")
Back to Journals » Patient Preference and Adherence » Volume 16
Nondisclosure of Medical Related Information by Persons with Type 1 and Type 2 Diabetes Mellitus to Their Healthcare Providers: Do Different Patterns Exist?
Authors Alrasheed AA, Wafa AN, Hamouda RH, Alharthi SA, AlMotairi HM, Alsadhan KF, AlSaif HI , Almigbal TH
Received 6 September 2022
Accepted for publication 22 October 2022
Published 28 October 2022 Volume 2022:16 Pages 2937—2945
DOI https://doi.org/10.2147/PPA.S387915
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qizhi (Cathy) Yao
Abdullah A Alrasheed,1,2 Amaal N Wafa,3 Reham H Hamouda,4 Sawsan A Alharthi,5 Hour M AlMotairi,3 Khalid F Alsadhan,1,2 Haytham I AlSaif,1,2 Turky H Almigbal1,2
1Department of Family and Community Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 3Department of Family Medicine, Vision College of Medicine, Vision Colleges, Riyadh, Saudi Arabia; 4Department of Family Medicine, College of Medicine, AlMaarefah University, Riyadh, Saudi Arabia; 5Department of Family Medicine, College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Correspondence: Abdullah A Alrasheed, Department of Family and Community Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia, Tel +966 55 644 0445, Email [email protected]
Purpose: The doctor–patient relationship is often challenged by complex communication issues and nondisclosure of important related medical information, especially in diabetes management. Very little information is known about diabetic patient nondisclosure to their doctors. The present study evaluated the prevalence of nondisclosure of information by persons with type 1 and type 2 diabetes mellitus to healthcare providers and its associated factors among the Saudi population, as well as the differences between persons with type 1 and type 2 diabetes mellitus.
Methods: A cross-sectional study targeting persons with type 1 and type 2 diabetes mellitus was conducted at King Saud University Medical City, Saudi Arabia, Riyadh. An online self-administered questionnaire was used to collect data.
Results: A total of 285 participants were included in the study (155 [54.4%] and 130 [45.6%] type 1 and 2 diabetic patients, respectively). Having an unhealthy diet (25.3%, n = 72), not regularly exercising (23.5%, n = 67), hiding some glucose readings (23.2%, n = 65), and not following instructions for weight loss (22.8%, n = 44) were the most common types of nondisclosed information among diabetic patients. The nondisclosure of information was significantly higher among type 2 patients (29.2%) than type 1 diabetic patients (18.7%) in terms of not participating in regular exercise (p = 0.018). Similarly, the nondisclosure of information was significantly higher among persons with type 1 diabetes compared to persons with type 2 diabetes in terms of hiding some glucose readings (p < 0.001) and not disclosing hyperglycemia (p = 0.011).
Conclusion: Nondisclosure of important related medical information among diabetic patients to their healthcare providers is prevalent among the Saudi population. Furthermore, the types and causes of nondisclosed information differ among persons with type 1 and type 2 diabetes mellitus.
Keywords: nondisclosure, diabetes mellitus, medical information, Saudi Arabia
Introduction
Patient disclosure of information to healthcare providers is a key element in the patient–doctor relationship as well as overall patient care and safety. Healthcare providers rely on patients to disclose accurate information about their symptoms and health-related habits and feelings so that an appropriate diagnosis, management plan, and recommendations can be made. Furthermore, without receiving accurate information from patients, physicians’ decisions may even have negative effects on their patients.
Despite the well-known benefits of disclosing accurate information to healthcare providers, there is a strong belief that patients might hold back essential clinical information. According to the Health Information National Trends Survey (HINTS), around 12.3% patients withhold clinical information from their clinicians.1 In addition, 81.1% of patients failed to disclose at least one piece of information that is relevant to their care to their clinicians. The most common reported reason for this behavior was that the patients do not want to be judged or lectured by their physicians.2
Diabetes mellitus (DM) is one of the major health problems. It has considerable consequences on public wellbeing and healthcare costs and is becoming one of the top 10 leading causes of death worldwide.3 Due to a lack of exercise and changes in dietary habits, the prevalence of DM is growing at an alarming rate. Globally, 462 million individuals have been diagnosed with type 2 diabetes (6.28%).4 In Saudi Arabia, the overall prevalence of DM was noted to be 23.7% according to Al-Nozha.5 From 1992 to 2010, the prevalence of DM has rapidly increased by 2.7 times over the past 20 years in Saudi Arabia.6
As the number of cases increases, DM-related complications also increase. The complications are divided into macro- and microvascular complications. Coronary artery disease, stroke, and diabetic foot are the most common macro-vascular complications, while neuropathy, retinopathy, and nephropathy are the most common microvascular ones.7 Type 2 diabetes is known to be the most common type of DM (90%–95% of DM cases).8
The management of DM depends mainly on the type of DM and patient-related factors. Generally, three approaches are used in DM management: (1) medications, (2) healthy diet, and (3) physical activity. Carbohydrate counting remains an effective method in lowering the glycemic index in persons with type 1 and type 2 diabetes mellitus along with medications, especially for DM patients who are on insulin. However, adopting a healthy diet based on recommendations issued by well-known and reliable medical bodies or based on the physician’s recommendations is highly effective in lowering the glycemic index. With appropriate education, patients can effectively monitor their carbohydrate intake. Glycosylated hemoglobin (HbA1C) levels, lipid profiles, blood pressure, and body weight can be significantly regulated with effective carbohydrate counting.9 However, it has been demonstrated that type 2 diabetic patients specifically have compliance issues with respect to medications, diabetic diets, and exercise.10
Patient disclosure of information was defined as releasing and transferring of health-related information from the patient or one of his family members to the assigned healthcare providers through one of the reliable communication channels.7 However, diabetic patient disclosure could be put in the context of patient disclosure throughout patient’s disclosing medical or health-related information to their DM status to the healthcare providers and these information might include their dietary behaviors, glucose monitoring measurements, social events affecting their self-care activities, and many other aspects of information related to their medical status.2
The clinical disclosure is viewed differently by the patients as significant stakeholders in the healthcare process. Therefore, it is significantly affected by their sociodemographic characteristics. For example, it was found that age, gender and living status are significant socio-demographic factors influencing the patients’ decision to disclose clinical information.2,11,12
Although disclosing medical information to healthcare providers remains a fundamental aspect in patient care, only a limited number of studies have explored this issue among patients with DM. Patients with chronic diseases, such as diabetes, might be prone to nondisclosure of relevant and essential information to their physicians. In particular, this issue could significantly affect overall healthcare delivery and safety of DM patients.
Thus, the aim of this study was to assess the prevalence of medical information nondisclosure to healthcare providers among patients with type 1 and 2 DM, as well as to identify the associated risk factors for nondisclosure.
Methods
Study Design and Setting
This cross-sectional study used an online self-administered questionnaire to examine persons with type 1 and type 2 diabetes mellitus who were being followed up in a tertiary hospital. The hospital provides tertiary diabetes care in a specialized diabetes center and primary care in a primary care clinic. The study was conducted at King Saud University Medical City, Saudi Arabia, Riyadh. Ethical approval was obtained through the institutional review board of King Saud University Medical City IRB (No E-21-5881). The present study was performed in compliance with the ethical principles for medical research in the Declaration of Helsinki.
A list of persons with type 1 and type 2 diabetes mellitus was obtained from the electronic health records, after which a systematic random sampling technique was applied to choose patients. Every third patient was included in the study. Each selected patient who was above 18 years old was contacted via phone, and details about objectives of the study were explained. If a patient refused to participate, the next selected patient was contacted. After obtaining verbal consent from the participants, a link for the online questionnaire was sent to them.
Telephone surveys were avoided to obtain more accurate information and data entry in addition to ensuring patient privacy and anonymity. The online-based survey was administered to patients using the GoogleForms® platform. This tool enables secure, anonymous data collection and ensures confidentiality. Informed consent to participate was obtained a second time in the survey before starting it. This was achieved through allowing the participants to either choose to agree or disagree to participate in the study. In case the participant agrees to participate, it is transferred directly to the study questionnaire. Otherwise, it would receive a thankful message and exit the study questionnaire. Moreover, the confidentiality of the participants’ data was ensured throughout and during the study. Respondents received no financial incentive for participating. Data were collected from May 1 to July 15, 2021.
Data Collection
From the electronic health system, a list of 1056 patients with type 1 and 2 DM was obtained. Patients who did not fulfil the inclusion criteria were excluded from the study, and the next selected patient was contacted. The online questionnaire was sent to the first 352 patients who fulfilled the criteria and verbally agreed to participate in the study on the phone.
Participants
The target population consisted of persons with type 1 and type 2 diabetes mellitus who were followed up in diabetic clinics at King Saud University Medical City. Men and women above the age of 18 years who understood Arabic were considered eligible for the study. Patients were excluded if they did not understand Arabic, had no access to the online questionnaire, did not know how to access it, or provided incomplete or incorrect data. Participation in the study was voluntary.
Survey Instruments and Variables
The questionnaire was developed by the primary investigator and co-investigators based on expert opinion and the literature.2 The survey was then reviewed by three specialized diabetologists and one family physician who had experience in questionnaire development. Next, the questionnaire was tested in a pilot study consisting of 45 participants to ensure clarity and flow of questions. Comments by these participants were taken into consideration, and modifications were applied accordingly.
The questionnaire was divided into three main sections. The first section contained demographic data, such as age, gender, marital status, education level, and type of diabetes. The second section included various questions about the type of nondisclosed information. Specifically, patients were asked if they had ever not disclosed any of the following information for diabetes disease follow-up: (i) if they were not dieting, (ii) no regular exercise, (iii) non-adherence to prescribed medications, (iv) not reporting some glucose readings, (v) not following instruction for weight loss, (iv) not telling the doctor about hypoglycemic episodes, (iiv) not telling doctor about hyperglycemic episodes, (iiiv) taking prescriptions from someone else, and (ix) not understanding the healthcare provider’s instructions. An additional two questions were specific for type 1 diabetes: (i) not monitoring carbohydrate intake and (ii) not taking correction doses as instructed. The third section included questions about the reasons behind nondisclosure of information to healthcare providers.
The validity of the data collection instrument was ensured through consulting seven experts who are specialized in patient education, chronic diseases, diabetes mellitus and health administration. The apparent validity was ensured after taking into consideration the linguistic and content amendments suggested by the experts. In addition, the data collection instrument was ensured for reliability through administering the data collection instrument over a sample of 20 persons with type 1 and type 2 diabetes mellitus with a time interval of two weeks. The Cronbach’s alpha coefficient was found to be 0.83.
Sample Size
To calculate the sample size, G*Power 3.1.9.7 software was used. The minimum sample size was found to be 271 participants based on the related χ2 test using an effect size of 0.5 based on the effect size reported in Levy et al2 a significance level of 0.05, and a power of 0.90. To avoid technical issues, such as drop-outs, another 30% was added. Therefore, the sample size was calculated to be 352 participants. A total of 352 questionnaires were distributed, and a total of 285 completed and valid questionnaires (response rate 80.9%) were retrieved for data analysis.
Data Analysis
Data were analyzed using the Statistical Package of Social Sciences (SPSS) (v. 26 IBM Corp.). Frequencies and percentages were used to describe the socio-demographic characteristics of the study participants). A chi-squared of independence was used to identify the differences in types and reasons of nondisclosed information between persons with type 1 and type 2 diabetes mellitus. In addition, a chi-squared of independence was used to identify the interaction between diabetic patients’ socio-demographic characteristics and nondisclosure of information. A value of α ≤ 0.05 was used as a threshold for statistical significance in this study.
Results
Study Population
The results presented in Table 1 show the demographic characteristics of the study participants. A total of 285 diabetic patients were included in this study, including 155 persons with type 1 DM (54.4%) and 130 persons with type 2 DM (45.6%). The most represented age range was 18 to 29 years, which constituted 27.4% (n = 78), whereas the least represented range was 70 years or more, which constituted 5.6% (n = 16). Females constituted 54.7% (n = 156), whereas male diabetic patients represented 45.3% (n = 129), as shown in Table 1.
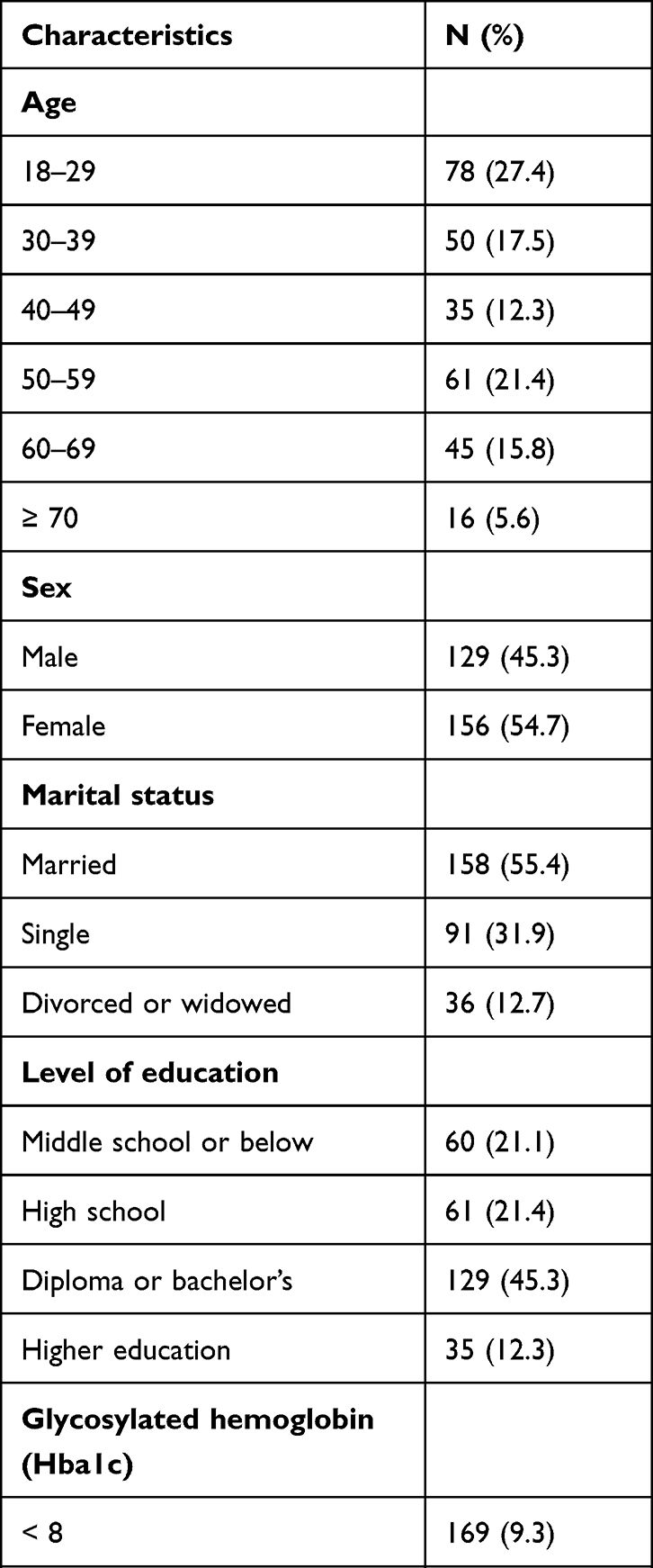 |
Table 1 Distribution of Respondents According to Demographic and Clinical Characteristics |
Nondisclosure Among the Diabetic Patients
Having unhealthy diets (unhealthy nutrition) was the most reported type of nondisclosed information (25.3%, n = 72), followed by not exercising regularly (23.5%, n = 67), hiding some glucose readings (23.2%, n = 65), and not following instructions for weight loss (22.8% n = 44) (Table 2). The most common reasons for nondisclosure were feeling apprehensive about telling the doctor about not following instructions (28.1%, n = 80), followed by the desire to be considered as a cooperative patient by healthcare providers (27%, n = 77), and feeling worried about healthcare providers (26.7%, n = 76), as shown in Table 3.
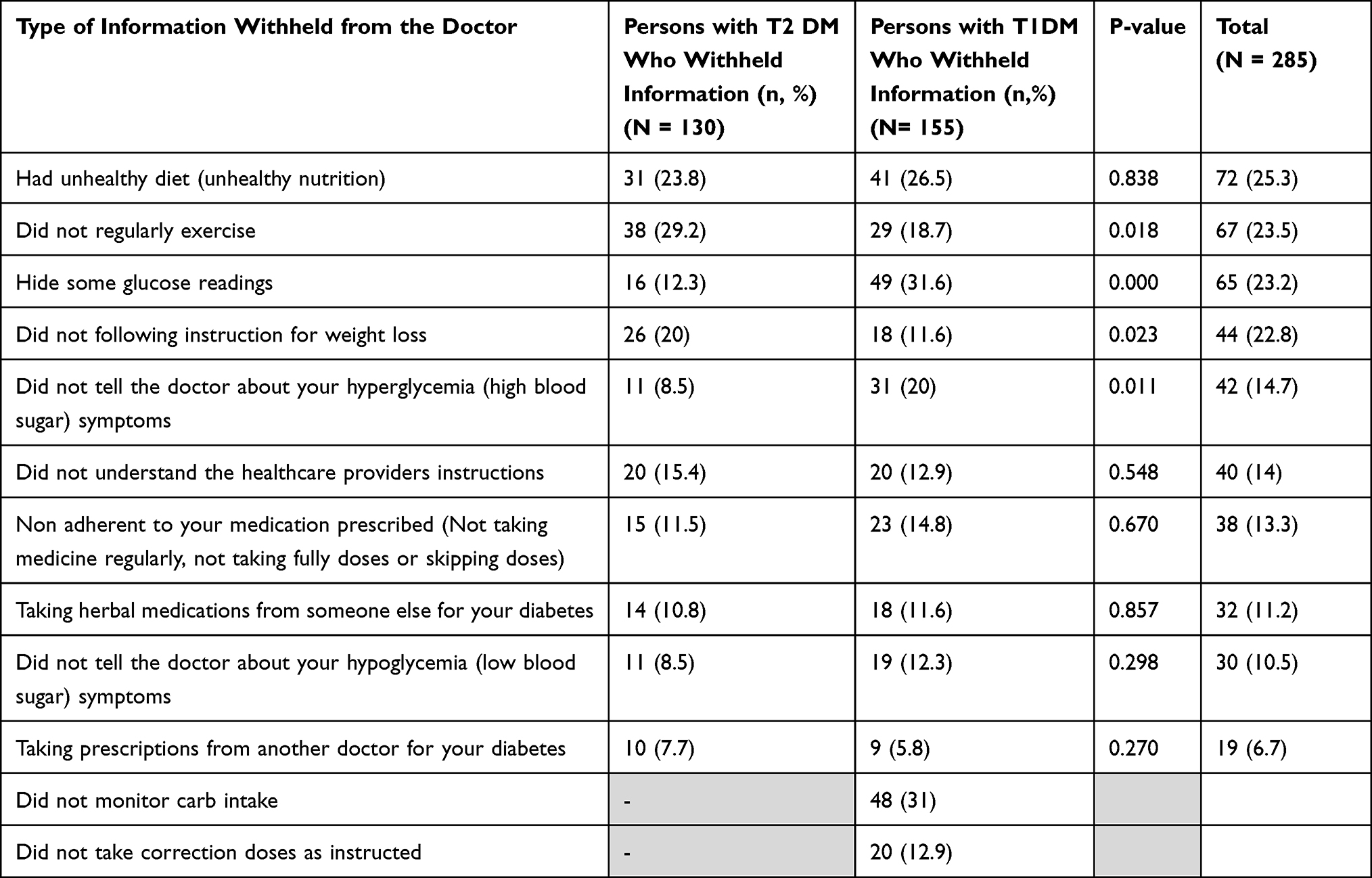 |
Table 2 Types of Information Not Disclosed to the Doctor |
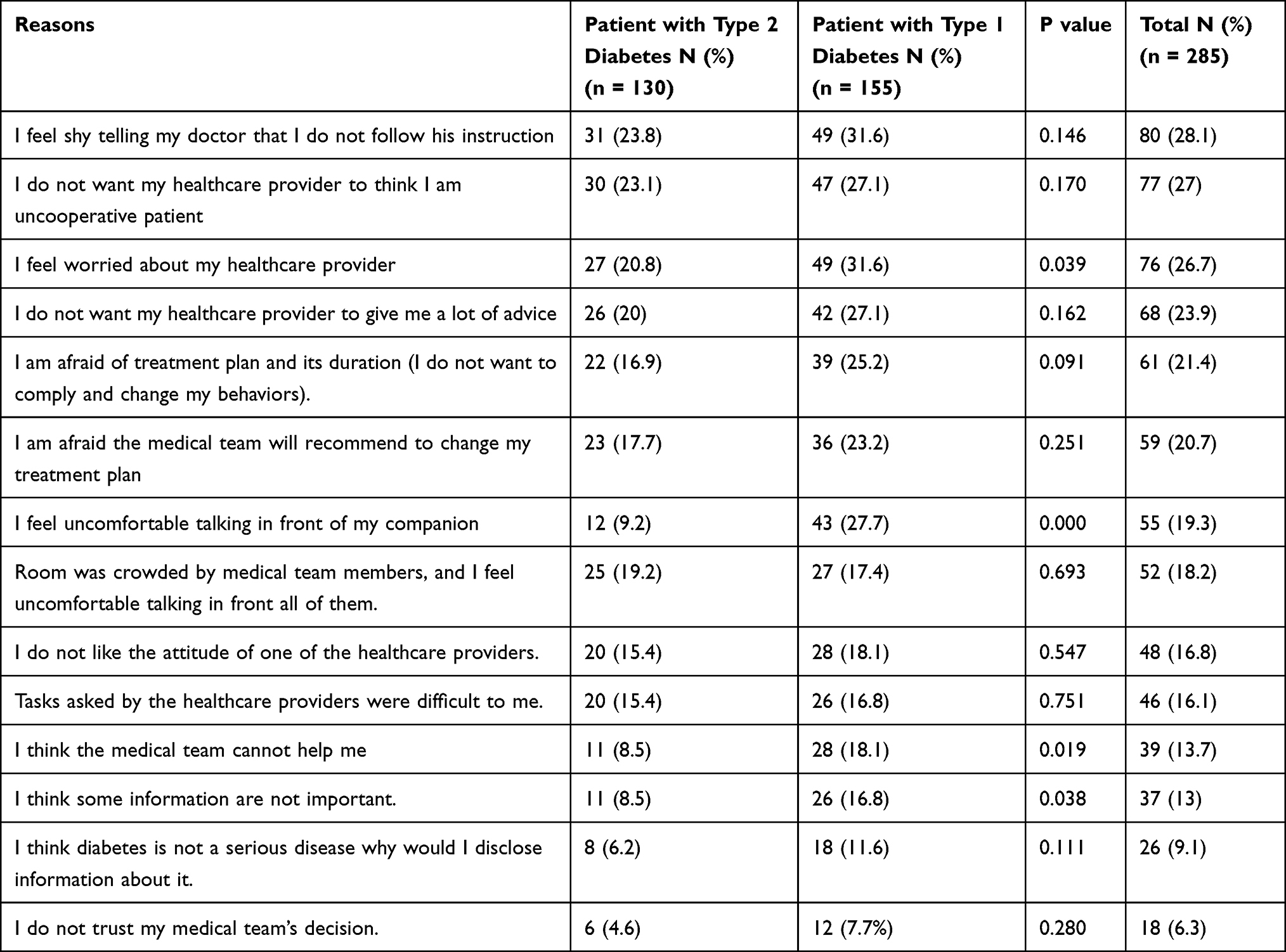 |
Table 3 Selected Reasons for Not Telling the Doctors Across Types of Information by Patients Who Reported Withhold of Information from the Doctor |
Nondisclosure Among Type 1 Diabetes
Among persons with type 1 DM, glucose readings were the most common type of information withheld from doctors (31.6%, n = 49), followed by not monitoring carb intake (31%, n = 48) and having an unhealthy diet (26.5%, n = 41), as shown in Table 2. The results in Table 3 reveal that significant differences in withholding information related about some glucose readings (p = p< 0.001) and not telling the doctor about hyperglycemia symptoms (p = 0.011) were the major differences between persons with type 1 and type 2 diabetes mellitus: persons with type 1 DM were more likely to withhold this type of information compared to persons with type 2 DM.
Finally, the statistical differences in reasons for nondisclosure between persons with type 1 and type 2 diabetes mellitus were inspected. Significant statistical differences were found in many aspects, including feeling worried about healthcare providers (p = 0.039), feeling uncomfortable talking in front of companions (p< 0.001), believing that the medical team cannot help them (p = 0.019), and considering that some information was not important (p = 0.038). Persons with Type 1 DM were more likely than persons with type 2 DM to withhold information for these reasons.
Nondisclosure Among Type 2 Diabetes
The types of information withheld from the doctor by persons with type 2 DM were most commonly not exercising regularly (29.2%, n = 38), having unhealthy diets (23.8%, n = 31), and not following instructions for weight loss (20%,(as shown in Table 2. The most common reasons were feeling apprehensive about telling the doctor about not following instructions (23.8%, n = 31), the desire to be considered as a cooperative patient by healthcare providers (23.1%, n = 30), and feeling worried about healthcare providers (20.8%, n = 27), as shown in Table 3. The results show that there were significant differences in concealing information about non-exercising on a regular basis (p = 0.018) between persons with type 1 and type 2 diabetes mellitus: persons with type 2 diabetes were more prone to hide this type of information than persons with type 1 DM.
Discussion
This cross-sectional study was conducted to evaluate the prevalence of medical information nondisclosure to healthcare providers among persons with type 1 and type 2 diabetes mellitus.
The most common types of information that is not disclosed by persons with diabetes are having an unhealthy diet, not doing exercise, hiding some readings, not following instructions about weight loss, and not talking about hyperglycemia. The top reason for nondisclosure was apprehension about telling healthcare providers about not following instructions.
Hiding some glucose readings and not exercising regularly were the most common types of nondisclosed types of information among persons with type 1 and type 2 diabetes mellitus, respectively. The nondisclosure of information was significantly higher among persons with type 2 DM compared to persons with type 1 and type 2 diabetes mellitus in terms of not participating in regular exercise. Similarly, the nondisclosure of information was significantly higher among persons with type 1 DM compared to persons with type 2 DM in terms of hiding some glucose readings and not talking about their hyperglycemia. Regarding reasons for nondisclosure, persons with type 1 DM had significantly higher trends compared to persons with type 2 DM in terms of being worried about their healthcare provider, feeling uncomfortable talking in front of their companions, feeling the medical team could not help them, and thinking that the information was not important. These might be referred to the lack of trust or even lack of effective communication among the healthcare providers and the DM patients. In addition, this might be referred to a weakness in the patient-healthcare provider relationship.
It is clear that clinicians’ decisions depend on accurate information reported by patients and their families, and effective bidirectional communication is necessary to make decisions. However, doctor–patient relationships are often challenged by complicated communications in which both the clinician and patient may withhold, fabricate, or hide information that can damage the relationship and may affect treatment.11 Disclosure of medical errors on the part of clinician and misrepresenting information on the part of patients are two examples of how information is often fabricated or withheld. The manipulation of information in clinical setup results in compromised care.11 In this context, if persons with DM are not truthful with clinicians for whatever reason, patient care and glycemic control will be compromised.
There are many reasons that can lead to nondisclosure of information. Levy et al2 conducted a study to determine the frequency and factors associated with patient nondisclosure. They reported that patients would withhold important information from clinicians when they disagreed with or misunderstood the clinicians’ advice. Most often, the patients did not want to be judged, lectured, or embarrassed.2
Most often, adherence to antidiabetic medicines seems to be suboptimal, which may result in nondisclosure of information to the clinicians, leading to poor and suboptimal glycemic control.12 Therefore, transparency of persons with DM with their healthcare providers is critical for the optimal management of diabetes and its complications. A good doctor–patient relationship may prevent nondisclosure of information among persons with DM. It has been reported that about 60%–80% of patients hide medically relevant information from their clinicians.13
Recently, a study reported that 47% of patients hide information about diet, exercise, sex life, and treatment adherence from their healthcare providers.13 Fekadu et al14 conducted a hospital-based study to determine challenges and factors associated with poor glycemic control among persons with type 2 DM. They reported “not following general dietary programs correctly” and “illiteracy” as the top causes of poor glycemic control. The present study reveals that having an unhealthy diet, not exercising, hiding some glucose readings, not following instructions about weight loss, and not talking about hyperglycemia were the most common types of nondisclosed medical related information among persons with DM. Hence, nondisclosed related medical information by persons with type 1 and type 2 diabetes mellitus may result in poor decisions by the healthcare providers, resulting in poor glycemic control, increased incidence of diabetes complications, and poor quality of life.15
The present study is unique and focuses on the prevalence of nondisclosure of medical information to healthcare providers among persons with DM in Saudi Arabia. It compares the types of nondisclosed information among persons with type 1 and type 2 diabetes mellitus. One interesting finding is that there were different trends in types and causes of nondisclosed related medical information among type 1 and 2 diabetic patients. Not only in Saudi Arabia, but studies worldwide are also lacking on this topic, and this study is the first to address nondisclosure among diabetic patients. A potential implication of this study may be to evaluate selected patients in high risk group for evaluation of non-disclosure of information as it may not be feasible to roll out to all diabetes patients in view of resource limitation.
One of the limitations of the study is that that it was a single-center study. Moreover, we recognize the possibility that respondents may not have been completely genuine in their responses to the survey. As a result, we believe our findings might underestimate the degree to which patients hide information from doctors. Another limitation is the inability to assess unintended omission of providing the information due to limited consultation time / lack of questioning from doctors. A third limitations is not considering the treatment and pathophysiological differences between patients with type I and type II when structuring the study questionnaire.
In conclusion, diabetic patients in Saudi Arabia often hide information from their healthcare providers for various reasons. To provide better care to persons with DM, this behavior must be overcome. In addition, the study concluded that DM patients hold negative perceptions and attitudes about their healthcare providers that lead them to withhold information from their doctors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agaku IT, Adisa AO, Ayo-Yusuf OA, Connolly GN. Concern about security and privacy, and perceived control over collection and use of health information are related to withholding of health information from healthcare providers. J Am Med Informatics Assoc. 2014;21:2. doi:10.1136/amiajnl-2013-002079
2. Levy AG, Scherer AM, Zikmund-Fisher BJ, Larkin K, Barnes GD, Fagerlin A. Prevalence of and factors associated with patient nondisclosure of medically relevant information to clinicians. JAMA Netw open. 2018;1:7. doi:10.1001/jamanetworkopen.2018.5293
3. World Health Organization. WHO - The Top 10 Causes of Death. 24 Maggio; 2018.
4. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Kaabi J. Epidemiology of Type 2 diabetes - Global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–111. doi:10.2991/jegh.k.191028.001
5. Al-Nozha MM, Arafah MR, Al-Maatouq MA, et al. Hyperlipidemia in Saudi Arabia. Saudi Med J. 2008;29:2.
6. Alotaibi A, Perry L, Gholizadeh L, Al-Ganmi A. Incidence and prevalence rates of diabetes mellitus in Saudi Arabia: an overview. J Epidemiol Glob Health. 2017;7(4):211. doi:10.1016/j.jegh.2017.10.001
7. Afroz A, Zhang W, Wei Loh AJ, Jie Lee DX, Billah B. Macro- and micro-vascular complications and their determinants among people with type 2 diabetes in Bangladesh. Diabetes Metab Syndr Clin Res Rev. 2019;13:5.
8. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14(2):88–98. doi:10.1038/nrendo.2017.151
9. Ewers B, Vilsbøll T, Andersen HU, Bruun JM. The dietary education trial in carbohydrate counting (DIET-CARB Study): study protocol for a randomised, parallel, open-label, intervention study comparing different approaches to dietary self-management in patients with type 1 diabetes. BMJ Open. 2019;9:9.
10. Mirahmadizadeh A, Khorshidsavar H, Seif M, Sharifi MH. Adherence to medication, diet and physical activity and the associated factors amongst patients with type 2 diabetes. Diabetes Ther. 2020;11:2. doi:10.1007/s13300-019-00750-8
11. Palmieri JJ, Stern TA. Lies in the doctor-patient relationship. Prim Care Companion J Clin Psychiatry. 2009;11:4. doi:10.4088/PCC.09r00780
12. Araya EM, Gebrezgabiher HA, Tekulu GH, et al. Medication non-adherence and associated factors among diabetic patients visiting general hospitals in the eastern zone of Tigrai, Northern Ethiopia. Patient Prefer Adherence. 2020;14:2071.
13. Vogel L. Why do patients often lie to their doctors? CMAJ. 2019;1:191.
14. Fekadu G, Bula K, Bayisa G, Turi E, Tolossa T, Kasaye HK. Challenges and factors associated with poor glycemic control among type 2 diabetes mellitus patients at nekemte referral hospital, Western Ethiopia. J Multidiscip Healthc. 2019;12:845.
15. Fiseha T, Alemayehu E, Kassahun W, Adamu A, Gebreweld A. Factors associated with glycemic control among diabetic adult out-patients in Northeast Ethiopia. BMC Res Notes. 2018;11(1):548. doi:10.1186/s13104-018-3423-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.