")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Nonsuicidal Self-Injury: Diagnostic Challenges And Current Perspectives
Authors Hooley JM , Fox KR , Boccagno C
Received 20 July 2019
Accepted for publication 15 October 2019
Published 10 January 2020 Volume 2020:16 Pages 101—112
DOI https://doi.org/10.2147/NDT.S198806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Jill M Hooley, 1 Kathryn R Fox, 2 Chelsea Boccagno 1
1Department of Psychology, Harvard University, Cambridge, MA 02138, USA; 2Department of Psychology, University of Denver, Denver, CO 80210, USA
Correspondence: Jill M Hooley
Department of Psychology, Harvard University, 33 Kirkland Street, Cambridge, MA 02138, USA
Tel +1617 495-9508
Email [email protected]
Abstract: Nonsuicidal self-injury (NSSI) involves deliberate and intentional injury to body tissue that occurs in the absence of suicidal intent. Typical examples here might include self-cutting, burning, or self-hitting. Behavior of this kind is fundamentally unsettling as well as perplexing. It is also the case that self-harming behavior of any kind runs counter to a fundamental survival instinct. In the past, behaviors such as these were viewed as self-mutilation and considered to be a form of attenuated suicide. Much has changed over time, culminating in the entry of NSSI Disorder into DSM-5 as a condition in need of further study. In this review we describe the evolution of the NSSI construct and consider current issues in its diagnosis and assessment.
Keywords: nonsuicidal self-injury; NSSI, NSSI disorder, self-harm, suicide, DSM-5, diagnosis
Background
To begin to understand something, we must be able to identify and define it. Unless terms and concepts are clear, scientific progress will naturally be slow. Over the last 20 years, the study of what we now call nonsuicidal self-injury (NSSI) has become a topic of widespread interest. In this review, we trace the evolution of NSSI as an independent clinical construct, highlighting recent developments in the conceptualization of NSSI and drawing attention to the issues and challenges that remain.
Historical Perspective
Clinical interest in behaviors that involve intentional acts of self-injury dates back to the 1930s and to the psychoanalyst Karl Menninger. Menninger used the term self-mutilation, considering such acts to be a form of attenuated suicide.1 Following this, in the early literature, all nonfatal and deliberate forms of self-injury were viewed as suicide attempts, regardless of whether there was any expressed suicide intent.2,3 Not everyone endorsed such an approach, however. Writing in 1969, Kreitman, Philip, Greer, and Bagley noted that, “the great majority of patients so designated are not in fact attempting suicide” (pp 746–7).4 Others complained that the term ‘attempted suicide’ is now misapplied to acts with a wide variety of intentions […], all of which are expressed in similar types of behavior, namely acts of self-poisoning or self-injury. (pp. 31)5
Reinforcing this point, in 1983, Pattison and Kahan6 noted that not all self-harming behaviors could be classified as suicidal; instead, they observed that many people will intentionally cause physical harm and damage to themselves without any intent to kill themselves.
In addition to debate about the motivation for self-injurious acts, the proliferation of descriptive terms to describe self-destructive behaviors created confusion.7,8 Terms such as “parasuicide”,4 “self-injury”,5,9 delicate self-cutting syndrome,10 and “deliberate self-harm” or “non-fatal deliberate self-harm”11 have all been used to describe self-injurious behaviors that did not result in death. This has been the case regardless of whether or not suicide intent was reported.
In recent years, however, support has grown for a more intent-based definition of suicidal behavior.12 In his widely acclaimed 1987 book, Bodies Under Siege, Armando Favazza13 described both historical and current manifestations of self-mutilation and set the stage for systematic research on this topic. He also defined self-mutilation as “the deliberate destruction or alteration of one’s body tissue without conscious suicidal intent.” (see14 page xviii). Although intent is difficult to measure, recognition of the importance of intent in the definition of suicide and non-fatal suicidal behaviors has allowed the study of NSSI to advance. More specifically it has facilitated the separation of self-injurious behavior (a broad and general category) into suicidal behavior (which involves the presence of at least some intent to die) and nonsuicidal self-injurious behavior. In the latter case, there is no intent to die.
What Do We Mean By NSSI?
For a behavior to be classified as NSSI (according to both Favazza’s definition and the DSM-5 diagnostic criteria) it must be intentional and deliberate. Accidentally cutting oneself is not NSSI. However, in some instances, the role of intentionality can be challenging to establish. For example, NSSI sometimes occurs during dissociative episodes.15 If the person engages in NSSI when they are detached from reality, can the NSSI be considered intentional? Of course, if the motivation for self-injury in such instances is to feel something, some degree of intentionality may perhaps be assumed. Nonetheless, the example of self-injury occurring in the context of dissociation highlights the importance of developing a clearer definition for intentionality to the extent that this is possible.
As we have noted and as the name itself suggests, NSSI must also be nonsuicidal. Although there is intent to self-injure, there is no intent to die. Additionally, as currently conceptualized and as codified in the DSM-5 criteria, NSSI must be direct, meaning there should be no intervening steps between the action and the injury.8 This excludes most forms of self-poisoning (with the exception of swallowing something such as bleach that burns mouth tissue) from being classified as NSSI.17 NSSI also does not include socially sanctioned behaviors. For mainstream Western cultures, this restriction primarily excludes behaviors such as body piercings and tattoos. However, we need to recognize here that different cultures and subcultures sanction different body modification practices.16
The extent of bodily damage is also relevant. NSSI involves a moderately intense injury.16 Use of the word moderate, however, does not mean that the self-injury is of little clinical concern. Most definitions include some variant of “destruction of body tissue,” and the current DSM-5 definition specifies bleeding or bruising. The key point here is that more minor and highly normative behaviors such as lip-biting, scab-picking, and nail-biting are not considered NSSI (although they are sometimes included in assessment measures). Skin picking and hair pulling are also excluded. When mild, these behaviors cause little bodily damage. And when severe, a different and more problem-specific diagnosis of skin excoriation disorder (in the former case) or trichotillomania (in the latter case) may be warranted. It should be noted, however, that the type of behavior a person engages in does not invariably dictate the degree of bodily damage that occurs. Severe damage could, in theory, be caused by behavior that might otherwise be considered mild and normative (eg, lip biting). In such cases, this behavior might appropriately be considered to be NSSI.
In addition, major self-injury, such as might occur in people with psychosis, is excluded from DSM-5 criteria. Such behavior is infrequent (eg, once in a lifetime) and involves extreme behaviors such as removing an eye or severing a limb.8 Finally, NSSI must be distinguished from the stereotypic self-injury that occurs in many developmental disorders. Stereotypic self-injury (eg, repetitive head-banging), often occurs at very high frequencies (many times per hour). The behavior is fixed and rhythmic in nature.8 It also tends to serve functions distinct from those reported among people who engage in NSSI. More specifically, it is routinely performed in front of other people and in the absence of shame and guilt.18 For these reasons, stereotypic self-harming behaviors are not considered NSSI.
The construct of NSSI has gained widespread acceptance in the USA, Europe, Australia, and many other parts of the world. Nonetheless, some researchers continue to advocate for combining all non-fatal self-injurious behaviors into one category of “self-harm.” Kapur et al19, for example, have argued that naming these behaviors “NSSI” is inaccurate given that they are highly comorbid with suicidal behavior. They also note that it is relatively common for people who engage in self-harming behaviors (such as self-poisoning) to report being ambivalent about living or dying (also see20). This calls into question the extent to which NSSI is indeed nonsuicidal. We consider this next.
How Nonsuicidal Is NSSI?
By definition, NSSI must occur in the absence of suicidal intent. Yet NSSI can hardly be considered entirely nonsuicidal. NSSI and suicidal thoughts and behaviors frequently co-occur. This has been noted in community and clinical samples, across age groups, and across sexes (see21 for a review). In addition to strong concurrent associations, NSSI longitudinally predicts suicidal thoughts and behaviors and the strength of this relationship is as strong (or even stronger) than that observed for suicidal thoughts and behaviors.22
It is also the case that many people engage in NSSI behaviors while (at times) experiencing thoughts of suicide, and even with a hope that they might die from these behaviors. Nonetheless, suicidal thoughts and hopes for death are markedly higher in suicidal behaviors so there is a difference in degree.23,24 In addition, and reminiscent of Menniger’s1 idea of attenuated suicide, there is evidence that people may engage in NSSI as a way to avoid acting on thoughts of suicide.25 Indeed, several studies demonstrate that people may engage in NSSI to help cope with, and prevent themselves from acting on, suicidal thoughts.26–28 In other words, for some people, self-harming via NSSI may serve to regulate and reduce suicidal thoughts and intentions. It is important to note, however, that not everyone who engages in NSSI does so for this reason, and the majority of people who engage in NSSI report multiple functions for these behaviors.29
Together, this work highlights that NSSI and suicidal thoughts and behaviors overlap in meaningful and non-trivial ways. Despite these overlaps, we maintain that it is still useful to categorize NSSI and suicidal behaviors as distinct. Many people who engage in NSSI deny any current or prior suicidal thoughts and behaviors.24 Similarly, many people who report suicidal thoughts and behaviors do not engage in NSSI behaviors. Indeed, most people engaging in NSSI endorse using these behaviors to help regulate emotion.29 Nonetheless, research seeking to understand the overlap among these behaviors could shed light on why these behaviors are comorbid, and could provide important insights into both treatment and prevention.
Other Forms Of Self-Harming Behaviors
NSSI is not the only way that people can hurt themselves. Other behaviors, such as drinking too much alcohol, using drugs and sharing needles, engaging in risky behaviors, or engaging in disordered eating behaviors immediately come to mind. Intentional poor medication adherence for a physical illness such as diabetes or heart disease could provide a further example. As with NSSI, each of these behaviors can cause physical harm, physical pain, and negative consequences in both the short- and longer-term.
As stated earlier, NSSI requires direct and intentional infliction of harm, and the harm inflicted must occur immediately after the behavior itself (eg, blood/wound immediately after self-cutting).8 In the case of most indirectly harmful behaviors, immediate personal harm is not a primary motivator of the behavior, and any physical harm and/or pain occurs downstream of the behavior itself. Yet direct and indirect forms of self-injury often co-occur. For example, nearly 25% of people who engage in NSSI report disordered eating behaviors,30 and just over 25% of people who are diagnosed with anorexia nervosa or bulimia nervosa report comorbid NSSI.31 There is also evidence that people report engaging in these eating disordered behaviors with some intent to cause physical harm – both in the moment and in the longer-term.24 This is especially so for those who engage in restrictive eating. On average, such individuals report a greater desire to hurt themselves in the longer-term via restrictive eating than do people who engage in binge eating or who use other compensatory behaviors. What this suggests is that traditionally defined “indirect” self-harming behaviors may have some directly harmful intentions in common with NSSI.
Nonetheless, distinguishing between direct and indirect forms of self-injury may be warranted. Although people who engage in direct and indirect forms of self-harm share many similarities,32,33 there are also some key differences. For example, St. Germain and Hooley32 compared people who engaged in both NSSI and indirect forms of self-harm with people who engaged in only indirect forms of self-harm (e.g., disordered eating, substance abuse, staying in abusive relationships, reckless behaviors). Results showed that those who engaged in both NSSI and indirectly harmful behaviors reported higher levels of self-criticism and increased suicide proneness compared to those who engaged only in indirect forms of self-harm. Of course, this single study involved only a relatively small sample of participants and combined different forms of indirect self-injury (eg, disordered eating, substance abuse, staying in an abusive relationship, reckless behaviors) together. More research is now needed to examine this issue in a more systematic manner.
Especially valuable will be research that examines whether and how people who engage in specific forms of indirect self-injury differ from individuals who engage in NSSI. As an illustration, researchers are now examining the similarities and differences between individuals with disordered eating and those who engage in NSSI.34 We also need to know whether the extent of these differences varies depending on the type of indirect self-injury examined.
The key point here is that self-injurious behaviors may be better understood as lying on a spectrum rather than as entirely distinct categories of behaviors. It is likely that direct self-harming intentions differ across individuals and even within individuals across time. Researchers and clinicians seeking to understand the motivations underlying the broad spectrum of these behaviors may gain important insights by asking questions about self-harming intentions rather than automatically assuming their absence based on the specific behavior or behaviors reported. For example, some people who engage in indirectly self-injurious behaviors may fail to be recognized as being in need of treatment for self-harming thoughts and behaviors because of the assumptions that clinicians already have about the motivations for their behavior (eg, addiction, fear of gaining weight, etc.). Work of this kind thus has implications for access to treatment as well as the type of intervention that a given individual may receive. It may also encourage us to reevaluate (or perhaps re-affirm) the boundaries of what we currently consider to be NSSI.
Why Are Definitions Important?
Definitional issues are important for several reasons, including their impact on prevalence estimates. Most clinicians and NSSI researchers are primarily interested in people who engage in what we have termed moderate NSSI behaviors, particularly individuals who engage in these behaviors frequently. Unfortunately, many NSSI studies, particularly those relying on self-report assessment instruments, capture infrequent and minor NSSI behaviors. This leads to inflated NSSI rates. For example, Lloyd-Richardson et al35 found that 55 percent of an adolescent community sample endorsed some form of NSSI behavior. This was reduced to 27.7% when only moderate NSSI (eg, self-cutting, burning) was considered, and fewer than 5% of respondents endorsed engaging in moderate NSSI behaviors more than five times. Similarly, Tang et al36 found that 33.6% of a large sample of Chinese adolescents endorsed some kind of NSSI, but only 11.9% endorsed moderate NSSI; fewer than 1% reported engaging in moderate NSSI behaviors more than five times. These discrepancies in prevalence estimates highlight the importance of having consensus definitions that map on to conceptually coherent and clinically meaningful behaviors. For example, minor (ie, behaviors that cause mild pain and/or temporary harm; picking at a scab) and moderate NSSI appear to be qualitatively different phenomena. Compared to minor NSSI, moderate NSSI tends to be associated with greater psychopathology, as well as more psychiatric hospitalizations, suicide ideation, and suicide attempts.35,37–39
Is NSSI A Symptom Or A Distinct Clinical Condition?
NSSI has been included as a symptom of borderline personality disorder since personality disorders first officially entered the DSM in 1980.40 Even today, many clinicians and researchers continue to view NSSI in terms of borderline personality disorder. However, within the past several years this perception has been changing. Research has demonstrated that NSSI is associated with a range of internalizing, externalizing, and personality disorders, and can even occur in the absence of any psychiatric diagnosis.41–43 In short, there is substantial evidence that NSSI is distinct from borderline personality disorder and all other psychiatric diagnoses. Reflecting this, NSSI disorder (NSSI-D) entered DSM-5 in 2013 as a Condition for Further Study.44
NSSI-D In DSM-5
The diagnostic criteria for NSSI-D are summarized in Table 1. Criterion A concerns the frequency and duration of NSSI. More specifically, to meet the criterion, “intentional self-inflicted damage”44 must have occurred on 5 or more days over the past year. This threshold was based on the idea that five or more acts of NSSI provided evidence of a repetitive problem.45
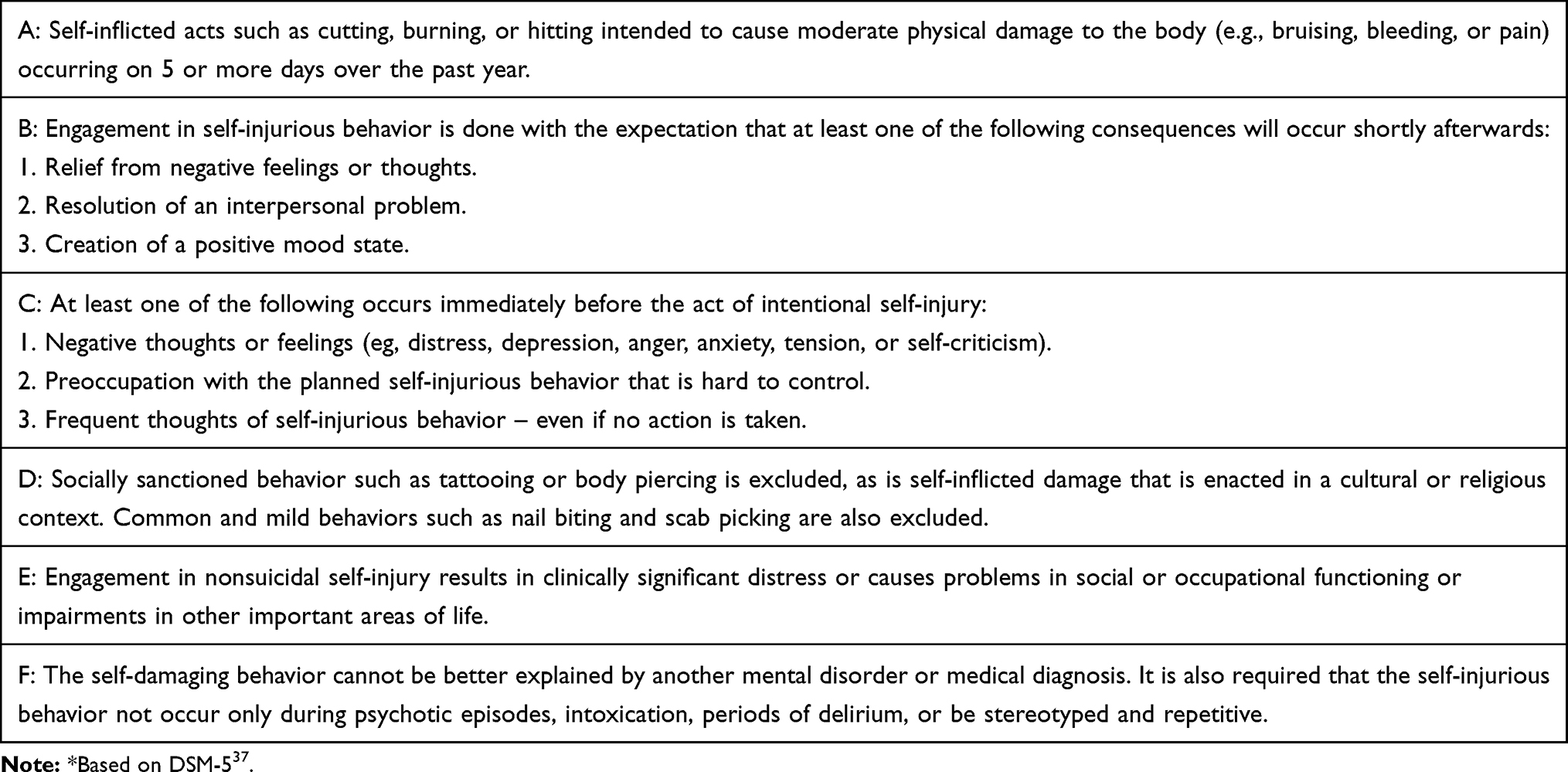 |
Table 1 NSSI Disorder: Summary of Proposed Diagnostic Criteria* |
A key issue, however, is whether the threshold of five NSSI days in the past year is too low to meaningfully differentiate between clinical and subclinical groups of people who engage in NSSI. Although many clinicians might reasonably be concerned if a patient or client showed evidence of NSSI behavior on five or more occasions over a one-year period, NSSI researchers have noted that a higher threshold might provide better separation between individuals meeting diagnostic criteria for NSSI-D and individuals who are subthreshold. For example, in a sample of community adults, Andover46 found that those diagnosed with NSSI-D engaged in NSSI on 86 days (mean frequency) in the past year compared to only 6 days for those who did not meet diagnostic criteria. A similar discrepancy was noted by Washburn et al47 using a clinical sample. In that study, the NSSI-D group engaged in NSSI on an average of 76.8 days compared to a mean of 1.9 days for the non-disordered group. Using a discriminant function analysis approach with a large sample of adolescent inpatients, Muehlenkamp et al47 identified 3 different groups. An NSSI frequency of 25 or more days represented the most severe group and a frequency of 5–24 days identified a group with relatively less overall pathology compared to a low frequency (1–4 days) group.
Taken together, these findings suggest that raising the frequency cut-off beyond that currently proposed in DSM-5 may be warranted. Nevertheless, as Muehlenkamp et al48 also note, the current threshold of 5 NSSI days may validly identify those in need of clinical attention. Early intervention with such individuals might prevent the development of a more severe disorder with more associated psychopathology as well as greater suicidal thoughts and plans. To the extent that this is the case, a frequency of five acts or episodes of NSSI on at least 5 days over the past year may be both clinically meaningful and give cause for concern.
Criterion B of NSSI-D in the DSM-5 requires that individuals engage in NSSI for one or more of the following reasons: (1) to obtain relief from a negative feeling or cognitive state, (2) to resolve an interpersonal difficulty, or (3) to induce a positive feeling state.44 Although most individuals who engage in NSSI endorse at least one of these three motivations,49,50 other motivations, including self-punishment and coping with suicidal thoughts, are neglected (for a meta-analysis and systematic review of functions of NSSI, see29). Initial research further indicates that most people endorse more than one NSSI function.51 Motivations for NSSI also tend to vary based on other comorbid diagnoses that might be present (eg, posttraumatic stress disorder versus major depressive disorder).52 NSSI motivations may also vary over time as well as being influenced by factors such as culture and race/ethnicity, although research on this topic has not yet been conducted.
More broadly, is a focus on the motivations of NSSI clinically informative? In other words, does Criterion B help to differentiate individuals who do and do not meet diagnostic criteria for NSSI-D? When comparing individuals who do and do not meet the frequency criterion for NSSI-D across both college undergraduates and adolescent and adult patients, Brausch et al51 found that the endorsement of motivations for NSSI was present regardless of NSSI frequency or the sample studied. This finding could be taken as evidence that Criterion B may not add diagnostic value and may not aid in distinguishing between individuals who self-injure and those who meet NSSI-D. However, considering the motivations for self-injury may still be important. In cases where self-injury is motivated by other factors (eg, desire to be part of a group; to intimidate others) this would help create a boundary condition that could be of value to clinicians.
The C Criterion of DSM-5 highlights the thoughts or mood states that are required to accompany self-injurious behavior. These include interpersonal difficulties or negative thoughts or feelings prior to NSSI, preoccupation with NSSI that is hard to control, or frequent thoughts of NSSI even if these are not always acted on. Although these features are clearly related to NSSI engagement, they may not be especially helpful in distinguishing clinically significant NSSI from less severe and more intermittent NSSI. The vast majority of people who engage in NSSI do so in the context of negative thoughts or feelings or following negative interpersonal events.47,50 Moreover, even though one study found that preoccupation with NSSI and difficulties resisting urges to self-injure was reported by fewer than half of a sample of German adolescent inpatients,53 failure to meet Criterion C is almost never the reason that people are not diagnosed with NSSI-D.54 To the extent that this is the case, Criterion C may not be especially informative when it comes to distinguishing between those who engage in self-injury and those warrant a formal NSSI-D diagnosis.
The D criterion is useful, however, because it creates boundary conditions and formally excludes socially sanctioned behaviors such as body piercing. It also excludes very minor and common forms of self-injury such as scab picking or nail biting. In a related manner, the F criterion is helpful because it specifies when self-injurious behavior should not be considered to reflect NSSI-D (eg, when self-injury occurs exclusively in the context of psychosis, or in individuals with developmental disorders as a part of repetitive stereotypies). As we have already noted, not all self-injurious behavior is NSSI. The F Criterion clarifies the contexts where this is the case. Criterion F excludes self-injury that occurs during psychotic episodes, and also specifies other disorders that may involve behaviors that might look like forms of NSSI but are not regarded as such (eg, trichotillomania [hair pulling], excoriation [skin picking]).
Although the F criterion is clearly helpful, care is needed with regard to its interpretation. Excluding acts of self-injury that occur only during episodes of psychosis removes from diagnostic consideration body modification behaviors that result from delusions (eg, belief that this will save the world) or command hallucinations. However, we do not interpret this criterion to mean that any person with a history of psychosis should automatically be excluded from ever receiving a diagnosis of NSSI-D. Much depends on the person’s clinical state at the time of the self-injury as well as their motivations for the behavior (highlighting again the potential value of criterion B). If someone engages in NSSI during periods of remission (eg, when not actively psychotic) and if their behavior meets all other DSM-5 criteria, a diagnosis of NSSI-D would likely be warranted.
Finally, we consider Criterion E. This is a common criterion throughout the DSM and requires that the behavior or its consequences be associated with clinically significant distress or impairment in specified areas of functioning. With respect to NSSI, however, this is potentially problematic. NSSI is often used to improve mood and to alleviate distress. Within the framework of a recent conceptual model, these are considered to be affective benefits.55 This may help explain why a minority of people who meet criteria for NSSI-D report that the behavior has not caused them distress.50 Individuals with a history of NSSI engagement are also not always certain that they want to stop self-injuring.46 Indeed, in one study, only 12% of college students with a NSSI history expressed a desire to stop the behavior (cited in Brausch).56
In contrast, Gratz et al49 found that Criterion E, relative to other NSSI-D criteria, most strongly distinguished between those who did and did not meet criteria for NSSI-D. In assessing Criterion E, Gratz and colleagues adopted a multidimensional approach that required clinicians to make dimensional ratings (0–4 scale) about NSSI-related interference on a variety of indicators of impairment. Although more research on this topic is warranted, the findings of this study suggest that a more comprehensive assessment may be necessary to gauge the extent to which self-injurious behavior causes clinically significant distress or impairment. Because NSSI is often used as a form of emotion regulation, people who engage in self-injury may not always be in the best position to have full insight into the problems such behaviors may cause for them.
When distress and impairment are measured more indirectly, most individuals with NSSI show greater levels of impairment than do those with NSSI who do not meet NSSI-D criteria.52 Specifically, individuals who meet criteria for NSSI-D score higher than those with subthreshold NSSI or no history of NSSI on variables such as past month suicide ideation and attempts, loneliness, and problems with emotion regulation.41 To the extent that these variables can be regarded as proxies for distress and impairment, the validity of Criterion E would seem to be supported. However, one key issue is the extent to which higher scores on measures of psychopathology, life satisfaction, and other variables that are used as proxies might be due to other comorbid conditions (such as depression or borderline personality disorder). What is relevant here is whether NSSI itself is the source of the distress and impairment. At the present time, this is not fully clear. A survey of clinicians found that fewer than 50% considered Criterion E to be a prototypic feature of NSSI-D.57 However, shame and guilt over NSSI often follow engagement in this behavior. If these are considered to be indicators of distress or impairment, the consequences of NSSI are likely to be viewed as more problematic.58 Going forward it will be important to clarify just how Criterion E should be evaluated and what forms of evidence are most valid.
The Assessment Of NSSI
In recent years, several interview-based and self-report measures have been developed to assess NSSI. Just as definitions and terms for NSSI have varied over time, these measures assess NSSI with varying underlying assumptions and language. Ideally, more consensus definitions for NSSI would allow for more consistent assessment of these behaviors across measures. However, to date, the reverse has primarily been true; researchers have adopted definitions consistent with the measures they are using rather than first deciding on an optimal definition.
As a result, NSSI assessments are not always consistent in what they measure. Whereas some include single-items, assessing only the presence or absence of NSSI engagement, others include assessment of numerous NSSI characteristics, including the frequency, functions, contexts, sensations/body parts injured, controllability, and likelihood of continuing these behaviors. The manner in which these characteristics are assessed also varies.
Although a full consideration of all measures assessing NSSI is beyond the scope of this review, in the following sections we provide a brief overview of some of the key attributes of the most commonly used measures. First, however, we highlight three newer instruments designed to assess NSSI-D.
NSSI-Disorder
Most NSSI assessments predate the entry of NSSI-D into the DSM-5 as a condition for further study. As such, they do not formally assess NSSI-D diagnostic criteria. To address this limitation, the Clinician-Administered Non-Suicidal Self Injury Disorder Index (CANDI),49 the Alexian Brothers Assessment of Self-Injury Scale (ABASI),47 and the Non-Suicidal Self-Injury Disorder Scale (NSSIDS)54 have been developed.
Published in 2015, the CANDI assesses all NSSI-D criteria as outlined in DSM-5. Each criterion is assessed with a yes/no question, and follow-up questions assess frequency, duration, intensity, functions, and impairment of NSSI on continuous Likert-type scales. The CANDI has demonstrated adequate internal consistency, construct validity, and interrater reliability in a community sample of young adults who endorsed NSSI.48 However, this measure has not yet been administered to the general community, and the predictive validity of the CANDI across time remains unexamined.49 Nevertheless, this measure shows promise. Notably though, since NSSI-D diagnostic criteria include an extremely narrow inclusion of motives for NSSI, the CANDI does not provide a comprehensive assessment of NSSI functions.
Like the CANDI, the ABASI assesses all NSSI-D diagnostic criteria. However, the ABASI is a self-report measure (it is not clinician administered) and it is designed to assess NSSI-D in individuals who already report engaging in NSSI. The ABASI assesses 21 types of NSSI behaviors, and includes the phrase “to hurt yourself or cause pain” when assessing specific forms of NSSI behaviors (eg, fighting, tattooing, over-exercising, food restriction) to clarify that these behaviors are completed for the explicit purpose of self-injury.47 Consequently, this measure assesses some behaviors (such as food restriction) that do not result in damage to the skin, again raising the question of whether we should include indirect forms of self-injurious behaviors when assessing NSSI-D. The ABASI has demonstrated adequate test–retest reliability and internal consistency in a large and demographically rich sample of patients admitted to an acute treatment program that treats NSSI, and factor analyses indicate that this instrument accurately reflects NSSI-D Criteria A through F. However, given that only one study to date47 has validated this measure, future research on the psychometric properties of the ABASI is needed.
Similar to the ABASI, the NSSIDS,54 also published in 2015, is a self-report measure that assesses diagnostic criteria for NSSI-D. However, this 16-item measure is entirely faithful to current NSSI-D criteria; as such it does not assess other indirectly harmful behaviors such as restrictive eating. The NSSIDS uses Likert-scale items to assess each NSSI-D criterion. It also includes explicit items to identify distress and impairment (Criterion E) following NSSI (eg, “does engaging in self-harm cause you stress?”). Items designed to identify rule-outs for NSSI-D (Criterion F) are also included (eg, “how often do you engage in these behaviors when under the influence of drugs or alcohol?”). In two samples of college students with a history of NSSI, the NSSIDS was shown to have strong internal reliability and construct validity, suggesting that this scale could meaningfully distinguish individuals with self-injury who do and do not meet NSSI-D criteria. However, test–retest reliability and divergent validity for this scale has not yet been assessed. Of note, this research also found that individuals who met NSSI-D criteria exhibited more anxiety and depressive symptoms than did those whose self-injurious behavior did not meet NSSI-D criteria. Additionally, a considerable proportion of individuals who met criteria A through D did not endorse Criterion E. This again raises the notion that individuals who engage in NSSI may often not endorse distress over NSSI given the effective short-term mood benefits of this behavior.
Thoughts About Self-Injury
Thoughts of NSSI are not included in the current DSM-5 diagnostic criteria. However, assessment tools that ask about thoughts can provide insight into risk for first-time or continued NSSI engagement. Some NSSI assessments ask about thoughts of NSSI in addition to actual NSSI engagement. The Self-Injurious Thoughts and Behavior Interview (SITBI),59 for example, is a widely used and comprehensive semi-structured interview for adolescents and adults. One advantage of this measure is that it assesses the presence, frequency, duration, and type of NSSI thoughts and behaviors (in addition to suicidal ideation, plans, preparations, gestures, and attempts).
Severity Of Injury
Two issues emerge when considering assessment of the severity of NSSI. First, assessments vary in whether they include or exclude mild and only slightly damaging self-harming behaviors. For example, several measures including the Functional Assessment of Self-Mutilation (FASM),35 Inventory of Statements about Self-Injury (ISAS),60 and Deliberate Self-Harm Inventory (DSHI)61 provide checklists of different forms of NSSI that include picking at scabs/wounds, rubbing skin against rough objects, and self-pinching. These measures may capture a wider representation of self-harming behaviors, and may be particularly useful in understanding the future risk of moderate self-harming behaviors. However, as we noted earlier, inclusion of these “milder” behaviors in assessment tools may result in higher rates of NSSI endorsement than would be observed using other measures.
Relatedly, some NSSI assessments include behaviors that may be better captured by other forms of psychopathology. For example, the FASM includes hair pulling as a form of NSSI, which may be better accounted for by trichotillomania. The ABASI47 also includes over-exercising; this may be better accounted for by an eating disorder diagnosis. Other assessments include more severe self-harming behaviors, like bone breaking (eg, DSHI).
A second key issue is how to define severity in general. Whereas some researchers consider the degree of tissue damage inflicted, others focus more on the recency or frequency of the behaviors. Although both factors are likely important, lack of consensus on how to define and measure severity is apparent across assessment measures. It is also worth noting that the number of methods used may also be an indicator of severity overall.39,62
Direct Versus Indirect Forms Of Self-Injurious Behavior
Contrary to the requirements listed in the DSM-5 that NSSI be direct, not all NSSI assessments require this criterion. As noted earlier, direct self-injury requires that the behavior immediately results in harm/tissue damage. Behaviors like overdosing on pills would therefore be considered indirect self-injury, as the harm they cause is downstream of the behavior itself.20 Several NSSI measures include these kinds of indirectly self-damaging behaviors (eg, swallowing chemicals, as in the ISAS or over-exercising, as in the ABASI).
Intentionality
Not all NSSI measures clarify that the self-inflicted injury be intentional (eg, Ottawa Self-Injury Inventory [OSI]).63,64 Although some may argue that this is tacit in the measure itself, the degree to which people would say “yes” to harming themselves via accidental injury (eg, accidental overdose, accidental cut while chopping food), without realizing that the assessment concerns intentional self-injury, remains unclear.
Frequency And Recency
Assessment measures often vary in how they determine frequency as well as in the time-frame that they use. Regarding how frequency is operationalized, most assessments examine the number of NSSI episodes engaged in (eg, the SITBI). However, some assessments ask about the number of days in which NSSI is engaged in over different intervals (eg, Non-Suicidal Self-Injury Assessment Tool [NSSI-AT]).65 This approach parallels NSSI-D criteria. Other assessments avoid questions about the specific number of episodes or days, and instead ask participants or interviewers to rate the frequency of behaviors on a Likert-type scale ranging in frequency and intensity. This is the case for the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS)66 for example.
NSSI Functions
Several measures (such as the SITBI, the FASM and the ISAS) include an assessment of NSSI functions. However, the measures tend to vary in the number and types of functions assessed. For example, whereas the FASM assesses 23 functions, including interpersonal and intrapersonal motivations, others assess 13 functions (eg, the ISAS) or a handful of functions (eg, the SITBI). Additionally, there is variability in how these functions are assessed, with some only questioning the frequency with which NSSI is engaged in for a specific function (eg, FASM, SITBI), and others assessing the self-identification with specific functions (eg, ISAS). Consequently, prevalence estimates of functions of NSSI differ considerably depending on the assessment measure that is used.29
Is There A Preferred Assessment Measure?
We are not of the opinion that any single measure of NSSI is best or that any specific measure should be universally used. The measure that any investigator selects should be based on the purpose of the study or the issues under investigation. However, we do believe that the wide range of questions used to assess NSSI, including disparate underlying assumptions and assessment methods, is problematic. Investigators need to be mindful of the strengths and limitations of any measure they employ, carefully considering the issues and concerns noted above. Readers of the NSSI literature should also remain aware that, as mentioned earlier, differences in the definition of NSSI can create large differences in the rates of NSSI observed. A meta-analysis of the prevalence of NSSI conducted by Swannell, Martin, Page, Hasking, and St. John67 reported higher rates of NSSI when checklists of behaviors, rather than open-ended questions, were used. Rates of NSSI endorsement were also higher when participants were anonymous, which is more likely to be the case for self-report compared to interviewer-based assessments. Problems such as these limit reliability and replicability across studies.
Concluding Comments
The addition of NSSI-D into the DSM represents a major step forward for research in this area. A more precise definition brings with it improved communication about what NSSI is and is not. It also provides a catalyst for research into clinically significant NSSI.
We must remember, however that the proposed DSM-5 criteria are exactly that – proposed criteria. They represent a beginning rather than an end point. Whether NSSI should remain categorical (diagnosis versus no diagnosis) or be assessed dimensionally (on a scale of severity) remains an open question. In one study, an ordinal scale of NSSI severity – relative to a categorical item of NSSI-D – was found to relate more closely to measures of psychopathology and impairment.47 Such a finding supports the broader movement in clinical research and practice towards a more dimensional approach to psychopathology symptoms and diagnoses.68
The validity of the current DSM-5 criteria remains to be fully established and many changes are to be expected for the future. An increase in the frequency threshold for Criterion A may be required. A more extensive consideration of the minimum number and types of NSSI motivations that should be covered in Criterion B may also be necessary if this criterion is to remain central to the diagnosis of NSSI-D. Moreover, as Kapur et al19 have noted, the exclusion of non-suicidal self-poisoning leaves this form of self-injurious behavior in the “classificatory wilderness” (see19 pp. 326).
Also unclear at the present time, is where – if it is added to the formal diagnostic nomenclature – NSSI-D will be placed. Given the mood benefits NSSI provides, should we think of it as a variant of an Addictive Disorder? Or does it belong with the Disruptive, Impulse-Control, and Conduct Disorders? Other possibilities might include placing NSSI-D with Depressive Disorders, Anxiety Disorders, OCD and Related Disorders, or perhaps even with Neurodevelopmental Disorders. Yet another option would be to add NSSI as a specifier for other disorders (eg, major depressive disorder with NSSI). However, this approach assumes that other clinical conditions will be present. This is not always the case. Given the current state of knowledge, we believe it is premature to make a specific recommendation on this matter.
Despite these challenges, we agree with Selby et al43 and also with Brausch56 that recognizing NSSI-D brings with it many advantages. Efforts to create a consistent definition of NSSI will improve assessment. In addition to generating better estimates of prevalence in small-scale studies, it will also permit NSSI-D to be included in larger epidemiological studies. Preliminary recognition of NSSI-D is also likely to facilitate treatment development. Specific interventions for NSSI are now being developed.69,70 However, much more needs to be done. Given the link between NSSI and suicide risk, treating NSSI may enhance suicide prevention efforts. This provides a powerful incentive to focus research attention to this area in a timely way.
Acknowledgments
The authors would like to thank Alexandria Onuoha and Zelal Kiliç for their assistance with manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Menninger KA. Man against Himself. Harcourt, Brace: New York; 1938.
2. Stengel E. Enquiries into attempted suicide [abridged]. Proc Roy Soc Med. 1952;45(613):17–24.
3. Stengel E. The complexity of motivations to suicidal attempts. J Ment Sci. 1960;106(445):1388–1393.
4. Krietman N, Philip AE, Greer S, Bagley CR. Parasuicide. Br J Psychiatry. 1969;115(523):746–747.
5. Kessel N. The respectability of self-poisoning and the fashion of survival. J Psychosom Res. 1966;10(1):29–36.
6. Pattison EM, Kahan J. The deliberate self-harm syndrome. Am J Psychiatry. 1983;140:867–872.
7. Hooley JM. Self-harming behavior: Introduction to the special series on non-suicidal self-injury and suicide. Appl Prev Psychol. 2008;12(4):155–158.
8. Nock MK, Favazza AR. Nonsuicidal self-injury: Definition and classification. In: Nock MK, editor. Understanding Nonsuicidal Self-Injury: Origins, Assessment, and Treatment. Washington, DC, US: American Psychological Association; 2009:9–18.
9. Johnson FG, Frankel BG, Ferrence RG, Jarvis GK, Whitehead PC. Self-injury in London, Canada: A prospective study. Can J Public Health. 1975;66:307–316.
10. Pao PE. The syndrome of delicate self-cutting. Br J Med Psychol. 1969;42(3):195–206. doi:10.1111/j.2044-8341.1969.tb02071.x
11. Turner RJ, Morgan HG. Patterns of health care in non-fatal deliberate self-harm. Psychol Med. 1979;9(3):487–492. doi:10.1017/s0033291700032037
12. Posner K, Brodsky B, Yershova K, Buchanan J, Mann J. The classification of suicidal behavior. In: Nock MK, editor. The Oxford Handbook of Suicide and Self-Injury. New York: Oxford University Press; 2014:7–22.
13. Favazza AR. Bodies under Siege: Self-Mutilation in Culture and Psychiatry. Baltimore: John Hopkins Press; 1987.
14. Favazza AR. Bodies under Siege: Self-Mutilation and Body Modification in Culture and Psychiatry. Baltimore: John Hopkins Press; 1996.
15. Calati R, Bensassi I, Courtet P. The link between dissociation and both suicide attempts and non-suicidal self-injury: Meta-analyses. Psychiatry Res. 2017;251:103–114. doi:10.1016/j.psychres.2017.01.035
16. Favazza AR. A cultural understanding of nonsuicidal self-injury. In: Nock MK, editor. Understanding Nonsuicidal Self-Injury: Origins, Assessment, and Treatment. Vol. 1. Washington, DC, US: American Psychological Association; 2009:19–36.
17. Andover MS, Morris BW, Wren A, Bruzzese ME. The co-occurrence of non-suicidal self-injury and attempted suicide among adolescents: Distinguishing risk factors and psychosocial correlates. Child Adolesc Psychiatry Ment Health. 2012;6(1):11. doi:10.1186/1753-2000-6-11
18. Favazza AR. Nonsuicidal self-injury: How categorization guides treatment. Curr Psychiatry. 2012;11(3):21–26.
19. Kapur N, Cooper J, O’Connor RC, Hawton K. Non-suicidal self-injury v. attempted suicide: New diagnosis or false dichotomy? Br J Psychiatry. 2013;202(5):326–328. doi:10.1192/bjp.bp.112.116111
20. Hawton K, Cole D, O’Grady J, Osborn M. Motivational aspects of deliberate self- poisoning in adolescents. Br J Psychiatry. 1982;141:286–291. doi:10.1192/bjp.141.3.286
21. Hamza CA, Stewart SL, Willoughby T. Examining the link between nonsuicidal self-injury and suicidal behavior: A review of the literature and an integrated model. Clin Psychol Rev. 2012;32(6):482–495. doi:10.1016/j.cpr.2012.05.003
22. Ribeiro JD, Franklin JC, Fox KR, et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: A meta-analysis of longitudinal studies. Psychol Med. 2015;46(2):225–236. doi:10.1017/S0033291715001804
23. Fox KR, Millner AJ, Franklin JC. Classifying nonsuicidal overdoses: Nonsuicidal self-injury, suicide attempts, or neither? Psychiatry Res. 2016;244:235–242. doi:10.1016/j.psychres.2016.07.052
24. Fox KR, Wang SB, Boccagno C, Haynos AF, Kleiman E, Hooley JM. Comparing self-harming intentions underlying eating disordered behaviors and NSSI: Evidence that distinctions are less clear than assumed. Int J Eat Disord. 2019;52(5):564–575. doi:10.1002/eat.23041
25. Klonsky ED. The functions of deliberate self-injury: A review of the evidence. Clin Psychol Rev. 2007;27(2):226–239. doi:10.1016/j.cpr.2006.08.002
26. Shearer SL. Phenomenology of self-injury among inpatient women with borderline personality disorder. J Nerv Ment Dis. 1994;182:524–526.
27. Nixon MK, Cloutier PF, Aggarwal S. Affect regulation and addictive aspects of repetitive self-injury in hospitalized adolescents. J Am Acad Child Adoolesc Psychiatry. 2002;41(11):1333–1341. doi:10.1097/00004583-200211000-00015
28. Laye-Gindhu A, Schonert-Reichl KA. Nonsuicidal self-harm among community adolescents: Understanding the “whats” and “whys” of self-harm. J Youth Adolesc. 2005;34(5):447–457. doi:10.1007/s10964-005-7262-z
29. Taylor PJ, Jomar K, Dhingra K, Forrester R, Shahmalak U, Dickson JM. A meta-analysis of the prevalence of different functions of non-suicidal self-injury. J Affect Disord. 2018;227:759–769. doi:10.1016/j.jad.2017.11.073
30. Gollust SE, Eisenberg D, Golberstein E. Prevalence and correlates of self-injury among university students. J Am Coll Health. 2008;56(5):491–498. doi:10.3200/JACH.56.5.491-498
31. Cucchi A, Ryan D, Konstantakopoulos G, et al. Lifetime prevalence of non-suicidal self-injury in patients with eating disorders: A systematic review and meta-analysis. Psychol Med. 2016;46(7):1345–1358. doi:10.1017/S0033291716000027
32. St. Germain SA, Hooley JM. Direct and indirect forms of non-suicidal self-injury: Evidence for a distinction. Psychiatry Res. 2012;197(1–2):78–84. doi:10.1016/j.psychres.2011.12.050
33. St. Germain SA, Hooley JM. Aberrant pain perception in direct and indirect non-suicidal self-injury: An empirical test of Joiner’s interpersonal theory. Compr Psychiatry. 2013;54(6):694–701. doi:10.1016/j.comppsych.2012.12.029
34. Brausch AM, Perkins NM. Nonsuicidal self-injury and disordered eating: Differences in acquired capability and suicide attempt severity. Psychiatry Res. 2018;266:72–78. doi:10.1016/j.psychres.2018.05.021
35. Lloyd-Richardson EE, Perrine N, Dierker L, Kelley ML. Characteristics and functions of non-suicidal self-injury in a community sample of adolescents. Psychol Med. 2007;37(8):1183–1192. doi:10.1017/S003329170700027X
36. Tang J, Ma Y, Guo Y, Ahmed NI, Yu Y, Wang J. Association of aggression and non-suicidal self injury: A school-based sample of adolescents. PLoS One. 2013;8:10. doi:10.1371/journal.pone.0078149
37. Tang J, Yu Y, Wu Y, et al. Association between non-suicidal self-injuries and suicide attempts in Chinese adolescents and college students: A cross-section study. PLoS One. 2011;6(4).
38. Klonsky ED, Olino TM. Identifying clinically distinct subgroups of self-injurers among young adults: A latent class analysis. J Consult Clin Psychol. 2008;76(1):22–27. doi:10.1037/0022-006X.76.1.22
39. Whitlock J, Muehlenkamp J, Eckenrode J. Variation in nonsuicidal self-injury: Identification and features of latent classes in a college population of emerging adults. J Clin Child Adolesc Psychol. 2008;37(4):725–735.
40. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
41. Glenn CR, Klonsky ED. Nonsuicidal self-injury disorder: An empirical investigation in adolescent psychiatric patients. J Clin Child Adolesc Psychol. 2013;42(4):496–507. doi:10.1080/15374416.2013.794699
42. Nock MK, Joiner TE
43. Selby EA, Bender TW, Gordon KH, Nock MK, Joiner TE
44. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
45. Muehlenkamp JJ. Self-injurious behavior as a separate clinical syndrome. Am J Orthopsychiatry. 2005;75(2):324–333. doi:10.1037/0002-9432.75.2.324
46. Andover MS. Non-suicidal self-injury disorder in a community sample of adults. Psychiatry Res. 2014;219(2):305–310. doi:10.1016/j.psychres.2014.06.001
47. Washburn JJ, Potthoff LM, Juzwin KR, Styer DM. Assessing DSM–5 nonsuicidal self-injury disorder in a clinical sample. Psychol Assess. 2015;27(1):31–41. doi:10.1037/pas0000021
48. Muehlenkamp JJ, Brausch AM, Washburn JJ. How much is enough? Examining frequency criteria for NSSI disorder in adolescent inpatients. J Consult Clin Psychol. 2017;85(6):611–619. doi:10.1037/ccp0000209
49. Gratz KL, Dixon-Gordon KL, Chapman AL, Tull MT. Diagnosis and characterization of DSM-5 nonsuicidal self-injury disorder using the clinician administered nonsuicidal self-injury disorder index. Assess. 2015;22(5):527–539. doi:10.1177/1073191114565878
50. Zetterqvist M, Lundh LG, Ö D, Svedin CG. Prevalence and function of non-suicidal self-injury (NSSI) in a community sample of adolescents, using suggested DSM-5 criteria for a potential NSSI disorder. J Abnorm Child Psychol. 2013;41(5):759–773. doi:10.1007/s10802-013-9712-5
51. Brausch AM, Muehlenkamp JJ, Washburn JJ. Nonsuicidal self-injury disorder: Does criterion B add diagnostic utility? Psychiatry Res. 2016;244:179–184. doi:10.1016/j.psychres.2016.07.025
52. Forbes CN, Tull MT, Richmond JR, Chapman AL, Dixon-Gordon KL, Gratz KL. Motives for nonsuicidal self-injury in individuals with lifetime depressive disorders and posttraumatic stress disorder. J Psychopathol Behav Assess. 2019;1–10.
53. In-Albon T, Ruf C, Schmid M. Proposed diagnostic criteria for the DSM-5 of nonsuicidal self-injury in female adolescents: Diagnostic and clinical correlates. Psychiatry J. 2013;2013:1–12. doi:10.1155/2013/159208
54. Victor SE, Davis T, Klonsky ED. Descriptive characteristics and initial psychometric properties of the non-suicidal self-injury disorder scale. Arch Suicide Res. 2017;21(2):265–278. doi:10.1080/13811118.2016.1193078
55. Hooley JM, Franklin JC. Why do people hurt themselves? A new conceptual model of nonsuicidal self-injury. Clin Psychol Sci. 2018;6(3):428–451. doi:10.1177/2167702617745641
56. Brausch A. Diagnostic classification of nonsuicidal self-injury. In: Washburn JJ, editor. Nonsuicidal Self-Injury: Advances in Research and Practice. New York: Routledge; 2019:71–87.
57. Lengel GJ, Mullins-Sweatt SN. Nonsuicidal self-injury disorder: Clinician and expert ratings. Psychiatry Res. 2013;210(3):940–944. doi:10.1016/j.psychres.2013.08.047
58. Burke TA, Ammerman BA, Hamilton JL, Alloy LB. Impact of non-suicidal self-injury scale: Initial psychometric validation. Cognit Ther Res. 2017;41(1):130–142. doi:10.1007/s10608-016-9806-9
59. Nock MK, Holmberg EB, Photos VI, Michel BD. Self-injurious Thoughts and Behaviors Interview: Development, reliability, and validity in an adolescent sample. Psychol Assess. 2007;19(3):309–317. doi:10.1037/1040-3590.19.3.309
60. Klonsky ED, Glenn CR. Assessing the functions of non-suicidal self-injury: Psychometric properties of the Inventory of Statements About Self-injury (ISAS). J Psychopathol Behav Assess. 2009;31(3):215–219. doi:10.1007/s10862-008-9107-z
61. Gratz KL. Measurement of deliberate self-harm: Preliminary data on the deliberate self-harm inventory. J Psychopathol Behav Assess. 2001;23(4):253–263. doi:10.1023/A:1012779403943
62. Victor SE, Klonsky ED. Correlates of suicide attempts among self-injurers: A meta-analysis. Clin Psychol Rev. 2014;34(4):282–297. doi:10.1016/j.cpr.2014.03.005
63. Martin J, Cloutier PF, Levesque C, Bureau JF, Lafontaine MF, Nixon MK. Psychometric properties of the functions and addictive features scales of the Ottawa Self-Injury Inventory: A preliminary investigation using a university sample. Psychol Assess. 2013;25(3):1013–1018. doi:10.1037/a0032575
64. Nixon MK, Levesque C, Preyde M, Vanderkooy J, Cloutier PF. The Ottawa Self-Injury Inventory: Evaluation of an assessment measure of nonsuicidal self-injury in an inpatient sample of adolescents. Child Adolesc Psychiatry Ment Health. 2015;9(1):26–32. doi:10.1186/s13034-015-0056-5
65. Whitlock J, Exner-Cortens D, Purington A. Assessment of nonsuicidal self-injury: Development and initial validation of the Non-Suicidal Self-Injury–Assessment Tool (NSSI-AT). Psychol Assess. 2014;26(3):935. doi:10.1037/a0036611
66. Kaufman J, Birmaher B, Brent D, et al. Schedule for affective disorders and schizophrenia for school-age children present and lifetime version (K-SADS-PL): Initial reliability and validity data. J Am Acad Child Adolesc Psychiatry. 1997;36(7):980–988. doi:10.1097/00004583-199707000-00021
67. Swannell SV, Martin GE, Page A, Hasking P, St John NJ. Prevalence of nonsuicidal self‐injury in nonclinical samples: Systematic review, meta‐analysis and meta-regression. Suicide Life Threat Behav. 2014;44(3):273–303. doi:10.1111/sltb.12070
68. Washburn JJ W, Ed., Nonsuicidal Self-Injury: Advances in Research and Practice. New York: Routledge; 2019:71–87.
69. Franklin JC, Fox KR, Franklin CR, et al. A brief mobile app reduces nonsuicidal and suicidal self-injury: Evidence from three randomized controlled trials. J Consult Clin Psychol. 2016;84(6):544. doi:10.1037/ccp0000093
70. Hooley JM, Fox KR, Wang SB, Kwashie AN. Novel online daily diary interventions for nonsuicidal self-injury: A randomized controlled trial. BMC Psychiatry. 2018;18(1):264. doi:10.1186/s12888-018-1840-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.