")
Back to Journals » Journal of Pain Research » Volume 14
Nonmedical Use of Xtampza® ER and Other Oxycodone Medications in Adults Evaluated for Substance Abuse Treatment: Real-World Data from the Addiction Severity Index-Multimedia Version (ASI-MV®)
Authors Green JL, Robbins RS, Dailey-Govoni T, Butler SF
Received 12 February 2021
Accepted for publication 28 May 2021
Published 15 June 2021 Volume 2021:14 Pages 1773—1783
DOI https://doi.org/10.2147/JPR.S304805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Jody L Green, Rebekkah S Robbins, Taryn Dailey-Govoni, Stephen F Butler
Inflexxion, A Division of Integrated Behavioral Health, Irvine, CA, USA
Correspondence: Jody L Green
Inflexxion, A Division of Integrated Behavioral Health, 2 Park Plaza, Suite 1200, Irvine, CA, 82614, USA
Tel +1 303 618 9044
Email [email protected]
Purpose: The purpose of this study was to evaluate real-world data related to past 30-day nonmedical use (NMU) and routes of administration of Xtampza® ER and comparator oxycodone medications in the US as captured within the Addiction Severity Index-Multimedia Version® (ASI-MV®).
Methods: Data were collected from July 2016 through December 2019 from 647 centers located in 44 states using the ASI-MV, a clinical instrument used to evaluate substance use and treatment planning. Demographic characteristics were assessed using Pearson’s chi-square test for categorical data and quarterly NMU rates were calculated. Distribution of route of administration was studied using a proportional reporting ratio (PRR) analysis.
Results: Of 192,810 assessments, 42,279 (21.9%) indicated past 30-day NMU of at least one prescription opioid, including Xtampza ER (N=73, 0.2%), other oxycodone ER (n=3802, 9.0%) and oxycodone IR (n=14,579, 34.5%). All quarterly Xtampza ER NMU rates per 100 ASI-MV assessments were significantly lower than those for other oxycodone ER and oxycodone IR. Overall, quarterly Xtampza ER NMU drug utilization adjusted rates were significantly lower than quarterly rates observed for other oxycodone ER NMU but not consistently significantly lower than oxycodone IR NMU. Although not all statistically significant, all ratios from the PRR analysis were less than 1.0, indicating that rates of use of any alternate route, any non-oral route, snorting, and injecting were higher for other oxycodone ER and oxycodone IR than for Xtampza ER.
Conclusion: Xtampza ER had significantly lower rates of NMU than other oxycodone ER products and oxycodone IR products, as well as significantly lower rates of non-oral NMU than oxycodone IR products, in a population of individuals seeking substance abuse treatment. Understanding risks associated with different opioid medications is important for prescribers as they manage risks of opioid misuse and abuse with effective pain therapy.
Keywords: pain management, analgesic, opioid, drug abuse, substance abuse treatment, real-world data
Introduction
Opioid therapy for chronic pain remains a challenge as providers weigh the medical need for therapy with the risks of opioid-related misuse, abuse, diversion, and overdose. A systematic review and meta-analysis evaluated the efficacy of opioid therapy in chronic pain. Based upon 15 studies that met the inclusion criteria, opioids appear to be efficacious for treatment of non-cancer chronic pain for up to 3 months.1 Published studies evaluating the risks of prescription opioid therapy suggest that rates of opioid misuse range from 21% to 29% and rates of opioid addiction range from 8% to 12%.2 Prescription opioid medications with abuse-deterrent properties (also known as abuse-deterrent formulations (ADF)) are opioid medications designated by the US Food and Drug Administration (FDA) as products that may meaningfully deter abuse, even if they do not fully prevent abuse.3 Currently marketed ADF opioid products are intended to deter manipulation for the purpose of snorting, smoking or injecting of the active ingredient. Almost all ADF opioid products are extended-release (ER) formulations. Compared with immediate-release (IR) formulations, ER products contain higher amounts of the active ingredient. When an ER mechanism can be defeated so that most or all of the active ingredients become immediately available (for example, by crushing, grinding or dissolving), the product becomes particularly attractive for abuse by nonoral routes (eg, snorting, smoking or injecting). Prescription opioid abuse via nonoral routes of administration has been associated with a significantly higher risk (2.5 times higher) of life-threatening effects or death than abuse via oral routes as demonstrated by a study of cases managed by poison centers.4
Xtampza® ER (Collegium Pharmaceutical, Inc, Stoughton, MA, USA) is a Schedule II, abuse-deterrent, ER oral formulation of oxycodone indicated for the management of pain severe enough to require daily, around-the-clock long-term management for which alternative treatment options are inadequate.5 Xtampza ER is available in capsule form and is intended to be ingested orally. Xtampza ER was approved by the FDA in April 2016, with ADF labeling, specifically that the formulation was expected to make abuse via injection difficult, and to reduce abuse by the oral and intranasal routes.6 Xtampza ER became available to patients in Q3 2016.
Premarket in vitro and in vivo testing of Xtampza ER is well documented and demonstrates the difficulties in manipulating the product as well as the product’s pharmacokinetic profile and human abuse potential.7–14 Published postmarket data is limited to a recent publication comparing Xtampza ER to IR oxycodone, other ADF ER opioids, and non-ADF ER opioids which suggested that Xtampza ER has low relative abuse rates and low relative likelihood of non-oral use.15 While these results were consistent across several data sources, additional real-world data are needed to further understand the relative risk of abuse of currently available opioid medications.
The goal of this study was to evaluate real-world data from the Addiction Severity Index-Multimedia Version® (ASI-MV®; Inflexxion, Irvine, CA, USA), a clinical tool used to evaluate substance abuse and treatment planning. Past 30-day nonmedical use (NMU) and route of administration of Xtampza ER were compared to other oxycodone products currently available in the United States (US).
Methods
A cross-sectional surveillance study design was used to examine past 30-day NMU and routes of administration for Xtampza ER and comparator prescription oxycodone products among adults aged 18 years or older evaluated for substance abuse problems and treatment planning using the ASI-MV assessment tool. The comparator prescription oxycodone product groups included: 1) other oxycodone ER and 2) oxycodone IR (Table 1). The comparator groups are not mutually exclusive as one assessment could have included reported NMU of multiple products; hence, one assessment could be included in more than one study group.
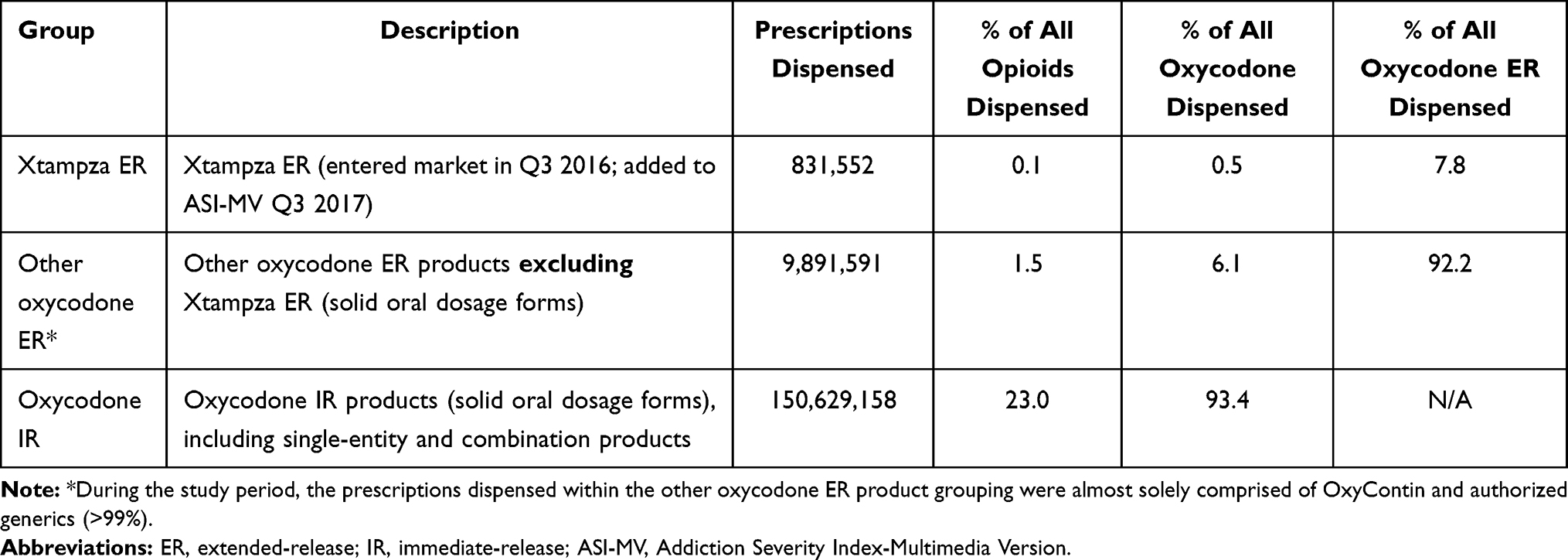 |
Table 1 Utilization of Xtampza ER and Comparator Oxycodone Groups Within the ASI-MV Network |
ASI-MV Data Collection
This study included ASI-MV assessments completed from 01 July 2016 (Q3 2016) through 31 December 2019 (Q4 2019), representing a 3.5-year time period. Xtampza ER was launched in Q3 2016 and added to the ASI-MV in Q3 2017, allowing for a 1-year transition period as the product was introduced to the US market. The ASI-MV is a clinical tool used in standard workflow to gather biopsychosocial data of individuals evaluated for substance use for the purpose of triage and treatment planning.16,17 This validated self-administered standardized tool is based on the Addiction Severity Index (ASI), a standard clinical assessment tool with well-established reliability and validity designed for use on admission to drug and alcohol treatment.18–20
In addition to patient characteristics, substance use and treatment history, and biopsychosocial domain assessments, the ASI-MV gathers self-reported NMU of specific prescription opioid medications. Respondents who report prescription opioid NMU are asked to identify the specific prescription opioid products used in the past 30 days from a list of brand and generic products. Product photos are presented to assist with product identification. Routes of administration ever used for each product are also collected.
Secondary analysis of ASI-MV data for research purposes has been determined to be exempt from institutional review board review by the New England Institutional Review Board. All data accessed complied with relevant data protection and privacy regulations.
Definition of NMU
NMU was defined with the use of an algorithm of responses to several questions (Figure 1). Using this algorithm, any deviation from legitimate medical use as prescribed was considered NMU. For purposes of this study, legitimate medical use is use of one’s own prescription medication from a healthcare provider only in the manner in which it was prescribed (frequency, dose and route of administration). While the ASI-MV captures NMU, abuse (a subtype of NMU) was not specifically collected. The FDA defines abuse as “the nonmedical use of a drug, repeatedly, or even sporadically, for the positive psychoactive effects it produces”. The ASI-MV does not query the intention or reason for reported NMU of opioid medications; hence, rates of any NMU were reported rather than “abuse” or “misuse”.
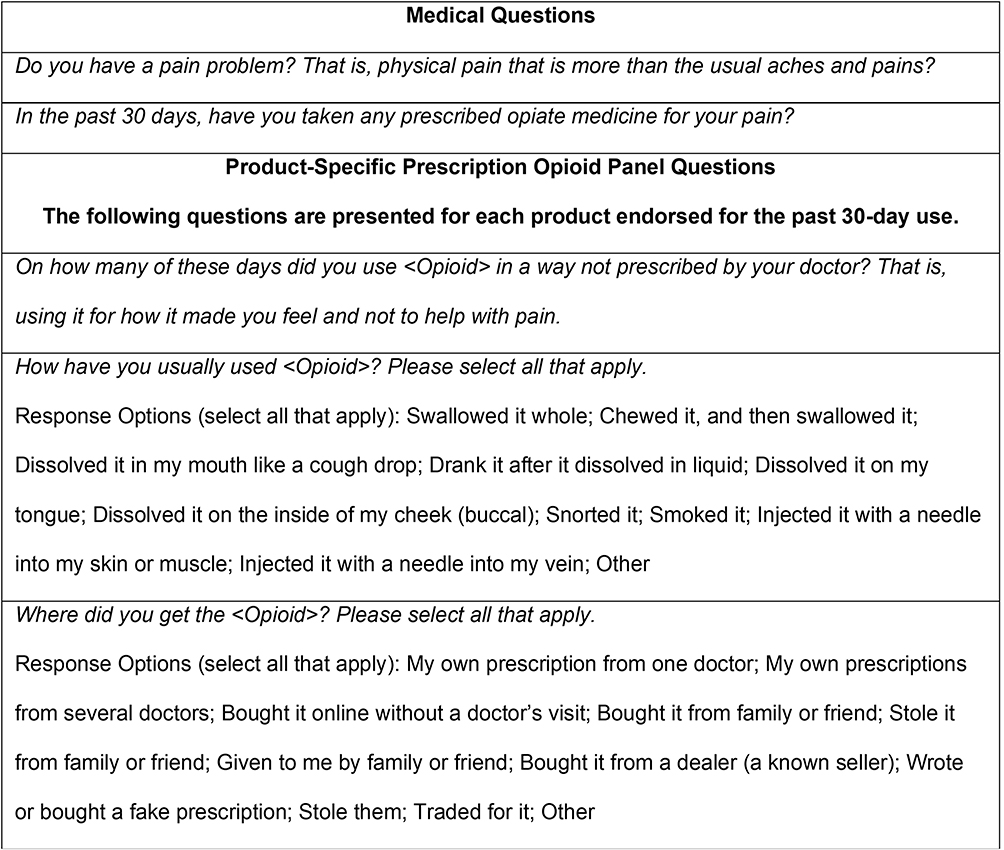 |
Figure 1 Items used in algorithm to define past 30-day nonmedical use (NMU) of prescription opioid products. Note: Italics represent verbatim question as presented in the ASI-MV. |
Data Analyses
Demographic characteristics were assessed using Pearson’s chi-square test (or Fisher's exact test for comparisons with small cell size) for categorical data and Wilcoxon rank sum tests for ordinal data. Statistical significance was determined for tests where p<0.05. Quarterly NMU was assessed during the study period using the following approaches: 1) rate (95% confidence interval) adjusted for volume of ASI-MV assessments completed during the study period, 2) rate (95% confidence interval) adjusted by the number of prescriptions dispensed, and 3) rate adjusted by the number of solid oral dosage units (eg, tablets, capsules, caplets) dispensed. Prescriptions and units dispensed data were obtained from the National Prescription Audit™ (NPA; IQVIA, Danbury, CT, USA), an industry standard source of national prescription activity for all pharmaceutical products. NPA includes prescriptions and units dispensed from the universe of retail, standard mail service, specialty mail service, and long-term care pharmacies. The database produces projected total prescriptions dispensed (counts) and projected total number of units dispensed (counts) at various levels of aggregation including state and 3-digit ZIP code for all opioid products by individual manufacturer and available dosage strengths. For the purposes of this analysis, only solid oral dosage formulations were included (tablets or capsules) and only states with sites that contributed at least one assessment to the ASI-MV dataset during a specific quarter during the study period were included in the prescription-adjusted analyses for that quarter. The prescriptions dispensed- and units dispensed-adjusted rates account for the variability in drug utilization of Xtampza ER and the comparator groups. 95% confidence intervals (CIs) for NMU rates were calculated using a binomial distribution or Poisson distribution (ie, in instances in which the number of cases is less than 30). Units dispensed was included as an adjuster for drug availability because each tablet represents an individual opportunity for abuse.21
The proportional reporting ratio (PRR) is a commonly used method to assess disproportionality in pharmacovigilance surveillance data and has been deemed a validated method in drug safety research and surveillance for signal detection.22,23 The PRR was calculated for specific routes of administration reported for Xtampza ER NMU versus routes of administration reported for comparator NMU. An individual assessment may include reported NMU of more than one oxycodone product by more than one route of administration. Each mention of a product and route was used to calculate the ratios. These ratios indicate if different routes of administration were more or less likely to be used for Xtampza ER NMU versus the comparators. Routes of administration included Any Oral (swallow whole, chew then swallow, dissolve like a cough drop, dissolved in liquid then drank) and Any Non-Oral (snort, smoke, inject). Multiple routes could be reported for each product; hence, routes are not mutually exclusive. All analyses were carried out using SAS Enterprise Guide version 7.1 (Cary, NC).
Results
During the study period, 647 sites located in 44 states contributed 192,810 assessments to the ASI-MV network. A total of 42,279 assessments (21.9%) reported past 30-day NMU of at least one prescription opioid. Less than 1% of those reporting prescription opioid NMU specified past 30-day Xtampza ER NMU (n=73; 0.2%). Past 30-day NMU of other oxycodone ER was reported by 9.0% (n=3802) and over one-third reported past 30-day oxycodone IR NMU (n=14,579, 34.5%) (Table 2). Those who reported Xtampza ER NMU were more likely to be female (54.8% versus 48.6% of those reporting other oxycodone ER product NMU and 49.4% of those reporting oxycodone IR NMU). Approximately 25% of those who reported Xtampza ER NMU were aged 45 years or older compared to 16.0% of those reporting NMU of other oxycodone ER products and 15.2% of those reporting NMU of oxycodone IR products. Those reporting Xtampza ER NMU were more likely than those endorsing comparator opioid drug NMU to self-report a current pain problem (71.2% versus 60.2% of other oxycodone ER product nonmedical users and 55.7% of oxycodone IR nonmedical users). Patients with moderate to extreme drug severity scores were similar across the study groups.
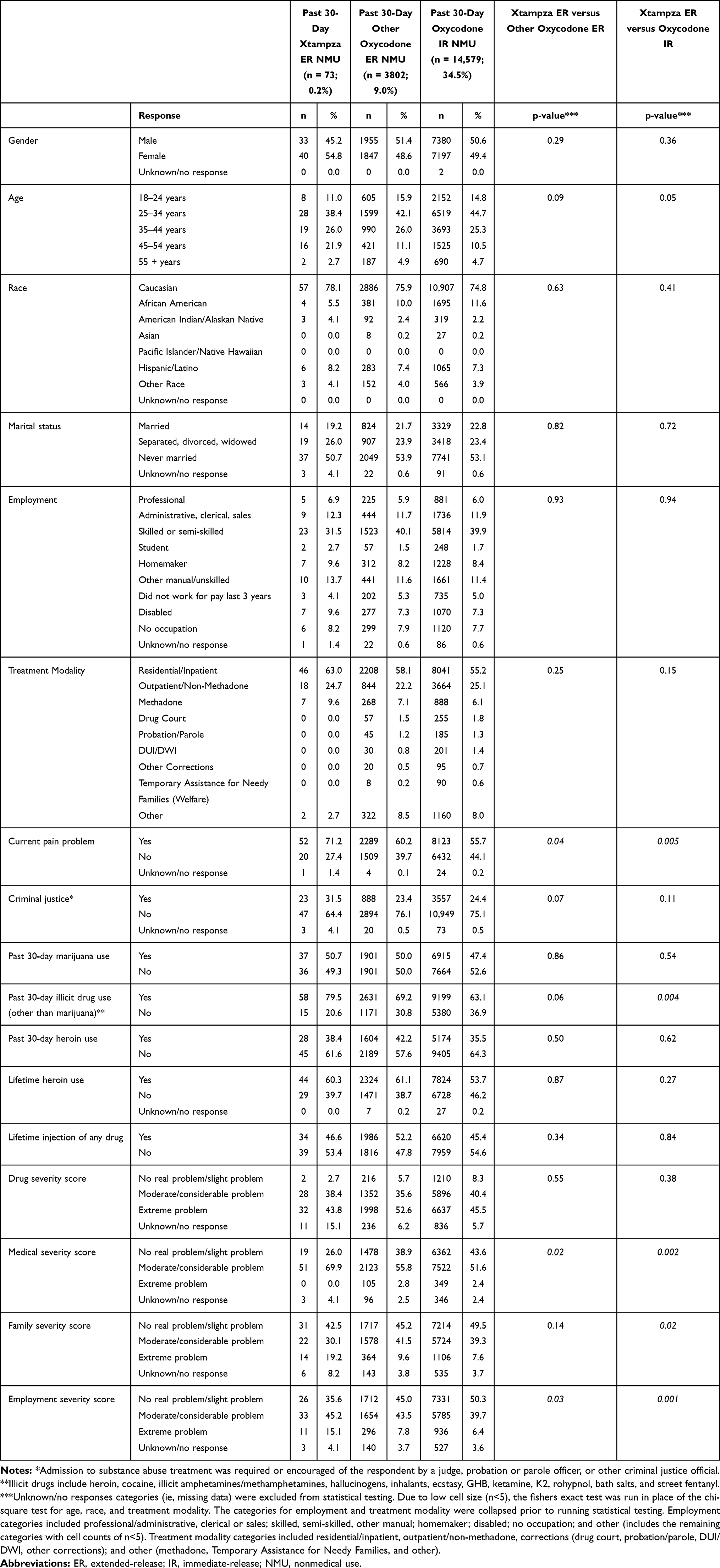 |
Table 2 Patient Demographics and Characteristics |
Quarterly past 30-day NMU rates of Xtampza ER per 100 ASI-MV assessments ranged from 0.01 (Q3 2017) to 0.10 (Q1 2018), other oxycodone ER NMU rates ranged from 1.25 (Q4 2019) to 2.97 (Q4 2016), and oxycodone IR NMU rates ranged from 10.87 (Q4 2019) to 23.37 (Q3 2016) (Figure 2A). All quarterly Xtampza ER NMU rates per 100 ASI-MV assessments were significantly lower than those for other oxycodone ER and oxycodone IR, as determined by discrete confidence intervals. Past 30-day oxycodone IR NMU quarterly rates per 100 ASI-MV assessments were significantly higher than all other groups.
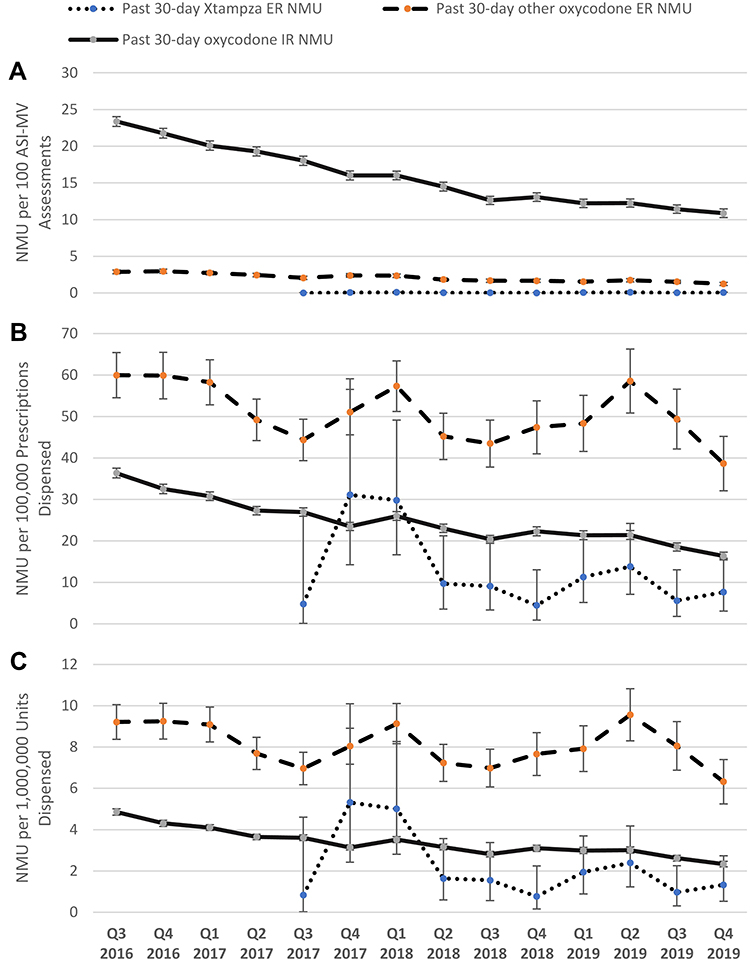 |
Figure 2 Quarterly (Q3 2016-Q4 2019) rates of past 30-day NMU (A) per 100 ASI-MV assessments, (B) per 100,000 prescriptions dispensed, and (C) per 1,000,000 units dispensed for Xtampza ER and comparator oxycodone products. Abbreviations: ER, extended-release; IR, immediate-release; ASI-MV, Addiction Severity Index-Multimedia Version; NMU, nonmedical use. Note: Xtampza ER was added to the ASI-MV in Q3 2017. |
When adjusting for the volume of prescriptions dispensed during the study period, past 30-day Xtampza ER NMU was reported at rates between 4.46 (Q4 2018) and 31.10 (Q4 2017), other oxycodone ER NMU rates ranged from 38.65 (Q4 2019) to 59.94 (Q3 2016), oxycodone IR NMU rates ranged from 16.35 (Q4 2019) to 36.37 (Q3 2016) mentions per 100,000 prescriptions (Figure 2B). Overall, quarterly Xtampza ER NMU rates per 100,000 prescriptions dispensed were significantly lower than quarterly rates observed for other oxycodone ER NMU (with the exception of Q4 2017), but not consistently significantly lower than oxycodone IR NMU rates.
The units dispensed adjusted rate of past 30-day Xtampza ER NMU was lowest in Q4 2018 (0.77) and highest in Q4 2017 (5.32). Other oxycodone ER past 30-day NMU adjusted for units dispensed ranged from 6.32 (Q4 2019) to 9.56 (Q2 2019). Oxycodone IR past 30-day NMU adjusted for units dispensed ranged from 2.33 (Q4 2019) to 4.86 (Q3 2016) (Figure 2C). Overall, Xtampza ER NMU rates per 1,000,000 units dispensed were significantly lower than quarterly rates observed for other oxycodone ER NMU but not significantly lower than oxycodone IR NMU rates.
Nonmedical users of Xtampza ER were significantly less likely to report any non-oral route of administration (28.8%) compared to nonmedical users of other oxycodone ER products (57.9%; Chi-square 18.57, p<0.001) and nonmedical users of oxycodone IR products (60.1%; Chi-square 52.47, p<0.001) (Table 3). Specifically, snorting and injecting were reported less frequently for Xtampza ER NMU (17.8% and 6.8%, respectively) compared to other oxycodone ER NMU (31.9% reported snorting and 21.9% reported injecting) and oxycodone IR NMU (40.6% reported snorting and 15.5% reported injecting).
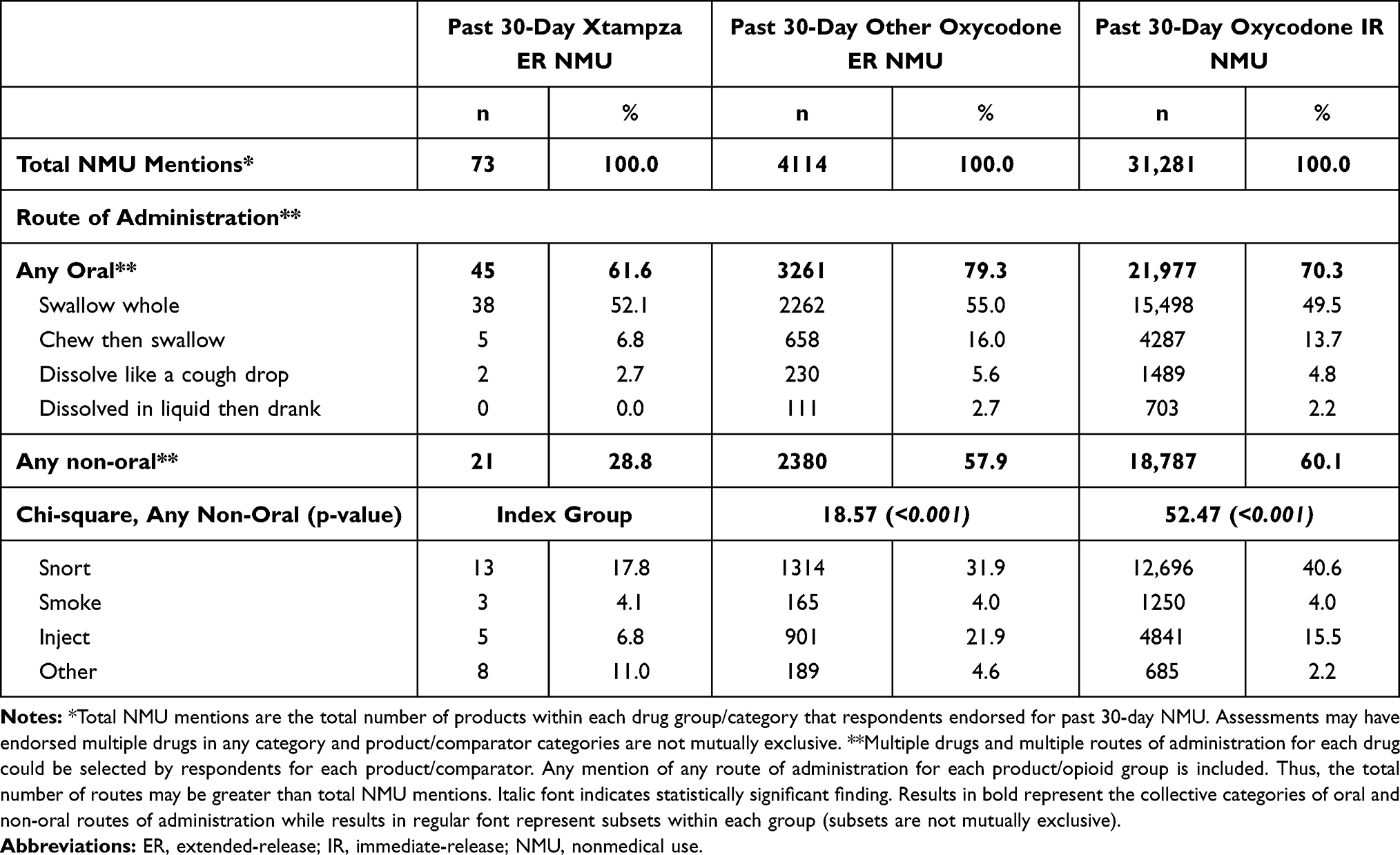 |
Table 3 Prevalence of Nonmedical Use (NMU) for Xtampza ER and Comparators by Route of Administration (7/1/2016–12/31/2019) |
The significant disproportionality in routes of administration between the study groups is further illustrated in the PRR analysis using Xtampza ER as the reference group (Figure 3). All ratios were less than 1.0 which indicates the ratio of the comparator group was higher than that of Xtampza ER. The PRR for other oxycodone ER was statistically significant for the evaluation of any non-oral route versus swallowing whole and for the evaluation of injection versus swallowing whole. The PRR for oxycodone IR was statistically significant for all comparisons except for injection versus swallowing whole. These data suggest that Xtampza ER is less likely to be used via a non-oral route (including injection) than swallowing, compared to other oxycodone ER medications and less likely to be used via any alternate route, any non-oral route, or snorting compared to oxycodone IR.
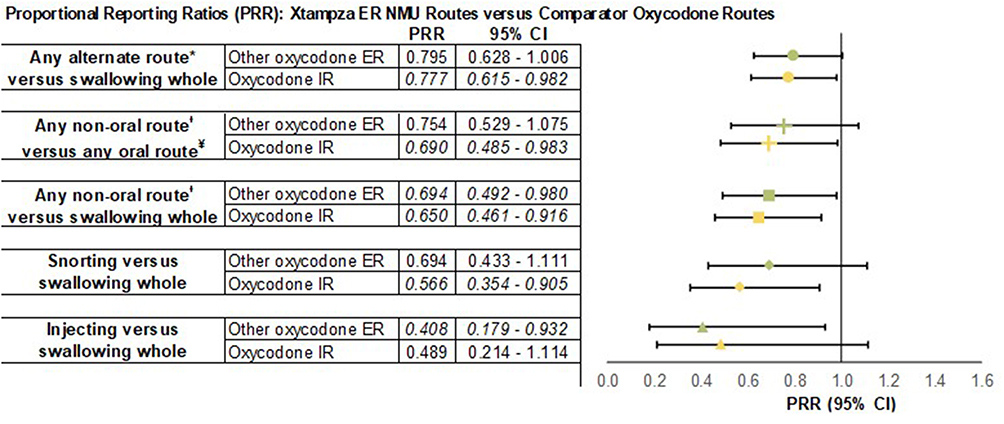 |
Figure 3 Proportional reporting ratios (PRR) of Xtampza ER NMU routes of administration versus routes of administration reported for NMU of comparator oxycodone groups (7/1/2016 – 12/31/2019). PRR <1.0 indicates the ratio of the comparator group was higher than that of Xtampza ER. Abbreviations: PRR, proportional reporting ratio; CI, confidence interval; ER, extended-release; IR, immediate-release; NMU, nonmedical use. Notes: *Alternate routes include chewed then swallowed, dissolved in mouth like a cough drop, dissolved in liquid and drank, snorted, smoked, injected and “Other” ROA. ᵻNon-oral routes include snorting, smoking, and injecting. ¥Oral routes include swallowing whole, chewing then swallowing, dissolving in mouth like a cough drop, and dissolving in liquid then drinking. Italicized PRR values indicate statistical significance (confidence intervals did not include 1.0). |
Discussion
This study analyzed 192,810 assessments from the ASI-MV network for Xtampza ER and oxycodone opioid comparator groups from 01 July 2016 through 31 December 2019. The ASI-MV is a standardized, validated clinical tool used for substance abuse evaluation and treatment planning which also allows for the study of opioid NMU within a high-risk population.
While all quarterly rates of past 30-day NMU adjusted for the volume of ASI-MV assessments and almost all drug utilization adjusted rates were lowest for Xtampza ER, many did not reach statistical significance likely due to the small number of Xtampza ER NMU cases reported (n=73) and low volume of prescriptions and units dispensed, particularly during introduction of the product to the market.
Additionally, all ratios from the PRR analysis were less than 1.0, indicating that rates of use of any alternate route, any non-oral route, snorting, and injecting were higher for other oxycodone ER and oxycodone IR than for Xtampza ER. The PRR between Xtampza ER and other oxycodone ER suggests a lower likelihood of Xtampza ER being used via any alternate route by 20%, any non-oral route by 25%, snorting by 31%, and injecting by 59%. However, the confidence intervals were large, and the PRR was statistically significant for any non-oral route versus swallowing whole and injection versus swallowing whole.
In this study, the other oxycodone ER group consisted almost entirely (>99%) of products that have ADF properties albeit with a different technology than Xtampza ER. Hence, some level of comparability of rates of alternate route of administration between the other oxycodone ER group and Xtampza ER relative to the oxycodone IR group would be expected but cannot be confirmed in this study, especially for injection. Further evaluation is needed regarding the deterrent effects between the different ADF formulations of oxycodone ER products and if differences found in premarket laboratory testing are detectable in postmarket real-world data.
Similar to the PRR analysis between Xtampza ER and other oxycodone ER, the PRR analysis between Xtampza ER and oxycodone IR illustrated a lower likelihood of Xtampza ER being used via any alternate route by 22%, any non-oral route by 31%, snorting by 43%, and injecting by 51%. These ratios were statistically significant for all except injection, despite it having the most remarkable ratio (PRR 0.489, CI 0.2142, 1.1141). In this study, oxycodone IR products accounted for 93.4% of all opioid prescriptions dispensed and had the highest proportion of non-oral routes (60.1%), including snorting (40.6%). This product group by far is the most widely available opioid medication and is the first-line therapy for treatment of acute pain. This is also a group of products that are easily manipulated for non-oral routes of administration which is an important consideration for any prescriber.
Opioid prescribing behaviors vary and cannot be ignored as a confounder when evaluating rates of opioid NMU and routes of administration. A recent study described the variability in prescribing ADF products using data from 2018. The rate of ADF prescribing per 1000 adult recipients of opioid analgesics was nearly twice as high in Florida (rate 14.57; 95% CI: 14.44, 14.69) than in California (rate 8.30; 95% CI: 8.22, 8.37) and Kentucky (rate 8.20; 95% CI: 8.01, 8.39).24 Variations were detected between states in proportion of ADF prescriptions in rural versus urban populations. It was also noted that patients prescribed ADF opioids were more often age 55–74 years of age, yet overdose deaths nationwide are more likely to occur in individuals age 35–54 years. The specific drivers for prescribing ADF opioid medications are unclear, though likely influenced by geographic region, institutional or state policy, formularies, payor requirements, and pricing. To date, patient-centric factors such as sociodemographics or the patient’s individual risk evaluation of potential or ongoing NMU have not been identified as significant influencers on prescribing behavior. Attention is warranted in this area to effectively utilize ADF opioid medications as a tool in deterring non-oral opioid use. While no product can be abuse-proof, incremental improvements are beneficial and should not be discounted.
While this study does not allow for the determination of why these opioid medication groups have different NMU profiles, some potential drivers are discussed. In summary, these potential drivers include the actual formulation, as Xtampza ER is the only oxycodone formulation to include ADF labeling specific to reduction of abuse by the oral route of administration; availability and ease of manipulation of oxycodone IR products; and administrative influences on prescribing behaviors rather than patient-centric or risk-based prescribing. While this list is not exhaustive and prescription opioid NMU is complex and impacted by many other confounders, these should be considered by prescribers when determining the most appropriate opioid therapy.
The strengths of this study include (1) access to a hard-to-reach, enriched population of opioid users, (2) data collection via a validated clinical tool used in standard workflow that captures product-specific NMU (using pictures and product names) and route of administration, (3) large sample of assessments during the study period and (4) novel approach of evaluating routes of administration. Limitations of this study include (1) reliance on self-report of historical behaviors, (2) self-reported product identification with potential product misclassification, (3) small sample size of some study groups, and (4) the inability to assign causality to the differences found between medication groups. Additionally, the ASI-MV is not a nationally representative sample; the data are obtained from sites that use ASI-MV in clinical practice and may not be representative of all individuals evaluated for substance abuse treatment or users not seeking treatment.
Conclusion
The ability to provide effective pain management therapy while reducing the risk of opioid misuse and abuse continues to be a challenge for medical professionals. Oxycodone-containing products are some of the most commonly prescribed opioids. Xtampza ER had significantly lower rates of NMU than other oxycodone ER products and oxycodone IR products, as well as significantly lower rates of non-oral NMU than oxycodone IR products, in a population of individuals seeking substance abuse treatment. Understanding NMU profiles of different opioid medications is important for prescribers as they balance opioid NMU risks with effective pain therapy.
Acknowledgments
This study was funded by Collegium Pharmaceutical, Inc. Inflexxion contracts with FDA and multiple companies with interests in some of the products included in the compounds evaluated for this article. Although the sponsor was involved in reviewing the content of this article, all data collection, analysis, and ultimate data interpretation were made by the authors without sponsor influence. XTAMPZA® is a registered trademark of Collegium Pharmaceutical, Inc. The abstract of this paper was presented at PAINWeek Conference 2020 as a poster presentation with interim findings. The poster’s abstract was published in the online PAINWeek Abstract Book 2020: https://doi.org/10.1080/00325481.2020.1824967.
Disclosure
JLG, RSR, and TDG are employees of and SFB is a consultant to Inflexxion, a division of Integrated Behavioral Health. The authors report no other conflicts of interest in this work.
References
1. Meske DS, Lawal OD, Elder H, Langberg V, Paillard F, Katz N. Efficacy of opioids versus placebo in chronic pain: a systematic review and meta-analysis of enriched enrollment randomized withdrawal trials. J Pain Res. 2018;11:923–934. doi:10.2147/JPR.S160255
2. Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, van der Goes DN. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569–576. doi:10.1097/01.j.pain.0000460357.01998.f1
3. United States Food and Drug Administration CDER: abuse deterrent opioids—evaluation and labeling, guidance for industry; April 2015. Available from https://www.fda.gov/downloads/Drugs/Guidances/UCM334743.pdf.
4. Green JL, Bucher Bartelson B, Le Lait MC, et al. Medical outcomes associated with prescription opioid abuse via oral and non-oral routes of administration. Drug Alcohol Depend. 2017;175:140–145. doi:10.1016/j.drugalcdep.2017.01.039
5. FDA. Highlights of prescribing information: xtampza ER; 2016. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/208090s000lbl.pdf.
6. FDA. Xtampza ER (oxycodone) extended-release capsules; 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2016/208090Orig1s000TOC.cfm.
7. Brennan MJ, Kopecky EA, Marseilles A, O’Connor M, Fleming AB. The comparative pharmacokinetics of physical manipulation by crushing of Xtampza® ER compared with OxyContin®. Pain Manag. 2017;7(6):461–472. doi:10.2217/pmt-2017-0030
8. Fleming AB, Scungio TA, Grima MP, Mayock SP. In vitro assessment of the potential for abuse via the intravenous route of oxycodone DETERx® microspheres. J Opioid Manag. 2016;12(1):57–65. doi:10.5055/jom.2016.0312
9. Gudin J, Levy-Cooperman N, Kopecky EA, Fleming AB. Comparing the effect of tampering on the oral pharmacokinetic profiles of two extended-release oxycodone formulations with abuse-deterrent properties. Pain Med. 2015;16(11):2142–2151. doi:10.1111/pme.12834
10. Gudin J. Effect of physical manipulation on the oral pharmacokinetic profile of Xtampza® ER (oxycodone DETERx® formulation): a review of published studies. J Opioid Manag. 2020;16(2):127–139. doi:10.5055/jom.2020.0559
11. Kopecky EA, Fleming AB, Levy-Cooperman N, O’Connor M, M. sellers E. Oral human abuse potential of oxycodone DETERx ® (Xtampza ® ER). J Clin Pharmacol. 2017;57(4):500–512. doi:10.1002/jcph.833
12. Kopecky EA, Fleming AB, Noonan PK, et al. Impact of physical manipulation on in vitro and in vivo release profiles of oxycodone DETERx®: an extended-release, abuse-deterrent formulation. J Opioid Manag. 2014;10(4):233–246. doi:10.5055/jom.2014.0211
13. Mayock SP, Saim S, Fleming AB. In vitro drug release after crushing: evaluation of Xtampza® ER and other ER opioid formulations. Clin Drug Investig. 2017;37(12):1117–1124. doi:10.1007/s40261-017-0561-9
14. Meske D, Kopecky EA, Passik S, Shram MJ. Evaluation of the oral human abuse potential of oxycodone DETERx® formulation (Xtampza® ER). J Opioid Manag. 2018;14(5):359–372. doi:10.5055/jom.2018.0468
15. Severtson SG, Scott ED, Amioka EC, et al. Postmarketing analysis of misuse, abuse, and diversion of Xtampza ER. Pain Med. 2020;21(12):3660–3668. doi:10.1093/pm/pnaa272
16. Butler SF, Budman SH, Licari A, et al. National Addictions Vigilance Intervention and Prevention Program (NAVIPPRO): a real-time, product-specific, public health surveillance system for monitoring prescription drug abuse. Pharmacoepidemiol Drug Saf. 2008;17(12):1142–1154. doi:10.1002/pds.1659
17. Butler SF, Budman SH, Goldman RJ, et al. Initial validation of a computer-administered addiction severity index: the ASI–MV. Psychol Addict Behav. 2001;15:4–12. doi:10.1037/0893-164X.15.1.4
18. Hendriks VM, Kaplan CD, van Limbeek J, Geerlings P. The Addiction Severity Index: reliability and validity in a Dutch addict population. J Subst Abuse Treat. 1989;6(2):133–141. doi:10.1016/0740-5472(89)90041-X
19. Kosten TR, Rounsaville BJ, Kleber HD. Concurrent validity of the Addiction Severity Index. J Nerv Ment Dis. 1983;171(10):606–610. doi:10.1097/00005053-198310000-00003
20. McLellan AT, Kushner H, Metzger D, et al. The fifth edition of the addiction severity index. J Subst Abuse Treat. 1992;9(3):199–213. doi:10.1016/0740-5472(92)90062-S
21. Secora AM, Dormitzer CM, Staffa JA, Dal Pan GJ. Measures to quantify the abuse of prescription opioids: a review of data sources and metrics. Pharmacoepidemiol Drug Saf. 2014;23(12):1227–1237. doi:10.1002/pds.3711
22. Bohm R. Primer on Disproportionality Analysis. Available from: http://openvigil.sourceforge.net/doc/DPA.pdf.
23. Duggirala HJ, Tonning JM, Smith E, et al. Use of data mining at the Food and Drug Administration. J Am Med Inform Assoc. 2016;23:428–434. doi:10.1093/jamia/ocv063
24. Brown JR, Oh G, Wang Y, et al. Variation in abuse-deterrent formulation opioid prescribing in California, Florida, and Kentucky in 2018. J Rural Health. 2020;37:23–28. doi:10.1111/jrh.12496
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.