")
Back to Journals » Cancer Management and Research » Volume 12
Normal Absolute Monocyte Count at the Time of Relapse is Associated with Improved Survival After First Salvage Therapy in Adult Patients with Early Relapsed B-Lineage Acute Lymphoblastic Leukemia
Authors Shi Y, Wang N, Huang Z, Chen R, Huang Y, Zhu Y, Xing C, Liang B, Yu K, Feng J
Received 23 May 2020
Accepted for publication 23 July 2020
Published 10 August 2020 Volume 2020:12 Pages 7097—7105
DOI https://doi.org/10.2147/CMAR.S264194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Rudolph Navari
Yi-fen Shi,1,* Na Wang,2,* Zi-yang Huang,1 Rong-rong Chen,1 Yi-sha Huang,1 Yi-yi Zhu,1 Chong-yun Xing,1 Bin Liang,1 Kang Yu,1 Jian-hua Feng1,3
1Department of Hematology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325000, People’s Republic of China; 2Health Care Center, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325000, People’s Republic of China; 3Department of Pediatric Hematology-Oncology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang 325000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian-hua Feng; Kang Yu Department of Hematology
The First Affiliated Hospital of Wenzhou Medical University, Ouhai District, Wenzhou, Zhejiang 325000, People’s Republic of China
Tel +86 577 55578999 extension 669889
Fax +86 577 55578999
Email [email protected]; [email protected]
Background: Peripheral monocytes, a key cell type for innate immunity, have been shown to be associated with survival in various types of hematological malignancies. However, no previous studies regarding the prognostic impact of peripheral absolute monocyte count (AMC) in early relapsed B-lineage acute lymphoblastic leukemia (B-ALL) have been reported.
Methods: Forty-nine cases of early relapsed adult B-ALL were reviewed. The upper (0.80 × 109/L) and lower limits (0.12 × 109/L) of the normal value for AMC were used as cut-off points. Kaplan–Meier curves and Log rank test were used for comparison of overall survival (OS). The univariate and multivariate Cox proportional hazards models were used for investigating the factors associated with OS.
Results: More than half (59.2%) of all patients showed a normal AMC (0.12– 0.80 × 109/L). The median follow-up was 5.3 months from the start of first salvage therapy. Univariate analysis revealed that normal AMC (versus low/high AMC) at the time of relapse was a prognostic factor for improved OS (P = 0.021). On multivariate analysis, normal AMC (versus low/high AMC) at the time of relapse remained an independent prognostic factor for improved OS (hazard ratio = 0.43, P = 0.030).
Conclusion: AMC at the time of relapse, which can be easily derived from routine clinical laboratory testing of complete blood count, might be used as a prognostic marker for survival outcomes in adult patients with early relapsed B-ALL.
Keywords: B-lineage acute lymphoblastic leukemia, early relapse, absolute monocyte count, prognosis, survival
Background
Despite about 90% of adult patients with acute lymphoblastic leukemia (ALL) achieve first complete remission (CR1) with modern first-line induction chemotherapy, more than half of the patients who do achieve CR1 will ultimately relapse.1,2 A second CR (CR2) may be achieved; however, subsequent treatment rarely results in long-term post-relapse survival.3,4 Early relapsed ALL (CR1 <12 months) represents a unique category with specific clinical, biologic, and prognostic features. Compared to those with late relapsed ALL (CR1 ≥12 months), the patients with early relapse appear to have a lower CR2 rate and a reduced post-relapse survival.5 Since only a minority of patients who experience early relapse will derive benefit from salvage therapy, it could be practically important to identify those patients with poor post-relapse life expectancy in order to include them in experimental treatment including palliative care with low-intensity therapies (such as epigenetic modifiers).6
Peripheral monocytes are a key cell type for innate immunity, and play an important role in restoration of tissue integrity and modulation of immunoinflammatory responses.7 In previous studies, monocytopenia has been found to be associated with reduced survival after diagnosis of invasive fungal infections in allogeneic hematopoietic stem cell transplantation (allo-HSCT) recipients.8 More relevantly, in patients with hematological malignancies (such as acute leukemia and multiple myeloma) receiving allo-HSCT, monocytopenia has been shown to be associated with reduced survival.9–11 On the other hand, peripheral monocytes, which reflect the tumor microenvironment, have been revealed to have a prognostic impact in various types of hematological malignancies, including acute myeloid leukemia (AML),12 diffuse large B-cell lymphoma (DLBCL),13 multiple myeloma,14 and Hodgkin’s lymphoma.15,16 To the best of our knowledge, however, no studies regarding the prognostic impact of peripheral absolute monocyte count (AMC) in early relapsed B-lineage ALL (B-ALL) have been previously reported. Thus, the primary purpose of this retrospective study was to evaluate the prognostic significance of AMC at the time of relapse in a cohort of 49 patients with early relapsed B-ALL.
Patients and Methods
Patients
Between November, 2006 and March, 2018, 49 patients with documented B-ALL (excluding mature B-ALL) in early relapse were treated with salvage programs in the First Affiliated Hospital of Wenzhou Medical University. Initial diagnosis of B-ALL was established according to standard criteria, which included morphologic, immunophenotypic, and cytogenetic features. The study was approved by our institutional review board. The requirement for informed consent was waived by the institutional review board due to the retrospective nature of this study, but the confidentiality of patient data was protected. This study complies with the Declaration of Helsinki statement of ethical principles for medical research involving human subjects.
Medical records were reviewed to determine patients’ age, sex, duration of CR1, white blood cell (WBC) count at the time of relapse, cytogenetics, salvage regimens, and responses to salvage regimen. The AMC value was collected from the complete blood count (CBC), and was determined either using the automated routine hematology analyzer XE-2100 or manual differential (in cases flagged for abnormal values). For cytogenetic study, bone marrow (BM) samples at the initial diagnosis were obtained and systematically examined using standard techniques. Unfavorable karyotypes were defined as hypodiploidy (<44 chromosomes), complex karyotype (≥5 chromosomal abnormalities), t(9;22)(q34;q11.2):BCR/ABL1, t(v;11q23):MLL rearrangement, t(1;19) (q23;p13.3):E2A/AML1; favorable karyotypes were defined as hyperdiploidy (51–65 chromosomes), 12p and 14q11 rearrangements; and intermediate risk karyotypes were defined as abnormalities other than those in unfavorable or favorable categories.17–19
Salvage Regimens
Multiple salvage regimens were utilized for B-ALL in early relapse and are grouped into 7 categories as follows: 1) vincristine (or vindesine or vinorelbine), daunorubicin (or doxorubicin or idarubicin or epirubicin or mitoxantrone), and prednisone (or dexamethasone) plus cyclophosphamide (750 mg/m2 for 1–2 doses) (VDCP or VDCP-like) or hyper-fractionated cyclophosphamide (300 mg/m2 every 12 hours for 6 doses) (hyper-CVAD) with/without L-asparaginase, 2) cytarabine administered at conventional doses (50–200 mg/m2/day) in combination with vincristine, prednisone (VP; OAP) and mitoxantrone (NOAP), or cyclophosphamide and 6-mercaptopurine (CAM), 3) high-dose cytarabine (2000 mg/m2 every 12 hours) in combination with methotrexate (1000 mg/m2) (hyper-CVAD[B]), or idarubicin, vindesine and prednisone (IAVP), 4) vindesine (or vinorelbine), prednisone (or dexamethasone) (VP) in combination with mitoxantrone (VNP) or idarubicin (VIP), 5) vinorelbine, prednisone (or dexamethasone) (VP) in combination with cyclophosphamide (VCP), 6) single agents, such as methotrexate, etoposide, and others, 7) miscellaneous treatment combinations, such as vindesine (or vinorelbine) and dexamethasone (or prednisone) alone (VP), or in combination with methotrexate (VPM), or mitoxantrone, teniposide, and methotrexate (VPNTM), or mitoxantrone and ifosfamide; etoposide and methotrexate alone (ME); ifosfamide/mesna in combination with mitoxantrone and etoposide (MINE); and others.
Supportive Care
Supportive care included red blood cell or platelet transfusions, antimicrobial therapy and parenteral nutrition when indicated. Agranulocytosis with fever was treated with empirical antibiotics-piperacillin-tazobactam combination, cefoperazone sodium and sulbactam sodium, imipenem, or meropenem. Patients who did not respond in 72 hours (or earlier if the evidence of hemodynamic changes) received additional voriconazole or the piperacillin-tazobactam combination (or cefoperazone sodium and sulbactam sodium) was changed to imipenem (or meropenem). The addition of vancomycin was considered only if the clinical and/or microbiological data indicated the requirement. Prophylactic antibacterial or antifungal treatment was not a part of the salvage protocols.
Statistical Analysis
The upper (0.80 × 109/L) and lower limits (0.12 × 109/L) of normal value for AMC were used as cut-off points. Categorical variables were compared using the Chi-square test (or Fisher’s exact test where appropriate). Numerical variables were compared by the nonparametric Wilcoxon rank-sum test. Overall survival (OS) was defined as the time from the start of salvage therapy to the date of death or last follow-up. Kaplan-Meier curves and Log rank test were used for comparison of OS. The univariate Cox proportional hazards model was used for investigating the factors associated with OS. Those variables that were P < 0.1 in the univariate analysis were included in the multivariate Cox proportional hazards model. All tests were two-sided and a P of <0.05 was considered statistically significant. All statistical analyses were performed using Stata software (version 12, StataCorp LP, College Station, TX).
Results
Patient Characteristics
The main characteristics of the study cohort are summarized in Table 1. The median age of relapsed patients was 41 years (range, 16–74) and 31 (63.3%) were female. The median duration of CR1 was 3.4 months (range, 0.3–11.4). Chromosomal analysis could be performed at the initial diagnosis in 43 patients. A total of 12 and 31 patients showed unfavorable and intermediate karyotype, respectively. Previous allo-HSCT before first relapse was performed in 2 patients (4.1%). Salvage therapy with VDCP, VDCP-like, or hyper-CVAD was given to 26 (53.1%) patients, whereas other regimens were administered to the remaining 23 (46.9%) patients. Death during salvage therapy occurred in 8 patients (16.3%). The remaining 41 patients were assessed for treatment response after the completion of salvage therapy. The second CR (CR2) was achieved in 23 out of 41 patients (56.1%) receiving salvage therapy.
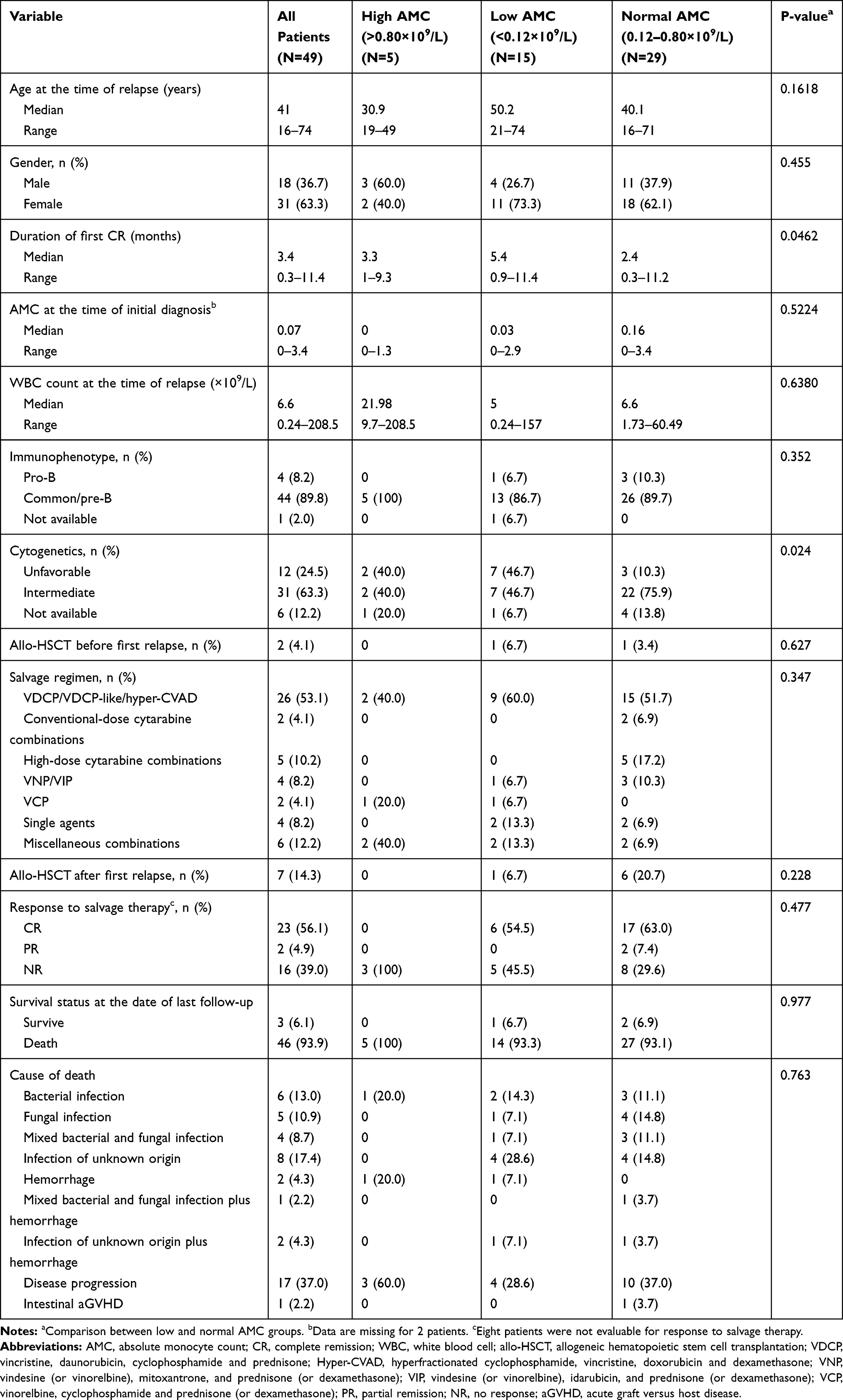 |
Table 1 Patient Characteristics in Early Relapsed Adult B-Lineage Acute Lymphoblastic Leukemia Cohorts |
In this cohort, the median AMC at the time of relapse was 0.30×109/L, with 15 (30.6%), 29 (59.2%), and 5 (10.2%) patients showed low (<0.12×109/L), normal (0.12–0.80×109/L), and high AMC (>0.80×109/L), respectively. Because there was relatively small number (n = 5) in the high AMC category, we further compared the patient characteristics only between the patients with low and those with normal AMC at the time of relapse. Patients with a normal AMC at the time of relapse tended to have a shorter duration of CR1 (P = 0.0462) and a low rate of unfavorable karyotypes (P = 0.024). The patient characteristics according to the AMC at the time of relapse are summarized in Table 1.
Prognostic Impact of AMC at the Time of Relapse
A total of 46 (93.9%) deaths occurred during the present study: 5 (100%) in the high AMC group, 14 (93.3%) in the low AMC group and 27 (93.1%) in the normal AMC group. The most common cause of death was disease progression (N = 3; 60.0%) in the high AMC group, while that was infection alone or in combination (N = 9; 64.3%) in the low AMC group. There was no statistical difference observed in the cause of death between the low and normal AMC groups (P = 0.763) (Table 1).
With a median follow-up duration of 5.3 months from the start of salvage therapy, the 1-year OS rate estimated for the entire cohort was 22±6%. One-year OS rates differed significantly when the three AMC groups were compared (P = 0.0007, Figure 1A). In comparisons between normal and either low or low/high AMC groups, normal AMC patients had a trend to higher one-year OS rate than that of patients with low AMC (31±9% versus 13±9%; P = 0.1141); while low/high AMC patients had a significantly lower one-year OS rate than that of patients with normal AMC (10±7% versus 31±9%; P = 0.0186; Figure 1B). Besides, the univariate analysis using Cox proportional hazards model showed that the following variables were significantly associated with OS: AMC at the time of relapse (normal AMC versus low/high AMC; P = 0.021), salvage regimen (VDCP/VDCP-like/hyper-CVAD versus others; P = 0.035), and response to salvage therapy (partial remission [PR]/no remission [NR] versus CR; P = 0.001). Additionally, the duration of CR1 (6–12 months versus <6 months; P = 0.081) was marginally significantly associated with OS. After adjusting for the above parameters having a P < 0.1 in the univariate analysis, multivariate analysis revealed that AMC at the time of relapse (normal AMC versus low/high AMC) had a significant effect on OS (hazard ratio [HR] = 0.43, 95% confidence interval [95% CI] 0.20–0.92, P = 0.030; Table 2).
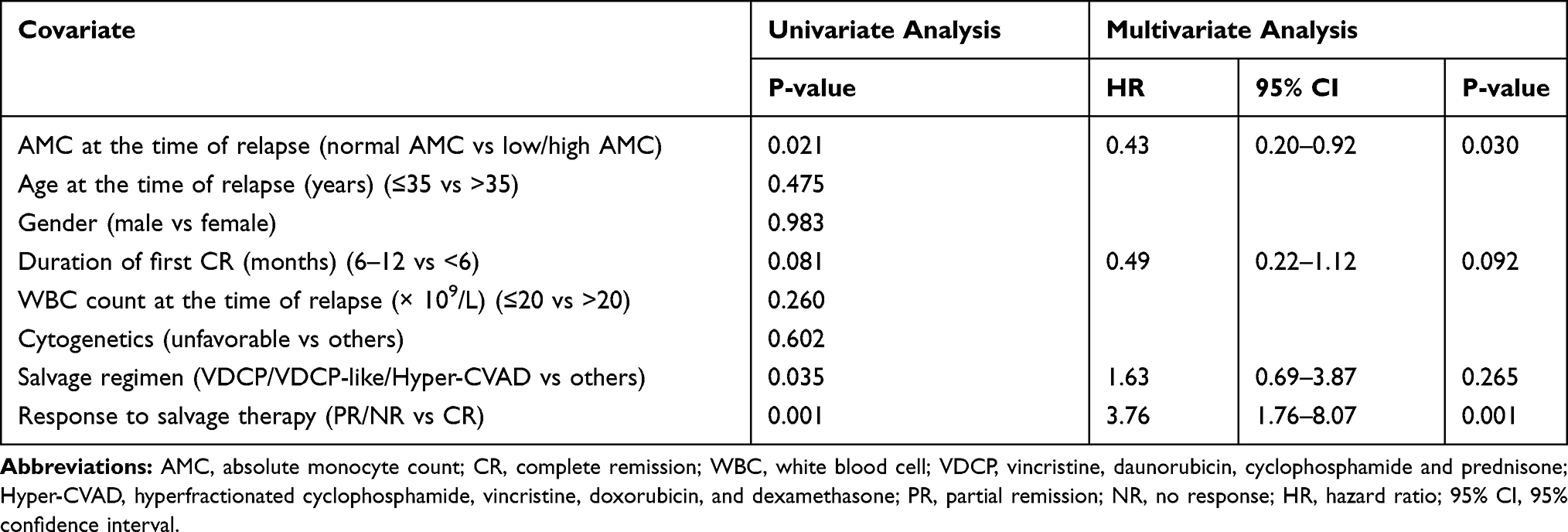 |
Table 2 Univariate and Multivariable Analyses for Overall Survival in Adult Patients with Early Relapsed B-Lineage Acute Lymphoblastic Leukemia |
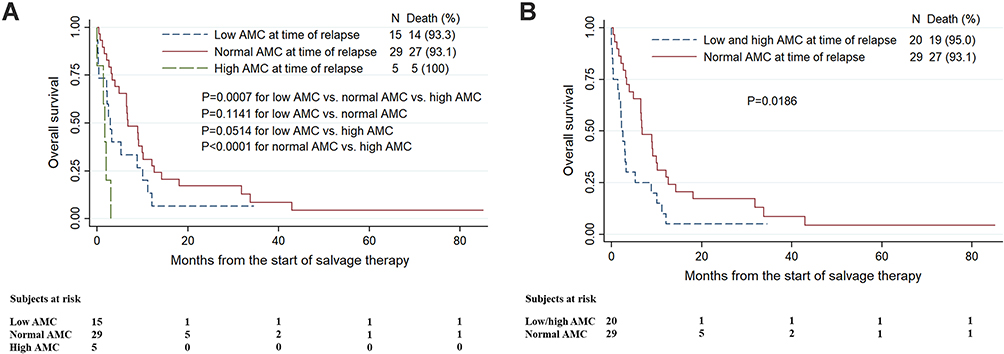 |
Figure 1 Kaplan-Meier estimates of overall survival in 49 early relapsed adult B-lineage acute lymphoblastic leukemia patients stratified by the absolute monocyte count (AMC) observed at the time of relapse are shown. (A) Comparison among low, normal and high AMC groups. (B) Comparison between low/high and normal AMC groups. |
Discussion
To the best of our knowledge, no other studies investigating the role of AMC in early relapsed B-ALL have been published to date. In the current study, we demonstrated that AMC at the time of relapse was associated with risk of death in patients with early relapsed B-ALL. In addition, in order to further verify the above finding, the non-parametric Spearman correlation test was performed to analyze the correlation between AMC and OS in patients with early relapsed B-ALL. The results demonstrated a moderate association (Spearman’s rho = 0.4240, P = 0.0033) between AMC (normal AMC versus low/high AMC) at the time of relapse and OS in early relapsed B-ALL patients who had died at the date of last follow-up. However, although we also investigated the prognostic role of AMC at the time of initial diagnosis in patients with early relapsed B-ALL, no relation between AMC at the time of initial diagnosis and OS was observed (Supplementary Table 1). The evidence linking monocytes at the time of relapse with clinical outcome in early relapsed B-ALL raises the possibility that AMC, the widely available laboratory parameter derived from a CBC, may be easily incorporated into prognostic classification for early relapsed B-ALL.
Monocytes, as a key cell type for innate immunity, have been shown to correlate with both survival and invasive fungal infections in patients with hematological malignancies. Previous studies have noted monocytopenia to be associated with reduced survival in patients with hematological malignancies (such as acute leukemia and multiple myeloma) receiving allo-HSCT.9–11 More importantly, there are also initial studies showed monocytopenia as a risk factor for invasive fungal infections between 40 and 100 days post-allo-HSCT, although this cytopenia has not been consistently identified in multivariable testing.20 However, in allo-HSCT recipients with invasive fungal infections, monocytopenia has been found to be associated with reduced survival.8 Considering that patients with hematological malignancies who receive intensive immuno- or myelosuppressive therapy are at increased risk for infectious complications, not surprisingly then, monocytopenia at the time of relapse, which might be a surrogate for decreased innate immunity, would confer negative prognosis for early relapsed B-ALL patients receiving intensive salvage therapy. In the present study, the most common cause of death in the low AMC group was infection alone or in combination. Unfortunately, however, the infectious agent could not be determined in 5 patients in the low AMC group and 5 patients in the normal AMC group, hampering the further analysis to test the association between fungal infection and AMC at the time of relapse.
On the other hand, elevated AMC at diagnosis has been reported to have a negative prognostic effect in patients with various types of hematological malignancies, including AML,12 DLBCL,13 multiple myeloma,14 and Hodgkin’s lymphoma.15,16 Although the exact mechanism is still unclear, it is well known that monocytes are able to promote tumorigenesis and angiogenesis and contribute to systemic immunosuppression. It is interesting to note that the most common cause of death in the high AMC group was disease progression. Considering that elevated AMC, which reflects increased immunosuppression, could have adverse effect on survival in patients with hematological malignancies as well as low AMC, which reflects decreased innate immunity, not surprisingly then, normal AMC at the time of relapse correlates with improved clinical outcome in patients with early relapsed B-ALL. However, in order to address the above possible mechanisms underlying the prognostic effect of AMC in early relapsed B-ALL, phenotypic and functional analysis of monocyte populations needs to be conducted in future studies. In fact, there are several initial studies focusing on the specific subpopulations of monocytes in ALL. For example, Lima et al demonstrated the presence of immunosuppressive CD14+/HLA-DRlow/− monocytes in pediatric patients with B-ALL.21 In addition, Sulicka et al showed an increase in the intermediate CD14++/CD16+ monocyte count of adult survivors of childhood ALL.22 Importantly, the intermediate CD14++/CD16+ monocytes are considered anti-inflammatory monocytes that can produce large amounts of the immunosuppressive factor interleukin-10.23,24
Awareness of early relapsed B-ALL patients that could benefit from salvage therapy might spare patients with poor prognosis with current salvage regimens and lead to individualized therapy. For example, for the early relapsed B-ALL patients with low AMC at the time of relapse, intensive supportive therapy including prophylactic antibacterials or antifungals might be considered during salvage treatment. While for those with high AMC at the time of relapse, immunomodulatory drugs might be added to the salvage regimens to deplete the immunosuppressive monocytes and thereby enhance antileukemia efficacy.
In the present study, only 21-point difference in the proportion alive at 1 year (31% for normal AMC patients versus 10% for low/high AMC patients) was observed. However, considering only about 26% one-year survival rate reported for B-ALL after first salvage with chemotherapy,3 the small survival difference observed between normal and low/high AMC groups is acceptable. In addition, it should be noted that only a small number of patients (N = 49) were included in the present study to establish a new prognostic factor for early relapsed B-ALL. However, accepting a type I error probability of two-sided 0.05, and assuming the effect size of 21-point difference in the proportion alive at 1 year (31% for normal AMC patients versus 10% for low/high AMC patients) as well as the ratio of 1.45:1 between the sample sizes of normal and low/high AMC groups, a sample size of 49 could achieve 99.92% power. Therefore, our sample is adequately powered to address our research question. Furthermore, in our study, salvage regimen was practically decided by each treating physicians, although some general rules for regimen selection were considered. These included the use of intensified multidrug regimens to treat early relapsed B-ALL. VDCP/VDCP-like/hyper-CVAD were frequently used salvage regimens in the present study and resulted in a CR rate of 54.5%. In addition, high-dose cytarabine continues to be used by many centers for the treatment of relapsed or refractory ALL.25,26 In the present study, among 5 patients who received salvage therapy with high-dose cytarabine combinations there were 3 patients who achieved CR. Clearly, CR rates depend on chemotherapy sensitivity. On the other hand, the response to salvage therapy is probably the most important prognostic factor for relapsed ALL. For example in our study, multivariate analysis demonstrated the response to salvage therapy to be an independent prognostic factor for OS in early relapsed B-ALL patients (HR = 3.76, 95% CI 1.76–8.07, P = 0.001; Table 2). In order to improve the survival outcome of early relapsed B-ALL, new agents, such as proteasome inhibitor bortezomib, antibody- or cell-mediated immunotherapy (for example, rituximab, inotuzumab, blinatumomab, or tisagenlecleucel),27–31 might be added to the salvage regimens to overcome treatment resistance and increase efficacy.
There are several drawbacks in our study. Firstly, as a retrospective study with a small sample size, potential selection bias should be taken into account and our results should therefore be interpreted with caution by clinical physicians. For example, the worse survival outcomes observed in 5 early relapsed B-ALL patients with high AMC at the time of relapse may occur by chance or attribute to other explanations such as unfavorable risk features. Further well-designed randomized clinical trials or observational studies with large patient populations are required to confirm our findings. Secondly, the marked heterogeneity of the patient groups according to cytogenetic risk classification as well as the duration of first CR represents an important drawback of the study. However, it should be noted that cytogenetics was not a significant predictor of patient outcome in this study (Table 2), which corroborates the findings in other series.32,33 The decreased prognostic relevance of cytogenetics at relapse indicated that, by then, disease biology may be more dependent on the in vivo sensitivity to therapy. On the other hand, the duration of first CR (6–12 months versus <6 months) was marginally significantly associated with OS in patients with early relapsed B-ALL (P = 0.092 in multivariate analysis; Table 2). In fact, the multivariate analysis demonstrated the response to salvage therapy to be the strongest independent predictor of OS after relapse (HR = 3.76, 95% CI 1.76–8.07, P = 0.001; Table 2). Therefore, the heterogeneity of the patient groups according to cytogenetic risk classification as well as the duration of first CR would not be a limiting factor for the validity of the present results. In addition, the heterogeneity in treatment regimens (for example, the use of a total of 7 different salvage regimens after relapse) is another limitation of the present study. Besides, some type of allo-HSCT after achievement of CR2 is considered necessary for early relapsed B-ALL. In the present study, however, only 7 in 23 patients with CR2 received allo-HSCT. Furthermore, there are still potential complicating factors that we could not rule out, such as the distribution of high-risk molecular genetics aberrations (for example, IKZF1), which was not examined in the present study because of the limited date. Therefore, the prognostic impact of AMC at the time of relapse in early relapsed B-ALL should be further evaluated in the multivariate context including molecular genetic information.
Conclusion
In summary, this study is the first to show that normal AMC at the time of relapse is associated with improved survival after first salvage in early relapsed B-ALL and could be used as a prognostic marker for survival outcomes. The advantage of our findings is that AMC can be easily derived from routine clinical laboratory testing of CBC. Larger prospective studies are needed to confirm the correlation between AMC at the time of relapse and clinical outcomes in adult patients with early relapsed B-ALL.
Abbreviations
ALL, acute lymphoblastic leukemia; allo-HSCT, allogeneic hematopoietic stem cell transplantation; AMC, absolute monocyte count; AML, acute myeloid leukemia; B-ALL, B-lineage ALL; BM, bone marrow; CBC, complete blood count; CR1, the first complete remission; CR2, the second complete remission; DLBCL, diffuse large B-cell lymphoma; HR, hazard ratio; NR, no response; OS, overall survival; PR, partial remission; WBC, white blood cell; 95% CI, 95% confidence interval.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the institutional review board of the First Affiliated Hospital of Wenzhou Medical University. Consent was waived by the institutional review board due to retrospective nature of this study, yet confidentialities of patients were protected.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rowe JM, Buck G, Burnett AK, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005;106(12):3760–3767. doi:10.1182/blood-2005-04-1623
2. Fielding AK, Richards SM, Chopra R, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood. 2006;109(3):944–950. doi:10.1182/blood-2006-05-018192
3. Gökbuget N, Dombret H, Ribera J-M, et al. International reference analysis of outcomes in adults with B-precursor Ph-negative relapsed/refractory acute lymphoblastic leukemia. Haematologica. 2016;101(12):1524–1533. doi:10.3324/haematol.2016.144311
4. Paul S, Rausch CR, Nasnas PE, Kantarjian H, Jabbour EJ. Treatment of relapsed/refractory acute lymphoblastic leukemia. Clin adv hematol oncol. 2019;17(3):166–175.
5. Oriol A, Vives S, Hernández-Rivas J-M, et al. Outcome after relapse of acute lymphoblastic leukemia in adult patients included in four consecutive risk-adapted trials by the PETHEMA Study Group. Haematologica. 2010;95(4):589–596. doi:10.3324/haematol.2009.014274
6. Helmer J, Iraburu R, Tirado C. Epigenetics of B-ALL. J Assoc Genet Technol. 2019;45(1):10.
7. Biswas SK, Mantovani A. Macrophage plasticity and interaction with lymphocyte subsets: cancer as a paradigm. Nat Immunol. 2010;11(10):889. doi:10.1038/ni.1937
8. Parody R, Martino R, Sánchez F, Subirá M, Hidalgo A, Sierra J. Predicting survival in adults with invasive aspergillosis during therapy for hematological malignancies or after hematopoietic stem cell transplantation: single‐center analysis and validation of the seattle, french, and strasbourg prognostic indexes. Am J Hematol. 2009;84(9):571–578. doi:10.1002/ajh.21488
9. Thoma MD, Huneke TJ, DeCook LJ, et al. Peripheral blood lymphocyte and monocyte recovery and survival in acute leukemia postmyeloablative allogeneic hematopoietic stem cell transplant. Biol Blood Marrow Transplant. 2012;18(4):600–607. doi:10.1016/j.bbmt.2011.08.007
10. DeCook L, Thoma M, Huneke T, et al. Impact of lymphocyte and monocyte recovery on the outcomes of allogeneic hematopoietic SCT with fludarabine and melphalan conditioning. Bone Marrow Transplant. 2013;48(5):708. doi:10.1038/bmt.2012.211
11. Dhakal B, Brazauskas R, Lara CA, Hari P, Pasquini M, D’Souza A. Monocyte recovery at day 100 is associated with improved survival in multiple myeloma patients who undergo allogeneic hematopoietic cell transplantation. Bone Marrow Transplant. 2016;51(2):297. doi:10.1038/bmt.2015.244
12. Feng J, Zhang W, Wu J, et al. Effect of initial absolute monocyte count on survival outcome of patients with de novo non-M3 acute myeloid leukemia. Leuk Lymphoma. 2016;57(11):2548–2554. doi:10.3109/10428194.2016.1166491
13. Tadmor T, Fell R, Polliack A, Attias D. Absolute monocytosis at diagnosis correlates with survival in diffuse large B‐cell lymphoma—possible link with monocytic myeloid‐derived suppressor cells. Hematol Oncol. 2013;31(2):65–71. doi:10.1002/hon.2019
14. Shin S-J, Roh J, Kim M, et al. Prognostic significance of absolute lymphocyte count/absolute monocyte count ratio at diagnosis in patients with multiple myeloma. Korean J Pathol. 2013;47(6):526. doi:10.4132/KoreanJPathol.2013.47.6.526
15. Porrata LF, Ristow K, Habermann TM, et al. Peripheral blood lymphocyte/monocyte ratio at diagnosis and survival in nodular lymphocyte‐predominant Hodgkin lymphoma. Br J Haematol. 2012;157(3):321–330. doi:10.1111/j.1365-2141.2012.09067.x
16. Porrata LF, Ristow K, Colgan JP, et al. Peripheral blood lymphocyte/monocyte ratio at diagnosis and survival in classical Hodgkin’s lymphoma. Haematologica. 2012;97(2):262–269. doi:10.3324/haematol.2011.050138
17. Wetzler M. Cytogenetics in adult acute lymphocytic leukemia. Hematol Oncol Clin North Am. 2000;14(6):1237–1249. doi:10.1016/S0889-8588(05)70184-2
18. Pullarkat V, Slovak ML, Kopecky KJ, Forman SJ, Appelbaum FR. Impact of cytogenetics on the outcome of adult acute lymphoblastic leukemia: results of Southwest Oncology Group 9400 study. Blood. 2008;111(5):2563–2572. doi:10.1182/blood-2007-10-116186
19. Moorman AV, Harrison CJ, Buck GA, et al. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood. 2006;109(8):3189–3197. doi:10.1182/blood-2006-10-051912
20. Garcia-Vidal C, Upton A, Kirby KA, Marr KA. Epidemiology of invasive mold infections in allogeneic stem cell transplant recipients: biological risk factors for infection according to time after transplantation. Clin Infect Dis. 2008;47(8):1041–1050. doi:10.1086/591969
21. Lima DS, Lemes RPG, Matos DM. Immunosuppressive monocytes (CD14(+)/HLA-DR(low/-)) increase in childhood precursor B-cell acute lymphoblastic leukemia after induction chemotherapy. Med Oncol. 2018;35(3):36. doi:10.1007/s12032-018-1092-9
22. Sulicka J, Surdacki A, Mikolajczyk T, et al. Elevated markers of inflammation and endothelial activation and increased counts of intermediate monocytes in adult survivors of childhood acute lymphoblastic leukemia. Immunobiology. 2013;218(5):810–816. doi:10.1016/j.imbio.2012.09.003
23. Skrzeczynska-Moncznik J, Bzowska M, Loseke S, Grage-Griebenow E, Zembala M, Pryjma J. Peripheral blood CD14high CD16+ monocytes are main producers of IL-10. Scand J Immunol. 2008;67(2):152–159. doi:10.1111/j.1365-3083.2007.02051.x
24. Wong KL, Tai JJ, Wong WC, et al. Gene expression profiling reveals the defining features of the classical, intermediate, and nonclassical human monocyte subsets. Blood. 2011;118(5):e16–e31. doi:10.1182/blood-2010-12-326355
25. Kantarjian HM, Estey EH, Plunkett W, et al. Phase I-II clinical and pharmacologic studies of high-dose cytosine arabinoside in refractory leukemia. Am J Med. 1986;81(3):387–394. doi:10.1016/0002-9343(86)90287-1
26. Dinner S, Lee D, Liedtke M. Current therapy and novel agents for relapsed or refractory acute lymphoblastic leukemia. Leuk Lymphoma. 2014;55(8):1715–1724. doi:10.3109/10428194.2013.856428
27. Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med. 2016;375(8):740–753. doi:10.1056/NEJMoa1509277
28. Maury S, Chevret S, Thomas X, et al. Rituximab in B-lineage adult acute lymphoblastic leukemia. N Engl J Med. 2016;375(11):1044–1053. doi:10.1056/NEJMoa1605085
29. Zahid MF. The role of bortezomib in the treatment of acute lymphoblastic leukemia. Future Oncol. 2016;12(16):1861–1864. doi:10.2217/fon-2016-0126
30. Kantarjian H, Stein A, Gokbuget N, et al. Blinatumomab versus chemotherapy for advanced acute lymphoblastic leukemia. N Engl J Med. 2017;376(9):836–847. doi:10.1056/NEJMoa1609783
31. Leahy AB, Elgarten CW, Grupp SA, Maude SL, Teachey DT. Tisagenlecleucel for the treatment of B-cell acute lymphoblastic leukemia. Expert Rev Anticancer Ther. 2018;18(10):959–971. doi:10.1080/14737140.2018.1512411
32. Chucrallah AE, Stass SA, Huh YO, Albitar M, Kantarjian HM. Adult acute lymphoblastic leukemia at relapse. Cytogenetic, immunophenotypic, and molecular changes. Cancer. 1995;76(6):985–991. doi:10.1002/1097-0142(19950915)76:6<985::AID-CNCR2820760611>3.0.CO;2-G
33. Specchia G, Mininni D, Guerrasio A, Palumbo G, Pastore D, Liso V. Ph positive acute lymphoblastic leukemia in adults: molecular and clinical studies. Leuk Lymphoma. 1995;18(Suppl 1):37–42. doi:10.3109/10428199509075301
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.