwide and represents an important public health problem.1 In the past years, the molecular understanding of this disease has shed light into its heterogeneity.2 The human epidermal growth factor receptor 2 (HER2) is a transmembrane receptor-like tyrosine kinase (RTK) overexpressed in 20%–25% of breast carcinomas.3 It is a member of the ErbB/EGFR receptor family that also encompasses EGFR/ErbB1, ErbB3, and ErbB4.4 Prior to the widespread use of targeted therapies, HER2-positive breast cancer was associated with more aggressive disease, poor prognosis, and resistance to chemotherapeutic agents.5
HER2 is the only member of the ErbB family that has no known ligand, and it is thought to be primarily the preferential heterodimerization partner for other ErbB receptors.6 In 2003, analysis of the crystal structure of HER2 revealed that the extracellular region of the receptor is in a fixed dimerization state, making it available to interact with any other ErbB RTK. This key observation led to a better understanding of the transforming capabilities of HER2 overexpression, with increasing availability to form hetero- or homodimers that lead to enhanced signaling in both the presence and absence of ligands.7
Trastuzumab, a humanized IgG1 monoclonal antibody directed against the extracellular domain of HER2, was the first targeted therapy against HER2 to show clinical efficacy in breast cancer.8 Multiple mechanisms of action have been proposed, including PI3K/Akt and MAPK signaling inhibition, antibody-dependent cell-mediated cytotoxicity exerted by the immune system, prevention of HER2 cleavage by matrix metalloproteinases, and angiogenesis inhibition.9 While the combination of trastuzumab with chemotherapy is effective both in the advanced and the adjuvant settings, virtually all metastatic patients will eventually progress to therapy8 and a proportion of patients will develop recurrence after postoperative treatment,10 making de novo and acquired resistance an important clinical problem.
Preclinical studies on trastuzumab resistance have proposed several mechanisms to explain this phenomenon. These include masking of HER2 epitopes by the membrane-bound mucin MUC-4,11 increased signaling through other ErbB receptors,12,13 activation of PI3K/Akt pathway by activating PIK3CA mutations and loss of PTEN,14–16 signaling through alternative RTK families such as IGF-1,17 and the expression of p95HER2 fragments that have lost variable portions of the extracellular domains and retain kinase activity.18,19
Trastuzumab emtansine (T-DM1) is one of the novel agents recently found to improve outcomes in HER2-positive breast cancer that is resistant to trastuzumab. This review focuses on the mechanism of action, early and late-phase clinical trials, and ongoing studies of T-DM1 in HER2-positive breast cancer.
Mechanism of action
T-DM1 is part of the antibody-drug conjugate (ADC) class of anticancer agents that combine cytotoxic agents with monoclonal antibodies as a means of enhancing drug delivery to specifically targeted cells. The key objective of this approach is to maximize efficacy while sparing toxicity to normal tissues. ADCs share three components: the antibody, a linker molecule, and the cytotoxic moiety.
Specificity of conventional chemotherapy relies on the fact that highly proliferative cells are more sensitive to cytotoxic effects, but this implies considerable activity on normal cells, which results in significant toxicity and partially explains the narrow therapeutic window often seen with this kind of therapy. T-DM1 results from the combination of trastuzumab and DM1, a derivative of the antimicrotubule agent maytansine, through a covalent bond, thus delivering highly effective chemotherapy to targeted cells and sparing unwanted adverse effects. Preclinical research identified a synergistic interaction between antimicrotubule agents and trastuzumab,20 and clinical efficacy of maytansine in breast cancer was confirmed in Phase I and II trials, but its poor tolerability limited its use in further research.21,22
The selection of trastuzumab as the antibody in T-DM1 is based on the low levels of HER2 expression in the normal cells compared to the breast cancer cells.23 In addition, the tumors that progress on trastuzumab-based therapy continue to express high levels of HER2,24 which enables T-DM1 to exert activity in cases of trastuzumab-resistant disease. The trastuzumab antibody in T-DM1 maintains its affinity to HER2 epitopes, and T-DM1 sustains the trastuzumab-mediated effects in cell signaling and antibody-dependent cell-mediated cytotoxicity.25
The linker molecule used in ADCs is of utmost importance, as the early release of the active agent in circulation decreases specificity and increases the likelihood of systemic toxicity. DM1 is bound to lysine residues in trastuzumab by N-succinimidyl 4-(N-maleimidomethyl)cyclohexane-1-carboxylate (SMCC). The mean ratio of DM1 to trastuzumab molecules is 3.5:1. DM1 is inactive while bound to the conjugate in circulation and gains activity when released inside the cancer cells.
The initial process involves receptor-mediated internalization of the drug into endosomes, which deliver the ligand-bound receptors to the lysosome compartment. Then, lysine-N-SMCC-DM1 is released upon proteolytic degradation.26,27 Active metabolites are absent in the presence of lysosomal inhibitors, further supporting this observation. Upon intracellular release, DM1 binds to the Vinca site at microtubules resulting in the inhibition of polymerization. Cell cycle arrest at G2/M checkpoint leads to apoptotic cell death. In addition, treatment of xenografts with T-DM1 resulted in cell death by mitotic catastrophe, and impaired intracellular trafficking by microtubule disruption could also explain T-DM1 activity on the nondividing cells.28
Phase I trials
The first T-DM1 Phase I trial in humans intended to evaluate safety, pharmacokinetics, and activity of the drug in patients with advanced HER2-positive breast cancer.29 Twenty-four patients who had progressed on trastuzumab-based therapy (median of four prior chemotherapy agents) received escalating doses of trastuzumab emtansine, from 0.3 mg/kg to 4.8 mg/kg on an every-3-weeks scheme. Premedication was not routinely used for the first infusion, which was given over 90 minutes. Reversible thrombocytopenia was dose limiting at 4.8 mg/kg; it was estimated that the maximum tolerated dose was 3.6 mg/kg, with a half-life of 3.5 days. Common drug-related adverse events observed were grade 1-2 thrombocytopenia, elevated liver enzymes, nausea, asthenia, and anemia. A possible explanation for transaminase elevation includes internalization of T-DM1 into the Fc receptor-bearing Kupffer cells with subsequent release of free DM1 into the local liver microenvironment. No cardiac effects requiring dose modification were reported. One patient experienced a serious adverse event (grade 3 pulmonary hypertension) considered to be possibly drug related. In terms of efficacy, the clinical benefit rate (defined as objective response plus stable disease at 6 months) among 15 patients treated at 3.6 mg/kg was 73%. Five objective responses were recorded. The response rate in patients with the measurable disease was 44%. The trial concluded that the dose for further study was 3.6 mg/kg every 3 weeks. Regarding toxicity, T-DM1 was associated with mild, reversible toxic effects, with a robust clinical activity in a heavily pretreated patient cohort.
The second Phase I trial included a weekly schedule. This was a multicenter, open-label, dose-escalation study.30 The aim was to assess the safety, tolerability, or pharmacokinetics of T-DM1 administered weekly or every 3 weeks in patients with HER2-positive advanced breast cancer previously treated with trastuzumab. Patients received escalating doses of T-DM1 once a week, starting at 1.2 mg/kg. Twenty-eight patients were included, and the maximum tolerated dose was determined to be 2.4 mg/kg. Of the six patients who were enrolled in the 2.4 mg/kg cohort, only one experienced a dose-limiting toxicity in the form of grade 2 thrombocytopenia that led to dosing being held on day 8 of cycle 1. In contrast, two of three patients who received T-DM1 at 2.9 mg/kg dose experienced adverse events preventing retreatment on day 8 of cycle 1. Population pharmacokinetic modeling and in vitro studies suggest that altered platelet production by megakaryocytes, rather than an effect on circulating platelets, likely accounts for the observed thrombocytopenia. Grade ≥3 adverse events were reported in 19 (67.9%) patients. Treatment-related adverse events occurred in 25 (89.3%) patients. In general, the tolerability of T-DM1 weekly appeared to be similar to that of T-DM1 every 3 weeks. Objective partial tumor responses were reported in 13 (46.4%) patients, and the 6-month clinical benefit rate was 57.1%. The authors concluded that a weekly dose of T-DM1 at 2.4 mg/kg had antitumor activity and was adequately tolerated.
Phase II trials
Based on the results from the Phase I studies described above, it became clear that T-DM1 was well tolerated at 3.6 mg/kg every 3 weeks and with sufficient efficacy in patients with HER2-positive metastatic breast cancer who were previously treated with trastuzumab. Phase II studies were logically conducted to further assess and define the safety and efficacy of T-DM1.
Burris et al31 reported a single-arm Phase II study that assessed efficacy and safety of T-DM1 at 3.6 mg/kg every 3 weeks in a population of patients with HER2-positive advanced breast cancer who had tumor progression with HER2-directed therapy and chemotherapy. A total of 112 patients were included and treated, with a follow-up of ≥12 months. Interestingly, the median number of systemic agents previously used in the metastatic setting was five and 60% of patients had received lapatinib. The objective response rate (ORR) was 25.9% (95% CI 18.4%–34.4%). The median duration of response was not reached as a result of insufficient events (lower limit of 95% CI 6.2 months), and the median progression-free survival (PFS) was 4.6 months (95% CI 3.9–8.6 months). The response rates were higher among patients with confirmed HER2-positive tumors. The ADC was well tolerated without dose-limiting cardiotoxicity. Most adverse events were of grade 1 or 2. The most frequently observed grade 3 or 4 adverse events were hypokalemia (8.9%), thrombocytopenia (8.0%), and fatigue (4.5%). Hypokalemia was intriguingly not associated with vomiting, diarrhea, or diuretic use. Thrombocytopenia was not associated with serious bleeding. The most commonly reported hemorrhagic adverse events were grades 1–2 epistaxis, recorded in 34% of patients. No cases of grade 3 decline in left ventricular ejection fraction or symptomatic heart failure were observed. No patients discontinued treatment as a result of cardiotoxicity. Regarding pharmacokinetics, systemic exposure to DM1 was consistently low and repeated T-DM1 administration did not result in DM1 accumulation. The authors concluded that in heavily pretreated patients with HER2-positive metastatic breast cancer, T-DM1 administration resulted in an appreciable number of objective responses and was well tolerated. In a post hoc exploratory analysis, response rates in patients who previously received both lapatinib and trastuzumab were not much different from the overall population.
Another single-agent study of T-DM1 at 3.6 mg/kg every 3 weeks in a more homogeneous patient population showed similar activity.32 This Phase II trial, in contrast to the previous one, required that all patients had received several drugs, including trastuzumab, lapatinib, a taxane, an anthracycline, and capecitabine. The primary objectives were overall response rate by independent review and safety. The study included 110 patients, and the overall response rate was 34.5%, with a clinical benefit rate of 48.2% and a median PFS of 6.9 months. In 80 patients with confirmed HER2-positive tumors, the response rate was 41.3% and the median PFS was 7.3 months. Interestingly, a response rate of 20% was observed in 15 patients designated as HER2 normal on central laboratory retesting. This observation might suggest that HER2 expression below the currently used clinical threshold may be enough to confer sensitivity to T-DM1. The most common adverse events of any grade were fatigue (61.8%), nausea (37.3%), and thrombocytopenia (38.2%), and the most frequent grade ≥3 events were thrombocytopenia (9.1%), fatigue (4.5%), and cellulitis (3.6%). Thrombocytopenia infrequently led to T-DM1 discontinuation or dose reduction.
Given the encouraging results described earlier, a randomized Phase II trial was launched in the first-line setting. One hundred and thirty-seven patients with HER2-positive recurrent locally advanced or metastatic breast cancer were randomly assigned to trastuzumab combined with docetaxel (HT) or T-DM1 as the first-line treatment.33 The primary end points were investigator-assessed PFS and safety. The median PFS was 9.2 months with HT and 14.2 months with T-DM1 (hazard ratio [HR] 0.59, 95% CI 0.36–0.97). Interestingly, the ORR was 58.0% (95% CI 45.5%–69.2%) with HT and 64.2% (95% CI 51.8%–74.8%) with T-DM1. In addition, the immunoconjugate had a favorable safety profile compared with HT, with fewer grade 3 adverse events (46.4% vs 90.9%) and serious adverse events (20.3% vs 25.8%). There were no reports of symptomatic congestive heart failure. The most common adverse events reported in the T-DM1 group were fatigue, nausea, increase in liver transaminases, pyrexia, and headache. The favorable safety profile observed with T-DM1 appeared to translate into superior global quality of life. Preliminary overall survival (OS) results were similar between the treatment arms. The limitations of this study included principally its open-label design and a primary end point of investigator-assessed PFS.
Phase III trials
The EMILIA trial was the first Phase III study to demonstrate the clinical efficacy of treatment with T-DM1 in the metastatic setting.34 This randomized, international, open-label clinical trial evaluated the efficacy of T-DM1 versus lapatinib and capecitabine in the second-line treatment in patients with unresectable, locally advanced, or metastatic HER2-positive breast cancer who had progressed on previous treatment with taxanes and trastuzumab. This study compared treatment with T-DM1 to the standard second-line therapy, lapatinib (1,250 mg daily) combined with capecitabine (2,000 mg/m2). The primary end points were PFS assessed by independent review, OS, and safety. The trial rapidly enrolled 991 patients in 32 months and randomized them in a 1:1 ratio to T-DM1 monotherapy or the combination standard second-line therapy. Both arms in the study were well balanced, with a high proportion of visceral metastasis (67% and 68%).
With a median follow-up of 19 months, treatment with T-DM1 improved PFS from 6.4 months to 9.6 months (HR 0.65, 95% CI 0.55–0.77, P<0.001). Most importantly, patients in the T-DM1 group experienced prolonged OS (30.9 months vs 25.1 months, HR 0.68, P<0.001). The estimated 1-year and 2-year survival rates were 85.2% and 64.7% for the T-DM1 arm and 78.4% and 51.8% for the control arm. The ORR was also improved with T-DM1 (43.6% vs 30.8%, P<0.001), mainly due to partial responses. Complete responses were rarely achieved in both groups, but the median duration of response was also increased with T-DM1 (12.6 months vs 6.5 months). Patients experienced different toxicities, the most common being grade 3 and 4 adverse events with T-DM1, thrombocytopenia (12.9%) and elevated liver transaminase (7.2%), compared to hand foot syndrome (16.4%) and diarrhea (20.7%) in the control arm. Cardiac toxicity was similar between the groups. Patient-reported outcomes also favored T-DM1 with prolonged time to symptom worsening with a median time of 7.1 months versus 4.6 months (HR 0.796, P=0.021).35
Based on the improved efficacy and toxicity profile of T-DM1 as a second-line treatment, the US Food and Drug Administration approved this treatment on February 2013 in patients who had received trastuzumab and a taxane. This was the first chemotherapy-linked monoclonal antibody approved in the cancer treatment.
T-DM1 proved to be an effective drug in the treatment of metastatic HER2-positive breast cancer after progression to trastuzumab over lapatinib. Nevertheless, the effect of this drug on patients who had progressed after treatment with lapatinib and trastuzumab was unknown. Sequential treatment with T-DM1 after lapatinib and trastuzumab could potentially improve disease control in these patients. The TH3RESA trial was a Phase III, open-label, multicenter clinical trial that aimed to answer this question.36 The trial compared treatment with T-DM1 with the physician’s treatment of choice in patients with metastatic HER2-positive breast cancer who had progressed on treatment with lapatinib and trastuzumab in the metastatic setting and a taxane in any setting. The study co-primary endpoints were PFS assessed by the investigator and OS in the intention to treat population. Patients were randomly assigned in a 2:1 ratio to treatment with T-DM1 at 3.6 mg/kg every 21 days or treatment of physician’s choice that was restricted to single-agent, approved chemotherapy; single-agent or combined HER2-directed therapy; combination of chemotherapy and HER2-directed therapy; or hormonal therapy for hormone receptor-positive disease. Patients continued treatment until disease progression or unmanageable toxicity. This trial completed accrual between September 2011 and November 2012. Based on the data reported in the EMILIA trial, in September 2012, the trial was amended to allow crossover to T-DM1 in patients who had disease progression in treatment of physician's choice. The trial randomized 602 patients, 198 to the physician treatment choice of whom 44 patients crossed over to treatment with T-DM1 at the data cutoff. The patient characteristics were even between the arms, including number of previous regimens for advanced disease, hormone receptor status, and visceral disease involvement. There was a slightly higher proportion of patients with previously treated symptomatic brain metastasis in the physician’s treatment choice arm (14% vs 10%). Most patients in the control arm (83%) were treated with HER2-directed agents in combination, the most common being trastuzumab and chemotherapy (68%) and lapatinib with trastuzumab (10%).
PFS was increased with T-DM1, 6.2 months versus 3.3 months (HR 0.528, P<0.0001). This was sustained even when compared to the group of patients receiving trastuzumab in the physician’s choice group, as prespecified. This benefit was also independent of hormone receptor status, number of previous treatments, the status of visceral metastasis, and the presence of previously treated brain metastasis. The final OS analysis was recently reported in San Antonio and showed a significantly longer survival with T-DM1 (median 22.7 months) compared with the control arm (median 15.8 months, P=0.0007).37 The toxicity profile was quite similar to the reports of the EMILIA trial, the most common adverse events being asthenia and thrombocytopenia (15%), though grade 3 and 4 thrombocytopenia was 5%. Globally, severe adverse events were more frequent in the physician’s treatment choice arm. Cardiac toxicity was similar between the arms, probably due to a high proportion of patients receiving trastuzumab in the control arm. However, three patients died due to the study drug from pneumonitis, hepatic encephalopathy, and subarachnoid hemorrhage. The latter was secondary to grade 4 thrombocytopenia in a patient receiving anticoagulant therapy. Oncologists should be cautious when prescribing T-DM1 with anticoagulants based on this potential interaction. This study confirmed the efficacy of T-DM1 after previous anti-HER2 therapy, reverting previously described mechanisms of resistance in many patients and encouraging investigators to continue testing the drug in the first-line setting.
The MARIANNE trial is the first Phase III study to assess the efficacy of T-DM1 in the first-line setting.38 This trial randomized 1,095 patients with metastatic HER2-positive breast cancer to treatment with trastuzumab and a taxane (HT), T-DM1 plus placebo, or T-DM1 plus pertuzumab. The primary objective of the trial was PFS, noninferiority, and superiority, assessed by an independent review. Secondary end points were OS, ORR and patient safety, tolerability, and patient-reported outcome. The characteristics of patients were well balanced between the groups. A total of 44–45 patients per arm did not receive any prior therapy. The median PFS was 13.7 months with HT, 14.1 months with T-DM1, and 15.2 months with T-DM1 and pertuzumab. Both T-DM1-containing arms demonstrated noninferior PFS to that of the control arm. However, treatment with T-DM1 alone or combined with pertuzumab was not superior to HT. There was no difference in OS or response rate; however, patients responding to T-DM1 had a longer duration of response than those responding to HT. There were fewer high-grade adverse events in patients treated with T-DM1 versus HT. Neutropenia and diarrhea were more common in patients treated with HT, and thrombocytopenia was more common in patients treated with T-DM1. It is difficult to put in context the results of MARIANNE for the first-line treatment of HER2-positive metastatic breast cancer when one considers the outstanding results from the CLEOPATRA trial, which recently established the combination of trastuzumab, pertuzumab, and docetaxel as the first-line treatment in this setting. In the CLEOPATRA trial, at an updated median follow-up of 50 months, the median OS was improved from 40.8 months with trastuzumab and docetaxel to 56.5 months when pertuzumab was added (HR 0.68, P<0.001).39 Thus, one of the limitations of MARIANNE was the absence of an arm containing trastuzumab, pertuzumab, and a taxane, which would have helped in further defining the role of T-DM1 in the first-line setting. The clinical impact of MARIANNE resides in the lack of benefit of adding pertuzumab to T-DM1 or T-DM1 alone compared to the historical standard of a taxane and trastuzumab. The equivalent results between the T-DM1 arms show no additional benefit with the addition of pertuzumab, demonstrating that the differential biological action of dual HER2 blockade depends largely on the partner drug. These results reject the simplistic idea that T-DM1 is a taxane combined with trastuzumab and teach us about the complexity of the HER2 activation pathway. Given the lack of benefit seen with the addition of pertuzumab to T-DM1, it is unlikely that a future clinical trial would compare this combination with the CLEOPATRA regimen, leaving T-DM1 solely as an indication in the second-line setting and beyond.
Table 1 summarizes the results of the three Phase III trials of T-DM1 mentioned earlier. A surprising finding in all of these studies, including CLEOPATRA, is that the absolute magnitude of improvements in OS are greater than the absolute magnitude of improvements in PFS, as measured by months. This observation is seen across all lines of therapy and contrasts with the survival benefits seen with other drugs in breast cancer. The reasons for the discrepancy between the absolute benefit in PFS and OS are unclear; it is possible that by blocking HER2 in different mechanisms with these novel agents, the cancer cells may be more sensitive to postprogression treatments. However, none of the trials have published details about subsequent therapies and their impact on survival, making the interpretation of these findings more difficult.
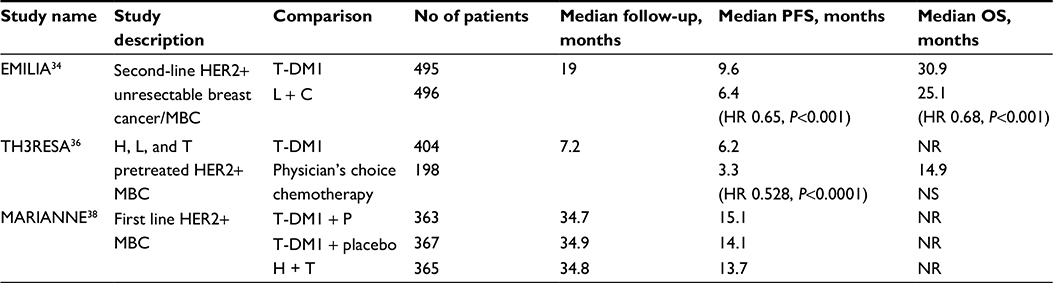 | Table 1 Summary of reported Phase III trials with T-DM1 |
Multiple clinical trials are currently ongoing in different settings evaluating T-DM1 alone and in combination with pertuzumab and other potential targets in breast cancer (Table 2). The results of three main Phase III trials – KATHERINE, KAITLYN, and KRISTINE – evaluating the role of T-DM1 in the neoadjuvant and adjuvant settings are eagerly awaited. These large adjuvant trials have the potential to improve outcomes in HER2-positive breast cancer beyond trastuzumab, which has been the standard adjuvant treatment for more than a decade.
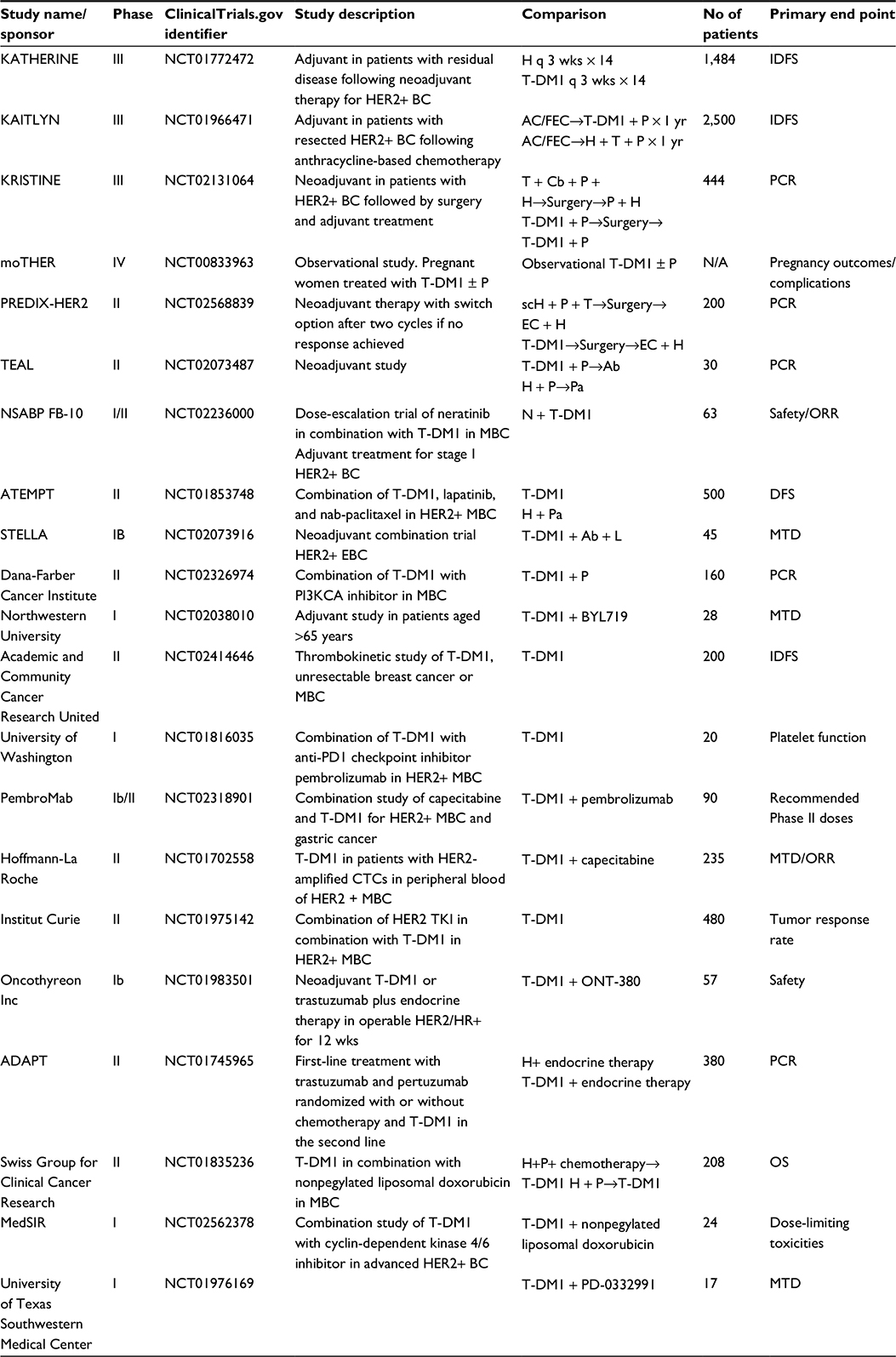 | Table 2 Ongoing trials evaluating T-DM1 in breast cancer |
Mechanisms of resistance to T-DM1
Although most patients with HER2-positive breast cancer will derive benefit from treatment with T-DM1 as shown in the abovementioned studies, unfortunately resistance eventually develops and remains a substantial problem. Resistance also affects patients who despite being HER2 positive will not experience any benefit from the therapy. The exact molecular mechanisms by which the cancer cells are refractory to the cytotoxic activity of T-DM1 are largely unknown. However, several hypotheses have been formulated based on the mechanism of action of the drug and on data collected from clinical trials.
Since binding of T-DM1 to the HER2 epitopes is a required first step in the cytotoxic process, one of the postulated resistance mechanisms is that cancer cells lose the HER2 expression, therefore preventing the binding of the drug and posterior internalization. There are preclinical models of T-DM1 resistance that show clear downregulation of the expression of HER2, which are in line with this hypothesis.40 However, retrospective data have shown that patients who develop disease progression after T-DM1 can still respond to other HER2-targeted agents.41 This suggests that either the loss of HER2 expression may not be involved with resistance or other mechanisms beyond downregulation of HER2 may be more relevant. The factors that affect intracellular levels of DM1, such as poor lysosomal degradation of T-DM1 and drug efflux pumps, might confer tumor resistance by preventing the drug reaching cytotoxic intracellular levels.25
Another mechanism of resistance could be related to alterations in the Vinca site at microtubules, affecting the mechanism of action of microtubule inhibitors like DM1. Finally, neuregulin b1, which is the ligand of HER3, can inhibit the cytotoxic activity of T-DM1 in breast cancer cell lines.42 On the other hand, a recent exploratory analysis of the EMILIA trial suggested that PIK3CA mutations might not be associated with T-DM1 resistance.43
Conclusion
The treatment of HER2-positive breast cancer is changing rapidly. Although the target has not changed, our understanding of the tumor biology and signaling pathways in HER2-positive tumors has increased tremendously. This now includes new ways of targeting HER2, with the goals of not only inhibiting its signaling but also using it as a selective target for the delivery of chemotherapy. T-DM1 has unique characteristics that have been shown to be efficacious for the treatment of metastatic breast cancer and to address resistance to trastuzumab. Studies have shown that T-DM1 is safe, with thrombocytopenia and elevated transaminases being the most important side effects. The benefits in OS are of greater magnitude than the benefits in PFS. However, several questions remain to be answered. There is an urgent need to identify mechanisms of resistance to T-DM1, which should be analyzed in future studies. The results of ongoing trials will assist us in further defining the role of T-DM1 in HER2-positive breast cancer and provide insights into the population of patients who derive the greatest benefit from this drug.
Acknowledgment
We want to thank The University of Iowa Libraries for supporting this publication.
Disclosure
Maximo de la Vega and Enrique Díaz-Cantón are members of the advisory board of Roche. The other authors report no conflicts of interests in this work.
References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. | ||
Cancer Genome Atlas Network. Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70. | ||
Owens MA, Horten BC, Da Silva MM. HER2 amplification ratios by fluorescence in situ hybridization and correlation with immunohistochemistry in a cohort of 6556 breast cancer tissues. Clin Breast Cancer. 2004;5(1):63–69. | ||
Lemmon MA, Schlessinger J. Cell signaling by receptor tyrosine kinases. Cell. 2010;141(7):1117–1134. | ||
Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. | ||
Graus-Porta D, Beerli RR, Daly JM, Hynes NE. ErbB-2, the preferred heterodimerization partner of all ErbB receptors, is a mediator of lateral signaling. EMBO J. 1997;16(7):1647–1655. | ||
Cho HS, Mason K, Ramyar KX, et al. Structure of the extracellular region of HER2 alone and in complex with the Herceptin Fab. Nature. 2003;421(6924):756–760. | ||
Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–792. | ||
Albanell J, Codony J, Rovira A, Mellado B, Gascon P. Mechanism of action of anti-HER2 monoclonal antibodies: scientific update on trastuzumab and 2C4. Adv Exp Med Biol. 2003;532:253–268. | ||
Slamon D, Eiermann W, Robert N, et al. Adjuvant trastuzumab in HER2-positive breast cancer. N Engl J Med. 2011;365(14):1273–1283. | ||
Nagy P, Friedlander E, Tanner M, et al. Decreased accessibility and lack of activation of ErbB2 in JIMT-1, a herceptin-resistant, MUC4-expressing breast cancer cell line. Cancer Res. 2005;65(2):473–482. | ||
Diermeier S, Horvath G, Knuechel-Clarke R, Hofstaedter F, Szollosi J, Brockhoff G. Epidermal growth factor receptor coexpression modulates susceptibility to Herceptin in HER2/neu overexpressing breast cancer cells via specific erbB-receptor interaction and activation. Exp Cell Res. 2005;304(2):604–619. | ||
Lipton A, Goodman L, Leitzel K, et al. HER3, p95HER2, and HER2 protein expression levels define multiple subtypes of HER2-positive metastatic breast cancer. Breast Cancer Res Treat. 2013;141(1):43–53. | ||
Nagata Y, Lan KH, Zhou X, et al. PTEN activation contributes to tumor inhibition by trastuzumab, and loss of PTEN predicts trastuzumab resistance in patients. Cancer Cell. 2004;6(2):117–127. | ||
Berns K, Horlings HM, Hennessy BT, et al. A functional genetic approach identifies the PI3K pathway as a major determinant of trastuzumab resistance in breast cancer. Cancer Cell. 2007;12(4):395–402. | ||
Majewski IJ, Nuciforo P, Mittempergher L, et al. PIK3CA mutations are associated with decreased benefit to neoadjuvant human epidermal growth factor receptor 2-targeted therapies in breast cancer. J Clin Oncol. 2015;33(12):1334–1339. | ||
Nahta R, Yu D, Hung MC, Hortobagyi GN, Esteva FJ. Mechanisms of disease: understanding resistance to HER2-targeted therapy in human breast cancer. Nat Clin Pract Oncol. 2006;3(5):269–280. | ||
Scaltriti M, Rojo F, Ocana A, et al. Expression of p95HER2, a truncated form of the HER2 receptor, and response to anti-HER2 therapies in breast cancer. J Natl Cancer Inst. 2007;99(8):628–638. | ||
Parra-Palau JL, Morancho B, Peg V, et al. Effect of p95HER2/611CTF on the response to trastuzumab and chemotherapy. J Natl Cancer Inst. 2014;106(11). | ||
Baselga J, Norton L, Albanell J, Kim YM, Mendelsohn J. Recombinant humanized anti-HER2 antibody (Herceptin) enhances the antitumor activity of paclitaxel and doxorubicin against HER2/neu overexpressing human breast cancer xenografts. Cancer Res. 1998;58(13):2825–2831. | ||
Neidhart JA, Laufman LR, Vaughn C, McCracken JD. Minimal single-agent activity of maytansine in refractory breast cancer: a Southwest Oncology Group study. Cancer Treat Rep. 1980;64(4–5):675–677. | ||
Cabanillas F, Bodey GP, Burgess MA, Freireich EJ. Results of a phase II study of maytansine in patients with breast carcinoma and melanoma. Cancer Treat Rep. 1979;63(3):507–509. | ||
Press MF, Cordon-Cardo C, Slamon DJ. Expression of the HER-2/neu proto-oncogene in normal human adult and fetal tissues. Oncogene. 1990;5(7):953–962. | ||
Spector NL, Xia W, Burris H 3rd, et al. Study of the biologic effects of lapatinib, a reversible inhibitor of ErbB1 and ErbB2 tyrosine kinases, on tumor growth and survival pathways in patients with advanced malignancies. J Clin Oncol. 2005;23(11):2502–2512. | ||
Barok M, Joensuu H, Isola J. Trastuzumab emtansine: mechanisms of action and drug resistance. Breast Cancer Res. 2014;16(2):209. | ||
Erickson HK, Park PU, Widdison WC, et al. Antibody-maytansinoid conjugates are activated in targeted cancer cells by lysosomal degradation and linker-dependent intracellular processing. Cancer Res. 2006;66(8):4426–4433. | ||
Austin CD, De Maziere AM, Pisacane PI, et al. Endocytosis and sorting of ErbB2 and the site of action of cancer therapeutics trastuzumab and geldanamycin. Mol Biol Cell. 2004;15(12):5268–5282. | ||
Barok M, Tanner M, Koninki K, Isola J. Trastuzumab-DM1 causes tumour growth inhibition by mitotic catastrophe in trastuzumab-resistant breast cancer cells in vivo. Breast Cancer Res. 2011;13(2):R46. | ||
Krop IE, Beeram M, Modi S, et al. Phase I study of trastuzumab-DM1, an HER2 antibody-drug conjugate, given every 3 weeks to patients with HER2-positive metastatic breast cancer. J Clin Oncol. 2010;28(16):2698–2704. | ||
Beeram M, Krop IE, Burris HA, et al. A phase 1 study of weekly dosing of trastuzumab emtansine (T-DM1) in patients with advanced human epidermal growth factor 2-positive breast cancer. Cancer. 2012;118(23):5733–5740. | ||
Burris HA 3rd, Rugo HS, Vukelja SJ, et al. Phase II study of the antibody drug conjugate trastuzumab-DM1 for the treatment of human epidermal growth factor receptor 2 (HER2)-positive breast cancer after prior HER2-directed therapy. J Clin Oncol. 2011;29(4):398–405. | ||
Krop IE, LoRusso P, Miller KD, et al. A phase II study of trastuzumab emtansine in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer who were previously treated with trastuzumab, lapatinib, an anthracycline, a taxane, and capecitabine. J Clin Oncol. 2012;30(26):3234–3241. | ||
Hurvitz SA, Dirix L, Kocsis J, et al. Phase II randomized study of trastuzumab emtansine versus trastuzumab plus docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer. J Clin Oncol. 2013;31(9):1157–1163. | ||
Verma S, Miles D, Gianni L, et al; EMILIA Study Group. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012;367(19):1783–1791. | ||
Welslau M, Dieras V, Sohn JH, et al. Patient-reported outcomes from EMILIA, a randomized phase 3 study of trastuzumab emtansine (T-DM1) versus capecitabine and lapatinib in human epidermal growth factor receptor 2-positive locally advanced or metastatic breast cancer. Cancer. 2014;120(5):642–651. | ||
Krop IE, Kim SB, Gonzalez-Martin A, et al. Trastuzumab emtansine versus treatment of physician’s choice for pretreated HER2-positive advanced breast cancer (TH3RESA): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(7):689–699. | ||
Wildiers H. Trastuzumab emtansine improves overall survival versus treatment of physician’s choice in patients with previously treated HER2-positive metastatic breast cancer: final overall survival results from the phase 3 TH3RESA study, San Antonio Breast Cancer Symposium, SABCS, December 2015; Abstract S5-05. Paper presented at: San Antonio Breast Cancer Symposium, SABCS; 2015; | ||
Ellis PA, Barrios CH, Eiermann W, et al. Phase III, randomized study of trastuzumab emtansine (T-DM1) ± pertuzumab (P) vs trastuzumab+ taxane (HT) for first-line treatment of HER2-positive MBC: primary results from the MARIANNE study. Paper presented at: ASCO Annual Meeting Proceedings; Chicago, 2015. | ||
Swain SM, Baselga J, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724–734. | ||
Lewis Phillips G. Mechanisms of acquired resistance to trastuzumab emtansine (T-DM1). World ADC Summit; 2011; San Francisco, CA. | ||
Olson EM, Lin NU, DiPiro PJ, et al. Responses to subsequent anti-HER2 therapy after treatment with trastuzumab-DM1 in women with HER2-positive metastatic breast cancer. Ann Oncol. 2012;23(1): | ||
Gagliato DM, Jardim DL, Marchesi MS, Hortobagyi GN. Mechanisms of resistance and sensitivity to anti-HER2 therapies in HER2+ breast cancer. Oncotarget. Epub 2016 Jan 27. | ||
Baselga J, Lewis Phillips GD, Verma S, et al. Relationship between tumor biomarkers and efficacy in EMILIA, a phase III study of trastuzumab emtansine in HER2-positive metastatic breast cancer. Clin Cancer Res. Epub 2016 Feb 26. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.